


Abstract
18F-FDG PET/CT is used for detecting cancer and monitoring cancer response to therapy. However, because of the variable rates of glucose metabolism, not all cancers are identified reliably. Sodium 18F was previously used for bone imaging and can be used as a PET/CT skeletal tracer. The combined administration of 18F and 18F-FDG in a single PET/CT study for cancer detection has not been reported to date. Methods: This is a prospective pilot study (November 2007–November 2008) of 14 patients with proven malignancy (6 sarcoma, 3 prostate cancer, 2 breast cancer, 1 colon cancer, 1 lung cancer, and 1 malignant paraganglioma) who underwent separate 18F PET/CT and 18F-FDG PET/CT and combined 18F/18F-FDG PET/CT scans for the evaluation of malignancy (a total of 3 scans each). There were 11 men and 3 women (age range, 19–75 y; average, 50.4 y). Results: Interpretation of the combined 18F/18F-FDG PET/CT scans compared favorably with that of the 18F-FDG PET/CT (no lesions missed) and the 18F PET/CT scans (only 1 skull lesion seen on an 18F PET/CT scan was missed on the corresponding combined scan). Through image processing, the combined 18F/18F-FDG scan yielded results for bone radiotracer uptake comparable to those of the 18F PET/CT scan performed separately. Conclusion: Our pilot-phase prospective trial demonstrates that the combined 18F/18F-FDG administration followed by a single PET/CT scan is feasible for cancer detection. This combined method opens the possibility for improved patient care and reduction in health care costs.
The role of 18F-FDG PET/CT is proven in a variety of cancers, including lymphoma, colorectal carcinoma, lung cancer, and melanoma, entities for which 18F-FDG PET/CT has changed the practice of oncology (1). However, because of the variable rates of glucose metabolism, not all malignant lesions are identified reliably, contributing to the overall limitations of 18F-FDG PET/CT (2).
Initial staging of patients diagnosed with certain cancers involves imaging with 18F-FDG PET/CT and 99mTc-methylenediphosphonate (99mTc-MDP) bone scintigraphy (3,4). Bone scintigraphy with sodium 18F was performed before the introduction of 99mTc-based agents, achieving excellent quality studies (5). 18F is a positron emitter, allowing for PET. Thus, imaging skeletal lesions with 18F PET/CT appears a logical approach for acquisition of highly sensitive and specific images.
Combining 18F and 18F-FDG in a single PET/CT scan for cancer detection has not been reported to date. However, if successful, such an approach has the potential to improve cancer diagnosis, staging, and possibly therapy monitoring. Therefore, we were prompted to prospectively evaluate the feasibility of the combined administration of 18F and 18F-FDG in a single PET/CT examination for pretherapy evaluation of extent of disease in patients with cancer.
MATERIALS AND METHODS
Preclinical Study
Approval was obtained from the Stanford University Administrative Panel on Laboratory Animal Care. Four mice were imaged with small-animal PET 1 h after tail vein administration of 18F (7,400 kBq [200 μCi]), 18F-FDG (7,400 kBq [200 μCi]), and combined 18F/18F-FDG (3,700 kBq [100 μCi] of each radiopharmaceutical) on separate days. Immediately after the combined 18F/18F-FDG PET, a micro-CT scan was obtained. Fiducial markers were placed for coregistration of the small-animal PET and micro-CT images. PET images were acquired using a microPET rodent R4 scanner (Concorde Microsystems). CT images were obtained using an eXplore RS MicroCT system (GE Healthcare). The CT data were used to create a bone mask that allowed the display of 18F/18F-FDG in the osseous structures on the PET scan. The image processing involved in this preclinical study required obtaining a bone mask from CT data, combining 18F/18F-FDG PET data with micro-CT data for coregistration (using fiducial markers), and displaying the 18F/18F-FDG uptake in the osseous structures on the PET scan. The processed images were compared with those obtained after separate 18F PET and 18F-FDG PET scans (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org).
