


Abstract
A single-site prospective open-label clinical study with cyclotron-produced sodium 99mTc-pertechnetate (99mTc-NaTcO4) was performed in patients with indications for a thyroid scan to demonstrate the clinical safety and diagnostic efficacy of the drug and to confirm its equivalence with conventional 99mTc-NaTcO4 eluted from a generator. Methods: 99mTc-NaTcO4 was produced from enriched 100Mo (99.815%) with a cyclotron (24 MeV; 2 h of irradiation) or supplied by a commercial manufacturer (bulk vial eluted from a generator). Eleven patients received 325 ± 29 (mean ± SD) MBq of the cyclotron-produced 99mTc-NaTcO4, whereas the age- and sex-matched controls received a comparable amount of the generator-derived tracer. Whole-body and thyroid planar images were obtained for each participant. In addition to the standard-energy window (140.5 keV ± 7.5%), data were acquired in lower-energy (117 keV ± 10%) and higher-energy (170 keV ± 10%) windows. Vital signs and hematologic and biochemical parameters were monitored before and after tracer administration. Results: Cyclotron-produced 99mTc-NaTcO4 showed organ and whole-body distributions identical to those of conventional 99mTc-NaTcO4 and was well tolerated. All images led to a clear final diagnosis. The fact that the number of counts in the higher-energy window was significantly higher for cyclotron-produced 99mTc-NaTcO4 did not influence image quality in the standard-energy window. Image definition in the standard-energy window with cyclotron-produced 99mTc was equivalent to that with generator-eluted 99mTc and had no particular features allowing discrimination between the 99mTc production methods. Conclusion: The systemic distribution, clinical safety, and imaging efficacy of cyclotron-produced 99mTc-NaTcO4 in humans provide supporting evidence for the use of this tracer as an equivalent for generator-eluted 99mTc-NaTcO4 in routine clinical practice.
Despite a steady increase in procedures with PET, the role of 99mTc in nuclear imaging remains important, and frequent use of this tracer will continue well into the future (1). At the same time, the conventional supply chain for 99mTc is currently fragile because of aging nuclear reactors and the transition from the use of highly enriched uranium to the use of low-enriched uranium in targets for nuclear reactors. In addition, full-cost recovery for the production of medical isotopes promises to increase the prices for 99Mo/99mTc generators, rendering alternative technologies for the production of medical isotopes more competitive (2). The direct production of 99mTc by cyclotrons is a decentralized approach that could satisfy the demand for 99mTc on a regional level (3) and help alleviate the low supply of 99mTc.
The production of 99mTc via proton irradiation of enriched 100Mo results in the coproduction of several 9xTc radionuclides. Hence, the safety and imaging characteristics of cyclotron-produced 99mTc must be assessed for any unanticipated adverse effects. The first clinical trial demonstrated that cyclotron-produced 99mTc-pertechnetate obtained at 17 MeV was safe in humans (4). Theoretic (5) and empiric (6) analyses showed that the 99mTc production yield doubled when incident energy increased from 16 to 24 MeV. However, the radionuclidic purity greatly depended on the irradiation conditions, in particular, on the incident proton beam energy and irradiation time (6,7).
To take advantage of the higher production capacity of medium-energy cyclotrons, we first investigated the quality of 99mTc produced at 24 MeV. Its chemical and radiochemical purity as well as patient dosimetry were shown to be suitable for human use (7). A prospective open-label clinical study with sodium 99mTc-pertechnetate (99mTc-pertechnetate; 99mTc-NaTcO4) prepared from a cyclotron at 24 MeV was initiated in patients with indications for a thyroid scan to demonstrate the clinical safety and diagnostic efficacy of the radiopharmaceutical and to confirm its utility in clinical procedures (ClinicalTrials.gov identifier: NCT02307175; approved by Health Canada). The images were analyzed qualitatively and quantitatively and compared with those obtained with conventional 99mTc-pertechnetate eluted from a generator.
MATERIALS AND METHODS
Provision of 99mTc-Pertechnetate
99mTc was produced on-site with a TR-24 cyclotron (Advanced Cyclotron Systems, Inc.) by irradiation of enriched 100Mo (99.815%; 0.17% 98Mo; 0.003% each 92Mo−97Mo) at 24 MeV for 2 h as described previously (7). The targets were processed to recover an effective thickness corresponding to an energy loss of approximately 5 MeV. Extraction of 99mTc was performed following a published procedure (7) that was a modification of another procedure (8). Quality control of the formulated 99mTc-pertechnetate solution for injection was done for all prepared batches in accordance with previously described standard procedures (7). The endotoxin levels were assayed by the Limulus amebocyte lysate method with an Endosafe-PTS test system (Charles River Laboratories International, Inc.). Sterility tests were performed by a licensed laboratory (Nucro-Technics). Generator-eluted 99mTc was supplied by Isologic Innovative Radiopharmaceuticals.
Study Design
This single-site prospective nonrandomized case–control open-label study included 19 patients who were referred to the nuclear medicine department with indications for a thyroid scan. The study was approved by the institutional ethics committee and by Health Canada. Each patient signed an approved written informed consent form. The recruited patients had thyroid disease (hyperthyroidism or thyroid nodule assessment), were 18−80 y old, had biochemical parameters within normal limits for their ages, and had a Karnofsky performance status of greater than 50%. Eleven recruited participants were administered cyclotron-produced 99mTc-NaTcO4 (340 MBq ± 10%). Eight participants were paired by sex and age (±1 y) with the first group and were administered the same amount of 99mTc-NaTcO4 supplied commercially (eluted from a generator) to serve as a control cohort. All participants underwent a prescribed thyroid imaging procedure and an additional whole-body scan.
