


Abstract
We compared the contributions of the labeled tracers 11C-methionine (Met) and 18F-FDG for PET-guided stereotactic biopsy of brain gliomas. Methods: In 32 patients with glioma, stereotactic Met PET and 18F-FDG PET were integrated in the planning of stereotactic brain biopsy. PET images were analyzed to determine which tracer offered the best information for target definition. The stereotactic coregistration of PET images allowed accurate comparison of the level, distribution, and extent of uptake for both tracers according to tumor location and grade. Results: A histologic diagnosis was obtained for all patients. All gliomas had an area of abnormal Met uptake, and 27 showed abnormal 18F-FDG uptake. 18F-FDG was used for target selection when its uptake was higher in tumor than in gray matter (14 gliomas). Seven were in the basal ganglia or brain stem. Met was used for target selection when there was no 18F-FDG uptake or when 18F-FDG uptake was equivalent to that in the gray matter (18 gliomas). Thirteen were in the cortex. Sixty-one of the 70 stereotactic trajectories obtained from the 32 patients were based on PET-defined targets and had an area of abnormal Met uptake. These 61 Met-positive trajectories always yielded a diagnosis of tumor. All nondiagnostic trajectories (n = 9) were obtained in areas with no increased uptake of Met. In all patients with increased uptake of both tracers, the focus of highest Met uptake corresponded to the focus of highest 18F-FDG uptake. However, the extent of uptake of both tracers was variable. Conclusion: Distributions of highest Met and 18F-FDG uptake are similar in brain gliomas. Because Met provides a more sensitive signal, it is the molecule of choice for single-tracer PET-guided neurosurgical procedures in gliomas.
Because brain tumors are histologically heterogeneous, CT- or MRI-guided stereotactic brain biopsy does not always yield a valid diagnosis or grading (1–5). PET provides useful, independent, and complementary metabolic information on brain tumors (5–8). We previously described a technique allowing the routine integration of PET data in the planning of stereotactic brain biopsy (9–12). We originally used 18F-FDG as the unique radiotracer because of the large core of information on the use of this tracer in neurooncology. The selection of targets on stereotactic PET images with 18F-FDG allows biopsies to be directed accurately toward the hypermetabolic foci of brain tumors (9,10). We have shown that 18F-FDG PET-guided stereotactic brain biopsy increases the diagnostic yield and accuracy of the technique (9–11,13).
Still, experience with 18F-FDG PET-guided biopsy has shown some limitations. Indeed, targeting may be difficult when there is no or minor 18F-FDG uptake, such as in low-grade tumors (14). Also, when a hypermetabolic lesion is near the cortical or subcortical gray matter, tumor 18F-FDG uptake and normal 18F-FDG uptake are difficult to differentiate (14–15). Therefore, we tested 11C-methionine (Met) as an alternative tracer for stereotactic PET guidance. The use of Met, a marker of amino acid uptake and protein synthesis, has also been validated in neurooncology (14,16–22). This PET tracer has several advantages: It is considered efficient and more suitable than 18F-FDG for delineating areas of tumor tissue (18,19,23,24); its uptake has been shown to be increased in low-grade glial tumors (15,17,18,24,25); its uptake is low in gray matter; and its biologic behavior in neoplastic tissues shows that its accumulation represents active transport of amino acids.
As a first step toward the use of PET with Met (Met PET) in stereotactic conditions, we previously used combined 18F-FDG and Met PET guidance for stereotactic brain biopsy (26). The aim of the present study was to compare the distribution, extent, and relative contributions of Met and 18F-FDG in a series of glioma patients who underwent PET-guided stereotactic brain biopsy with both tracers.
MATERIALS AND METHODS
Patient Selection
Since June 1991, we have routinely performed PET-guided stereotactic brain biopsy on patients suspected, on the basis of a preoperative neuroimaging work-up, of having a nonresectable brain tumor. Our current series comprised more than 250 patients. Between July 1992 and June 1997, 45 consecutive patients underwent biopsy guided by combined 18F-FDG PET and Met PET performed under stereotactic conditions. The double-tracer procedure was proposed for those patients because they presented with a tumor considered unresectable and located in the cortical or subcortical gray matter (including the basal ganglia and the brain stem). Thirty-two of the patients had a diagnosis of glioma. They were 20 men and 12 women whose ages ranged from 2 to 85 y (mean, 52.6 y). All patients were previously untreated.
Stereotactic PET Data Acquisition
For data acquisition, the technique of combined stereotactic PET with Met and 18F-FDG was adapted from our previous experience with 18F-FDG PET-guided stereotactic brain biopsy (9–11). Placement of the stereotactic frame; data acquisition, including stereotactic PET with Met and 18F-FDG, and CT or MRI; surgical planning; and biopsy were performed on the same day. All patients gave informed consent, and the procedure met the ethical guidelines of our institution.
