


Abstract
The aim of this study was to compare the detection of bone metastases by 99mTc-methylene diphosphonate (99mTc-MDP) planar bone scintigraphy (BS), SPECT, 18F-Fluoride PET, and 18F-Fluoride PET/CT in patients with high-risk prostate cancer. Methods: In a prospective study, BS and 18F-Fluoride PET/CT were performed on the same day in 44 patients with high-risk prostate cancer. In 20 of the latter patients planar BS was followed by single field-of-view (FOV) SPECT and in 24 patients by multi-FOV SPECT of the axial skeleton. Lesions were interpreted separately on each of the 4 modalities as normal, benign, equivocal, or malignant. Results: In patient–based analysis, 23 patients had skeletal metastatic spread (52%) and 21 did not. Categorizing equivocal and malignant interpretation as suggestive for malignancy, the sensitivity, specificity, positive predictive value, and negative predictive value of planar BS were 70%, 57%, 64%, and 55%, respectively, of multi-FOV SPECT were 92%, 82%, 86%, and 90%, of 18F-Fluoride PET were 100%, 62%, 74%, and 100%, and of 18F-Fluoride PET/CT were 100% for all parameters. Using the McNemar test, 18F-Fluoride PET/CT was statistically more sensitive and more specific than planar or SPECT BS (P < 0.05) and more specific than 18F-Fluoride PET (P < 0.001). SPECT was statistically more sensitive and more specific than planar BS (P < 0.05) but was less sensitive than 18F-Fluoride PET (P < 0.05). In lesion–based analysis, 156 lesions with increased uptake of 18F-Fluoride were assessed. Based on the corresponding appearance on CT, lesions were categorized by PET/CT as benign (n = 99), osteoblastic metastasis (n = 46), or equivocal when CT was normal (n = 11). Of the 156 18F-Fluoride lesions, 81 lesions (52%), including 34 metastases, were overlooked with normal appearance on planar BS. SPECT identified 62% of the lesions overlooked by planar BS. 18F-Fluoride PET/CT was more sensitive and more specific than BS (P < 0.001) and more specific than PET alone (P < 0.001). Conclusion: 18F-Fluoride PET/CT is a highly sensitive and specific modality for detection of bone metastases in patients with high-risk prostate cancer. It is more specific than 18F-Fluoride PET alone and more sensitive and specific than planar and SPECT BS. Detection of bone metastases is improved by SPECT compared with planar BS and by 18F-Fluoride PET compared with SPECT. This added value of 18F-Fluoride PET/CT may beneficially impact the clinical management of patients with high-risk prostate cancer.
Prostate cancer is the most common malignancy in men. Clinical nomograms based on prostate-specific-antigen (PSA) levels, Gleason score at biopsy, and clinical stage at presentation have been generated for pretreatment risk stratification and prediction of the probability for local recurrence or distant metastatic spread. On the basis of these parameters, patients are categorized at diagnosis as having low-risk or high-risk primary cancer (1–3). Patients with low-risk cancer are unlikely to have metastatic bone involvement. Therefore, the routine use of bone scintigraphy (BS) for primary staging in all patients with newly diagnosed prostate cancer has been discouraged (3–6). BS is mainly reserved for patients with high-risk cancer, elevated serum alkaline phosphatase levels, bone pain, or equivocal bone lesions on other imaging modalities (3,4,7,8). As the disease evolves, patients may experience biochemical progression, local recurrence, or metastatic spread. The most frequent sites of metastasis are lymph nodes and bone; 90% of patients who die of prostate cancer harbor bone metastases (2,9). The extent of osseous metastatic disease from prostate cancer is an independent prognostic factor (10,11).
BS has been the most widely used method for evaluating skeletal metastases of prostate cancer. However, the results of more recent reports have raised doubts whether BS is as effective for confirming metastatic bone disease as was previously perceived (12–14). The addition of SPECT to planar acquisition has been reported to improve the diagnostic accuracy of BS for detecting malignant bone involvement and to allow for a straightforward comparison with other tomography-based techniques such as CT and MRI (15–18).
Tumor detection using PET, and more recently PET/CT technology, is rapidly growing. The role of 18F-FDG PET in patients with prostate cancer is still under investigation (3,18–22). Other PET tracers suggested for assessment of patients with prostate cancer include 11C- or 18F-labeled choline and acetate, 11C-methionine, 18F-fluorodihydrotestosterone, and 18F-Fluoride (3). The latter was reported to be highly sensitive for detecting bone metastases in oncologic patients (13,23). Increased 18F-Fluoride uptake in malignant bone lesions reflects the increase in regional blood flow and bone turnover characterizing these lesions (16,24,25). Taking advantage of both the favorable characteristics of 18F-Fluoride and the better performance of PET, 18F-Fluoride PET has been reported to be more sensitive for detection of metastases than 99mTc-methylene diphosphonate (99mTc-MDP) BS (12,13,16,17,25,26). A previous study on the initial experience with 18F-Fluoride PET/CT for detection of malignant bone involvement in oncologic patients with various human malignant diseases revealed encouraging results. It appeared that 18F-Fluoride PET/CT may take advantage of the high sensitivity of 18F-Fluoride PET, reducing the risk of false-positive rate by determining the morphology of the scintigraphic lesions on the CT data of the PET/CT study (27).
The purpose of the current study was to prospectively compare the diagnostic accuracy of planar, single, and multifield-of-view (multi-FOV) SPECT, 18F-Fluoride PET, and 18F-Fluoride PET/CT in detection of bone metastases in prostate cancer patients with high-risk for bone metastases.
MATERIALS AND METHODS
Patients
This is a prospective study. 99mTc-MDP BS and 18F-Fluoride PET/CT were performed on the same day in 44 patients (mean age, 71.6 ± 8.8 y) with prostate cancer, high risk for bone metastases. Twenty-five patients were newly diagnosed, with Gleason score ≥ 8 or prostate-specific antigen (PSA) levels ≥ 20 ng/mL or nonspecific sclerotic lesions on CT (4,5). Nineteen patients were referred for evaluation of suspected recurrence or progression, later in the course of the disease. The study was approved by the local ethical committee, and all patients gave written consent to participate in this prospective study.
Planar and SPECT BS
BS was the first to be performed. Planar images of the entire skeleton were acquired 2–3 h after intravenous injection of 925 MBq (25 mCi) 99mTc-MDP using a dual-head camera (Discovery VH; GE Healthcare). In 20 patients, we performed single-FOV SPECT of the lower thoracic and lumbar spine region after a whole-skeleton planar acquisition. In the remaining 24 patients, SPECT of the entire axial skeleton was performed, consisting of 3- or 4-FOV SPECT. SPECT data were reconstructed on the Xeleris workstation (GE Healthcare), using a novel collimator–detector response (CDR) method (Evolution software package; GE Healthcare), which incorporates a quantitative model of CDR function of the acquisition system into an iterative reconstruction algorithm. Because collimator–detector blur is one of the main factors affecting the quality of reconstructed SPECT images, the resulting SPECT data obtained by the CDR method have improved resolution and signal-to-noise characteristics (28). Using this algorithm, a good-quality SPECT view may be acquired within 8 min of acquisition and SPECT of the axial skeleton within 24–32 min (Fig. 1).

