


Abstract
The objective of this study was to evaluate the rate of detection of bone metastases obtained with the prostate-specific membrane antigen (PSMA)–targeting tracer 99mTc-MIP-1427, as opposed to conventional bone scanning with 99mTc-methylene diphosphonate (99mTc-MDP), in a collective of patients with known advanced-stage osseous metastasized prostate cancer. Methods: Twenty-one patients with known metastatic disease were staged with both conventional bone scanning and PSMA ligand scintigraphy within a time frame of less than 10 d. Imaging included planar whole-body scanning and SPECT or SPECT/CT with 2 bed positions 3 h after injection of either 500–750 MBq of 99mTc-MIP-1427 or 600–750 MBq of 99mTc-MDP. Lesions were scored as typical tumor, equivocal (benign/malignant), or normal within a standard reporting schema divided into defined anatomic regions. Masked and consensus readings were performed with sequential unmasking: planar scans first, then SPECT/CT, the best evaluable comparator (including MRI), PET/CT, and follow-up examinations. Results: Eleven patients had PSMA-positive visceral metastases that were predictably not diagnosed with conventional bone scanning. However, SPECT/CT was required to distinguish between soft-tissue uptake and overlapping bone. Four patients had extensive 99mTc-MDP–negative bone marrow lesions. Seven patients had superscan characteristics on bone scans; in contrast, the extent of red marrow involvement was more evident on PSMA scans. Only 3 patients had equivalent results on bone scans and PSMA scans. In 16 patients, more suspect lesions were detected with PSMA scanning than with bone scanning. In 2 patients (10%), a PSMA-negative tumor phenotype was present. Conclusion: PSMA scanning provided a clear advantage over bone scanning by reducing the number of equivocal findings in most patients. SPECT/CT was pivotal for differentiating bone metastases from extraosseous tumor lesions.
In early-stage prostate cancer, imaging is often performed with curative intent for very low prostate-specific antigen (PSA) levels and very small tumor lesions. In this setting, maximum spatial image resolution and optimal signal-to-noise ratios are important. Prostate-specific membrane antigen (PSMA)–targeting PET/CT is a novel advance that has already demonstrated promising results for primary tumor and lymph node staging as well as for tumor allocation in biochemical relapse (1–3). However, PET/CT is not widely available in less developed countries, and the number of γ-cameras worldwide exceeds the number of PET/CT scanners. Consequently, 99mTc-labeled PSMA tracers have been developed and have already been applied in phase 1 or phase 2 studies (4–7)—but predominantly for patients with early-stage prostate cancer, that is, before prostatectomy or in biochemical recurrence. In contrast, conventional bone scanning (BS) is of limited value in early-stage prostate cancer because positive findings are rare until PSA levels increase to greater than 30 ng/mL (8,9).
On the other hand, more than 90% of patients with metastatic castration-resistant prostate cancer develop bone involvement over time (10). It has already been proven that 18F-NaF PET/CT is superior to conventional 99mTc-labeled BS for the diagnosis of bone metastasis in prostate cancer and other tumors (11–13). However, after curative approaches have been exhausted, improved lesion-level detection rates have limited clinical consequences because patients have already received systemic therapy and the clinical question concerns determining whether there is progression rather than counting lesion numbers. The recent Prostate Cancer Clinical Trials Working Group 3 recommendation suggested that BS is one of the most reliable tools for response assessment (14). Thus, BS is still the mainstay for follow-up examinations of metastatic castration-resistant prostate cancer patients given systemic therapy (15–17). In contrast, the value of PSMA imaging in patients with advanced-stage disease has not been evaluated systematically. With the recent introduction of PSMA radioligand therapy, the interest in this field is increasing. Targeting therapies can be effective only if the target is sufficiently expressed in most tumor lesions. Therefore, all available studies of 177Lu- or 225Ac-PSMA ligand therapy have been performed on patients preselected by PSMA imaging (18–20). However, the highest possible resolution (i.e., that obtained with PET) might not be necessary in this setting, and 99mTc-based PSMA ligands might represent a clinical alternative. In this medical situation, patients scheduled for PSMA-targeting therapy at our clinic receive both conventional BS and PSMA-targeting 99mTc-MIP-1427 scintigraphy within a short interval.
The aim of this retrospective analysis was to compare BS with 99mTc-methylene diphosphonate (99mTc-MDP) and PSMA ligand 99mTc-MIP-1427 in patients with known osseous metastasized prostate cancer.
MATERIALS AND METHODS
Patients
Twenty-one patients who had metastatic castration-resistant prostate cancer and were preparing for possible PSMA radioligand therapy underwent both conventional BS including SPECT and PSMA SPECT/CT for staging. For all patients, the examinations were performed within 10 d of each other (mean and median, 7 d). Table 1 shows the characteristics of the patients.
Patient Characteristics
Selection criteria for this retrospective evaluation were the availability of PSMA and BS performed on the basis of clinical indications within 10 d. The examinations were conducted in accordance with the Helsinki Declaration (“unproven intervention in clinical practice”) and national regulations [German Pharmaceutical Products Act, AMG §13(2b)]. All patients signed a written informed consent form. The ethical committee of the University Hospital Heidelberg approved this retrospective evaluation.
Radiopharmaceuticals
The PSMA ligand MIP-1427 was labeled with 99mTc as already described (21). The precursor was produced in-house as previously described (22) and labeled in accordance with the described protocol but with a minor modification: the deprotected precursor was radiolabeled with the tricarbonyl method using a conventional IsoLink kit (Covidien). Quality control for 99mTc-labeled PSMA ligand MIP-1427 was performed by reversed-phase high-performance liquid chromatography, and 99mTc-labeled PSMA ligand MIP-1427 was discarded if purity was lower than 95%. Quality control for 99mTc-MDP BS was performed by chromatography in accordance with the manufacturer’s (ROTOP-MDP) requirements for purity.
Application and Imaging Protocol
The 99mTc-MDP solution was applied via an intravenous catheter as a bolus injection of 693 ± 33 (mean ± SD) MBq. 99mTc-MIP-1427 was also applied intravenously as a bolus injection (672 ± 94 MBq) via a sterile filter system (Filtropur S 0.2; Sarstedt). Clinical conditions during application and imaging were observed to detect possible adverse events.