After placement of the CT- and MRI-compatible base ring (Fischer ZD-Neurosurgical Localizing Unit; Howmedica Leibinger), stereotactic CT or MRI without and with intravenous contrast enhancement was performed. For stereotactic PET, a clamp specifically designed to secure the head ring to the Siemens couch (Howmedica Leibinger) was used. To create a fiducial reference system compatible with PET, we used the commercial MRI localizers with minor modifications as previously described (9–10). After the transmission scan, the patient first received an intravenous injection of 370–555 MBq of Met. Met PET images used for stereotactic calculation were acquired between 20 and 40 min after injection of the tracer. Eighty minutes after Met injection, the patient was injected with 74–185 MBq of 18F-FDG (specific activity > 74 Bq/μmol). 18F-FDG PET images used for stereotactic calculation were acquired between 40 and 60 min later. The PET camera (933/08/12 tomograph; CTI/Siemens) allowed simultaneous 2-dimensional acquisition of 15 slices about 6.5 mm thick, with a resolution of about 5 mm in full width at half maximum.
Analysis of Stereotactic PET Images and Target Definition
The surgical planning began with analysis of the PET images. Because this series represented an evaluation of Met PET, we always started with an independent analysis of 18F-FDG PET images based on our previous experience (9–11). Met PET images were analyzed afterward. Areas of abnormal metabolism used for target selection were either zones of 18F-FDG or Met uptake that were higher than the surrounding normal-appearing brain tissue or foci of relatively increased 18F-FDG or Met uptake in a hypometabolic lesion. 18F-FDG was used for target selection when its uptake in the tumor was higher than, or distinguishable from, the gray matter. To be considered distinguishable from the gray matter, 18F-FDG uptake needed to be outside normally located or displaced gray matter. This was evaluated on coregistered PET and MR images. Met was used for target selection when there was no 18F-FDG uptake or when 18F-FDG uptake was attributable to metabolic activity in gray matter. If the PET images revealed areas of abnormally increased tracer uptake within the area of the lesion, the plane that best displayed the abnormal 18F-FDG or Met uptake was selected. On visual inspection, the surgeon interactively pointed at a pixel in the center of this zone, and its calculated coordinates set a target for biopsy. Because, in all cases, the biopsy was planned to establish a histologic diagnosis and not to define the extension of the lesion, all PET-defined targets were maintained within the boundaries of the lesion on CT or MRI. When a target was selected on 18F-FDG PET, it was then projected onto the corresponding Met PET slice to analyze and compare the local uptake of both tracers. The targets were also projected onto the corresponding stereotactic CT or MRI slice to control the reliability and safety of the target selection and trajectory.
Whenever possible, 2 targets sampling different metabolic areas of the tumor were selected for biopsy. When the area of highest 18F-FDG uptake was smaller than the limits of the lesion visualized on the corresponding slice of Met PET, another target was selected on the Met PET image, outside the area of increased 18F-FDG uptake. In patients with no obvious abnormal 18F-FDG or Met uptake that could be used to select a target for biopsy, surgery was planned using CT or MRI data only.
Data Analysis
In all patients, serial stereotactic biopsies were performed along each trajectory, following the technique described by Kelly et al. (27). For all biopsy specimens, smear preparation and formalin-fixed samples were analyzed after appropriate staining (9–11,28,29). Gliomas were classified using a 3-tier system: low-grade glioma (LGG), including astrocytoma, oligodendroglioma, giant cell astrocytoma, and gangliocytoma; anaplastic astrocytoma (AA); and glioblastoma (GB).
For each patient, a histologic diagnosis was established. Then, the pathologic description obtained for each biopsy trajectory was recorded separately, regardless of the patient’s final diagnosis. If nontumor samples made of gliotic, inflammatory, or necrotic tissue were found, they were classified as nondiagnostic trajectories.
In order to evaluate the role of Met PET in target selection, we retrospectively classified biopsy trajectories in 3 groups, according to their metabolic characteristics: 18F-FDG PET-guided trajectory, Met PET-guided trajectory, and CT/MRI-guided trajectory. For that purpose and because we found that all areas of increased 18F-FDG uptake were within areas of increased Met uptake, we first looked at whether areas of increased Met uptake were present [Met(+)] or absent [Met(−)]. In Met(+) trajectories, we further looked at whether 18F-FDG PET was used for the target selection. Indeed, as already described, 18F-FDG PET images were used first for target selection (18F-FDG PET-guided trajectory). When 18F-FDG PET did not provide information considered valid for target selection, Met PET was used (Met PET-guided trajectory). In Met(−) trajectories, target selection was based on CT or MRI only (CT/MRI-guided trajectory).
RESULTS
A total of 70 stereotactic biopsy trajectories were performed on the 32 patients (2.2 trajectories per patient). A histologic diagnosis was obtained for all patients. The diagnoses included 10 GBs, 12 AAs, and 10 LGGs (6 astrocytomas, 2 oligodendrogliomas, 1 giant cell astrocytoma, and 1 gangliocytoma).