Safety Monitoring
Safety was assessed by monitoring vital signs, biochemical laboratory test results, and adverse events at various time points during the study. On the day of the procedure, the participants were examined by a physician. Physical examination included the lungs, heart, vascular system, lymph nodes, and skin and a neurologic assessment. Vital signs (body temperature, blood pressure, heart rate, and respiratory rate), electrocardiogram, and oxygen saturation level were monitored before and after tracer administration. Blood samples were collected for hematologic and biochemical tests (complete blood count with differential and comprehensive metabolic panel) before and after tracer administration. Adverse events were monitored during the procedure and up to 24 h after the procedure. Participants were enrolled sequentially when no adverse events were reported by previous participant.
Estimation of Internal Radiation Dose
Estimation of the internal radiation dose for each patient was based on the amount of each technetium radioisotope present in the radiopharmaceutical preparation at the time of intravenous administration. The calculations were performed as described elsewhere (7), and the obtained values were compared with the predicted dose increase (7).
Image Acquisition
Thyroid images were acquired for 10 min in the planar mode with an Infinia Hawkeye 4 SPECT/CT camera (GE Healthcare) equipped with a 3-mm pinhole collimator (image matrix, 256 × 256). After thyroid imaging, anterior and posterior whole-body planar projections (4 or 5 bed positions; 3 min each) were acquired with a Discovery NM/CT 670 SPECT/CT camera (GE Healthcare) equipped with low-energy high-resolution collimators (image matrix, 256 × 1,024). For whole-body imaging, data were acquired in lower-energy (117 keV ± 10%) and higher-energy (170 keV ± 10%) windows in addition to the standard-energy (140.5 keV ± 7.5%) window.
Image Analysis: Biodistribution and Quality Evaluation
Qualitative image analysis based on visual interpretation was performed to compare the biodistributions of 99mTc-pertechnetate produced by both methods. Two nuclear medicine specialists were asked to rate the uptake as absence of uptake, light uptake, or intense uptake in the brain, thyroid, salivary glands, heart blood pool, lungs, liver, stomach, kidneys, bladder, soft tissues, and bone. Next, the interpreters were asked to rate the biodistribution of 99mTc-pertechnetate as normal or abnormal, taking into account the presence of specific diseases that may modify the biodistribution (e.g., complete thyroid resection explaining the absence of thyroid uptake or gastric hiatal hernia indicating mediastinal uptake). For the evaluation of image quality, both nuclear medicine specialists were shown the images randomly and were asked to tentatively discriminate between 99mTc-pertechnetate production methods.
For the quantitative evaluation of possible interference due to scatter from high-energy isotopic impurities, the geometric means of the raw count data from the anterior and posterior whole-body projections in each acquisition were computed for the standard-, lower-, and higher-energy windows. The ratios of the geometric mean counts in the lower-energy window and the higher-energy window to those in the standard-energy window were then calculated and compared for the cyclotron- and generator-produced radiotracers.
Statistics
Blood test results, biochemical test results, and vital signs were compared before and after 99mTc-pertechnetate injection with a Wilcoxon matched-pairs signed rank test. Results with P values of less than 0.05 were considered significant and clinically significant when outside normal physiologic limits.
Phantom Imaging
Planar images were acquired with a Discovery NM/CT 670 SPECT/CT camera equipped with low-energy high-resolution collimators (image matrix, 512 × 512). Three energy windows were used for image acquisition: standard, 141 keV ± 7.5%; lower, 120 keV ± 5%; and higher, 165 keV ± 5%. A Jaszczak phantom (Jaszczak Flangeless Deluxe SPECT Phantom [Biodex]; cold-rod diameters: 4.8, 6.4, 7.9, 9.5, 11.1, and 12.7 mm; cylinder interior dimensions: Ø 20.4 × 18.6 cm) filled with a solution of 99mTc-pertechnetate was positioned vertically on top of the camera collimator. Images (1 at each time point) were acquired to reach comparable total numbers of counts for generator-eluted 99mTc (730 MBq) and cyclotron-produced 99mTc (620−746 MBq) at 5, 7.5, 9, 11, 13, 15, and 17 h after the end of bombardment (EOB). Image contrast and contrast-to-noise ratio (CNR) were calculated with the following equations:  where Ri are counts per second per pixel and σi are standard deviations. The Rcold values were determined by averaging the background count rates in the largest (12.7 mm) cold spots, whereas the Rhot values were estimated in a large region of interest surrounding the cold spots.
where Ri are counts per second per pixel and σi are standard deviations. The Rcold values were determined by averaging the background count rates in the largest (12.7 mm) cold spots, whereas the Rhot values were estimated in a large region of interest surrounding the cold spots.
RESULTS
Provision of 99mTc-Pertechnetate
Cyclotron-produced 99mTc-NaTcO4 solutions for injection had a radioactive concentration of 329 ± 84 (mean ± SD) MBq/mL (range, 230−471 MBq/mL), a pH of 5.0−5.5, a radiochemical purity of at least 98%, and a radioisotopic purity of greater than 99.97% (Table 1). All prepared batches complied with standard requirements for parenteral injections, including sterility and endotoxin level.