For BS, images were acquired 2 h after injection. Planar images were acquired with an ECAM scanner system (Siemens), and SPECT imaging (Infinia Hawkeye 4 scanner system; GE Healthcare) included 2 fields of view of 40 cm per bed position. The first field of view covered the neck/thorax, and the second field of view covered the abdomen/pelvis. PSMA imaging was performed 3 h after nuclide application. Imaging included planar scintigraphy with the ECAM scanner and 2-field-of-view SPECT/CT with the Infinia Hawkeye 4 scanner, covering the neck/thorax and the abdomen/pelvis.
For planar images acquired with the ECAM scanner, low-energy high-resolution collimators were used. The scan velocity was 15 cm/min in a 1,025 × 256 matrix. For SPECT imaging acquired for BS and PSMA scanning, the Infinia Hawkeye 4 scanner system was used with low-energy high-resolution collimation and the following parameters: 128 × 128 matrix; zoom of 1; step-by-step scan by 30 s and 120 images with a 3° angle cut in a 128 × 128 matrix. CT imaging for attenuation correction and lesion evaluation was performed as 4-slice low-dose CT in the Infinia Hawkeye 4 scanner system (140 keV; 40 mAs) on the same day as the PSMA scan and included the neck/thorax and abdomen/pelvis regions.
To reduce the radiation dose, as there is no clinical indication for 2 CT scans in this setting within 10 d, only PSMA imaging was amended by SPECT/CT, whereas BS was amended by SPECT. Afterward, the CT data from PSMA SPECT/CT were transferred to a Siemens Leonardo workstation (syngo MultiModality Workplace VE36A), and software fusion to the bone SPECT data was performed using an automatic soft-fusion toolkit.
Masked Reading
The intensity of tumor uptake was scored visually. Planar images of PSMA scans and 99mTc-MDP bone scans were anonymized and masked for image assessment by 5 nuclear medicine physicians (3 with >5 y of experience and 2 residents in their third and fourth years). Lesions in planar scans were interpreted with regard to their respective characteristic patterns: normal, equivocal, or tumor pattern. Lesion locations were grouped for further analysis; predefined regions were scalp, sternum, thorax, shoulder/scapula, upper arm, lower arm, upper spine, middle spine, lower spine, sacroiliac joint, hip, thighs, knees, and lower limbs. Figure 1 shows further details. In a second step, SPECT for BS (including the CT dataset [soft fusion]) and SPECT/CT (hybrid imaging) for PSMA scanning were unmasked, and the findings were reevaluated, taking into account the additional information.
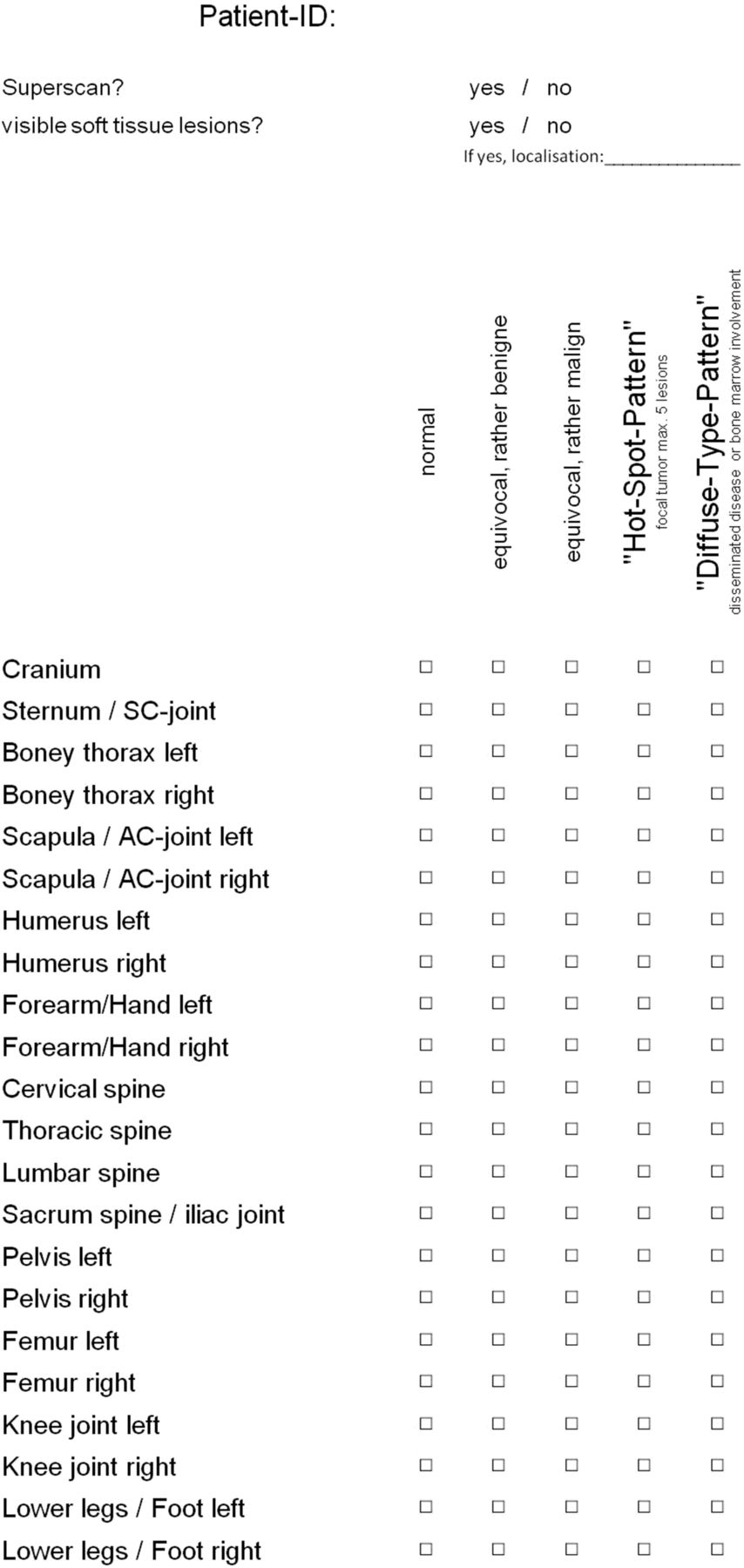
Report form for standardized evaluation of masked patients.
