


Abstract
Alzheimer disease (AD) is associated with an increase in the brain of the 18-kDa translocator protein (TSPO), which is overexpressed in activated microglia and reactive astrocytes. Measuring the density of TSPO with PET typically requires absolute quantitation with arterial blood sampling, because a reference region devoid of TSPO does not exist in the brain. We sought to determine whether a simple ratio method could substitute for absolute quantitation of binding with 11C-PBR28, a second-generation radioligand for TSPO. Methods: 11C-PBR28 PET imaging was performed in 21 healthy controls, 11 individuals with mild cognitive impairment, and 25 AD patients. Group differences in 11C-PBR28 binding were compared using 2 methods. The first was the gold standard method of calculating total distribution volume (VT), using the 2-tissue-compartment model with the arterial input function, corrected for plasma-free fraction of radiotracer (fP). The second method used a ratio of brain uptake in target regions to that in cerebellum—that is, standardized uptake value ratio (SUVR). Results: Using absolute quantitation, we confirmed that TSPO binding (VT/fP) was greater in AD patients than in healthy controls in expected temporoparietal regions and was not significantly different among the 3 groups in the cerebellum. When the cerebellum was used as a pseudo-reference region, the SUVR method detected greater binding in AD patients than controls in the same regions as absolute quantification and in 1 additional region, suggesting SUVR may have greater sensitivity. Coefficients of variation of SUVR measurements were about two-thirds lower than those of absolute quantification, and the resulting statistical significance was much higher for SUVR when comparing AD and healthy controls (e.g., P < 0.0005 for SUVR vs. P = 0.023 for VT/fP in combined middle and inferior temporal cortex). Conclusion: To measure TSPO density in AD patients and control subjects, a simple ratio method SUVR can substitute for, and may even be more sensitive than, absolute quantitation. The SUVR method is expected to improve subject tolerability by allowing shorter scanning time and not requiring arterial catheterization. In addition, this ratio method allows smaller sample sizes for comparable statistical significance because of the relatively low variability of the ratio values.
Alzheimer disease (AD) is associated with neuroinflammation characterized by activated microglia and reactive astrocytes. Because these reactive neuroimmune cells overexpress the 18-kDa translocator protein (TSPO), TSPO density has been used as a biomarker for neuroinflammation in AD and other neurologic diseases (1). We recently found that TSPO binding was greater in AD patients than in age-matched controls or patients with mild cognitive impairment (MCI) who had a positive amyloid scan result (2). That is, increased TSPO binding appeared to mark, and might play a pathophysiologic role in, the transition from MCI to AD.
A major barrier to expanding studies that use TSPO imaging to assess the potential role of inflammation in AD is that PET measurements of TSPO density typically require absolute quantitation relative to the concentration of radioligand in arterial blood. This measurement of plasma concentrations adds error to the final values, requires significant equipment and expertise, and entails arterial catheterization of the subject. A relative method of measurement (e.g., one brain region compared with another) would be expected to have smaller variability than an absolute value, in part because of cancellation of global scale changes or errors in measurement of plasma concentrations. However, relative measurement requires either a reference or a pseudo-reference region. Unfortunately, a true reference region (i.e., devoid of TSPO) does not exist in the brain, because TSPO is present in gray matter, white matter, vessel walls, and even choroid plexus (3,4). A pseudo-reference region would contain TSPO but not differ between comparison groups. Such a region could, for example, be used to compare the ratio of target to pseudo-reference region in patients versus controls. However, this approach requires that prior studies using absolute quantitation confirmed that the pseudo-reference region does not significantly differ between patients and controls. To date, no study has identified or proved that a pseudo-reference region exists for second-generation TSPO imaging in AD, including white matter.
Using absolute quantitation, we previously found that TSPO binding in the cerebellum, measured with 11C-PBR28, did not differ between AD patients and either healthy controls (HCs) or MCI subjects (2). This finding is consistent with the cerebellum of AD patients being relatively spared of pathology, including inflammation (5–7), and suggests that the cerebellum could be used as a pseudo-reference region as an alternative to absolute quantification.