Clinical Study
The clinical component was approved by the Stanford University Institutional Review Board and the Cancer Center Scientific Committee. A total of 14 consecutive patients (3 women and 11 men; mean age ± SD, 50.4 ± 17.8 y, age range, 19–75 y) were recruited for this pilot-phase study. Their diagnoses were soft-tissue sarcoma (4 patients), prostate cancer (3 patients), breast cancer (2 patients), osteosarcoma (2 patients), colon cancer (1 patient), lung cancer (1 patient), and malignant paraganglioma (1 patient). The patients underwent a separate 18F PET/CT scan and a separate 18F-FDG PET/CT scan, followed by a combined administration of 18F/18F-FDG for the third PET/CT scan. All 3 scans were obtained within a 2-wk interval.
PET/CT Protocols and Image Reconstruction
Whole-body PET/CT images were obtained in 2D mode using a GE Discovery LT scanner (GE Healthcare). The PET images were reconstructed with a standard iterative algorithm (ordered-subset expectation maximization, 2 iterative steps, 28 subsets). Images were reformatted into axial, coronal, and sagittal views and reviewed with the software provided by the manufacturer (Xeleris, version 2.0551; GE Medical Systems, Haifa, Israel). The prescribed radiotracer doses were 555 MBq (15 mCi) for 18F-FDG, 370 MBq (10 mCi) for 18F, and 555 MBq (15 mCi) of 18F-FDG + 185 MBq (5 mCi) of 18F for the combined (cocktail) scan. For the combined 18F/18F-FDG scans, the 2 radiotracers were delivered from the local cyclotron facility in separate syringes and administered sequentially, without delay between the 2. PET and CT images were obtained starting at 60 min after intravenous administration of the radiotracers.
Image Analysis
The 18F PET/CT, 18F-FDG PET/CT, and combined 18F/18F-FDG PET/CT scans were interpreted by 2 board-certified nuclear medicine readers unaware of the diagnosis and results of the other imaging studies. In addition to the separate interpretation of the 3 scans for each patient, the CT data from the combined 18F/18F-FDG scan were used to create a bone mask that allowed the display of 18F/18F-FDG in the osseous structures on the PET scan. The first step was to reformat the CT to the dimensions of the PET scan (i.e., 1282 × n from 5122 × n). The CT was interactively thresholded to eliminate all soft tissue but keep the bone densities. The nonzero values are made 1 to form a digital bone mask. The PET image multiplied by the mask left the bone image with a combined 18F/18F-FDG signal. These steps are illustrated in Figure 1. Each detected lesion was directly compared among the 3 PET/CT scans.