Radioisotopic Composition of Cyclotron-Produced (24→19 ± 1 MeV, 2 h) 99mTc-Pertechnetate at EOB
Patient Demographics and Study Design
The 11 participants injected with cyclotron-produced 99mTc-NaTcO4 received 325 ± 29 MBq (range, 271−353 MBq). Most participants were women (73%). The mean age was 44.7 ± 17.3 y (range, 19−77 y; median, 45 y). The body mass index was 26.3 ± 5.8 (range, 17.2−35.8). Four of the 11 patients had Graves disease, 4 had thyroiditis, and the others had hypothyroidism, subclinical hyperthyroidism, or multinodular goiter. Cyclotron-produced 99mTc-pertechnetate was administered between 4 h 40 min and 7 h 3 min (280−423 min) after the EOB. On average, the time of injection was approximately 6 h from the EOB.
Eight participants paired by age and sex with the first group were injected with conventional 99mTc-NaTcO4 and received 342 ± 5 MBq. In this cohort, 75% of the participants were women. The mean age was 43.8 ± 13.9 (range, 28−66; median, 41). The body mass index was 23.8 ± 8.0 (range, 16.2−39.8). By indication, 2 patients had Graves disease, 2 had subclinical hyperthyroidism, 2 had nonfunctional nodules, 1 had multinodular goiter, and 1 had thyroiditis. The patients were not paired by clinical indication.
All patients enrolled in the study completed the trial. Nevertheless, 2 patients did not undergo the entire study protocol because of technical issues. One patient injected with cyclotron-produced 99mTc-NaTcO4 had an incomplete blood test. Patient demographics are summarized in Table 2.
Demographic Data
Safety Evaluation
For cyclotron-produced 99mTc-NaTcO4, heart rate and blood pressure were within normal limits for all patients and did not change significantly after injection. Hematologic and biochemical test results did not show any significant changes and were well within physiologic values (Table 3). No clinically detectable pharmacologic effects or adverse events were reported during the study.
Results of Selected Biochemical and Hematologic Tests
Dosimetry
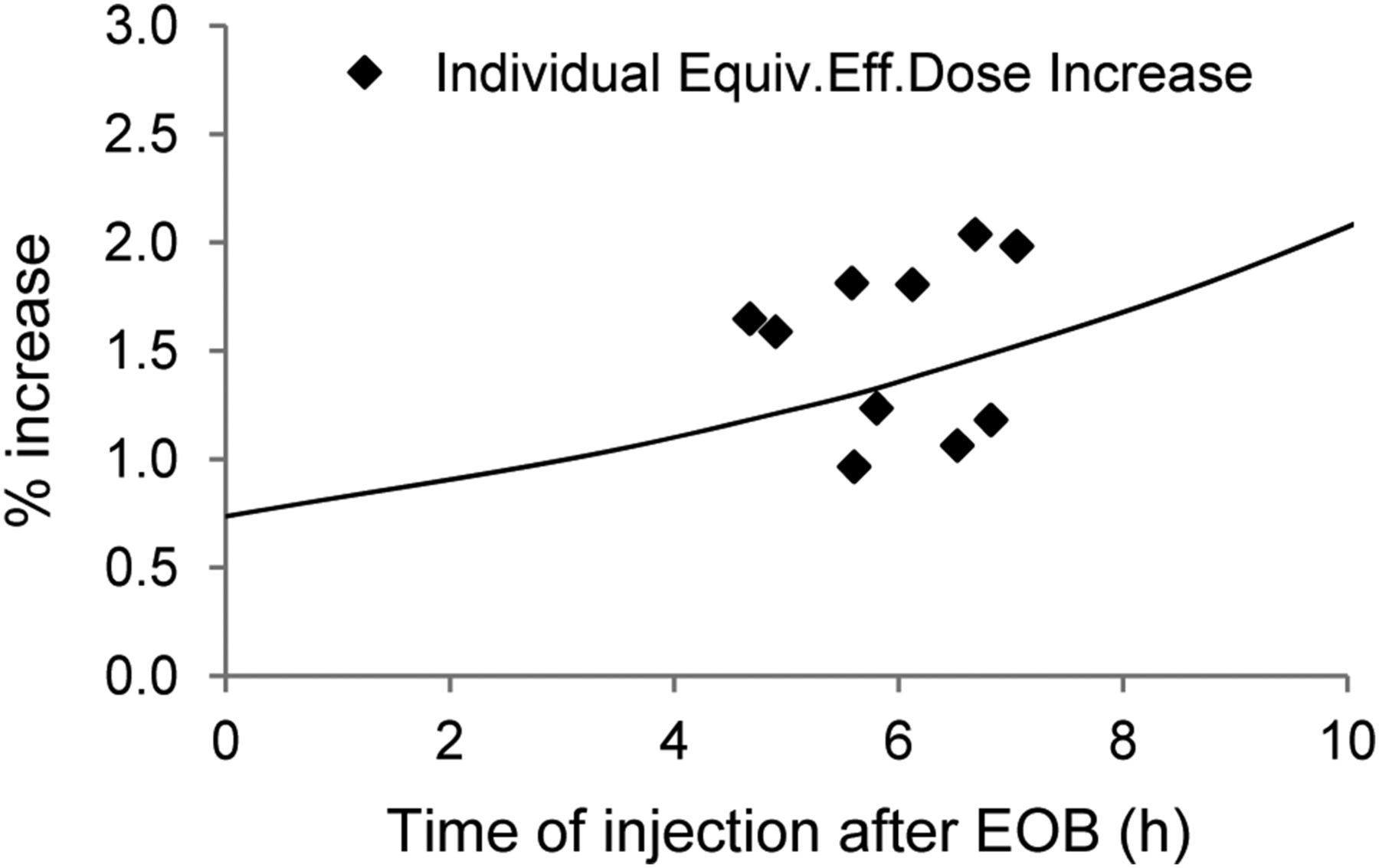
On average, the increase in the effective dose over that for 99mTc-pertechnetate without any radionuclidic impurities was 1.5% ± 0.4%.