This study sought to determine whether the method of absolute quantitation that requires arterial blood sampling could be substituted with a simple method that uses only the ratio of brain radioactivity in a target region compared with that in the cerebellum. We recruited 15 more subjects than in our previous report (2) and then measured TSPO binding in 25 AD patients, 21 HCs, and 11 patients with MCI. We compared 2 methods of analysis, absolute quantitation of receptor binding, which requires an arterial input function, and relative quantitation of receptor binding, which requires only PET images and was calculated as the ratio of brain uptake in target regions compared with that in the cerebellum (i.e., standardized uptake value ratio [SUVR]).
MATERIALS AND METHODS
Subjects
Subjects included 21 HCs (15 men and 6 women; mean age ± SD, 55.1 ± 15.3 y), 11 MCI patients (7 men and 4 women; mean age ± SD, 72.2 ± 9.3 y), and 25 AD patients (11 men and 14 women; mean age ± SD, 63.0 ± 8.3 y). All patients were amyloid-positive on PET imaging with 11C-Pittsburgh compound B (11C-PIB) based on criteria used in our earlier study (2). AD patients met updated criteria for probable AD dementia with evidence of AD pathophysiologic process (8), and MCI patients met updated criteria for MCI due to high or intermediate likelihood of developing AD (9). Some subjects were included in our previously published study (2). Binding affinity status (high, mixed, or low) was determined using leukocyte binding assay as previously described (2,10), and low-affinity binders were excluded from the study. There were 7 high-affinity binders (HABs) and 14 middle-affinity binders (MABs) among HCs, 5 HABs and 6 MABs among MCI patients, and 11 HABs and 14 MABs among AD patients. Both radioligand preparation and acquisition and processing of 11C-PBR28 PET and MR images are described in the supplemental materials (available online at http://jnm.snmjournals.org). PET images were not corrected for partial-volume effects (PVEs).
This study was approved by the Combined Neuroscience Institutional Review Board of the National Institutes of Health Intramural Research Program. All subjects or their surrogate provided written informed consent to participate.
Estimation of Binding Values
All kinetic analyses were performed with the PKIN module in PMOD 3.1 (PMOD Technologies Ltd.). The consensus nomenclature of reversible binding radioligands was followed (11).
Metabolite-corrected plasma input function and whole-blood radioactivity were fitted to a triexponential function. The time delay from the radial artery to the brain was calculated with the whole-blood radioactivity curve and whole–gray matter time–activity curve. A model curve was fitted to regional time–activity curves with a metabolite-corrected input function using the 2-tissue-compartment model, as described previously (12). Finally, total distribution volume (VT) was calculated using the rate constants (K1, k2, k3, and k4) estimated from this model and corrected for plasma-free fraction of radioligand (fP).
For a noninvasive measure of 11C-PBR28 binding, we created time-averaged images from 30-min intervals of scan data (10–40, 20–50, 30–60, 40–70, 50–80, and 60–90 min) and converted the measured activity to standardized uptake value (SUV) by multiplying subject body weight and dividing by injected activity. Regional SUVs were measured by overlaying the volume-of-interest mask using the same regions of interest studied in our prior report (2), and regional SUVRs were calculated by dividing the SUV of each region by cerebellar SUV. We sought to determine which time points best provided SUVRs, similar to the determination made for 11C-PIB by Price et al. (13). Unlike 11C-PIB, which shows a stable ratio of radioactivity in the cerebellum to plasma in late time points of the PET scan (13), for 11C-PBR28 this ratio increased until the end of the scan without plateauing. Therefore, to acquire an optimal time interval for SUVR, we performed a linear regression analysis between VT/fP values calculated from the entire 90-min scan and SUVRs calculated from sequential 30-min time intervals of the image data from the combined middle and inferior temporal cortex (Supplemental Fig. 1). Because the best correlation was achieved with data from 60 to 90 min (r = 0.35, P = 0.008), we used 60–90 min as the time interval for obtaining SUVRs for the remainder of the analysis. We also compared group binding using distribution volume ratio (DVR) by dividing the VT of each target region by VT of the cerebellar pseudo-reference region.