Consensus Reading
Consensus reading was performed after the evaluation of planar imaging and SPECT/CT (soft fusion for bone; hybrid imaging for PSMA) and was amended with all other available clinical information and with data that were acquired from imaging modalities (such as CT, MRI, and PET) during the follow-up period. The results were evaluated by the 5 observers against the definition of the gold standard. This concept (best evaluable comparator) was applied previously in other radiologic research (23). For each patient, a clinical follow-up of at least 6 mo (or until death) was available. Future imaging modalities were chosen according to the respective clinical needs and were not bound to a specific protocol. The ongoing evaluation of primary unknown or equivocal findings usually led to a definite result, as lesions disappeared, remained at a constant level, or grew rapidly (characteristic for malignant lesions in this patient collective with short PSA doubling times).
Statistical Analysis
For every anatomic region and patient, we determined whether each of the readers agreed with the consensus result, in regard to both the 2--step evaluation (benign or malignant) and the finer, 5-step evaluation (normal, equivocal [probably benign], equivocal [probably malignant], focal tumor, or diffuse tumor). The average number (± SD) of readers agreeing with the consensus reading was determined for each method and each patient, and the results were compared using a 2-sided Wilcoxon signed rank test. The results were assessed using Microsoft Excel 2007 (Microsoft Corp.) and R Version 3.3.2 (R Foundation for Statistical Computing). The statistical significance level was set at a P value of less than or equal to 0.05.
Sensitivity and specificity for both PSMA scanning and BS were calculated separately for each reader and region and then averaged, first over readers and then over regions. SEs were calculated for each estimate. Differences between methods were checked for significance using 2-sided paired t tests.
RESULTS
No adverse events during application and imaging were reported. All images of 99mTc-MDP scans (n = 21) and PSMA scans (n = 21) were evaluable. In 3 patients, equal findings from BS and PSMA scanning were present. In 16 patients, PSMA scanning identified more suspect lesions than BS. In 4 patients, 99mTc-MDP–negative but PSMA-positive bone marrow involvement was present. In 3 patients, more bone lesions were detected with PSMA scanning than with BS.