In all cases, a PET-defined target could be set using either the 18F-FDG data or the Met data (Table 1). All gliomas had an area of abnormal Met uptake, and 27 showed abnormal 18F-FDG uptake. When 18F-FDG uptake was higher in tumor than in gray matter (n = 14), that tracer was used for target selection. This occurred in 7 GBs, 6 AAs, and 1 LGG. Met was the tracer used to define a biopsy target for the other 18 tumors (56%). These corresponded to 9 high-grade tumors and 9 LGGs.
Target Definition in 32 PET-Guided Stereotactic Biopsy Procedures
Twenty of the 32 gliomas involved the cortical area, and Met was used for target selection for 13 of them (65%) (Table 2; Figs. 1 and 2). The 13 cortical gliomas targeted on Met PET included 4 that were not enhanced on CT or MRI (3 LGGs and 1 AA). The other 12 gliomas involved either the basal ganglia (n = 10) or the brain stem (n = 2) (Table 3; Figs. 3 and 4). In 7 of these 12 gliomas (58%), 18F-FDG was used for target selection. However, in 1 GB (patient 10), a second trajectory was performed in an area of high Met uptake outside the limits of high 18F-FDG uptake and yielded similar tumor tissue.
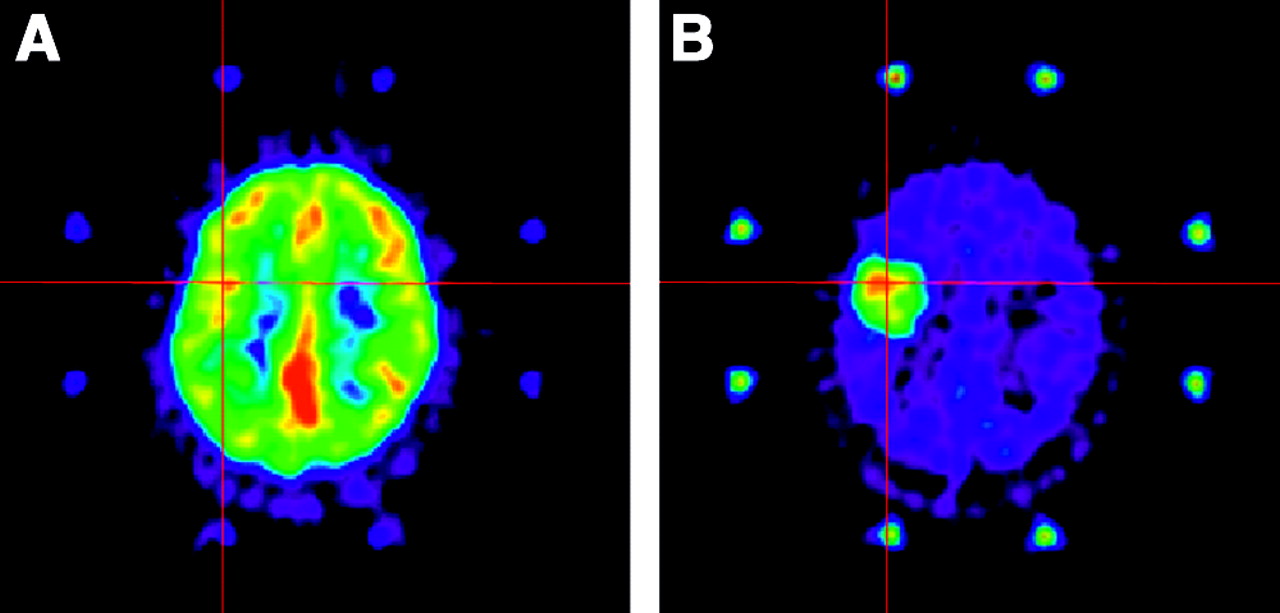
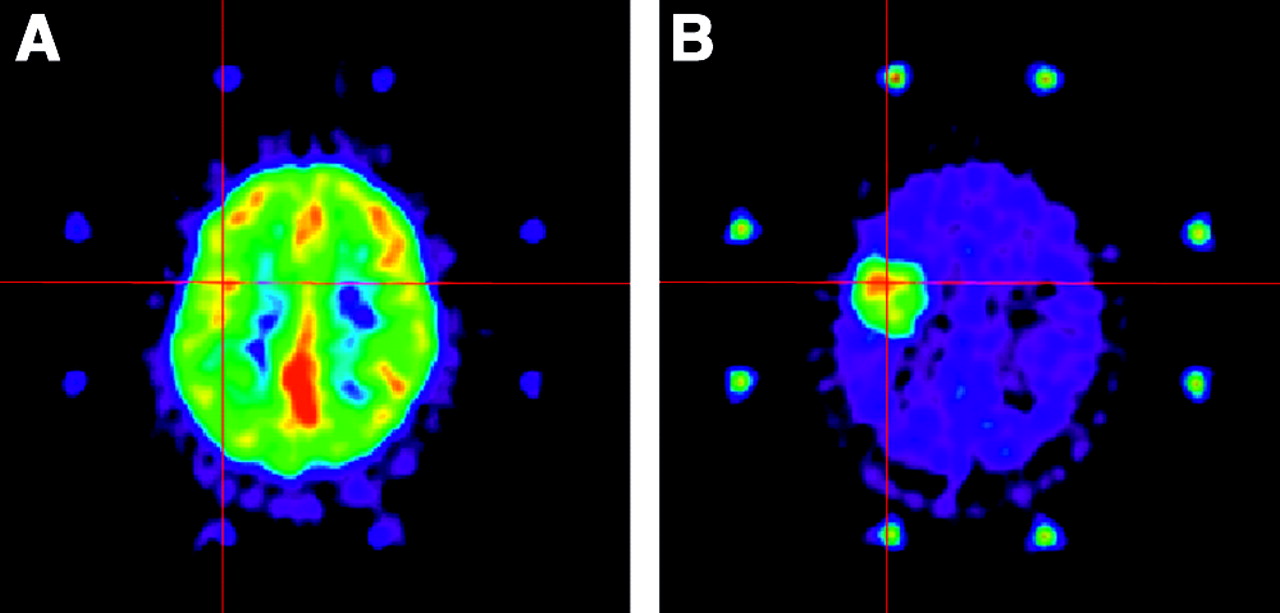
PET performed with 18F-FDG (A) and Met (B) on a 32-y-old man with an AA in the left frontorolandic cortical area. Uptake of 18F-FDG in tumor was equivalent to that in cortical gray matter. Uptake of Met was higher in tumor than in cortex, allowing definition of a target for biopsy. When PET images obtained with the 2 tracers were coregistered, the focus of highest Met uptake corresponded to the unique focus of 18F-FDG uptake within the tumor (crosses).
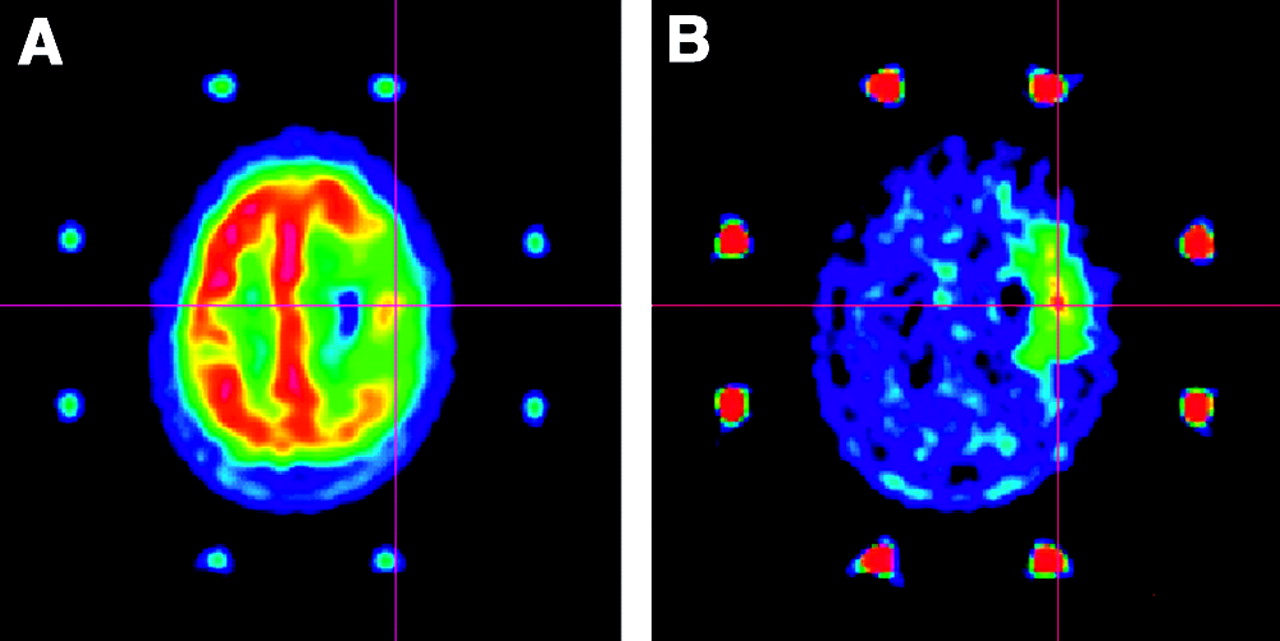
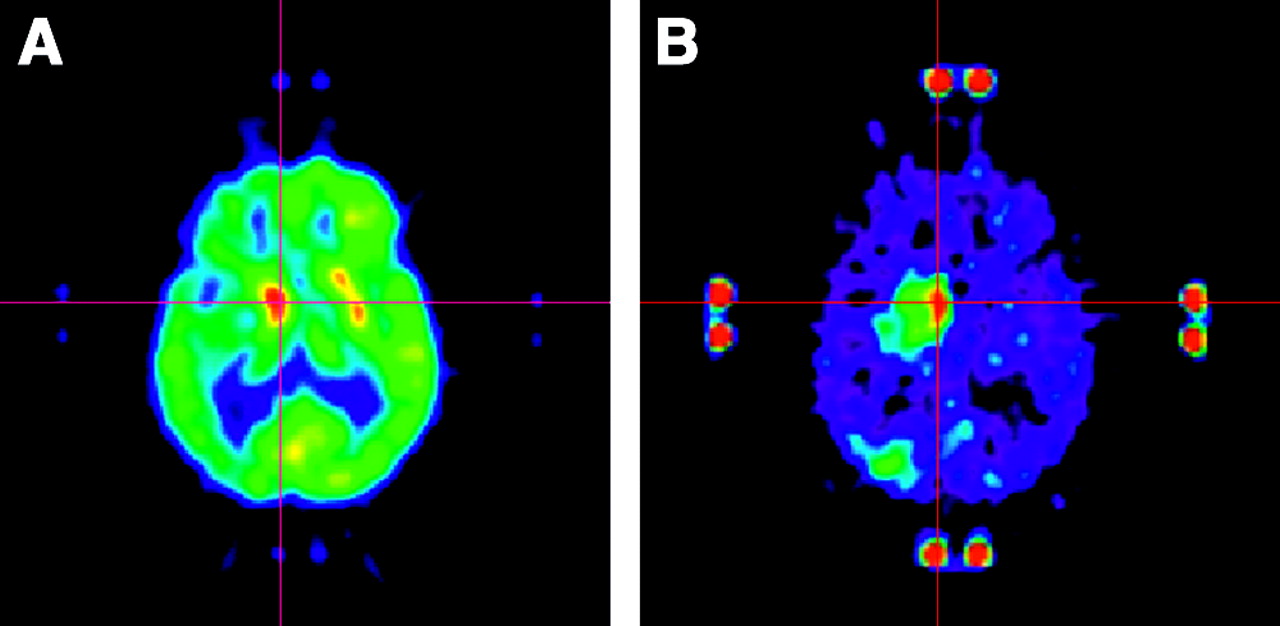