Statistical Analysis
SPSS 11.5 (SPSS Inc.) was used for the statistical analysis. Statistical correction for TSPO genotype was performed according to previously published methods (2). For VT/fP, SUVR, and DVR, TSPO genotype was used as a fixed factor to correct for affinity differences caused by the rs6971 single nucleotide polymorphism (SNP). For SUVR, statistical analysis was also performed without TSPO genotype correction. Benjamini-Hochberg’s false-discovery rate with a threshold P value of 0.05 was used to correct for regionwise multiple comparisons (14). Bonferroni adjustment was used for multiple comparisons of each between-group comparison. The variability of binding values was defined as coefficient of variation (%COV) = SD/mean × 100%. For correlative analyses, correlations were first run between the individual outcome measures and TSPO genotype. Standardized residuals were then plotted against each other. To determine whether both VT/fP and SUVRs correlate with clinical severity of AD, we performed correlative analysis with the Clinical Dementia Rating scale – sum-of-boxes scores as independent variables and 11C-PBR28 binding values in combined middle and inferior temporal cortex as dependent variables.
RESULTS
We used the cerebellar gray matter segmented by FreeSurfer (http://surfer.nmr.mgh.harvard.edu) to measure uptake in the pseudo-reference tissue. The mean volume of the cerebellar gray matter of HCs was slightly greater than that of MCI and AD patients (HCs, 96.5 ± 12.0 cm3; MCI, 95.8 ± 9.4 cm3; and AD, 91.3 ± 9.8 cm3). However, no statistically significant difference was observed in cerebellar gray matter volume among the 3 groups, either with or without correction for age.