Agreement of Raters
The ratio of typical benign and probably benign lesions and the ratio of typical malignant and probably malignant lesions are shown in Table 2.
Ratio of Equivocal to Normal or Malignant Lesions
The agreement of raters with the consensus reading was significantly greater for PSMA scanning than for 99mTc-MDP BS (Table 3). On the 2-step scale (benign or malignant), 0.43 ± 0.36 of 5 misclassifications were observed for PSMA and 0.76 ± 0.64 of 5 misclassifications were observed for 99mTc-MDP (P = 0.039). On the 5-step scale (normal, equivocal benign, equivocal malignant, focal tumor, or diffuse tumor), an average of 1.45 ± 0.39 of 5 raters misclassified each region using PSMA scans and an average of 2.41 ± 0.66 of 5 raters misclassified each region using 99mTc-MDP scans (P < 0.001). The results for senior physicians and residents were comparable.
Agreement of Raters with Consensus Reading
Sensitivity/Specificity
A significant difference (P < 0.001) was detected between the 92% sensitivity of PSMA scanning (SE = 2%) and the 76% sensitivity of 99mTc-MDP BS (SE = 3%) for the evaluation of bone lesions. On planar scans, the specificity of PSMA scanning for bone lesions was 86% (SE = 3%) and that of 99mTc-MDP BS was 90% (SE = 2%). Differences in specificity were not significant (P = 0.13).
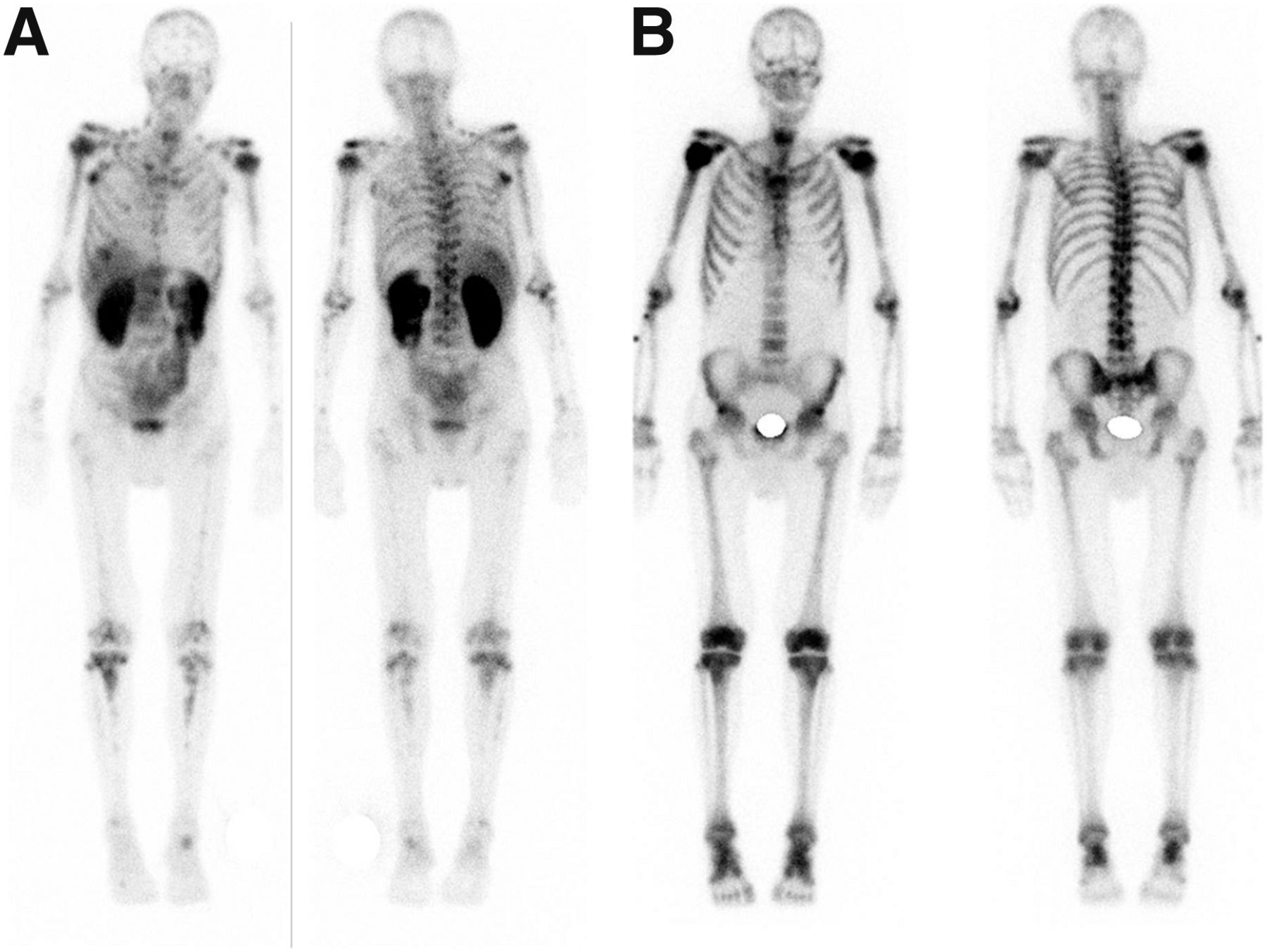
After unmasking of the additional SPECT/CT data, the test quality criteria for 99mTc-MDP remained unchanged. However, the specificity of PSMA for patients with phenotype-positive cancers improved from 86% to 97% (significant). The data for 1 patient with a PSMA-negative but 99mTc-MDP–positive tumor phenotype are shown in Figure 2. The main reason for the low specificity of planar PSMA scans was liver and lung metastases that were projected on ribs and consequently scored as false-positive bone metastases on 2-dimensional planar scans. These dislocations were successfully allocated using transverse slices (Fig. 3).
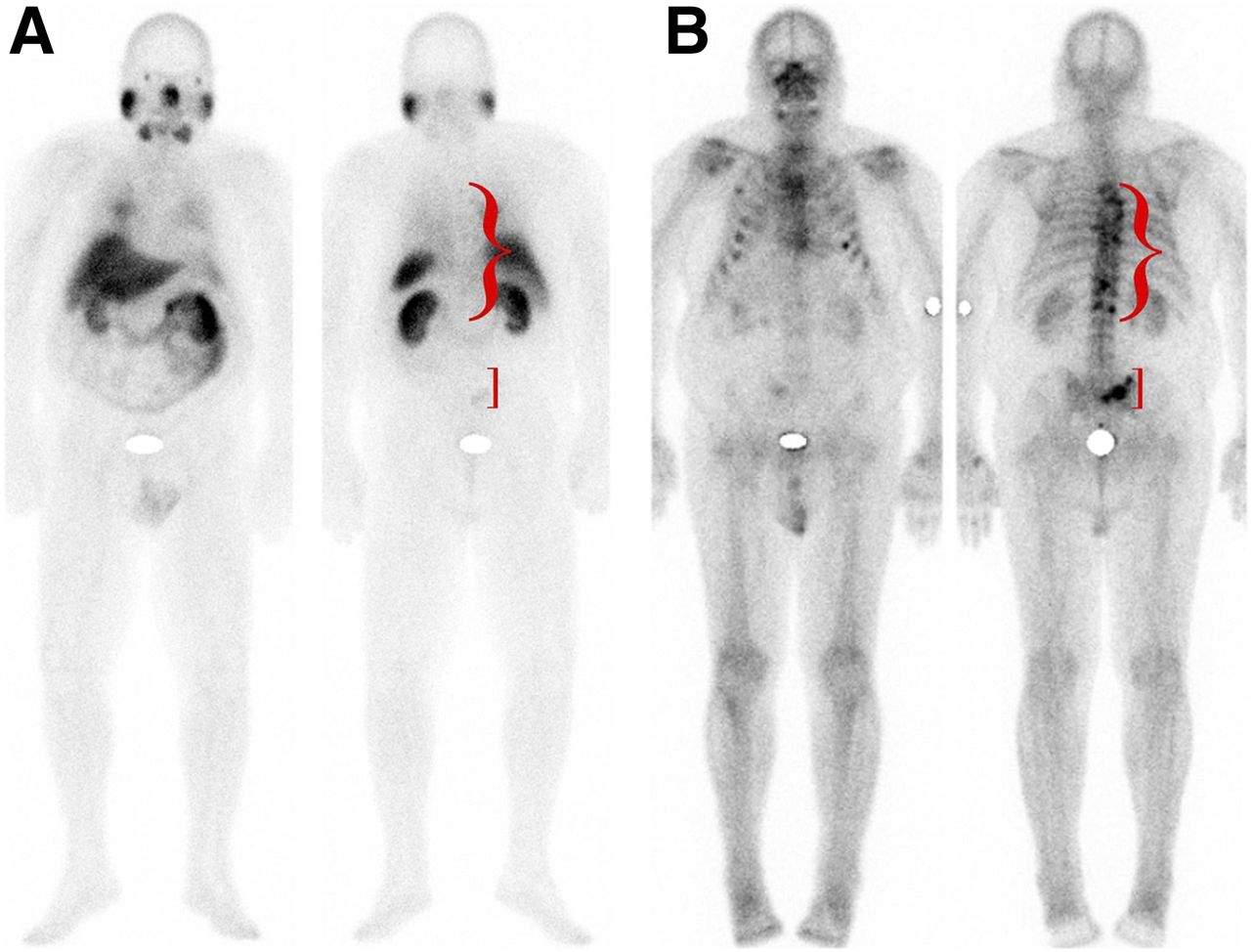
Patient with PSMA-negative tumor phenotype. No pathologic findings in spine or pelvis were depicted with PSMA (A) but were successfully diagnosed by BS (B).