PET performed with 18F-FDG (A) and Met (B) on a 62-y-old woman with a GB in the right prerolandic cortical area. Uptake of 18F-FDG was reduced in the tumor area except for 1 spot of uptake equivalent to that in the surrounding gray matter. Uptake of Met was higher in tumor than in cortex, allowing definition of a target for biopsy. When PET images obtained with the 2 tracers were coregistered, the highest focus of Met uptake corresponded to the hot spot of 18F-FDG (crosses).
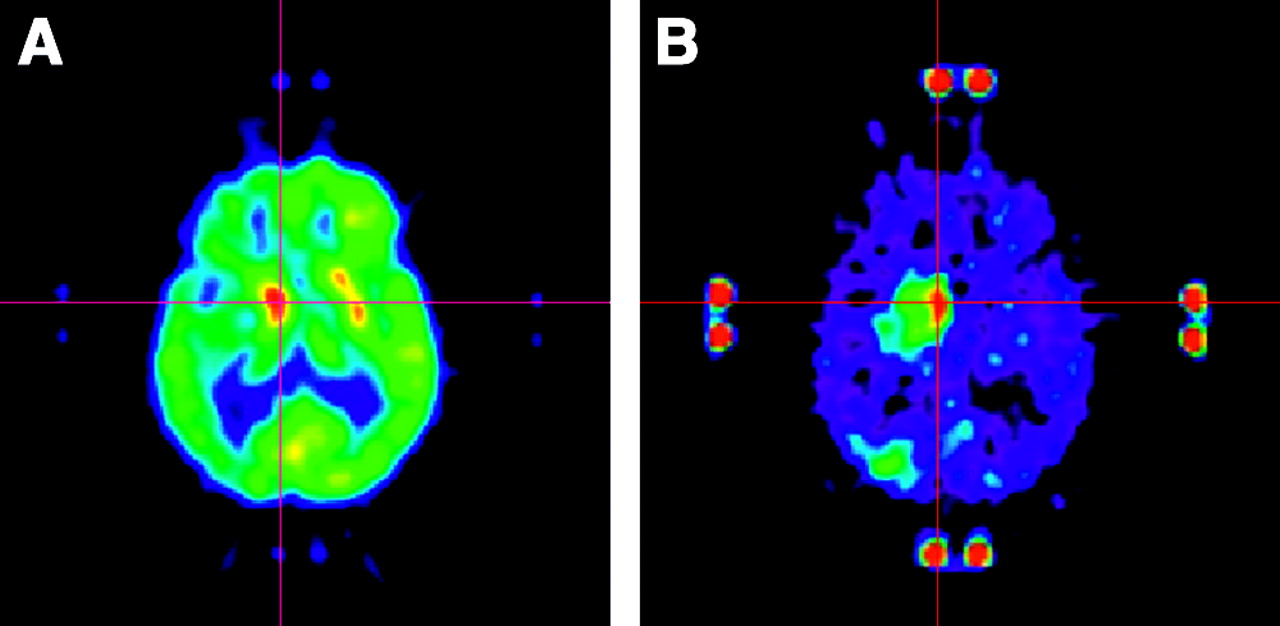
PET performed with 18F-FDG (A) and Met (B) on a 74-y-old man with a GB in the right basal ganglia. Uptake of 18F-FDG was higher in tumor than in surrounding gray matter and allowed definition of a target for biopsy. Uptake of Met was also higher in tumor than in surrounding gray matter, and zones of highest uptake of both tracers corresponded on coregistered images (crosses).