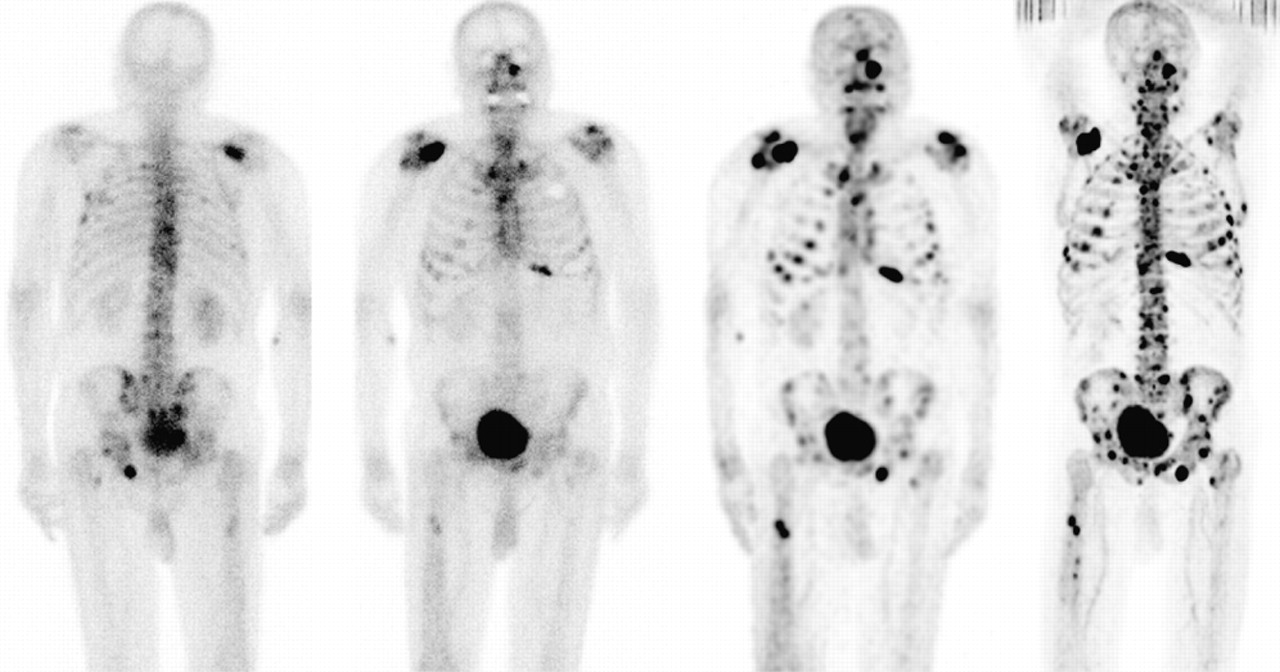
An 82-y-old patient with numerous bone metastases. From left to right: posterior and anterior planar BS, multi-FOV SPECT, and 18F-Fluoride PET images. More lesions are detected on SPECT compared with planar images and on 18F-Fluoride PET compared with SPECT images.
18F-Fluoride PET/CT Study
18F-Fluoride preparation was previously reported in detail (27). No special preparations were needed before the 18F-Fluoride PET/CT study. The PET/CT study was performed in the afternoon, on the same day as BS. Scanning was performed 60–90 min after intravenous administration of 296–444 MBq (8–12 mCi) 18F-Fluoride using a Discovery LS PET/CT system (GE Healthcare). Low-dose CT acquisition was performed first with 140 kV, 80 mA, 0.8 s per CT rotation, a pitch of 6, and a table speed of 22.5 mm/s, without any specific breath-holding instructions. A PET emission scan was performed immediately after acquisition of the CT, without changing the patient's positioning. From 5 to 9 bed positions were performed with an acquisition time of 3 min for each, imaging the skeleton from skull to midthigh. PET images were reconstructed using an ordered-subsets expectation maximization algorithm. CT data were used for attenuation correction. Studies were interpreted on a Xeleris workstation.
Image Interpretation and Analysis of Findings
Planar, SPECT, 18F-Fluoride PET, and 18F-Fluoride PET/CT images were interpreted blindly and separately. The interpretation of 99mTc-MDP BS was made as a consensus reading of 2 nuclear medicine physicians and that of the PET/CT as a consensus reading of a nuclear medicine physician and a radiologist.
Each site of abnormally increased uptake of 99mTc-MDP or 18F-Fluoride was recorded and categorized as normal (no increased uptake), benign, malignant, or equivocal. Scintigraphic lesions were categorized as benign when they appeared as hot osteophytes or when they were located around joints. Vertebral lesions were considered malignant when they involved the posterior aspect of the vertebral body and pedicle or when they involved the vertebra extensively (15,29). Rib lesions were categorized as malignant when they presented as elongated uptake, categorized as benign (fractures) when vertically they involved several ribs, and as equivocal otherwise. Based on the corresponding morphology on the CT data of PET/CT, lesions were diagnosed as benign when degenerative changes, fractures, or other benign bone lesions such as bone cysts were detected at the corresponding location on CT. Lesions were diagnosed as metastases if they were associated with characteristic osteoblastic metastases on CT. If neither blastic nor benign abnormalities were found on CT at the corresponding location with the PET abnormality, the PET/CT lesion was categorized as equivocal. Patients were monitored for at least 6 mo (mean, 10 ± 3 mo; range, 6–15 mo), and their medical records were reviewed with an attempt to get a final diagnosis of equivocal lesions.
Statistical Analysis
Patient-based and lesion-based analyses were performed. For each of the modalities the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were determined for the differentiation of malignant bone involvement from benign. Comparison of the detection of bone metastases by planar BS, SPECT, 18F-Fluoride PET, and 18F-Fluoride PET/CT was performed using the McNemar test with P < 0.05 being statistically significant.
RESULTS
Patient-Based Analysis
Of the 44 study patients, 23 had bone metastases (52%) based on definitive PET/CT findings, biopsy, and imaging follow-up. PET/CT clearly identified malignant bone involvement, detecting skeletal lesions with increased uptake of 18F-Fluoride on the PET data and corresponding osteoblastic metastases on the CT data in 20 of the 23 patients. In the remaining 3 patients, PET/CT was categorized as equivocal because one or two 18F-Fluoride lesions were detected with normal CT. MRI was also not definitive. The diagnosis of osseous metastases was established by a rib biopsy in 1 patient and by progression of osseous metastases by clinical and imaging follow-up in 2 other patients. In spite of the fact that these patients with equivocal 18F-Fluoride PET/CT were found to have metastases, for the purpose of assessing the accuracy of imaging techniques in detection of bone metastases at a given time point, we analyzed the results twice: categorizing the equivocal reading as suggestive for malignancy and, again, categorizing the equivocal reading as benign.