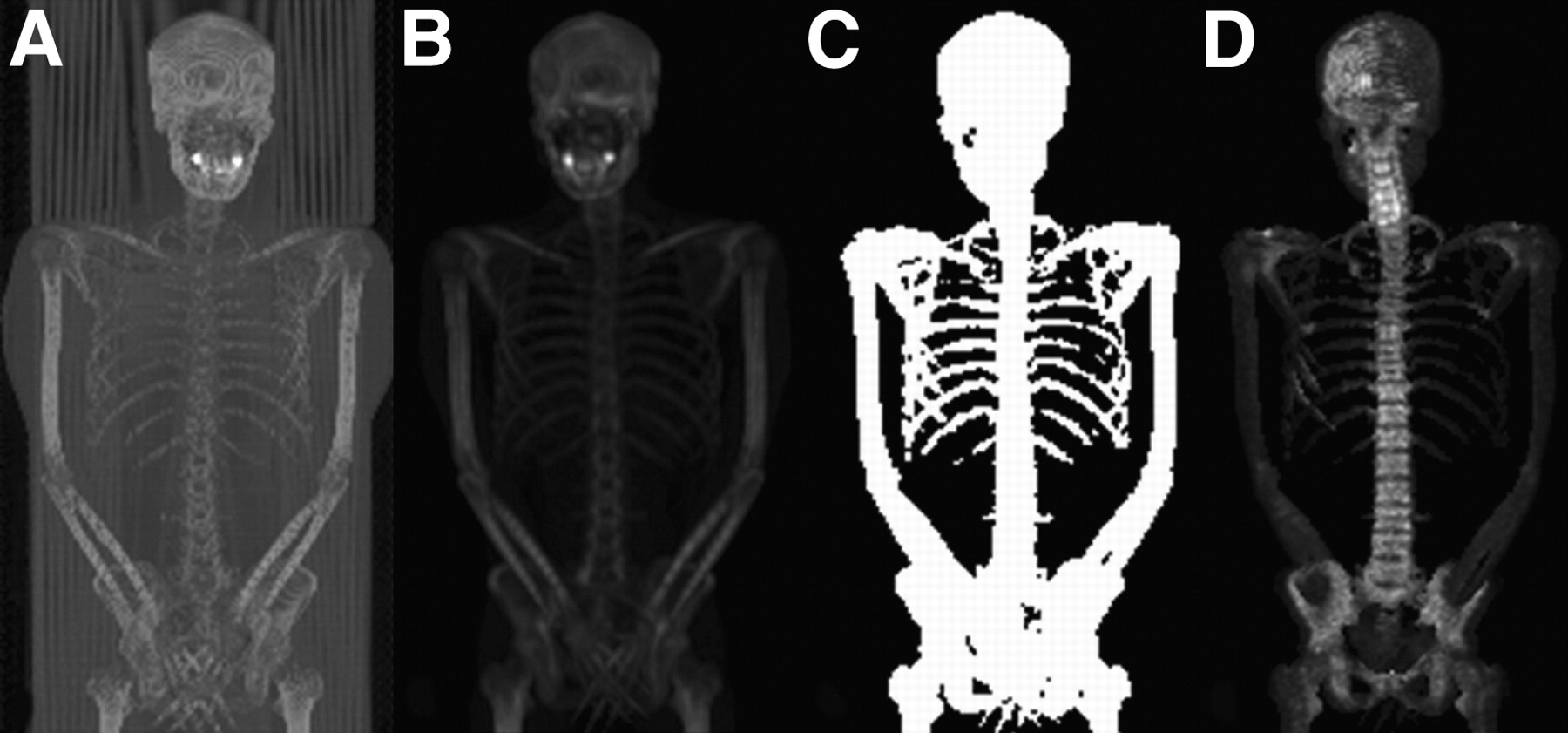
(A) The first step is to reformat CT image to dimensions of PET image. (B) Bed is eliminated by indicating most dependent part of body as image limit. (C) CT image is interactively thresholded to eliminate all soft tissue but keep bone densities. (D) PET image multiplied by mask leaves bone image with combined 18F/18F-FDG uptake.
RESULTS
Evaluation of Combined 18F/18F-FDG PET of Mice
We first investigated the feasibility of combined 18F/18F-FDG PET in mice. Through the aid of a bone mask from the micro-CT and using the fiducial markers for coregistration of CT and PET images, we processed the small-animal PET images of mice obtained after administration of combined 18F/18F-FDG to display only the combined radiotracer uptake in the skeleton. These images compared favorably with the images obtained from the 18F PET scan alone, supporting the translation of this method to a pilot clinical trial.
Evaluation of Combined 18F/18F-FDG PET/CT Versus 18F PET/CT in Humans
We then investigated bone images acquired with combined 18F/18F-FDG PET/CT versus 18F PET/CT performed separately. For this comparison, we used the image-processing algorithm validated by the mouse study and visual analysis of the 18F/18F-FDG PET/CT scans.
Through image processing, the combined 18F/18F-FDG scan yielded results for bone radiotracer uptake comparable to those of the 18F PET/CT scan performed separately. Thus, the combined 18F/18F-FDG cocktail tracer administration followed by single PET/CT appears to be feasible in this patient population referred for pretherapy evaluation of the extent of a known malignancy.
Visual analysis of the combined 18F/18F-FDG PET/CT scans without processing compared favorably with that of the 18F PET/CT scans. The results of this analysis are presented in Table 1. There was no disagreement (in this limited number of scans) between the readers. Only 1 skull lesion seen on an 18F scan was missed on the corresponding combined scan; however, this did not change the patient's management because other skeletal lesions were identified. Figure 2 shows a 44-y-old man with soft-tissue sarcoma (patient 6). Both 18F and combined 18F/18F-FDG scans can show more extensive skeletal disease, as does the case presented in Figure 3 (patient 4).