Imaging
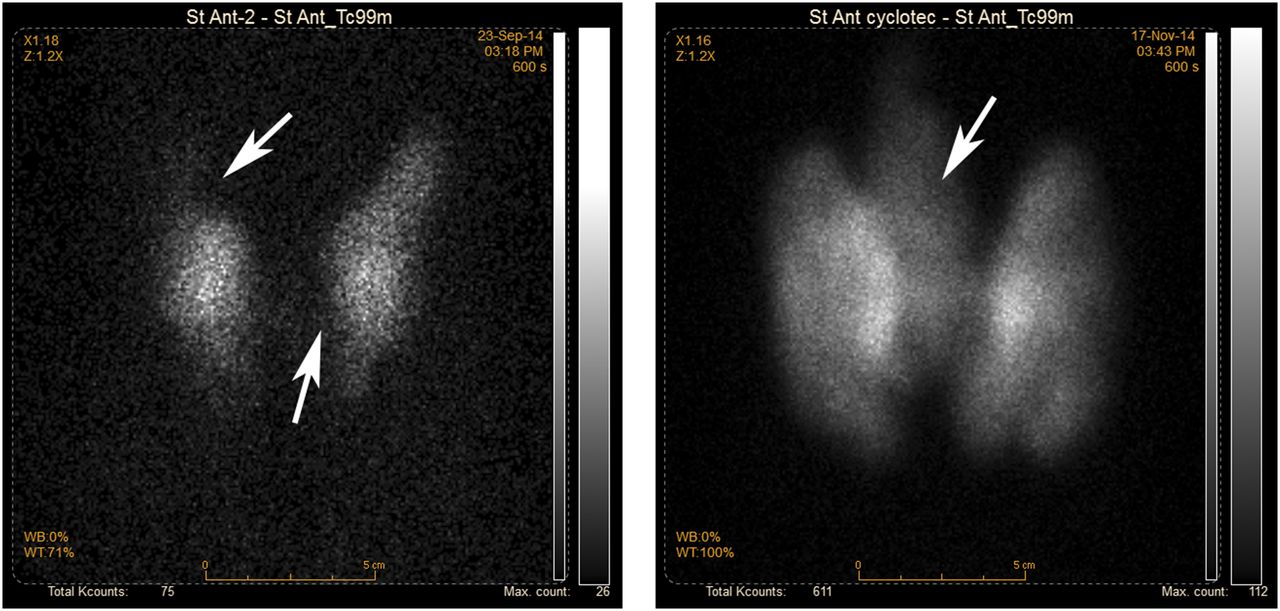
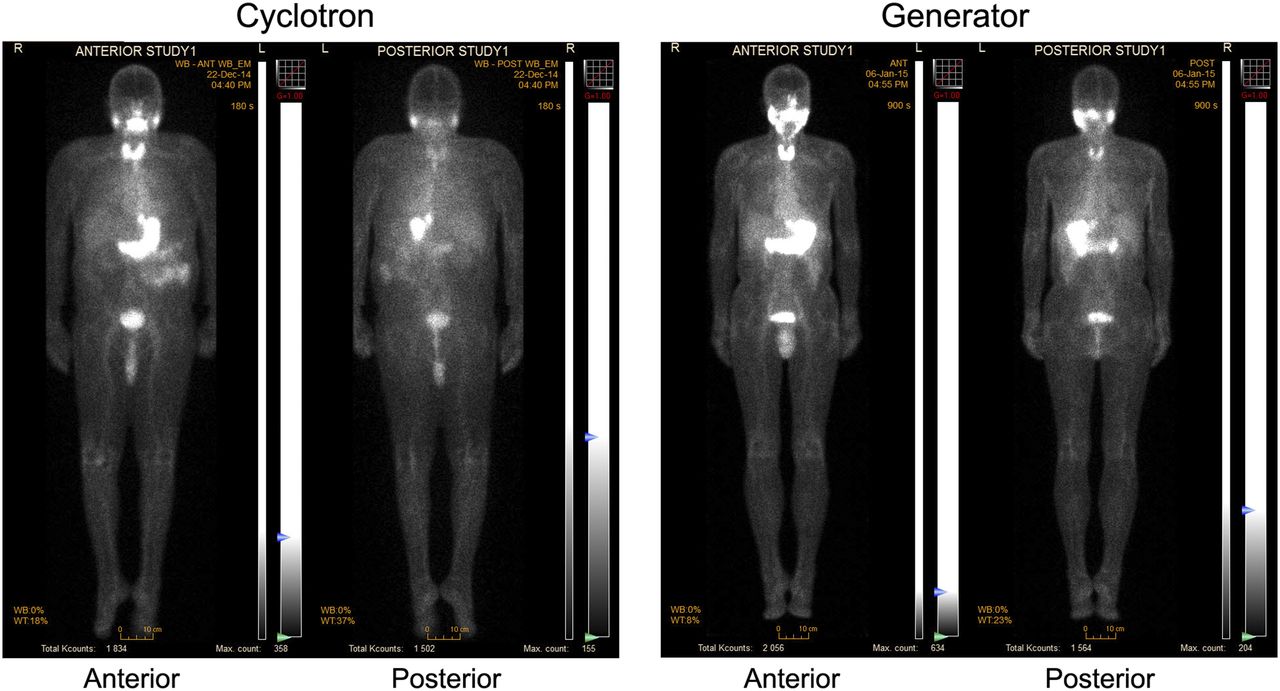
At the time of imaging, low-level radioactivity was still present in the blood pool. Low-level radioactivity was also observed in the lungs, liver, bone, and soft tissues. The salivary glands, stomach, kidneys, and bladder had the highest uptake among the nontargeted organs, as expected. Tracer uptake in the thyroid varied from weak to strong and was dependent on the underlying pathology, as exemplified by Figure 1. As expected for 99mTc-pertechnetate, there was no uptake in the brain. The organ distributions were the same for men and women, as shown in representative images (Fig. 2). Among matched patients, the organ distributions were identical for cyclotron-produced 99mTc-pertechnetate and generator-eluted 99mTc-pertechnetate (Fig. 3).