Nineteen patients had benign bone lesions on scintigraphic imaging but no metastases. The benign nature of the lesions was determined by detection of benign findings in the corresponding location on the CT part of PET/CT. In 2 additional patients scintigraphic studies were normal. Follow-up of patients included monitoring of PSA and alkaline phosphatase levels and imaging follow-up by BS and diagnostic CT. All 21 patients who were negative for bone metastases on 18F-Fluoride PET/CT had no clinical or imaging evidence of metastatic spread for at least the 6-mo follow-up period. Table 1 summarizes the comparison in detection of bone metastases by BS (planar and single-FOV or multi-FOV SPECT) and 18F-Fluoride PET/CT. In 20 of the 44 study patients (45%), the definition of malignant bone involvement by PET/CT and by 99mTc-MDP BS did not correlate. In 7 patients with benign PET/CT, BS was interpreted as equivocal or malignant, and in 13 patients with metastatic spread on PET/CT, BS was interpreted as benign or equivocal. Table 2 summarizes the sensitivity, specificity, PPV, and NPV of planar BS, combined planar and SPECT BS (a single-FOV SPECT in 20 patients and multi-FOV SPECT in 24), 18F-Fluoride PET, and 18F-Fluoride PET/CT in the 44 study patients. Using the McNemar comparison test, sensitivity of 18F-Fluoride PET/CT was significantly better than that of BS when equivocal reading was categorized as malignant or when categorized as benign (P < 0.05 and P < 0.001, respectively). Specificity of 18F-Fluoride PET/CT was significantly better when equivocal reading was categorized as malignant (P < 0.05). It was higher (100% vs. 82%) but not statistically significant when equivocal reading was categorized as benign. Sensitivity of 18F-Fluoride PET and 18F-Fluoride PET/CT was the same. Specificity of PET/CT was significantly higher compared with PET alone (P < 0.001).
Comparison of Detection of Bone Metastases by 99mTc-MDP BS and by 18F-Fluoride PET/CT
Assessment of Skeletal Metastatic Spread by Planar 99mTc-MDP BS, Planar and SPECT BS, 18F-Fluoride PET, and 18F-Fluoride PET/CT: Patient-Based Analysis in 44 Patients with High-Risk Prostate Cancer