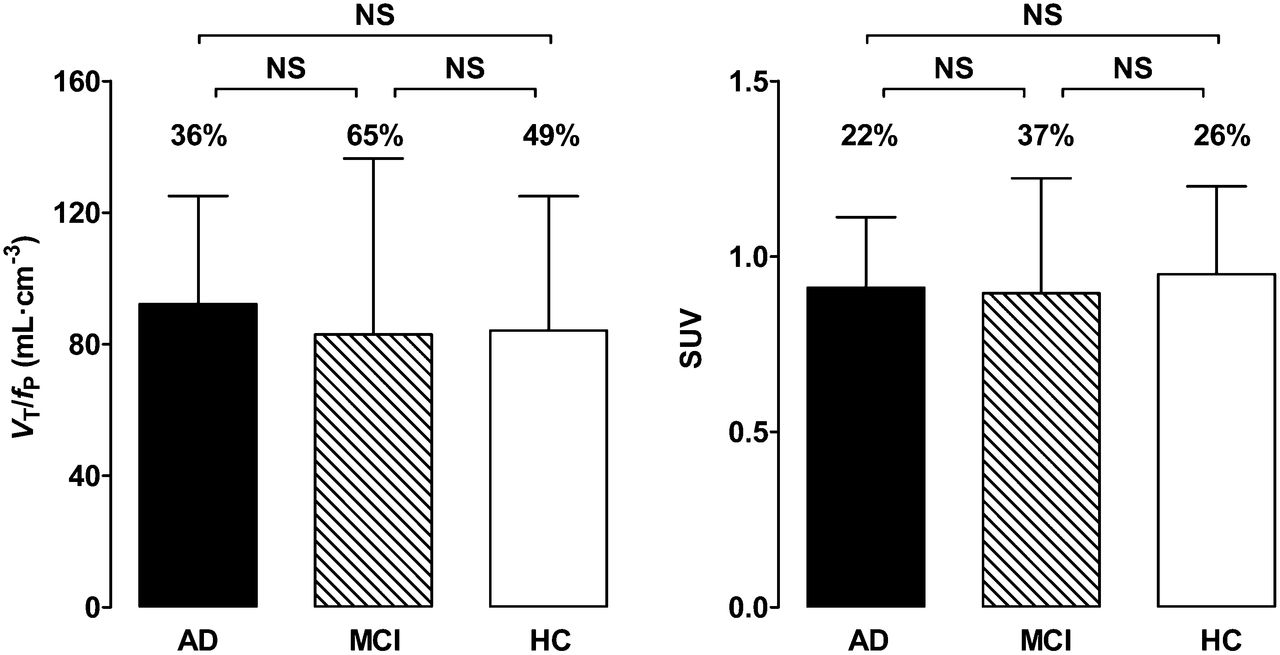
No differences in VT values were observed between the groups (Supplemental Table 1). In contrast, and consistent with results from our earlier study (2), AD patients showed greater VT/fP values than controls in the inferior parietal, combined middle and inferior temporal, and entorhinal cortices (P < 0.05; Table 1; Fig. 1; Supplemental Table 1). AD patients showed greater VT/fP values than MCI patients in the entorhinal and combined middle and inferior temporal cortices. All these regions survived correction for multiple comparisons. Cerebellar VT/fP and SUVs did not differ among controls, MCI patients, and AD patients (P > 0.05; Table 1; Fig. 2).
Effect of Quantification Method on Level of Statistical Significance in Detecting Differences in 11C-PBR28 Binding

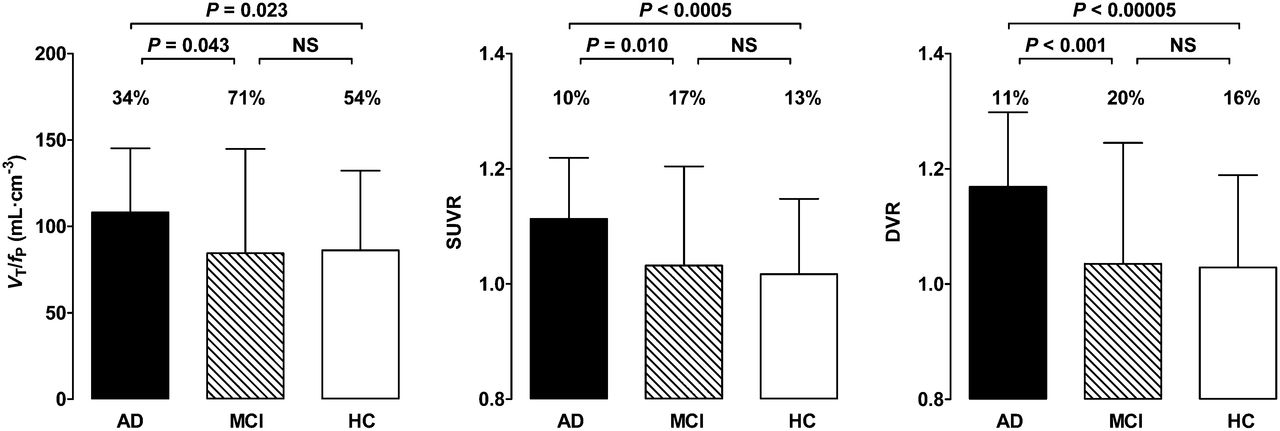
In combined middle and inferior temporal cortex, VT/fP, SUVR, and DVR values were greater for AD patients than for MCI patients or controls. Error bars denote mean ± SD. SD bars have similar heights for VT/fP and SUVR due to different scales on the y-axes. Coefficient of variation of VT/fP was 3–4 times greater than that for SUVR and DVR, as shown by %COV values above SD bars. NS = not significant. Binding values are adjusted for TSPO genotype.