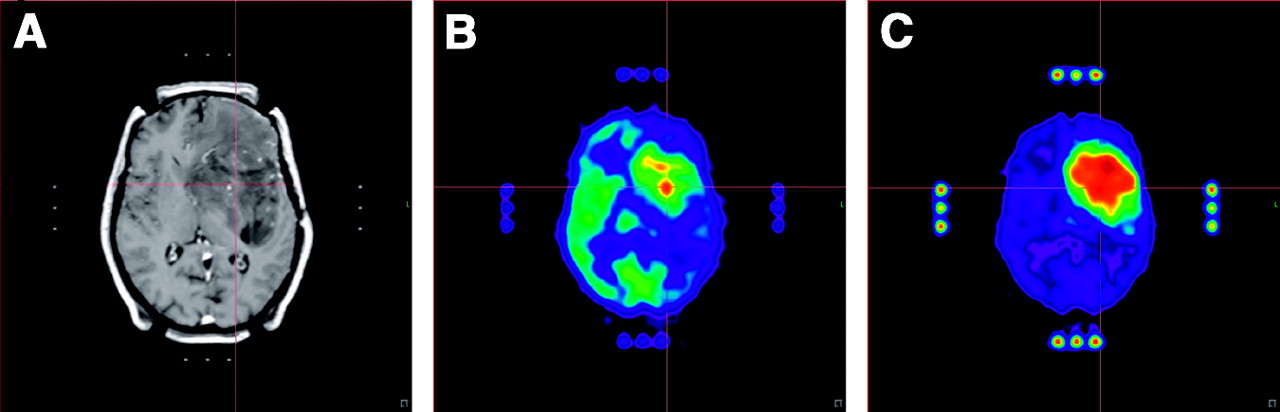
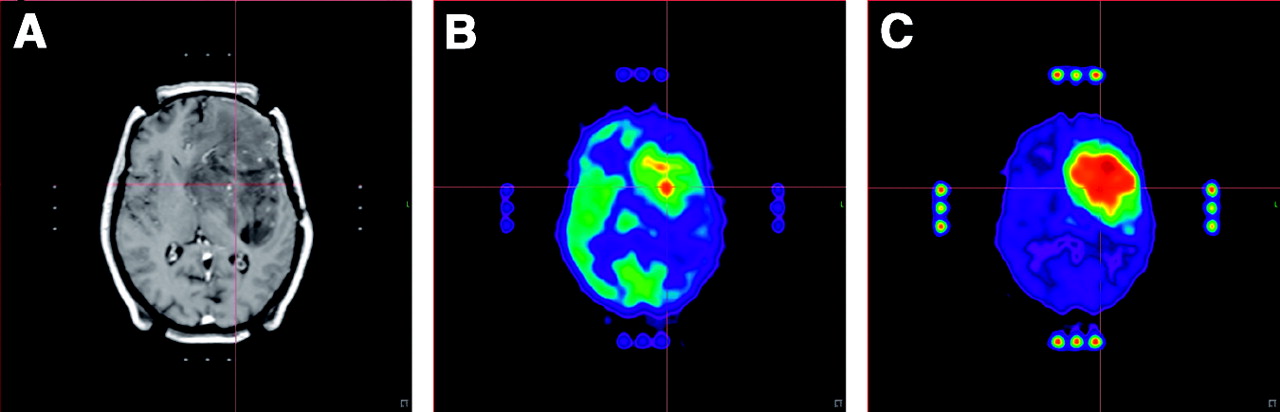
MRI (A) and PET performed with 18F-FDG (B) and Met (C) on a 57-y-old woman with an infiltrating AA in the left basal ganglia and subcortical frontal region. Uptake of 18F-FDG was higher in tumor than in surrounding gray matter and allowed definition of a target for biopsy. Uptake of Met was also higher in tumor than in surrounding gray matter. Coregistration of PET images showed that Met uptake was more extended than 18F-FDG uptake but that zones of highest uptake corresponded (crosses).
Target Definition in 20 Gliomas in Cortex
Target Definition in 12 Gliomas in Basal Ganglia or Brain Stem
Table 4 analyses the diagnostic yield of the 70 stereotactic trajectories performed on the 32 patients according to their Met uptake. Sixty-one trajectories corresponded to an area of increased Met uptake. The other 9 trajectories showed no abnormal Met uptake, and biopsy was based on CT- or MRI-defined targets. All 61 Met(+) trajectories yielded tumor tissue, whereas the 9 Met(−) trajectories yielded nontumor tissue and were nondiagnostic. In 22 trajectories, 18F-FDG uptake was higher in the tumor than in the gray matter. This group included 11 GB, 10 AA, and 1 LGG samples. The targets used to define these trajectories were all CT or MRI enhanced. Thirteen (59%) were in the basal ganglia or the brain stem. In 22 other trajectories, tumor 18F-FDG uptake was equivalent to that of the gray matter. This group included 7 GB, 9 AA, and 6 LGG samples. Sixteen targets corresponded to enhanced areas on CT or MRI and 6 to unenhanced areas. Finally, 17 trajectories had very low or no tumor 18F-FDG uptake and were guided on Met PET. They included 3 AA and 15 LGG samples. All hypodense or hyposignal targets on CT or MRI were in this group. Thus, Met was used efficiently to define the biopsy target for 39 of the 61 trajectories (64%).