Twenty-two of the study patients, 13 patients with bone metastases and 11 without, had axial SPECT composed of 3 or 4 FOVs. In this subgroup of patients it was possible to assess the impact of tomography comparing the detection of metastases by SPECT with that of planar BS and to assess the impact of the different radiopharmaceutical (99mTc-MDP vs. 18F-Fluoride) and the different technology (SPECT vs. PET) comparing the detection of metastases by SPECT with that of 18F-Fluoride (Figs. 1–3⇓). Table 3 summarizes this comparison. SPECT was statistically more sensitive (P < 0.05) and more specific (P < 0.05) than planar BS for detection of bone metastases. 18F-Fluoride PET was significantly more sensitive than SPECT BS in detecting metastases (P < 0.05,). Specificity of 18F-Fluoride PET and of SPECT BS was identical.

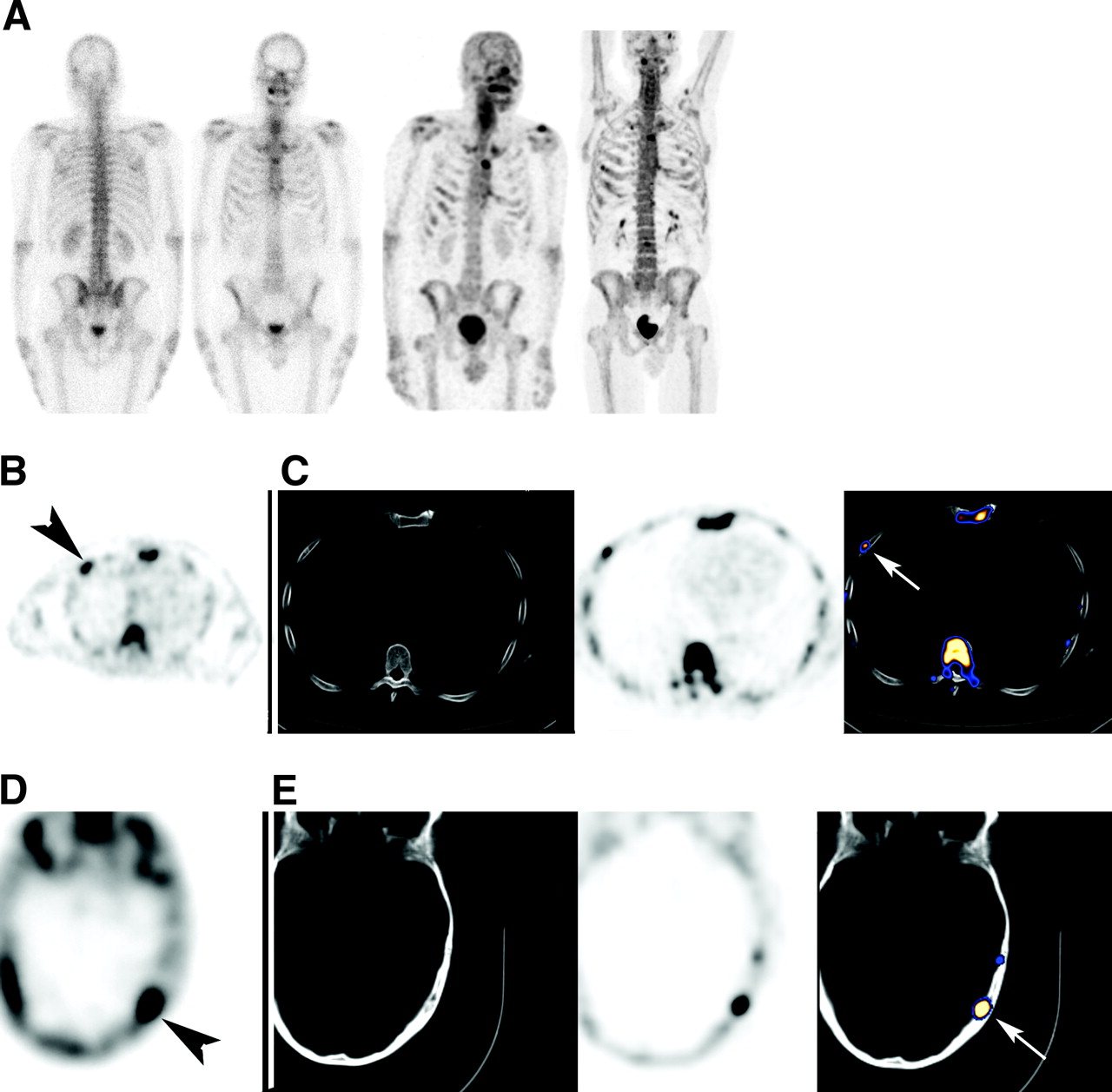
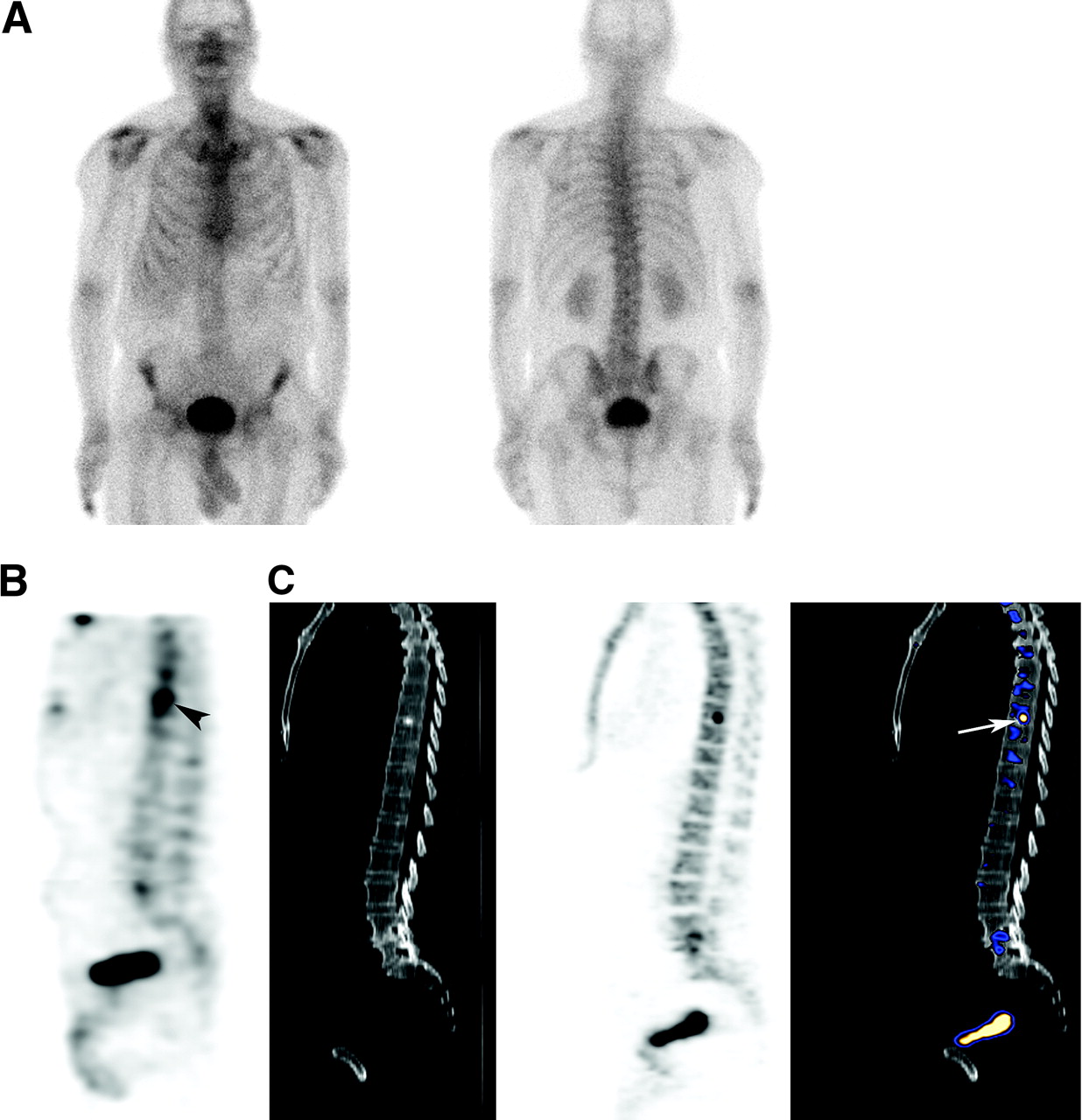
Early metastatic spread missed on planar BS in 57-year-old patient with prostate cancer at diagnosis. (A) From left to right: posterior and anterior planar BS, multi-FOV SPECT, and 18F-Fluoride PET images. Planar BS was interpreted as negative for bone metastases. (B and C) Osteoblastic rib metastasis on SPECT (B) and on 18F-Fluoride PET/CT (C). From left to right: SPECT (metastasis marked by arrowhead), CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT (metastasis marked by arrow). (D and E) Osteoblastic metastasis in skull on SPECT (D) and on 18F-Fluoride PET/CT (E). From left to right: SPECT (metastasis marked by arrowhead), CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT (metastasis marked by arrow).
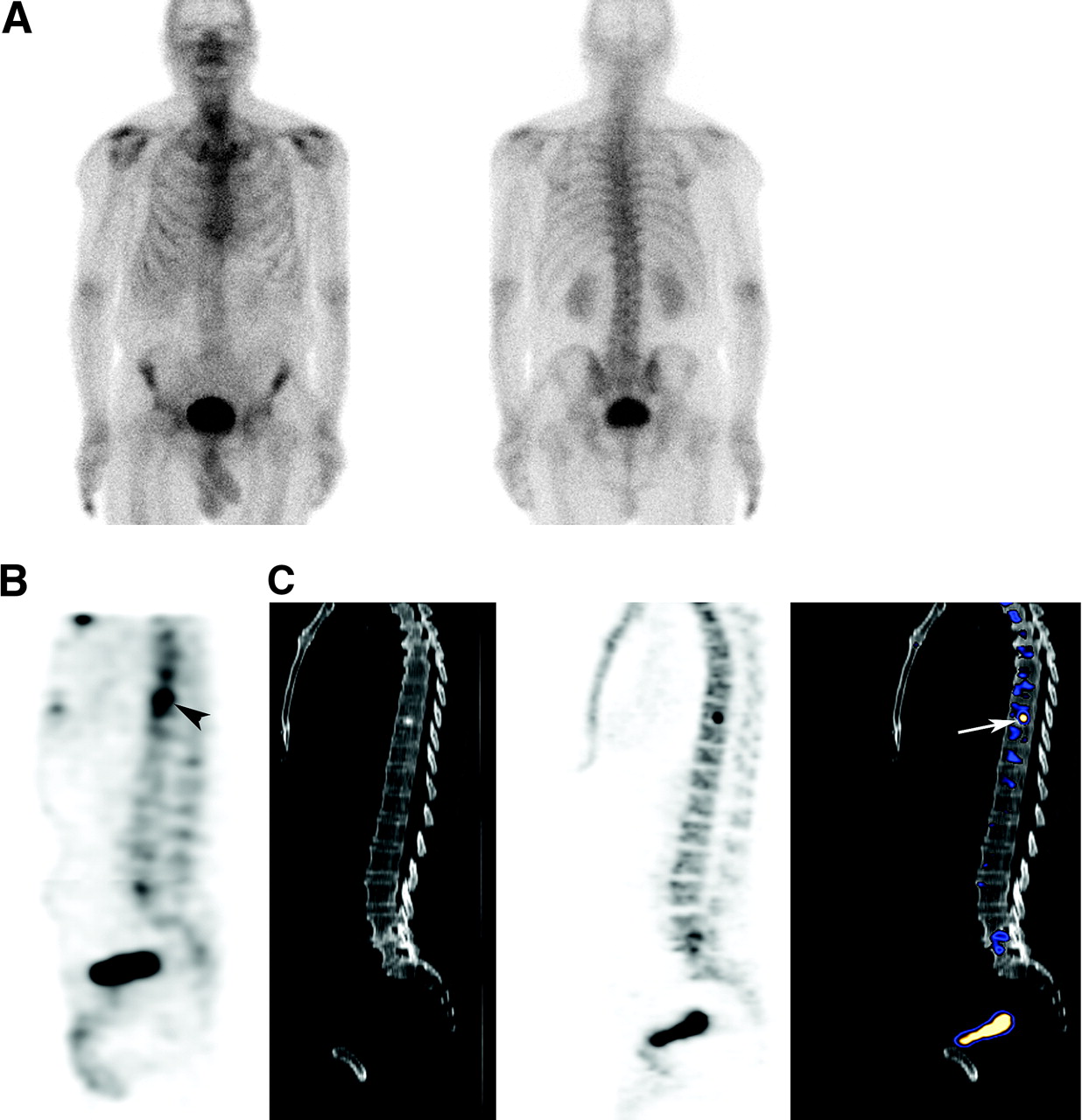
A single metastasis missed on planar BS in 63-y-old patient with prostate cancer at diagnosis. (A) Anterior and posterior planar BS, which was interpreted as negative for bone metastases. (B and C) Osteoblastic metastasis in D8 vertebra identified on SPECT (B) and on 18F-Fluoride PET/CT (C). From left to right: SPECT (metastasis marked by arrowhead), CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT (metastasis marked by arrow).