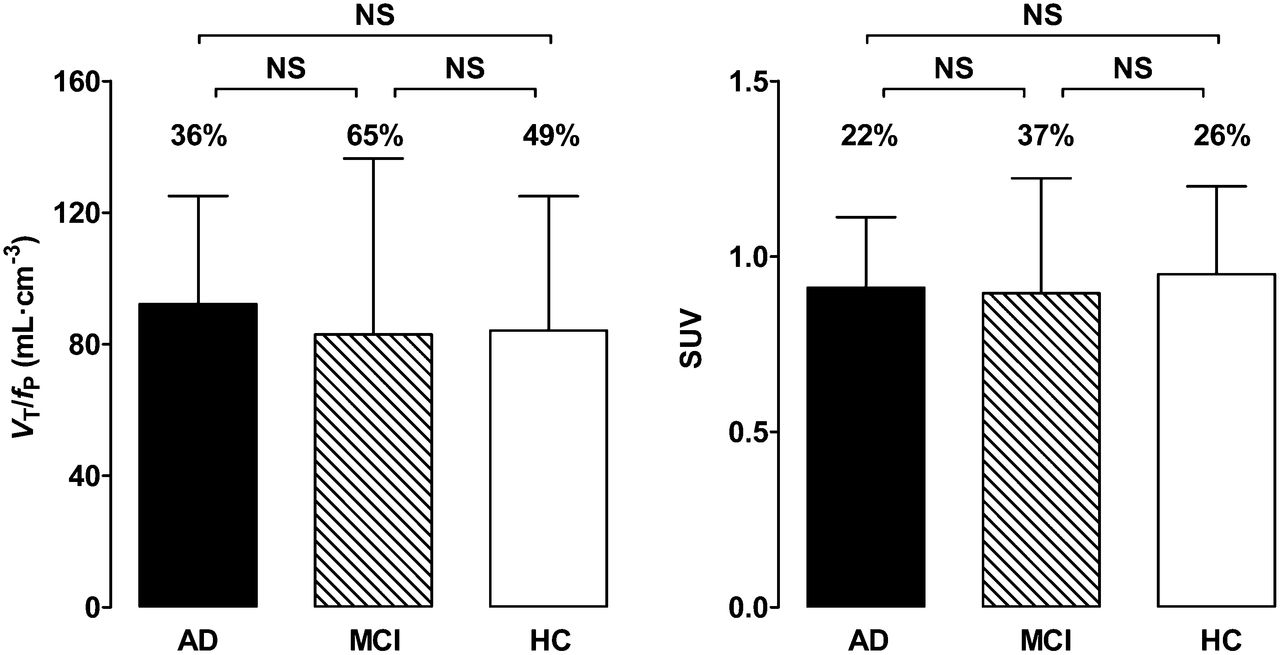
In cerebellum, 11C-PBR28 binding did not differ between controls and patients with MCI or AD. 11C-PBR28 binding values in VT/fP and SUV are shown. Error bars denote mean ± SD. %COV values are shown above vertical bars. NS = not significant. Binding values are adjusted for TSPO genotype.
SUVRs for 11C-PBR28 were greater in AD patients than controls in the inferior parietal and combined middle and inferior temporal cortices; precuneus; and entorhinal and parahippocampal cortices (Table 1; Fig. 1). With the exception of the precuneus, these regions survived correction for multiple comparisons. The SUVRs of the combined middle and inferior temporal cortex were greater in AD patients than MCI patients and survived correction for multiple comparisons. Both VT/fP values and SUVRs in the combined middle and inferior temporal cortex were positively correlated with the Clinical Dementia Rating sum-of-boxes scores (P < 0.01; Fig. 3).

Correlation between binding values and severity of cognitive impairment measured by sum-of-boxes of Clinical Dementia Rating (CDR) score. VT/fP, SUVR, and DVR of combined middle and inferior temporal cortex similarly correlated with severity of cognitive impairment. Noninvasive ratio method did not deteriorate correlation with clinical severity.
The variability of SUVRs (%COV) was much lower than that of VT/fP values in every region and every diagnostic group (Table 2). Also, within the same TSPO genotype groups, the variability of SUVRs was much lower than that of VT/fP values (%COV of SUVR for HAB, 1%–9%, and MAB, 4%–13%, vs. %COV of VT/fP for HAB, 13%–27%, and MAB, 16%–36%).