Intrahepatic lesion and pleural carcinosis. Three-dimensional imaging was pivotal for correct allocation of respective lesions. In particular, liver and lung lesions were often misinterpreted and falsely assigned to overlapping bone structures.
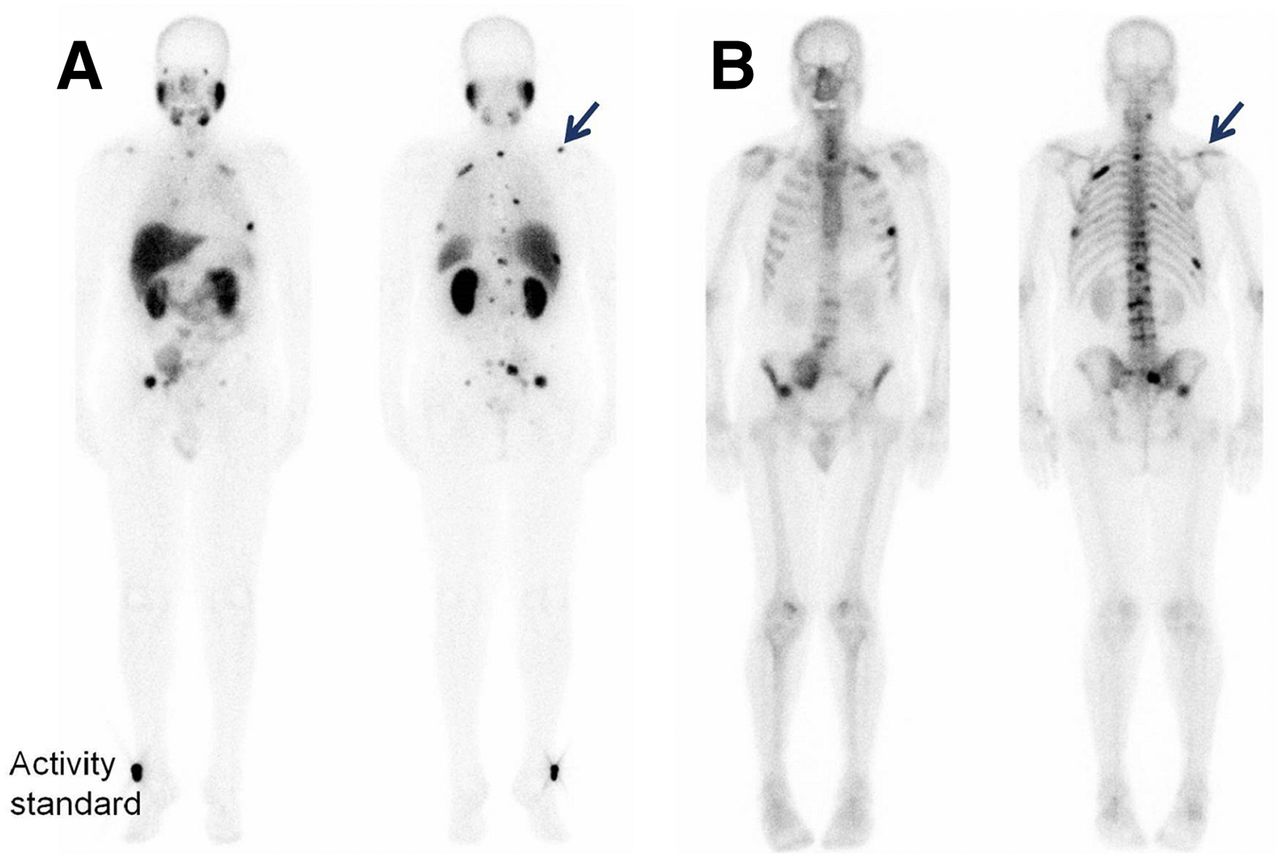
In 11 of 21 patients, lymphadenopathy or soft-tissue lesions were present in addition to bone lesions. For the 2 patients with PSMA-negative tumors, no visceral metastases or growing lymph nodes were reported during the follow-up period, and calculation of test quality criteria (such as sensitivity or specificity) was not reasonable. For the 19 patients with a PSMA-positive tumor phenotype, correlations with the whole set of clinical data (including other imaging modalities, such as MRI) (Fig. 4) and follow-up examinations were added to the consensus reading. PSMA-positive soft-tissue lesions did not show any false-positive findings. Heterogeneous PSMA expression and bone turnover in BS were present in 1 patient and led to various interpretations (Fig. 5); no gold standard could be defined for this patient during the consensus reading, but follow-up data implied that PSMA-positive and PSMA-negative lesions could occur within 1 patient.

Patient with intracerebral metastasis (A, green arrow) that was misinterpreted as skull lesion on planar scan (B, green arrow). Similarly, pulmonary lesion (C, red arrow) was also misinterpreted as rib lesion (B, red arrow). (A) MRI. (B) 99mTc-PSMA whole-body scan. (C) 99mTc-PSMA SPECT/CT.