Detection of Bone Metastases in 24 Study Patients Who Had Multi-FOV Axial-Body SPECT
Lesion-Based Analysis
One hundred fifty-six sites of increased 18F-Fluoride uptake were assessed. Three of the patients with positive PET/CT had extensive spread with countless metastases and, therefore, could not be included in a lesion-based analysis (Fig. 1).
Location and final diagnosis of 156 lesions with increased 18F-Fluoride uptake are summarized in Table 4. A benign abnormality in a corresponding location with the scintigraphic lesions was identified on the CT part of the PET/CT study for 99 lesions (64% of lesions). Forty-six lesions (29% of lesions) showed characteristic osteoblastic metastases and 11 lesions (7% of lesions) were equivocal because of normal CT. Of the 11 equivocal PET/CT lesions, 1 lesion was a biopsy-proven metastasis and 4 lesions appeared as clear osteoblastic metastasis on follow-up CT. The remaining 6 equivocal lesions were not further assessed as the patients had clear evidence of bone metastases in other sites. The 5 proven metastases, which presented as increased 18F-Fluoride uptake and normal CT, led us to categorize all 11 lesions showing this pattern as metastases in the analysis.
Location and Final Diagnosis of 156 Skeletal Lesions with Increased 18F-Fluoride Uptake
Of the 156 lesions with increased 18F-Fluoride uptake, abnormal uptake of 99mTc-MDP was reported on planar BS in only 75 of the sites (48%). The remaining 81 18F-Fluoride sites showed no increased 99mTc-MDP and were interpreted as normal on BS, including 34 metastases and 47 benign lesions (skull, 6; cervical spine, 8; upper thoracic spine, 9; lower thoracic spine, 11; lumbar spine, 19; pelvis, 12; ribs, 11; long bones, 5) (Figs. 4–6⇓). Fifty-two of the 81 sites missed by planar BS were included in a SPECT FOV, which identified abnormalities in 32 (62%) of these lesions and missed 20. SPECT was available for 24 of the 34 metastases overlooked because of their normal appearance on planar images, identifying abnormal uptake of 99mTc-MDP in 14 and missing 10. Of the 47 benign lesions, SPECT was available in 28, identifying abnormal uptake of 99mTc-MDP in 18 and missing 10.
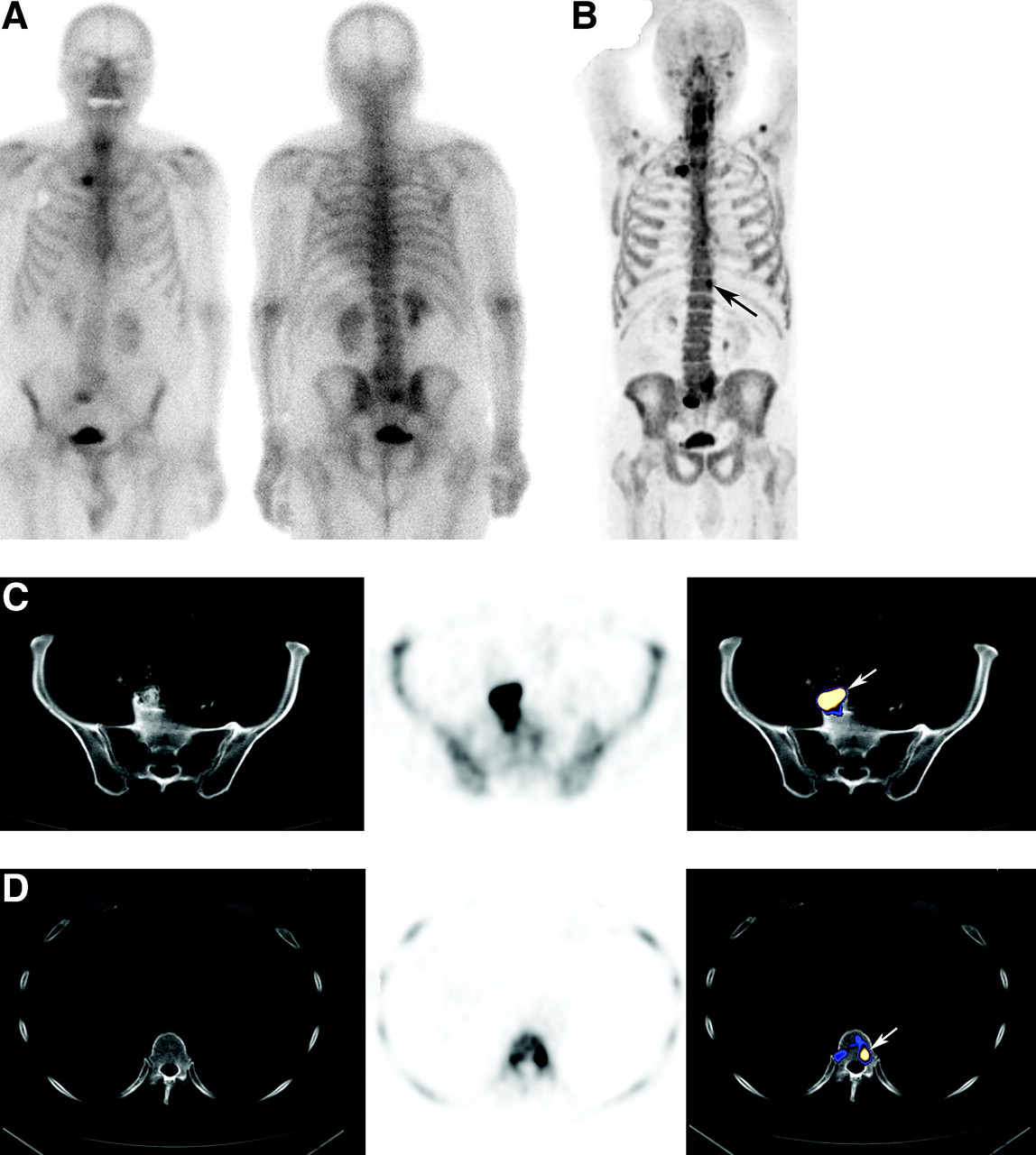
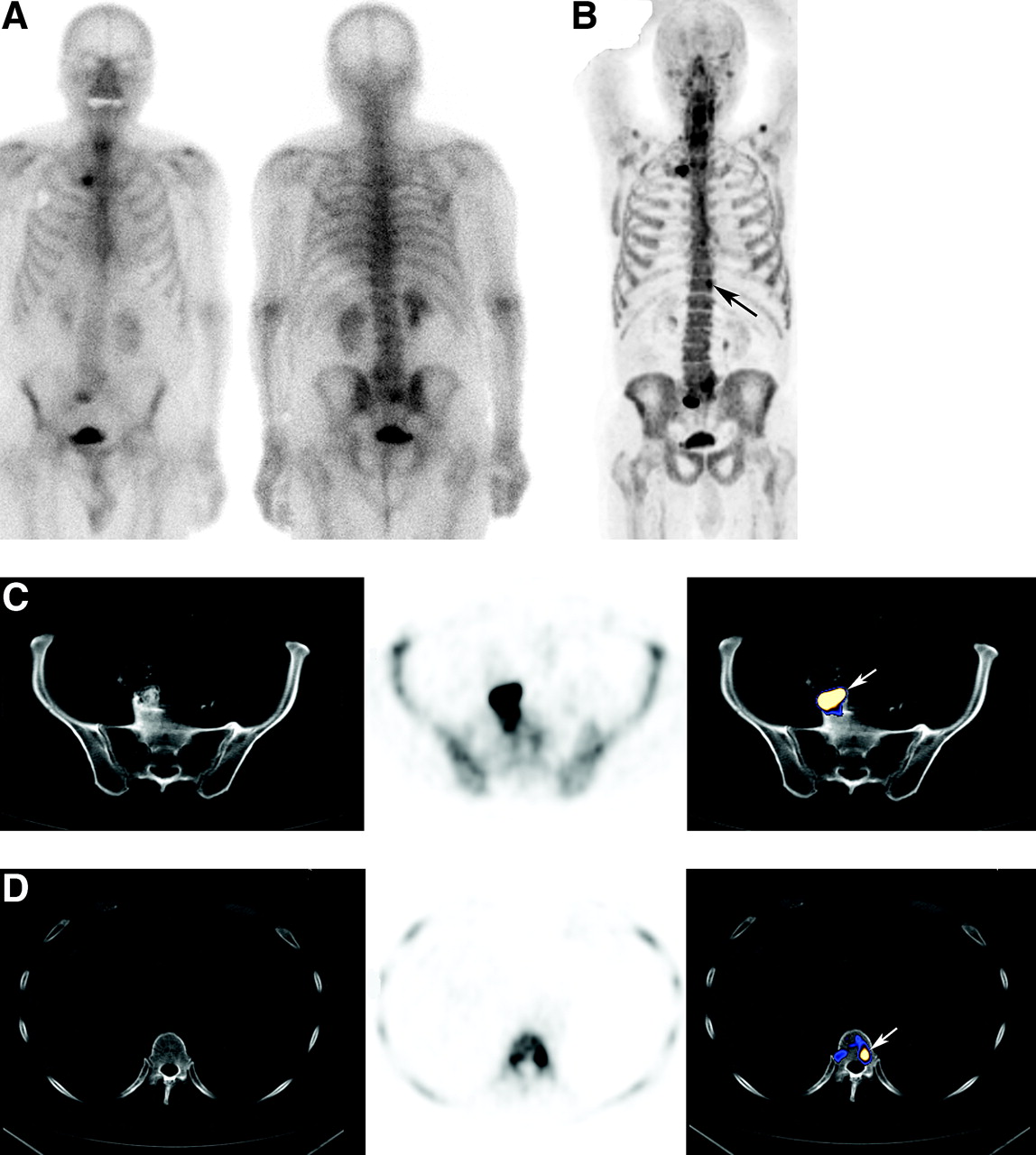
A single metastasis overlooked by planar images in 81-y-old patient with suspected recurrence because of rising PSA levels. (A) On planar bone images, increased uptake is detected in sacrum and right sternoclavicular joint. Degenerative findings are based on correlation with CT. (B) 18F-Fluoride PET maximum-intensity-projection image detecting additional site of uptake in left aspect of D12 (arrow). (C) Lesion identified by planar images is an osteophyte (marked by arrow). From left to right: CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT. (D) Metastasis (marked by arrow) overlooked by planar images. From left to right: CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT.