Examples of thyroid images obtained with cyclotron-produced 99mTc-pertechnetate. (Left) Low radioactivity accumulation in cold nodules (arrows) in upper inner right lobe and in isthmus in proximity of left lobe of thyroid gland. (Right) High accumulation in thyroid gland with visible pyramidal lobe (arrow) in presence of hyperthyroidism (Graves disease).

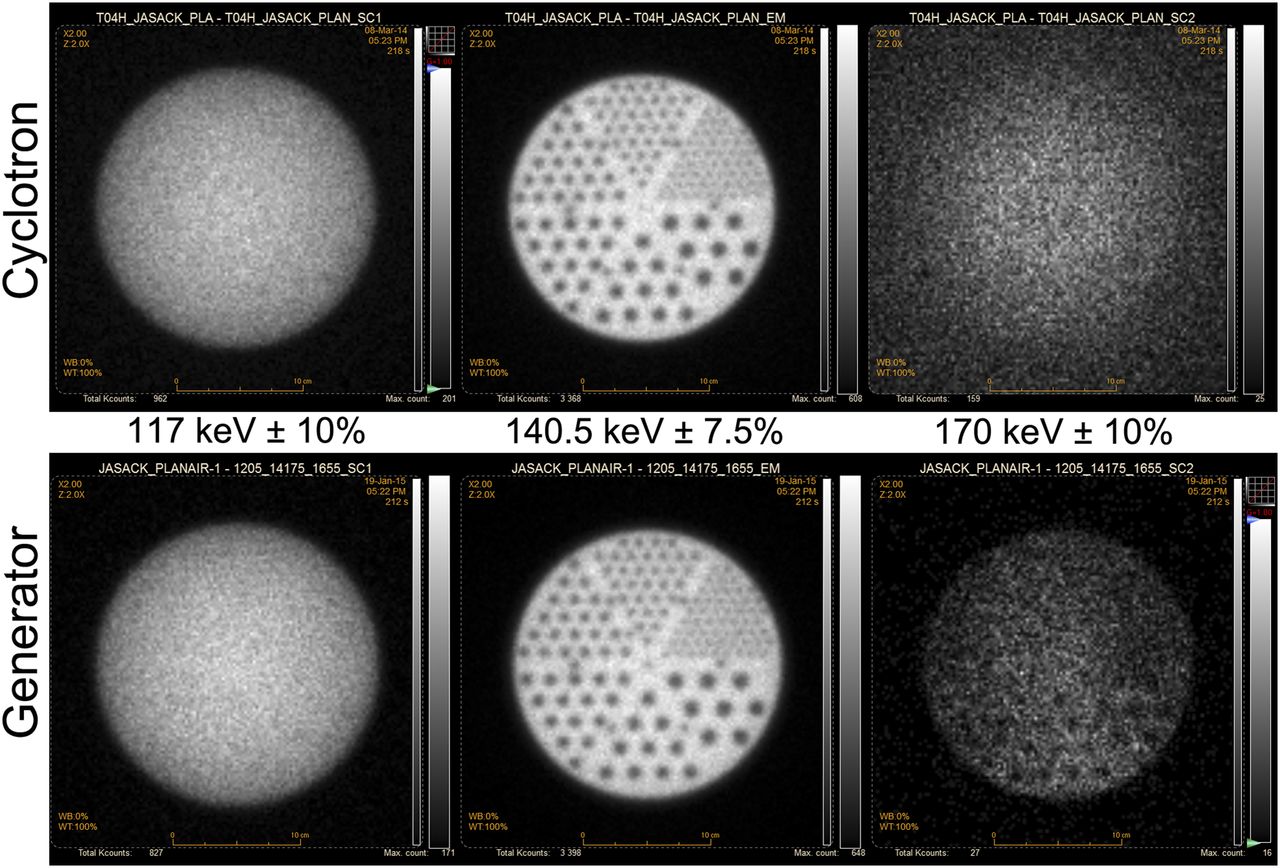
Scans obtained for 2 women and 2 men with cyclotron-produced (patient C2 [A] and patient C6 [B]) and generator-eluted (patient G6 [C] and patient G7 [D]) 99mTc-pertechnetate; anterior images are shown. Visually, image quality in standard-energy window (middle in each quadrant) and in lower-energy window (left in each quadrant) were identical for both radiotracers. Increased uniform background was observed in higher-energy window (right in each quadrant) for cyclotron-produced 99mTc. Patient data are provided in Table 2.