Diagnostic Yield and 18F-FDG/11C-Methionine Uptake of 70 Biopsy Trajectories
All Met(−) nondiagnostic trajectories occurred in patients for whom the diagnosis was obtained from another trajectory that presented increased Met uptake. These diagnoses included 2 GBs, 3 AAs, and 4 LGGs. Among them, 5 were targets with no contrast enhancement on MRI. One showed discrete but significant enhancement on MRI.
This study also allowed us to correlate the 18F-FDG- and Met PET images stereotactically and to compare the tumor level, extent, and distribution of the 2 tracers. Of the 14 gliomas in which uptake of both tracers was higher than in surrounding gray matter, Met uptake was more extended than 18F-FDG uptake in 10 (Fig. 4) and equally extended in 4. In all cases, the focus of highest Met uptake corresponded to the focus of highest 18F-FDG uptake (Figs. 3 and 4). When tumor 18F-FDG uptake was equivalent to 18F-FDG uptake in the surrounding gray matter (13 gliomas), the projection of the highest Met uptake on 18F-FDG PET images corresponded to an individualized focus of highest 18F-FDG uptake within the gray matter in 5 of 8 high-grade gliomas. Still, on the 18F-FDG scans, these foci were not differentiated from the rest of the gray matter (Figs. 1 and 2). For the 5 LGGs in which 18F-FDG uptake was equivalent to that in surrounding gray matter, the areas of highest uptake of Met and 18F-FDG never matched.
DISCUSSION
Brain tumors, especially gliomas, are characterized by regional variations of histologic malignancy (24,30) that cannot be distinguished on conventional anatomic imaging such as MRI even with contrast injection (31). Therefore CT- or MRI-guided stereotactic brain biopsy does not always yield valid diagnosis or grading, since target selection may lead to a significant sampling error and secondary understaging (1–5).
PET provides independent and complementary metabolic information on brain tumors (5–8). The literature has collected numerous data on PET of brain tumors, mainly with the tracer 18F-FDG. When combined with anatomic imaging techniques, 18F-FDG PET can provide information on tumor grading (11,32,33), response to therapy (34), and prognosis (35,36). In particular, early clinical studies have demonstrated that the glycolytic rate of brain tumors, as assessed by 18F-FDG uptake, is a more accurate reflection of tumor grade than is contrast enhancement (31).
To take advantage of these metabolic data in the management of brain tumors, we previously developed a technique allowing the routine integration of PET data in the planning of stereotactic brain biopsy (9,10). We originally used 18F-FDG because it was the most widely used radiotracer for brain tumors (24). The selection of targets on stereotactic 18F-FDG PET-generated images allows biopsies to accurately be directed toward the abnormal metabolic foci of brain tumors (9,10). We have shown that 18F-FDG PET-guided stereotactic brain biopsy increases the diagnostic yield and accuracy of the technique (11–13). Moreover, PET-guided stereotactic brain biopsy has allowed accurate correlation of metabolism and histology and confirmation of the correlation between PET tracer uptake and tumor grade (21). Indeed, with this method we have found a significant relationship between 18F-FDG uptake, as well as Met uptake, and the presence of anaplasia (29,30).
Our results confirm our preliminary data showing that Met may be a good alternative to 18F-FDG for target selection in PET-guided stereotactic brain biopsy (26).
With Met PET guidance, a histologic diagnosis was obtained for all patients. The 9 nondiagnostic samples were exclusively from trajectories defined on CT or MRI in areas with no Met uptake. Because CT or MRI findings were abnormal in those areas, one cannot rule out the possibility that biopsy guidance limited to CT/MRI data in those 9 patients would have led to the final diagnosis. This high diagnostic value of Met PET is also illustrated by the fact that, in this series of patients, all gliomas presented as an area of increased Met uptake.
Our experience with both tracers, acquired and compared under stereotactic conditions, shows that, in 18 of the 32 gliomas, all of which were in gray matter, Met was the only tracer that could safely be used for target selection. This was the case for AAs and GBs in which tumor 18F-FDG uptake and normal 18F-FDG uptake were difficult to differentiate, as well as for LGGs in which there was no 18F-FDG uptake. Indeed, in 9 LGGs, the highest focus of Met uptake was used for target definition. One could argue that Met uptake in LGG is not a constant finding (18,35). However, the chance of finding abnormally increased uptake of radiotracer remains higher with Met than with 18F-FDG (32,33,37).