Bone metastases overlooked by planar images in 72-y-old patient with suspected recurrence because of rising PSA levels. (A) From left to right: posterior and anterior planar BS and 18F-Fluoride PET maximum-intensity-projection image. (B) From left to right on each row: CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT. Top row illustrates a metastatic thoracic vertebra, which was also detected on planar BS (arrow). Middle row illustrates a metastasis in right posterior elements of L1, overlooked by planar BS (arrow). Bottom row illustrates a metastasis in right pubis, barely seen on planar scintigraphy (arrow). Increased site of uptake marked on PET/CT image (arrowhead) is urinary bladder located within an inguinal hernia.

Two examples of bone metastases in pelvic bone, missed by planar images and seen by 18F-Fluoride PET/CT. Each row is separate and includes examples from left to right: CT, 18F-Fluoride PET, and fused 18F-Fluoride PET/CT. Metastases are marked by arrows.
Table 5 summarizes the sensitivity, specificity, PPV, and NPV of BS, 18F-Fluoride PET, and 18F-Fluoride PET/CT as assessed for 156 bone lesions, once by categorizing equivocal findings as suggestive for malignancy and again by categorizing equivocal reading as benign.
Using the McNemar comparison test, sensitivity of 18F-Fluoride PET/CT was significantly better than that of BS when equivocal reading was categorized as malignant or when categorized as benign (P < 0.001 and P < 0.001, respectively). Specificity of 18F-Fluoride PET/CT was significantly better when equivocal reading was categorized as malignant (P < 0.001).
Assessment of Skeletal Metastatic Spread by Planar 99mTc-MDP BS, Planar and SPECT BS, 18F-Fluoride PET, and 18F-Fluoride PET/CT: Lesion-Based Analysis of 156 Lesions
Sensitivity of 18F-Fluoride PET and 18F-Fluoride PET/CT was identical when equivocal reading was categorized as suggestive for malignancy. However, specificity of PET/CT was significantly higher compared with PET alone (P < 0.001). Categorizing equivocal reading as benign, sensitivity of PET/CT was significantly higher than that of PET alone (P < 0.001).
One- hundred twelve of the 156 lesions comprised of 41 metastases and 71 benign lesions were included in a SPECT FOV. Table 6 summarizes the comparison of metastases detection in the latter 112 lesions, by planar BS, SPECT BS, 18F-Fluoride PET, and 18F-Fluoride PET/CT. Categorizing equivocal reading as suggestive for malignancy, SPECT had a significantly higher sensitivity than planar BS (P < 0.001) and a similar specificity. 18F-Fluoride PET had a significantly higher sensitivity compared with SPECT (P < 0.01) and a similar specificity. 18F-Fluoride PET/CT was significantly more specific than 18F-Fluoride PET alone (P < 0.01).
Lesion-Based Analysis of 112 Lesions with Increased 18F-Fluoride for Which SPECT Was Available
Table 7 is a summary of detection of bone metastases by planar BS, multi-FOV SPECT, and 18F-Fluoride PET/CT in 23 study patients with malignant bone involvement.