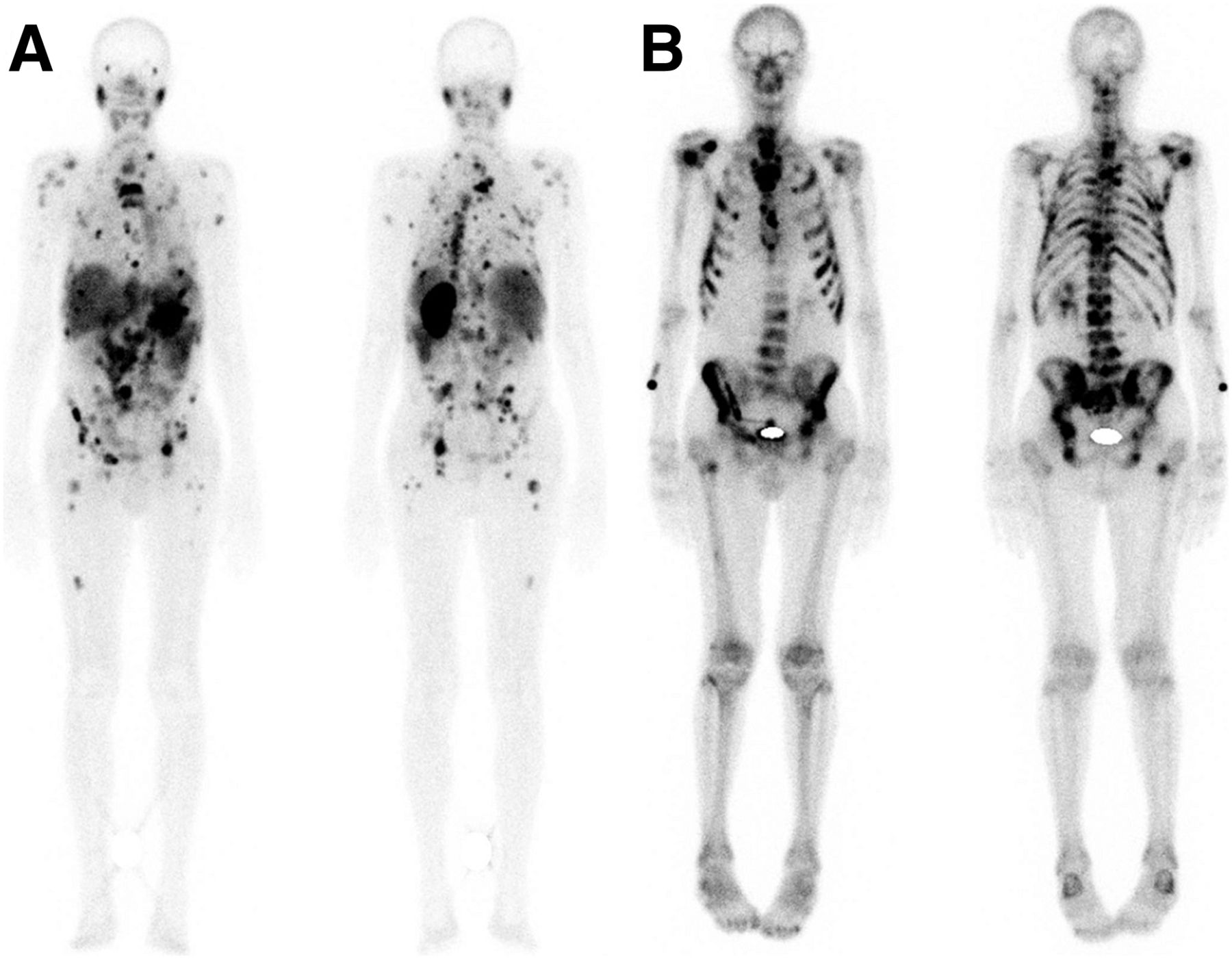
In patient with heterogeneously PSMA-expressing lesions, PSMA scanning (A) presented highly discordant lesion distribution pattern in comparison to 99mTc-MDP BS (B).
Tumor lesions in heavily burdened joints (e.g., knee and acromioclavicular joint) were more often misinterpreted as degenerative or equivocal lesions by 99mTc-MDP BS. After unmasking of morphologic imaging, these findings could successfully be verified; this sequence represents the actual clinical work flow. However, PSMA-positive or -negative findings in 99mTc-MIP-1427 scans were already correct without additional examinations. Figure 6 shows an example of a lesion that was interpreted as having a degenerative nature with 99mTc-MDP but as a typical tumor with 99mTc-MIP-1427.
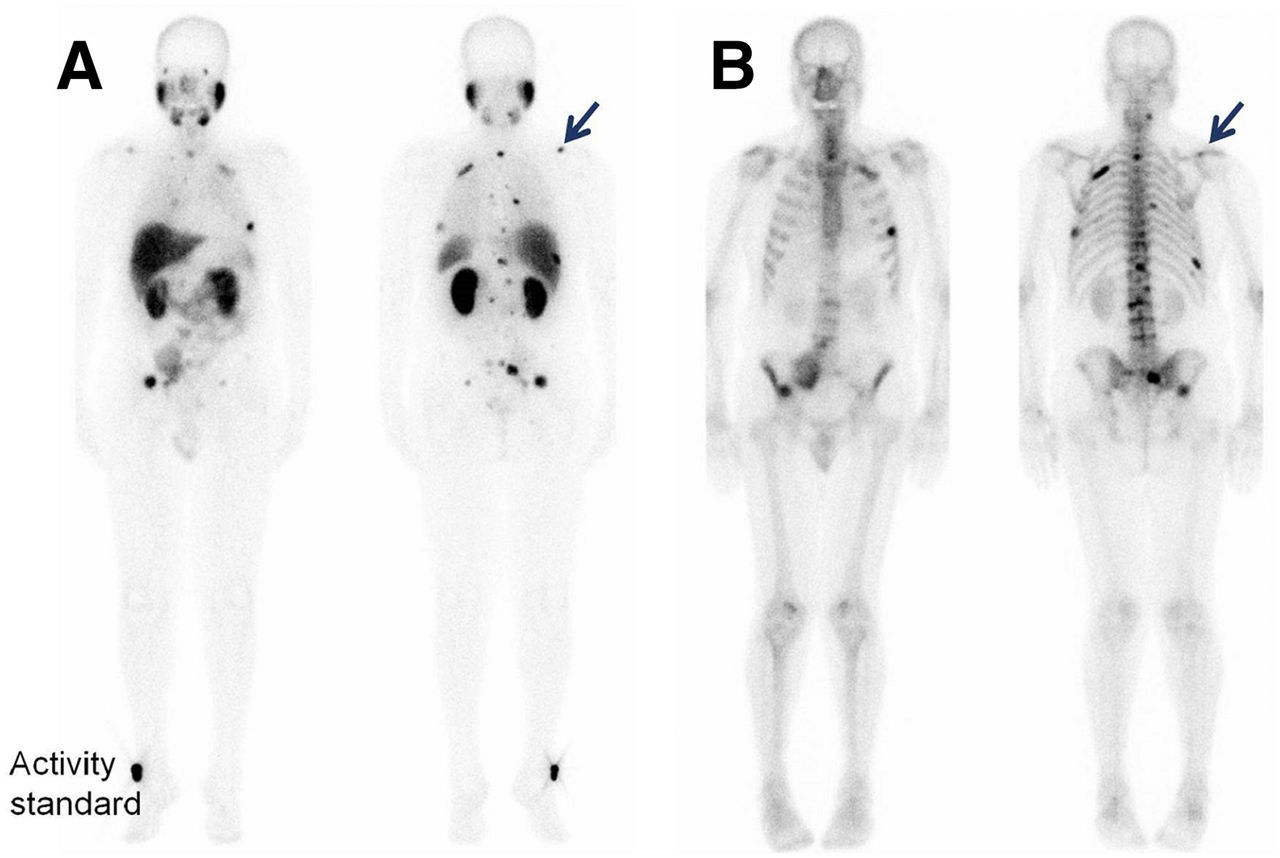
PSMA imaging (A, arrow) of typical malignant lesion that was scored as equivocal by BS (B, arrow).