Effect of Quantification Method on Variability of 11C-PBR28 Binding Values
DVR values were greater in patients with AD than controls in the inferior parietal lobule, combined middle and inferior temporal cortex, precuneus, hippocampus, entorhinal cortex, and parahippocampal gyrus (P < 0.01). DVR values were greater in AD patients than MCI patients in the inferior parietal lobule, middle and inferior temporal cortex, occipital cortex, entorhinal cortex, and parahippocampal gyrus (P < 0.04) (Supplemental Table 1). Variability was similar for both SUVRs and DVR values after genotype correction (%COV, 7%–21% vs. 8%–25%).
SUVRs for 11C-PBR28 were greater in AD patients than controls even without genotype correction in the inferior parietal (P = 0.002) and combined middle and inferior temporal cortices (P = 0.003). However, the statistical significance was greater (P < 0.0005 for 2 regions above), and 2 more regions (entorhinal and parahippocampal cortices) became significant, after correcting for TSPO genotype. Paradoxically, mean SUVRs in HABs were consistently lower than those in MABs in all diagnostic groups and in all regions (mean SUVRs of combined middle and inferior temporal cortex [HAB vs. MAB]: 0.98 vs. 1.05 in HC, 0.98 vs. 1.10 in MCI, and 1.08 vs. 1.15 in AD; Supplemental Table 2; Supplemental Fig. 2).
DISCUSSION
This study found that a simple ratio method (SUVR) can substitute for, and may even be more sensitive than, absolute quantitation for 11C-PBR28 PET. Therefore, this ratio method may be promising for the clinical application of 11C-PBR28 PET to study AD. One may expect the ratio method to provide results independent of TSPO genotype because affinity status is the same in both the target regions and the cerebellum. However, because genotype differences affect specific binding and not nonspecific binding, this ratio method should not completely remove the effect of TSPO genotype on total binding values. Therefore, TSPO genotype correction is still recommended.
The major limitation shared by all tested second-generation TSPO radioligands is differential affinity for the target protein caused by the rs6971 (Ala147Thr) SNP in exon 4 of the TSPO gene (15). Individuals without the SNP demonstrate the expected affinity of radioligand for TSPO (high-affinity binding). In the case of 11C-PBR28, the presence of 1 copy of this SNP reduces specific TSPO binding by more than 40% (mixed-affinity binding); those homozygous for the SNP show no discernible binding at all (low-affinity binding) (10). Therefore, the gold standard method of quantification for second-generation TSPO radioligands—calculating the VT using arterial input function (12)—requires correction for affinity status to avoid underestimating TSPO density in SNP carriers. Affinity status must be determined by genetic analysis or in vivo binding assay (10,15).
However, even within the same affinity group, significant overlap in binding values exists (10,16), suggesting that factors other than genotype contribute to this variability (10,17,18). Altered TSPO expression in response to external stimuli (for instance, stress) as well as normal physiologic changes may partly explain this individual variability (19,20); it should also be noted that, even in the same subject, the contribution of these factors may change between scans. These factors may explain the low test–retest reproducibility of the TSPO radioligands 11C-(R)-PK11195 and 11C-DPA713 using traditional analytic methods (20,21). In addition, the 2-tissue-compartment model requires arterial catheterization to measure the concentration of parent radioligand in plasma. In addition to being invasive, arterial sampling adds a potential source of error that may increase PET data variability. The fP may also contribute to variability in clinical PET studies. Therefore, a target-to-reference ratio approach may be preferable to absolute quantification with compartmental modeling, both for eliminating individual variation of physiologic TSPO expression and for avoiding errors in measuring plasma concentration of the radioligand. Our ratio approach appears to at least partly reduce the variability caused by differences in TSPO genotype as well. In the present study, the %COV of VT/fP was higher than 30% in all regions. This high variability requires relatively large sample sizes to detect statistically significant differences between groups. However, the variability of the SUVR was much lower (<22%), and we expect this ratio method to increase statistical power to detect differences in TSPO binding in clinical studies of AD.