Detection of Bone Metastases on Planar BS and on Multi-FOV SPECT in 23 Patients with Metastatic Bone Involvement on 18F-Fluoride PET/CT: Patient-Based and Lesion-Based Analysis*
Correlation Between 18F-Fluoride PET/CT Findings and Patient Management
Among the 25 patients with newly diagnosed disease, 18F-Fluoride PET/CT accurately identified or suggested the presence of metastatic bone spread in 11 and excluded bone metatstases in 14 patients, 6 of whom had nonspecific sclerotic bone changes on CT with no corresponding increased uptake of 18F-Fluoride, probably bone islands. In 5 of the 11 patients with newly diagnosed disease, previously unknown bone metastases were identified on scintigraphic assessment and patient management was altered to systemic therapy with androgen withdrawal and bisphosphonate therapy, withholding local therapy approach with external beam radiotherapy. In 3 of the latter patients, early malignant bone involvement was identified by 18F-Fluoride PET/CT but was overlooked by planar BS (scintigraphic data of 2 of the latter patients are illustrated in Figs. 2 and 3). In the remaining 6 newly diagnosed patients with bone metastases, 18F-Fluoride PET/CT findings did not modify the treatment approach as the patients had known osseous or soft-tissue metastases based on other assessment. Local therapy was given only to newly diagnosed patients in whom metastatic spread was excluded. Among the 19 patients with suspected recurrence or disease progression, 18F-Fluoride PET/CT identified bone metastases in 12 patients and excluded bone metastases as the cause for rising PSA levels in 7 patients. The latter patients maintained their previous therapy. On the basis of detection of bone metastases by 18F-Fluoride PET/CT and not by planar BS, 2 patients were referred for chemotherapy, and in 2 other patients androgen withdrawal therapy was modified (Fig. 4).
DISCUSSION
Early detection or exclusion of bone metastases is of a high clinical importance in management of patients with high-risk prostate cancer. Newly diagnosed patients with localized disease and no metastases may benefit from radical localized curative treatment, in contrast with patients who bear metastases, in whom early initiation of androgen withdrawal and bisphosphonate therapy and withholding of unnecessary radical therapy such as radiotherapy is the appropriate treatment approach. Later in the course of the disease, the detection of bone metastases in patients with advanced hormone-refractory disease may indicate the need to modify therapy or treat with chemotherapy. The primary goal of scintigraphic assessment in patients with high-risk prostate cancer is therefore to detect, as early as possible, the presence of bone metastases. Exclusion of bone metastases by negative scintigraphy is another goal, particularly when nonspecific equivocal bony lesions have been detected on CT. Despite adverse clinical parameters, exclusion of metastases allows offering radiotherapy or radical prostatectomy with a curative intent to high-risk patients who otherwise would be managed in a palliative approach (30).
In the current prospective study on 44 patients with high-risk prostate cancer, we compared the detection of bone metastases by 99mTc-MDP planar BS, 99mTc-MDP SPECT, 18F-Fluoride PET, and 18F-Fluoride PET/CT. Bone metastases were found in 52% of the study patients, at least 10 times the prevalence of bone metastases among low-risk patients with prostate cancer (4,5).
18F-Fluoride PET has been found to be more sensitive than 99mTc-MDP BS, particularly when compared with planar images but also when compared with SPECT. 18F-Fluoride, a bone-seeking positron-emitting agent, is characterized by a 2-fold higher bone uptake than 99mTc-MDP, a faster blood clearance, and a better target-to-background ratio (6,16,25,31). In the current study the better sensitivity of 18F-Fluoride PET was reflected by the detection of metastases, which were overlooked by 99mTc-MDP BS. In extreme cases, patient management was altered on the basis of identification of malignant bone involvement solely by 18F-Fluoride PET.
18F-Fluoride is, however, not tumor specific and, therefore, prone to a high false-positive rate (6,31). Differentiation between benign and malignant lesions is obtained by further validation by CT or MRI. As was previously reported, correlation of 18F-Fluoride lesions with CT can be easily made using integrated PET/CT systems with higher specificity of 18F-Fluoride PET/CT compared with 18F-Fluoride PET (27). In the current study, 46 of 57 metastases identified by increased 18F-Fluoride uptake were associated with corresponding osteoblastic changes on the CT part of the study. The remaining 11 metastases presented with increased 18F-Fluoride uptake and normal CT. It should be borne in mind that when assessing tumor detection by a new imaging modality, some suggestive tumor sites cannot be fully characterized, and the more sensitive technique will provide its own standard of criteria. That was the case with proven metastases presenting with increased uptake of 18F-Fluoride and normal CT, reflecting the higher sensitivity of the former (17). The detection of fractures, cysts, or degenerative changes on CT, in corresponding location with increased 18F-Fluoride uptake, has determined the benign nature of other scintigraphic lesions. Nonspecific equivocal sclerotic CT lesions with no corresponding increased 18F-Fluoride uptake reflected benign lesions such as bone islands. The morphologic characterization of scintigraphic lesions by PET/CT resulted in a lower percentage of equivocal interpretations compared with interpretation of 99mTc-MDP BS or 18F-Fluoride PET alone, both on patient-based analysis and on lesion-based analysis.
Schirrmeister et al. reported superiority of 18F-Fluoride PET for detection bone metastases over BS in patients with various human malignancies, including prostate cancer (12,13,17). It was noted that 18F-Fluoride PET was of a higher value when compared with planar BS than when compared with bone SPECT, reflecting the potential benefit of tomographic techniques. A single SPECT view, however, provides tomographic data of only limited skeletal region, whereas several SPECT views with prolonged acquisition protocol can be performed in only a small number of patients (13,32). In 24 of the study patients we used a novel multi-FOV SPECT technology with 3 or 4 SPECT views of the axial skeleton being acquired within 24–32 min (28). The sensitivity of BS on a patient-based analysis improved from 69% for planar images to 92% for multi-FOV SPECT. Similarly, on a lesion-based analysis, sensitivity improved from 39% to 71%. In 13 patients with bone metastases, multi-FOV SPECT was available for correlation, identifying metastases in 12. Planar images were positive in only 8 of the latter 13 patients. Improved lesion detection by SPECT was previously reported primarily for lesions located at the lower thoracic and lumbar vertebral column (14,15,29,32,33). In the current study, the performance of SPECT on the entire axial skeleton resulted in detection of metastases in other locations, including the skull, upper vertebral column, rib cage, pelvis, and long bones (Figs. 2–6⇑⇑⇑).
In spite of the high sensitivity and specificity found for 18F-Fluoride PET/CT, the latter is the most expensive and less available modality among the techniques assessed in the current study. For one to be able to draw a conclusion whether 18F-Fluoride PET/CT should be introduced as a routine imaging approach of metastatic bone survey in cancer patients who are at high-risk for bone metastases, a meticulous cost-effective analysis is required. This was not done in the current study, which is a major limitation. However, because the availability of PET and PET/CT systems, of high-quality SPECT algorithms, and the cost of radiopharmaceuticals may vary in different sites, such an analysis might not be applicable universally. Thus, until precise conclusive indications will be widely available, it might be valuable to exploit the high sensitivity and specificity of 18F-Fluoride PET/CT in selected cases in which the presence of bone metastasis cannot be definitely confirmed or equally excluded by other imaging modalities.
CONCLUSION
18F-Fluoride PET/CT is a highly sensitive and specific modality for detection of bone metastases in patients with high-risk prostate cancer. It is more specific than 18F-Fluoride PET alone and more sensitive and specific than planar and SPECT BS. Detection of bone metastases is improved by SPECT compared with planar BS and by 18F-Fluoride PET compared with SPECT. This added value of 18F-Fluoride PET/CT may beneficially impact the clinical management of patients with high- risk prostate cancer.
Acknowledgments
The study was supported, in part, by a grant of the Israeli Cancer Research. The authors thank Avishay Sella, MD, for referring patients and reviewing the manuscript.
References
- Received for publication September 4, 2005.