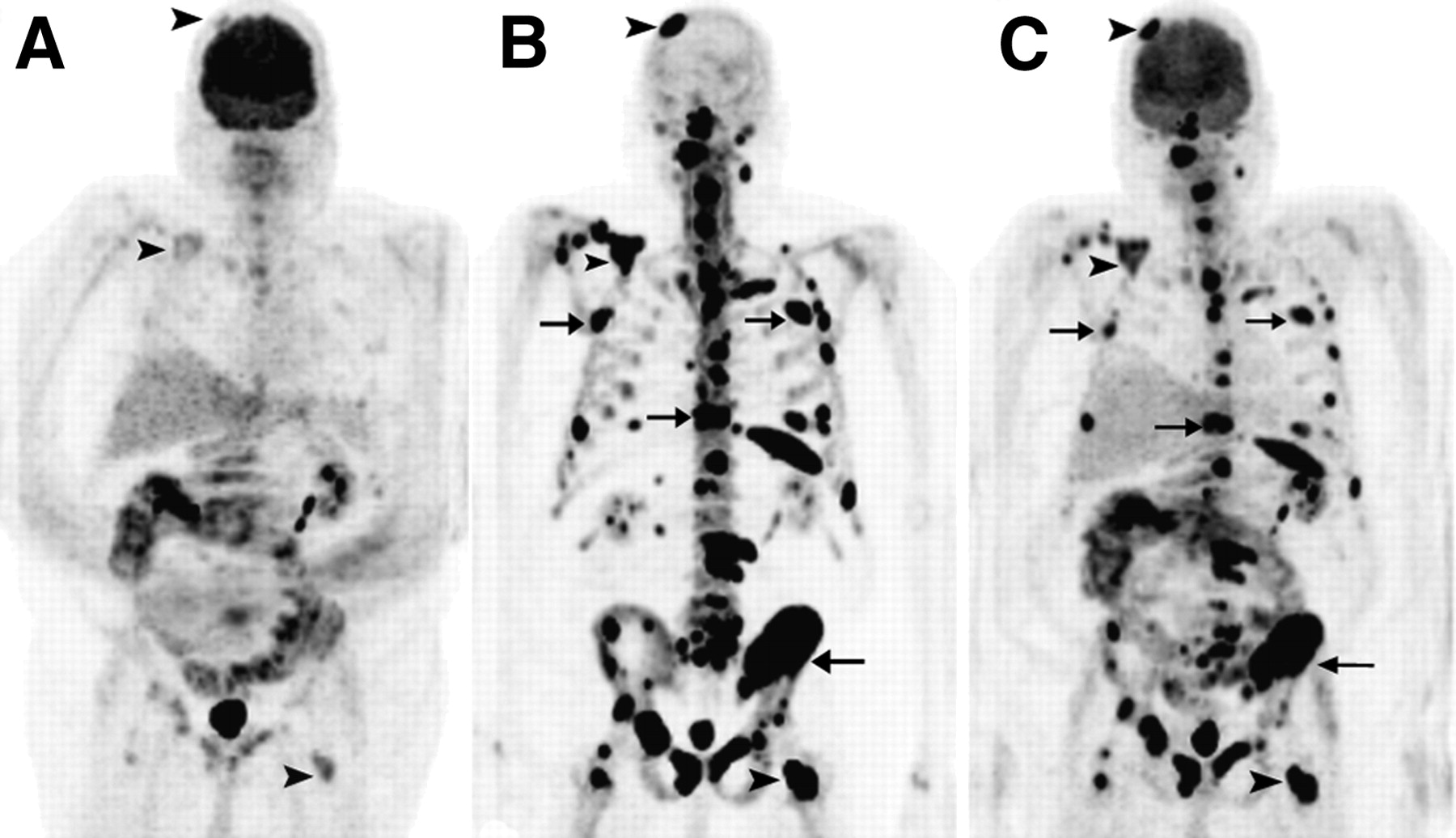
A 44-y-old man with soft-tissue sarcoma. (A) MIP image of 18F-FDG PET shows normal radiotracer uptake. (B) MIP image of 18F PET shows intense radiotracer uptake in skull lesion (arrow) and in T10 vertebra and right pubis (arrowheads). (C) Skull lesion is missed on MIP image of combined 18F/18F-FDG PET, but MIP image of combined 18F/18F-FDG PET shows skeletal lesions in T10 vertebra and right pubis noted on 18F PET (arrowheads). Skull lesion (arrow) is seen on transaxial CT (D) and 18F PET (E) but not on combined 18F/18F-FDG PET (F). Lesion in T10 vertebra (arrowhead) is seen on transaxial CT (G), 18F PET (H), and combined 18F/18F-FDG PET (I).