Errors in measuring the free fraction of radioligand may also contribute to high variability in clinical PET studies. Because only free radioligand enters the brain, correcting VT for fP should theoretically increase the accuracy of PET measurement of receptor density. However, correcting for fP may introduce noise, thereby reducing precision. In our study, we found no difference in the %COV between VT and VT/fP values after genotype correction (36%–74% vs. 34%–71%). Using VT/fP thus did not reduce precision, suggesting that the theoretically more accurate VT/fP should be used for absolute measurement of 11C-PBR28 binding.
For a ratio method to be clinically useful in PET studies, the reference region should be relatively unaffected by disease pathology in terms of the density of the target protein. Although diffuse amyloid plaques with surrounding microglia can be found in the cerebellum in advanced AD, the morphology of the cerebellar microglia differs from that of typical activated microglia in the neocortex, and the cerebellum is relatively spared from neurodegeneration (5–7). Therefore, we can reasonably assume that pathologic increases in TSPO are much lower in the cerebellum than in cortical gray matter regions most affected by AD and that the cerebellum can serve as the best reference region in AD (22). This argument is supported by the similar values observed for VT/fP and SUV in the cerebellum among the HCs and MCI and AD patients in this and in our previous study (2).
When using 11C-PBR28, both DVR and SUVR discriminate AD patients from MCI patients and controls. Although the DVR method has the advantage of using the full kinetics of the radioligand, SUVR is more practical because it does not require arterial catheterization and allows for shorter scanning time.
An earlier study using the second-generation TSPO radioligand 11C-DAA1106 found greater binding in AD patients than controls in several regions, including the cerebellum (23). In that study, the cerebellar binding potential was 14% greater in AD patients than in controls (10 AD patients vs. 10 controls). In our larger study (25 AD patients vs. 21 controls), we found no difference in binding (using VT/fP) in the cerebellum. This discrepancy could be due to several factors, including the outcome measure used and the number and characteristics of the study subjects. However, the difference in the TSPO radioligand used could also be a factor. Therefore, studies using TSPO radioligands other than 11C-PBR28 should compare cerebellar binding using absolute values (e.g., VT/fP) between patient and control groups before using this SUVR method.
Our approach in this study was similar to that of Coughlin et al., who showed that normalizing the VT values of regions for 11C-DPA713 to that of total gray matter lowered variability and improved test–retest reproducibility (20). This normalization also removed the effect of TSPO genotype differences. However, using global gray matter as the reference region means that binding in the target region is represented in both the numerator and the denominator. Therefore, this approach may underestimate binding in target regions, particularly relatively preserved areas in AD, and may produce unexpected results of decreased binding in those regions in AD patients.
Unlike the gray matter normalization by Coughlin et al., SUVR with cerebellar pseudo-reference region did not completely ameliorate the TSPO genotype effect as larger differences between AD patients and controls were detected after correcting 11C-PBR28 binding values for affinity status. Therefore, we recommend genotype correction when using the SUVR method. In this study, TSPO genotype had a paradoxical effect on the ratio method of analysis, resulting in MABs having larger SUVRs than HABs. We are not certain if this unexpected finding represents a true result or not. Additional studies with larger sample sizes are needed to clarify the significance of this finding.
One of the most notable results of this study is clear replication of our previous findings. In our earlier study (2), we found that the AD patients showed greater VT/fP values in the inferior parietal, entorhinal, and combined middle and inferior temporal cortices than controls when using PET data not corrected for PVE. By including 15 additional subjects (42 subjects in the previous vs. 57 in the current study), we found greater 11C-PBR28 binding in AD patients in the same regions. Moreover, using the SUVR method we found that AD patients showed greater binding than controls in a larger number of regions, with distribution similar to that seen in our previously reported results using 11C-PBR28 with a 2-tissue-compartment model and PVE-corrected data. Using SUVRs did not reduce the correlation between clinical severity and 11C-PBR28 binding seen with VT/fP. Although we did not include PVE correction in this study, we would expect to see even larger differences between AD patients and controls.