- Accepted for publication October 31, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Efficacy of Various Imaging Modalities Across Different Stages of Prostate Cancer: A Network Meta-Analysis of Diagnostic Studies
- Use of 18F-NaF PET in the staging of skeletal metastases of newly diagnosed, high-risk prostate cancer patients: a nationwide cohort study
- Whole-Skeleton SUVmean Measured on 18F-NaF PET/CT Studies as a Prognostic Indicator in Patients with Breast Cancer Metastatic to Bone
- Skeletal sarcoidosis; an uncommon mimic of metastatic disease
- Appropriate Use Criteria for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer After Definitive Primary Treatment
- 18F-Sodium Fluoride PET: History, Technical Feasibility, Mechanism of Action, Normal Biodistribution, and Diagnostic Performance in Bone Metastasis Detection Compared with Other Imaging Modalities
- Observer Agreement and Accuracy of 18F-Sodium Fluoride PET/CT in the Diagnosis of Bone Metastases in Prostate Cancer
- No Added Value of 18F-Sodium Fluoride PET/CT for the Detection of Bone Metastases in Patients with Newly Diagnosed Prostate Cancer with Normal Bone Scintigraphy
- Comparison of the Variability of SUV Normalized by Skeletal Volume with the Variability of SUV Normalized by Body Weight in 18F-Fluoride PET/CT
- Validation of the Semiautomatic Quantification of 18F-Fluoride PET/CT Whole-Body Skeletal Tumor Burden
- SNMMI Procedure Standard for Bone Scintigraphy 4.0
- A Prospective Comparison of 18F-Sodium Fluoride PET/CT and PSMA-Targeted 18F-DCFBC PET/CT in Metastatic Prostate Cancer
- Potential Impact of 68Ga-PSMA-11 PET/CT on the Planning of Definitive Radiation Therapy for Prostate Cancer
- Intraindividual Comparison of 99mTc-Methylene Diphosphonate and Prostate-Specific Membrane Antigen Ligand 99mTc-MIP-1427 in Patients with Osseous Metastasized Prostate Cancer
- Imaging Cardiovascular Calcification
- The Utility of PET/CT in the Planning of External Radiation Therapy for Prostate Cancer
- Anatomic and Molecular Imaging in Prostate Cancer
- Repeatability of Quantitative 18F-NaF PET: A Multicenter Study
- The Role of 18F-Sodium Fluoride PET/CT Bone Scans in the Diagnosis of Metastatic Bone Disease from Breast and Prostate Cancer
- Internalization of secreted antigen-targeted antibodies by the neonatal Fc receptor for precision imaging of the androgen receptor axis
- Evaluation of Prostate Cancer Bone Metastases with 18F-NaF and 18F-Fluorocholine PET/CT
- Bone-Targeted Imaging and Radionuclide Therapy in Prostate Cancer
- Evaluation of Prostate Cancer with PET/MRI
- Prospective Study Evaluating Na18F PET/CT in Predicting Clinical Outcomes and Survival in Advanced Prostate Cancer
- Imaging Bone Metastases in Breast Cancer: Staging and Response Assessment
- Prospective Comparison of 99mTc-MDP Scintigraphy, Combined 18F-NaF and 18F-FDG PET/CT, and Whole-Body MRI in Patients with Breast and Prostate Cancer
- Determination of Skeletal Tumor Burden on 18F-Fluoride PET/CT
- Multimodal Partial-Volume Correction: Application to 18F-Fluoride PET/CT Bone Metastases Studies
- Prognostic Factors in Patients Treated with 223Ra: The Role of Skeletal Tumor Burden on Baseline 18F-Fluoride PET/CT in Predicting Overall Survival
- Evaluation of 18F-Fluoride PET/MR and PET/CT in Patients with Foot Pain of Unclear Cause
- Applications of ImmunoPET: Using 124I-Anti-PSCA A11 Minibody for Imaging Disease Progression and Response to Therapy in Mouse Xenograft Models of Prostate Cancer
- Picture the future: emerging imaging modalities
- Impact of 18F-Fluoride PET on Intended Management of Patients with Cancers Other Than Prostate Cancer: Results from the National Oncologic PET Registry
- PET/MR in Oncology: Non-18F-FDG Tracers for Routine Applications
- Impact of 18F-Fluoride PET in Patients with Known Prostate Cancer: Initial Results from the National Oncologic PET Registry
- PET/CT with Sodium 18F-Fluoride for Management of Patients with Prostate Cancer
- Comparison of 18F-fluoride PET/CT, 18F-FDG PET/CT and bone scintigraphy (planar and SPECT) in detection of bone metastases of differentiated thyroid cancer: a pilot study
- Unmet Needs in the Prediction and Detection of Metastases in Prostate Cancer
- Clinical utility of fluoride-18 positron emission tomography/CT in temporomandibular disorder with osteoarthritis: comparisons with 99mTc-MDP bone scan
- Combined 18F-Fluoride and 18F-FDG PET/CT Scanning for Evaluation of Malignancy: Results of an International Multicenter Trial
- Combined 18F-Fluoride and 18F-FDG PET/CT Scanning for Evaluation of Malignancy: Results of an International Multicenter Trial
- Biodistribution, Tumor Detection, and Radiation Dosimetry of 18F-DCFBC, a Low-Molecular-Weight Inhibitor of Prostate-Specific Membrane Antigen, in Patients with Metastatic Prostate Cancer
- Utility of 18F-Fluoride PET/CT and 18F-FDG PET/CT in the Detection of Bony Metastases in Heightened-Risk Head and Neck Cancer Patients
- Measuring Oncogenic Signaling Pathways in Cancer with PET: An Emerging Paradigm from Studies in Castration-Resistant Prostate Cancer
- The Kinetics and Reproducibility of 18F-Sodium Fluoride for Oncology Using Current PET Camera Technology
- Coronary Arterial 18F-Sodium Fluoride Uptake: A Novel Marker of Plaque Biology
- Imaging Androgen Receptor Signaling with a Radiotracer Targeting Free Prostate-Specific Antigen
- Androgen-Independent Molecular Imaging Vectors to Detect Castration-Resistant and Metastatic Prostate Cancer
- SNM Practice Guideline for Sodium 18F-Fluoride PET/CT Bone Scans 1.0
- Assessment of Patient Exposure to X-Radiation from SPECT/CT Scanners
- Usefulness of Combined FDG-PET with CT or Tumour Markers in Lung Cancer Diagnosis
- The Science and Practice of Bone Health in Oncology: Managing Bone Loss and Metastasis in Patients With Solid Tumors
- New Agents and Techniques for Imaging Prostate Cancer
- Novel Strategy for a Cocktail 18F-Fluoride and 18F-FDG PET/CT Scan for Evaluation of Malignancy: Results of the Pilot-Phase Study
- Magnetic Resonance Imaging Versus Bone Scan in High-Risk Prostatic Carcinoma: Some Methodological Considerations
- Skeletal PET with 18F-Fluoride: Applying New Technology to an Old Tracer
- Magnetic Resonance Imaging of the Axial Skeleton for Detecting Bone Metastases in Patients With High-Risk Prostate Cancer: Diagnostic and Cost-Effectiveness and Comparison With Current Detection Strategies
- An Introduction to Na18F Bone Scintigraphy: Basic Principles, Advanced Imaging Concepts, and Case Examples
- SPECT/Multislice Low-Dose CT: A Clinically Relevant Constituent in the Imaging Algorithm of Nononcologic Patients Referred for Bone Scintigraphy