When located in the cortex, most high-grade gliomas (14/20) limited the ability of 18F-FDG PET to define a target. Met is therefore superior to 18F-FDG for target selection in enhanced or unenhanced gliomas in the cortex. When the glioma was in subcortical gray matter, 18F-FDG was more frequently useful for target selection: In 7 of 12 cases 18F-FDG was useful, whereas in the other 5 only Met showed abnormal uptake. All stereotactic biopsies performed on brain stem gliomas yielded a diagnosis of tumor, as anticipated by a high uptake of Met. This further confirms that the integration of stereotactic PET, especially with Met, should allow an increase in diagnostic yield while reducing the number of trajectories in highly functional brain areas (13).
Because Met uptake was increased in all gliomas, whatever the grade, one could argue that Met PET was not discriminating enough to direct the biopsy to the most malignant area of the tumor, as allowed by 18F-FDG PET (11). With stereotactic coregistration, however, we found that the area of highest Met uptake and the area of highest 18F-FDG uptake usually corresponded. This observation confirms the findings of our previous study of Met and 18F-FDG uptake in biopsy samples. That study demonstrated a significant correlation between the uptake of both tracers and the degree of anaplasia (33).
Because Met provides better information than 18F-FDG on tumor extent, Met has already gained a place, in combination with MRI, in the neurosurgical strategies aimed at delineating the entire tumor volume, either for resection under neuronavigation or for radiosurgery (38–40). In this series, Met has also appeared suitable for “within-tumor” biopsy planning. Further tests should be conducted with 18F-labeled amino acids to make the method accessible in centers not able to produce tracers in-house (23).
CONCLUSION
The results of the current retrospective analysis confirm that Met can be used accurately as a radiotracer for routine image-guided neurosurgery of brain gliomas. Compared with 18F-FDG, Met offers an equivalent possibility of target selection in areas of highest metabolic activity. The higher sensitivity of Met makes it the best choice for single-tracer PET-guided stereotactic brain biopsy.
Footnotes
Received Nov. 29, 2003; revision accepted Feb. 11, 2004.
For correspondence or reprints contact: Benoit Pirotte, MD, Department of Neurosurgery, Erasme Hospital, Université Libre de Bruxelles, 808, Route de Lennik, 1070 Brussels, Belgium.
E-mail: bpirotte{at}ulb.ac.be
REFERENCES





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Extent and Instability of Trimethylation of Histone H3 Lysine Increases With Degree of Malignancy and Methionine Addiction
- Metabolic Phenotypes, Dependencies, and Adaptation in Lung Cancer
- The linkage of methionine addiction, overmethylation of histone H3 lysines and malignancy demonstrated when cancer cells revert to methionine-independence
- Chronic Treatment of an Advanced Prostate-cancer Patient With Oral Methioninase Resulted in Long-term Stabilization of Rapidly Rising PSA Levels
- Lowering and Stabilizing PSA Levels in Advanced-prostate Cancer Patients With Oral Methioninase
- Histone H3K4me3 and H3K9me3 are super over-methylated in soft tissue sarcoma compared to normal muscle in patient-derived xenograft (PDX) mouse models: an indicator of cancer methionine addiction
- Differentiation between Treatment-Induced Necrosis and Recurrent Tumors in Patients with Metastatic Brain Tumors: Comparison among 11C-Methionine-PET, FDG-PET, MR Permeability Imaging, and MRI-ADC--Preliminary Results
- Molecular Imaging to Plan Radiotherapy and Evaluate Its Efficacy
- Imaging Intratumor Heterogeneity: Role in Therapy Response, Resistance, and Clinical Outcome
- Clinical Impact of Amino Acid PET in Gliomas
- Correlation of 18F-FLT Uptake with Tumor Grade and Ki-67 Immunohistochemistry in Patients with Newly Diagnosed and Recurrent Gliomas
- Clinical applications of imaging biomarkers. Part 2. The neurosurgeon's perspective
- Multimodality Assessment of Brain Tumors and Tumor Recurrence
- Voxel-Based Analysis of Dual-Time-Point 18F-FDG PET Images for Brain Tumor Identification and Delineation
- Evaluation of 18F-FDG PET and MRI Associations in Pediatric Diffuse Intrinsic Brain Stem Glioma: A Report from the Pediatric Brain Tumor Consortium
- Quantitative, Preclinical PET of Translocator Protein Expression in Glioma Using 18F-N-Fluoroacetyl-N-(2,5-Dimethoxybenzyl)-2-Phenoxyaniline
- 1-11C-Acetate Versus 18F-FDG PET in Detection of Meningioma and Monitoring the Effect of {gamma}-Knife Radiosurgery
- Evaluation of Focal Cortical Dysplasia and Mixed Neuronal and Glial Tumors in Pediatric Epilepsy Patients Using 18F-FDG and 11C-Methionine PET
- Tumor Cell Metabolism Imaging
- Evaluation of Primary Brain Tumors Using 11C-Methionine PET with Reference to a Normal Methionine Uptake Map
- Clinical Applications of PET in Brain Tumors