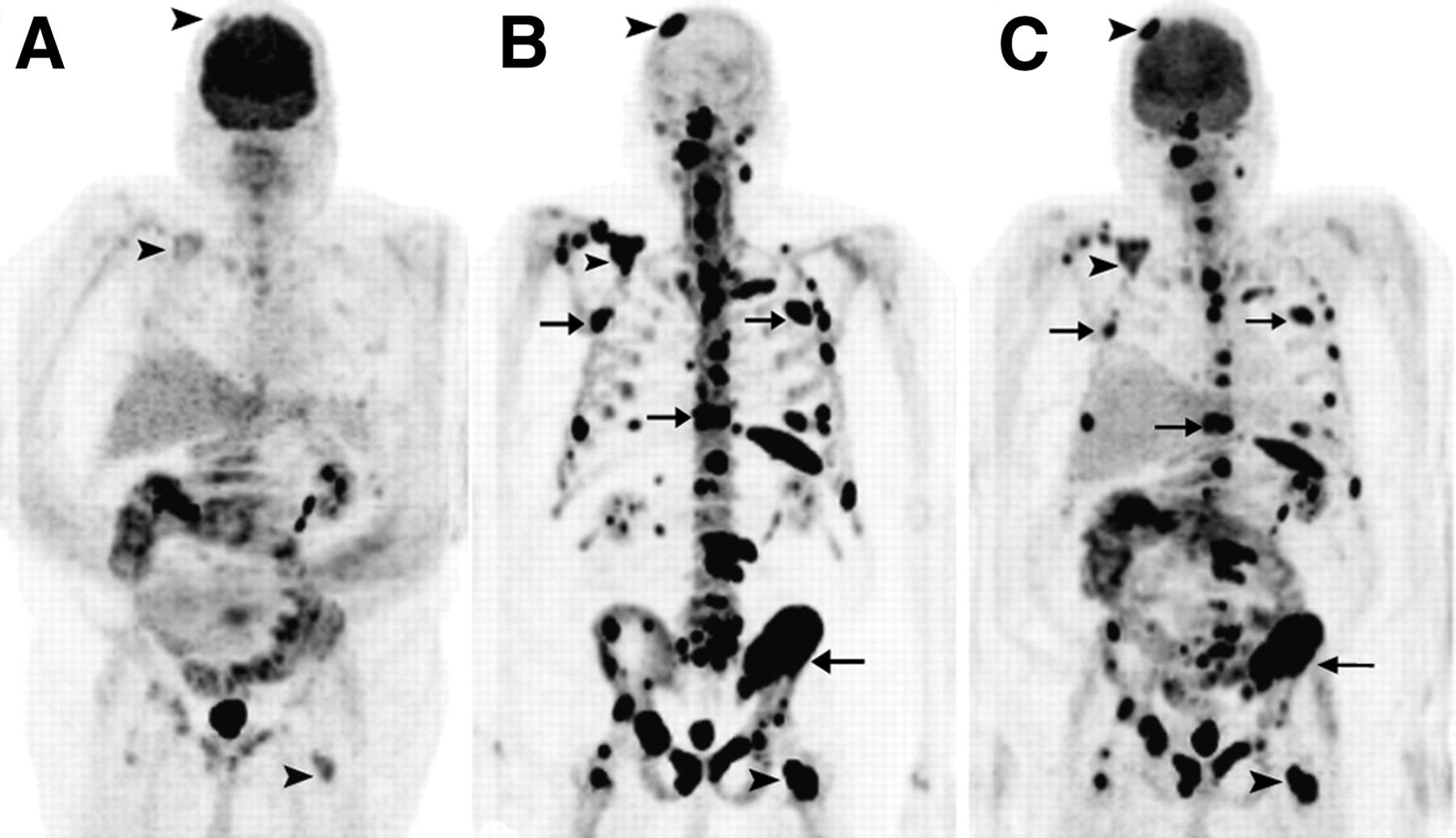
A 68-y-old man with colon cancer. (A) MIP image of 18F-FDG PET shows faint radiotracer uptake in several skeletal lesions (arrowheads). (B) MIP image of 18F PET shows intense radiotracer uptake in multiple bone lesions, including better visualization of lesions seen on 18F-FDG PET (arrowheads) and more extensive skeletal metastases (arrows). (C) MIP image of combined 18F/18F-FDG PET shows skeletal lesions noted on 18F PET (arrowheads).
Data from 14 Patients Included in Pilot Study and Results of PET/CT Scans
Evaluation of Combined 18F/18F-FDG PET/CT Versus 18F-FDG PET/CT in Humans
For all the patients enrolled, visual analysis of the combined 18F/18F-FDG PET/CT scans shows that 18F/18F-FDG images allow for accurate interpretation of the radiotracer uptake in the soft tissues, with findings identical to those of the 18F-FDG PET/CT scan alone (no lesions missed). The results of this analysis are also detailed in Table 1. There was no disagreement (in this limited number of scans) between the readers. In Figure 4, we present images of a 75-y-old man with prostate cancer (patient 1).