Scans obtained for 2 men, both with thyroiditis, with cyclotron-produced (patient C8 [left]) and generator-eluted (patient G2 [right]) 99mTc-pertechnetate. Images acquired in standard-energy window were visually equivalent in terms of expected biodistribution of tracer as well as image quality.
Visually, the images acquired in the standard- and lower-energy windows were equivalent for cyclotron-produced 99mTc-pertechnetate and generator-eluted 99mTc-pertechnetate. Interpreters were unable to classify the images according to the origin of 99mTc because of the absence of systematic image features (interobserver κ-value, 0.17; χ2 test P = 0.83). The count rate observed in the higher-energy window increased considerably for the cyclotron-produced 99mTc-pertechnetate, resulting in a subject’s faint silhouette on an almost uniform background (Fig. 2). Because no characteristic γ-rays from contaminants can be identified in the 170 keV ± 10% range, most detected events in the higher-energy window are scatters from high-energy γ-rays. The high uniform background in the higher-energy window suggests the same.
Image Analysis
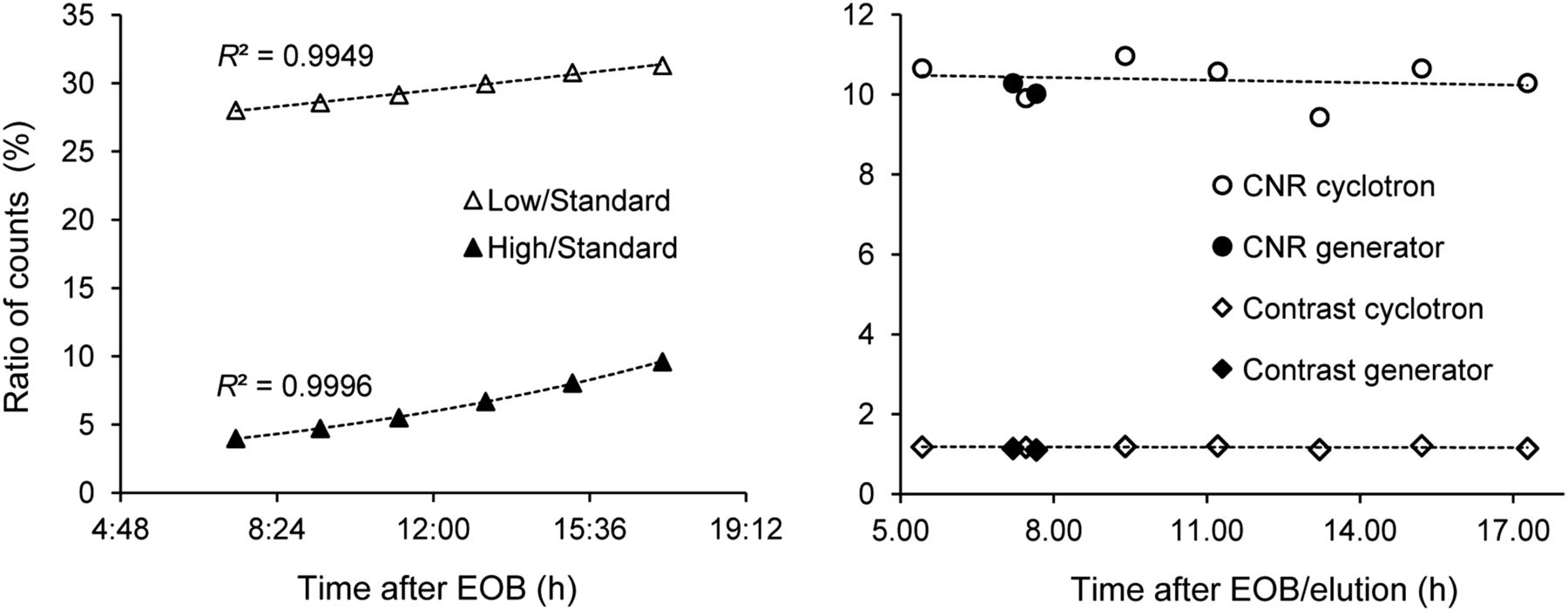
The ratios of counts in the lower-energy window to those in the standard-energy window were comparable for the cyclotron-produced radiotracer (59% ± 2%) and the generator-eluted radiotracer (54% ± 4%). The ratios of counts in the higher-energy window to those in the standard-energy window were significantly higher for cyclotron-produced 99mTc-pertechnetate (15% ± 3% vs. 4% ± 1%), in accordance with the visual image interpretation (Fig. 2). Data for individual study participants are shown in Table 4. Count ratios in the higher-energy window (170 keV ± 10%) were consistent with the expected buildup of longer-lived 96Tc (Fig. 4).