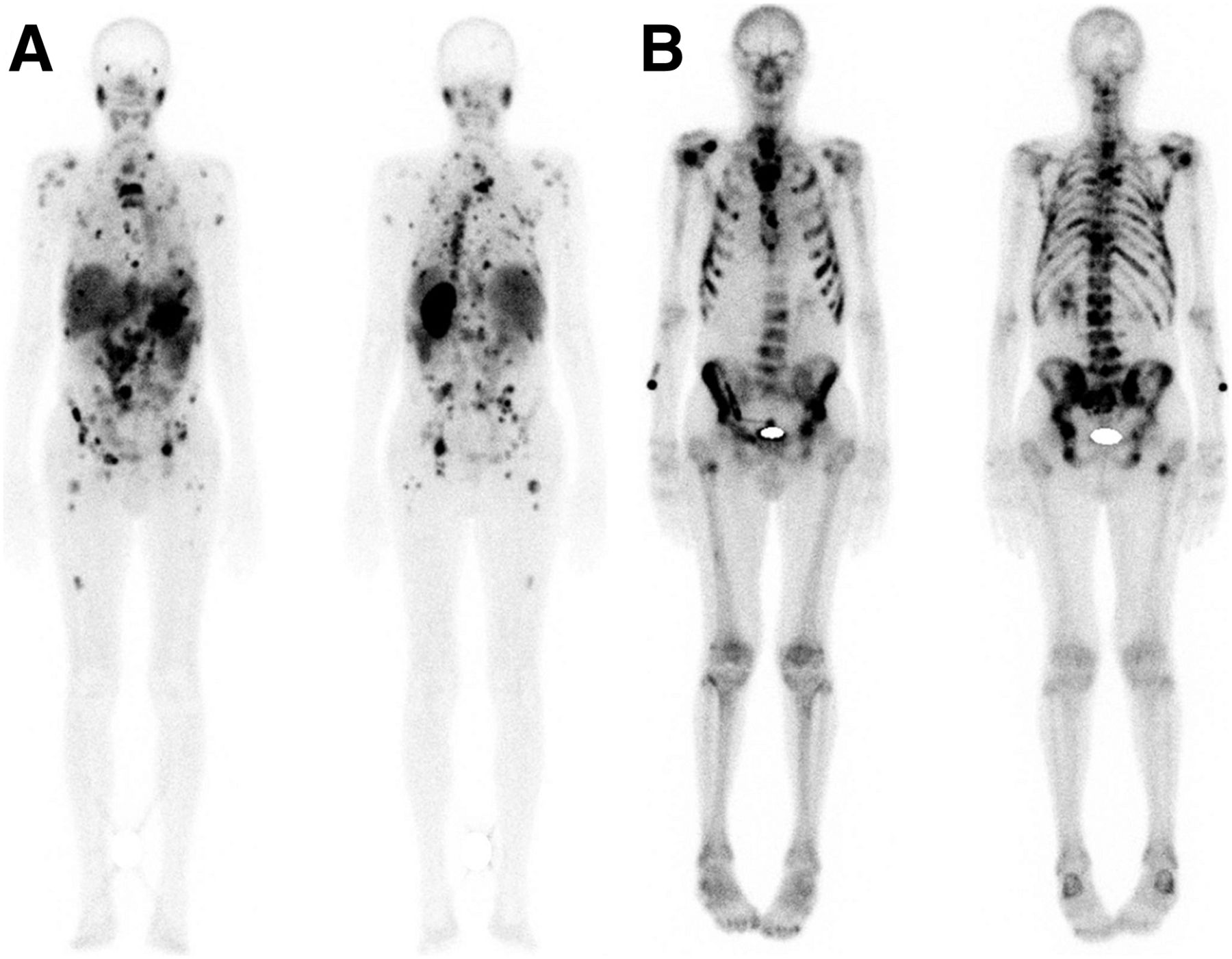
Special Case: Superscan Pattern
Seven patients had a superscan pattern on 99mTc-MDP BS, and all skeletal regions were considered to show tumor involvement. For these patients, PSMA imaging allowed the delineation of specific lesions in the peripheral limbs (Fig. 7). The treating physicians interpreted the additional information regarding the extent of red marrow involvement as helpful for estimating the red marrow reserve before initiating the next therapeutic treatment line instead of best supportive care. Improvements in clinical decisions for these patients were not assessed in this analysis.

Example of superscan pattern in patient imaged by PSMA scanning (A) and BS (B). Excessive tumor uptake in highly perfused red marrow resulted in at least relatively or even absolutely reduced uptake in salivary glands (PSMA scanning) and kidneys (BS).
DISCUSSION
The imaging findings for 99mTc-PSMA scanning and BS were evaluated in patients who had known bone metastases and were scheduled for an evaluation of PSMA-targeting therapy, which requires PSMA imaging in advance. With regard to this objective, PSMA scans were sufficient to determine whether patients had PSMA-positive or -negative tumor phenotypes.