Because MCI patients with amyloid-positivity on PET are at high risk for developing dementia due to AD (24), the increased neuroinflammation observed with 11C-PBR28 PET may be a marker for conversion to clinical AD (2). We hope this SUVR method for 11C-PBR28 PET could prove useful for testing antiinflammatory agents in AD (25).
CONCLUSION
A simple ratio method (SUVR) can substitute for, and may even be more sensitive than, absolute quantitation for detecting regions with increased binding to TSPO in AD. This method reduces variability and has the advantages of not requiring arterial sampling and allowing for shorter scanning time. TSPO genotype correction was still required to increase sensitivity. This method is expected to improve subject tolerability for 11C-PBR28 PET studies in AD, particularly longitudinal studies, and increase the power necessary to detect group differences. The method also needs to be replicated in larger samples of AD patients before it can be widely used. For other diseases, application of this method will first require validation with gold standard methods of quantification that binding in the cerebellum is not affected by the disease itself.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This project was funded in part by the Intramural Research Program of the National Institute of Mental Health, National Institutes of Health (IRP-NIMH-NIH), and a fellowship award from the American Academy of Neurology Foundation, under clinicaltrials.gov identifier NCT00613119 (protocol # 08-M-0066). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
Ioline Henter provided excellent editorial assistance.
Footnotes
Published online Mar. 12, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 23, 2014.
- Accepted for publication February 3, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [11C]PS13 Demonstrates Pharmacologically Selective and Substantial Binding to Cyclooxygenase-1 in the Human Brain
- Remote Neuroinflammation in Newly Diagnosed Glioblastoma Correlates with Unfavorable Clinical Outcome
- [18F]DPA-714 PET Imaging in the Presurgical Evaluation of Patients With Drug-Resistant Focal Epilepsy
- Individual regional associations between A{beta}-, tau- and neurodegeneration (ATN) with microglial activation in patients with primary and secondary tauopathies
- [18F]ROStrace detects oxidative stress in vivo and predicts progression of Alzheimers disease pathology in APP/PS1 mice
- Mitochondrial control of microglial phagocytosis in Alzheimers disease
- Microglia Activation in Basal Ganglia Is a Late Event in Huntington Disease Pathophysiology
- Association of Early {beta}-Amyloid Accumulation and Neuroinflammation Measured With [11C]PBR28 in Elderly Individuals Without Dementia
- Olfactory impairment is related to tau pathology and neuroinflammation in Alzheimers disease
- Moving Toward Multicenter Therapeutic Trials in Amyotrophic Lateral Sclerosis: Feasibility of Data Pooling Using Different Translocator Protein PET Radioligands
- Regional protein expression in human Alzheimers brain correlates with disease severity
- Automatic Extraction of a Reference Region for the Noninvasive Quantification of Translocator Protein in Brain Using 11C-PBR28
- We need to talk about reliability: Making better use of test-retest studies for study design and interpretation
- Head-to-Head Comparison of 11C-PBR28 and 18F-GE180 for Quantification of the Translocator Protein in the Human Brain
- Neuroinflammation Appears Early on PET Imaging and Then Plateaus in a Mouse Model of Alzheimer Disease
- Pseudoreference Regions for Glial Imaging with 11C-PBR28: Investigation in 2 Clinical Cohorts
- The 5-HT1A Receptor PET Radioligand 11C-CUMI-101 Has Significant Binding to {alpha}1-Adrenoceptors in Human Cerebellum, Limiting Its Use as a Reference Region
- Parametric Binding Images of the TSPO Ligand 18F-DPA-714
- Glial Activation and Glucose Metabolism in a Transgenic Amyloid Mouse Model: A Triple-Tracer PET Study
- Imaging Microglial Activation with TSPO PET: Lighting Up Neurologic Diseases?