Ratios of Counts in Lower- and Higher-Energy Windows to Those in Standard-Energy Window for Individual Patients

Steady increase in ratios of counts in higher-energy window to those in standard-energy window with expected buildup of longer-lived 96Tc.
Phantom Imaging
Phantom imaging data (Fig. 5) were in agreement with the information derived from patients’ scans. We observed an increase in the ratio of counts in the higher-energy window from 2% with generator-derived 99mTc to 4%−10% with cyclotron-produced 99mTc, and this increase was dependent on the time elapsed after the EOB (Fig. 6). Nevertheless, the contrast and contrast-to-noise ratio in the standard-energy window remained stable over the course of the experiment (up to 18 h after irradiation) (Fig. 6).

Typical phantom images obtained with cyclotron-produced (9 h after EOB; 723 MBq [top]) and generator-eluted (730 MBq [bottom]) 99mTc. Images are on linear gray scale, with white representing maximum intensity. Cold rods were 4.8, 6.4, 7.9, 9.5, 11.1, and 12.7 mm in diameter.
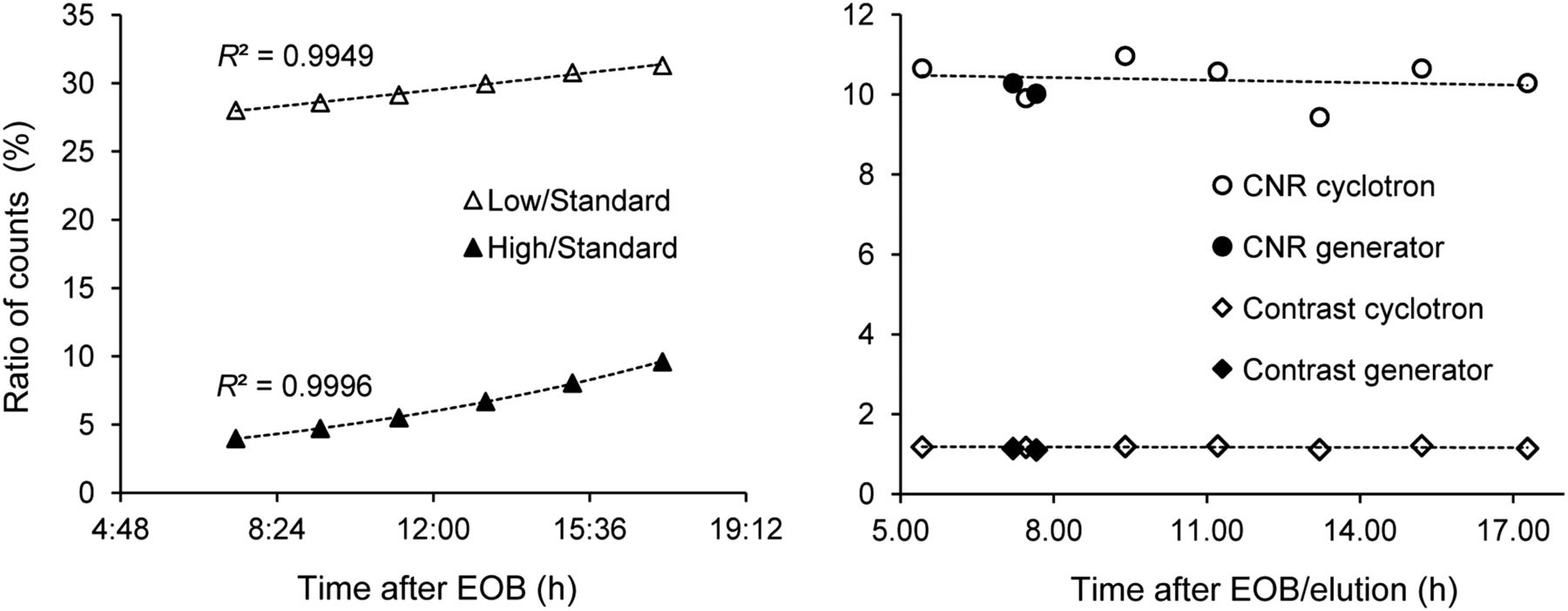
(Left) Ratios of counts in lower- and higher-energy windows to those in standard-energy window as function of time. (Right) Contrast and contrast-to-noise ratio (CNR) in standard-energy window as function of time.
DISCUSSION
The main feature distinguishing cyclotron-produced 99mTc from generator-eluted 99mTc is the presence of other technetium isotopes (Table 1) that may contribute to additional radiation doses for patients and affect image quality. The radioisotopic purity of 99mTc-pertechnetate produced with a cyclotron at medium energies (20−24 MeV) was previously evaluated, and the quality of the final formulation was confirmed to be fully adequate for clinical use, provided that the isotopic composition of the starting molybdenum and its irradiation parameters (energy and time) were appropriately selected (7). Although the radiochemical entity in the cyclotron-produced formulation (99mTc-pertechnetate) was the same as that in the generator-eluted formulation, the raw materials and chemical reagents used for manufacturing were different. Therefore, the cyclotron-produced radiopharmaceutical formulation needed to be assessed for safety for human use, and its imaging efficacy needed to be confirmed in a clinical study with a limited number of patients.
Eleven patients were successfully imaged with cyclotron-produced 99mTc-pertechnetate. The injection was well tolerated, and the patients did not report any discomfort due to tracer administration. The safety evaluation results did not indicate any alterations in sequential blood values and vital signs.