Other groups have already reported comparisons between 68Ga-PSMA PET/CT and planar BS with (24) or without (25,26) routinely performed SPECT. These reports had some remarkable limitations; for example, the mean intervals between the imaging modalities were 21 d (range not reported) (25), up to 80 d (24), or up to 100 d (26). One advantage of our analysis was that both imaging procedures were performed within a median of 7 d (maximum, 10 d). However, this strict patient selection criterion was responsible for the smaller number of evaluable patients in our analysis—a limitation of our evaluation. Another limitation of the previous reports was the comparison of scintigraphy and PET. An advantage for the imaging modality with the higher inherent resolution and the better signal-to-noise ratio was predictable. Several researchers have already found an advantage of 18F-fluoride PET over multi–field-of-view SPECT/CT and planar 99mTc BS (11,13,27,28). Thus, for the comparison of PSMA PET/CT and 18F-fluoride PET/CT, only case reports are available (29,30). To our knowledge, our data represent the first comparison of 99mTc-PSMA imaging and 99mTc BS using the same imaging modality and parameters.
With regard to diagnostic performance, we found several advantages for the PSMA scan, at least for PSMA-positive tumors, which are present in most metastatic castration-resistant prostate cancer patients. Evaluation of the agreement of raters with the consensus reading indicated less reader-dependent influence on PSMA scanning than on 99mTc-MDP BS. PSMA imaging commonly reported typical benign or typical malignant lesions, showing a decrease in equivocal findings and a decrease in misclassifications of tumor spread (Table 2). The probability for equivocal findings decreased by using PSMA imaging. For example, benign lesions were found with a normal-to-equivocal ratio of 27.7:1 for PSMA and only 1.9:1 for MDP scanning (Table 2). On the basis of our results, every third lesion detected with 99mTc-MDP BS remained unclear. In current practice, equivocal findings require further evaluation with additional imaging of higher specificity, such as MRI focused on a particular lesion (23). Thus, the widespread use of PSMA scintigraphy may be useful for reducing additional examinations.
Our data suggested a relatively high sensitivity of PSMA imaging (92%) in comparison to 99mTc-MDP imaging (76% [BS]) for planar scans. These data are concordant with previously published data, although those were from intermodal comparisons of SPECT or SPECT/CT and PET/CT (26). Pyka et al. calculated sensitivities of 98.7%–100% for PET/CT (26).
For planar imaging, the specificity of 86% for PSMA was lower but not significantly different from that of 90% for BS. However, when 99mTc-based PSMA imaging was conducted and evaluated as SPECT/CT, the accuracy of our results was close to that of PSMA PET/CT. These results showed that the planar imaging technique was not optimal for correct tumor allocation. Especially for non–organ-confined tumor tracers, the improvement of hybrid imaging was highly pronounced. A benefit of SPECT/CT over planar BS was also reported previously (11,13,27,28). In contrast to these literature data, we did not observe a significant improvement of SPECT/CT (soft fusion) over planar images for BS. Therefore, a possible explanation is the high prevalence of true-positive bone metastases in comparison to only a few equivocal degenerative lesions in our cohort with advanced-stage disease.
In our group of patients with late-stage disease, visceral metastases—such as those in the liver, lung, and brain—were common. In addition to bone lesions, soft-tissue lesions were present in 11 of 21 patients. In patients with advanced-stage disease, it seems mandatory for PSMA imaging to be performed as SPECT/CT, covering the complete field of view, to cope with the challenge of correct lesion allocation to overlapping organs. In contrast, early-stage prostate cancer has a low probability for visceral metastases; SPECT/CT focused on the pelvis may be sufficient to identify and allocate lymph node metastases, whereas planar whole-body scans can be used to rule out distant metastases (14). The diagnosis of visceral metastases is important for prognosis and treatment stratification, as visceral metastases or lymph nodes of greater than 3 cm prohibit the application of 223RaCl2 and necessitate another therapeutic strategy (31).
In our retrospective patient population, 2 patients had insufficient PSMA uptake in lesions that were considered undoubtedly malignant in the reference examinations and follow-up. In these 2 patients, a weak or nonexistent PSMA-positive tumor phenotype may have been present. This finding is consistent with previously published data for PSMA-negative tumor sites in patients with biochemical relapse, irrespective of the PSA level (1,32). The demonstration of intense PSMA expression led to PSMA radioligand therapy. In contrast faint PSMA uptake, but intense uptake in BS, led to the decision that PSMA radioligand therapy was contraindicated. In such cases, a therapeutic regimen using bone-seeking drugs, such as 153Sm-EDTMP or 223RaCl2, may be more appropriate.
Because our patient collective was a cohort with very advanced disease and high pretest probability, true-positive and, consequently, highly specific findings were present disproportionately. In contrast, the similar sensitivity and specificity found with PSMA PET/CT were derived from patients with clinically more challenging conditions. The specificity of SPECT imaging in our cohort with a high tumor burden seems to be overestimated, especially because recently published data indicated the superiority of 68Ga-PSMA PET/CT over 99mTc-PSMA SPECT/CT, particularly in patients with low-volume disease or PSA relapse (33,34).
CONCLUSION
In this intraindividual comparison of PSMA scans and bone scans, the PSMA tracer presented a clear advantage in most patients. The amount of equivocal findings decreased for PSMA scans in comparison to bone scans. However, SPECT or SPECT/CT was pivotal for differentiating between bone metastases and extraosseous tumor lesions.
DISCLOSURE
99mTc-MIP-1427 was synthesized and used for compassionate-use applications with the permission of Molecular Insight Pharmaceuticals, Inc. (subsidiary of Progenics Pharmaceuticals, Inc.). There was no funding or other support from either Molecular Insight Pharmaceuticals, Inc., or Progenics Pharmaceuticals, Inc. Thomas Armor is a full-time employee of Progenics Pharmaceuticals, Inc. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 25, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 5, 2017.
- Accepted for publication January 9, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}