All technetium isotopes are chemically equivalent and have the same biologic retention and distribution characteristics. For the purpose of effective dose estimation, however, the actual residence time depends on the physical half-life of each isotope. In addition, the particle emission profile and energy are different for individual isotopes. Therefore, the tissue-to-organ absorbed doses vary for each technetium isotope. Since the relative proportions of technetium isotopes in a formulation change with time because of their distinct decay characteristics, the radioisotopic content of the product at the time of intravenous administration must be used to estimate patients’ doses. The obtained values, expressed as a percentage dose increase compared with 99mTc without any radionuclidic impurities (Fig. 7), fitted well with our previous calculations (7). The estimated effective dose increase observed in the present study was minimal and well below the postulated acceptable limit of 10%.

Estimated equivalent (Equiv.) effective (Eff.) dose increase for each patient injected with cyclotron-produced 99mTc. Solid line shows predicted radiation dose increase (7).
99mTc eluted from generators also contains radionuclidic impurities (9–11), but their contributions are not accounted for in a dose assessment because biokinetic data are not available for all nuclides or their corresponding radioactive chemical species. Recently, another group used a theoretic model to investigate the influence of the isotopic composition of starting molybdenum on a potential dose increase for patients and suggested thresholds for isotopic contamination of initial 100Mo by other Mo isotopes (12).
As expected, the whole-body images confirmed the normal distribution of 99mTc-pertechnetate in the thyroid, salivary glands, stomach, and urinary bladder. A comparative assessment of images of paired participants also showed this finding (Figs. 2 and 3). Images of the thyroid also correlated well with the underlying pathology (Fig. 1; Table 2); these data provided supporting evidence of the suitability of cyclotron-produced 99mTc-pertechnetate for diagnostic clinical use.
No particular characteristics were noted when the 2 nuclear medicine specialists were asked to determine which patients were injected with cyclotron-produced pertechnetate. Clinically, the images were of similar quality and showed similar biodistributions. Impurities present in the cyclotron formulation did not create any clinically relevant features on images obtained in the standard-energy window.
Quantitatively, for cyclotron-produced 99mTc, the ratio of counts increased by approximately 9% in the lower-energy window (from 54% ± 4% to 59% ± 2%). At the same time, a 4-fold increase (from 4% ± 1% to 15% ± 3%) was observed in the higher-energy window (Table 4). Nonetheless, despite the increased background in adjacent energy windows, trace amounts of isotopic impurities present in cyclotron-produced 99mTc did not affect in any significant way the image definition in the standard-energy window. As demonstrated with phantoms earlier (7) and in the present study (Figs. 5 and 6), the spatial resolution and contrast in the standard-energy window remained comparable for both cyclotron-produced 99mTc and generator-eluted 99mTc. Theoretic simulations support these findings (13). Therefore, the effect that may be due to scattering of high-energy γ-rays originating from isotopic contaminants such as 94Tc, 94mTc, and 96Tc can be considered negligible as long as the product meets radionuclidic purity specifications based on dosimetry considerations or product shelf-life, whichever is shorter.
The production of 99mTc with cyclotrons is a reiterated idea (14) that received little attention before the ongoing supply of inexpensive and readily available 99mTc from 99Mo generators became uncertain. In recent years, several groups, including our consortium, developed new targets and robust separation procedures to manufacture high-purity 99mTc with cyclotrons (7,15–20). There is increasingly convincing evidence that the quality of cyclotron-produced 99mTc is comparable to that of conventional 99mTc (6,7,21,22,23) and that sufficient quantities can be made to satisfy the demand of large urban communities (3).
The present clinical trial confirmed that cyclotron-produced 99mTc-pertechnetate provides clinical safety and diagnostic efficacy equivalent to those of the conventional radiopharmaceutical. Whether cyclotron-produced 99mTc will reach the status of an approved radiopharmaceutical or be forgotten again remains to be seen. Although the cost of its commercialization (infrastructure and marketing authorization) may be orders of magnitude lower than that of nuclear reactor–based production of 99mTc, it is still significant and will require commitment from governments and investors. Economic factors, including the implementation of full-cost recovery models for 99Mo/99mTc production (2), will be a decisive point in this almost 50-y-old story.
CONCLUSION
We showed that 99mTc produced with a cyclotron at medium energy can be safely used for humans and yields clinical images that are fully satisfactory for diagnostic procedures. The results of the present study provide further supporting evidence for the adoption of cyclotron-produced 99mTc-pertechnetate in clinical practice.
DISCLOSURE
This work was supported by Natural Resources Canada through the Isotope Technology Acceleration Program (ITAP) and by the Medical Imaging Trial Network of Canada (MITNEC). The Research Center of CHUS (CRCHUS) is supported by the Fonds de Recherche du Québec–Santé (FRQS). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We gratefully acknowledge Jim Garrett, Laboratory of Materials Preparation and Characterization, Brockhouse Institute for Materials Research, McMaster University, for preparing 100Mo targets. We thank cyclotron operators Eric Berthelette and Paul Thibault for excellent technical help and continuing availability for this research project and Otman Sarrhini for phantom image analysis. We acknowledge our ITAP partners, University of Alberta and Advanced Cyclotron Systems Inc.
Footnotes
Published online Oct. 13, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 9, 2016.
- Accepted for publication September 13, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.