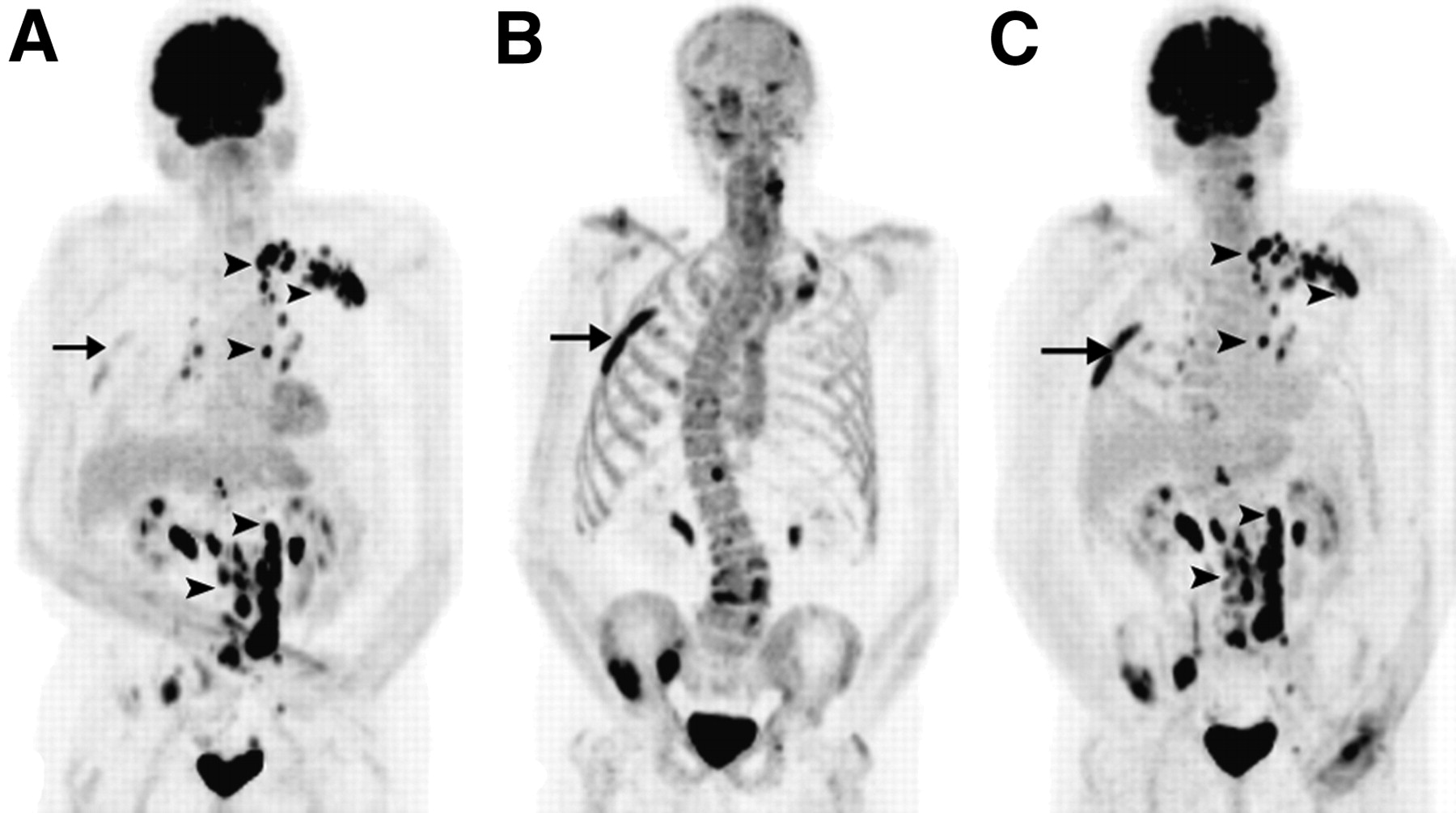
A 75-y-old man with prostate cancer. (A) MIP image of 18F-FDG PET shows lymph node metastases (arrowheads) and faint uptake in osseous lesions, such as a right rib (arrow). (B) MIP image of 18F PET shows intense radiotracer uptake in multiple bone lesions, including right rib lesion (arrow) seen on 18F-FDG PET. (C) MIP image of combined 18F/18F-FDG PET shows both lesions noted on 18F-FDG PET (arrowheads) and skeletal lesions noted on 18F PET (reference right rib lesion marked with arrow).
Evaluation of 18F PET/CT Versus 18F-FDG PET/CT in Humans
In 6 patients, the skeletal disease was more extensive on the 18F PET/CT scan than on the 18F-FDG PET/CT scan, whereas in another patient 18F PET/CT showed osseous metastases and 18F-FDG PET/CT findings were negative. The remaining 7 patients had no osseous metastases identified on the 18F PET/CT or the 18F-FDG PET/CT scans.
DISCUSSION
The spatial resolution of 99mTc-MDP skeletal scintigraphy and SPECT affects their sensitivity for detecting osseous metastases. Thus, the transition to the better resolution of PET/CT for detection of osseous metastases appears appealing, with the positron emitter 18F as the radiotracer of choice. 18F PET/CT was proved to be superior in bone lesion detection over a 99mTc-MDP bone scan and SPECT (6).
18F-FDG PET/CT contributes unique information about the metabolic activity of musculoskeletal lesions (7). However, several researchers concluded that 99mTc SPECT is superior to 18F-FDG PET in detecting bone metastases in breast cancer, and the sensitivity for osteoblastic lesions is limited with 18F-FDG PET/CT (8,9). For prostate cancer, evidence exists that 18F-FDG PET is less sensitive than bone scintigraphy. 18F-FDG PET is limited in the detection of osseous metastatic lesions but may be useful in the detection of metastatic nodal and soft-tissue disease (10). There is limited data relating to lymphoma, but the 18F-FDG PET scan seems to perform better than does the bone scan. An increasing body of evidence relates to the valuable role of an 18F-FDG PET scan in multiple myeloma, in which it is clearly better than the bone scan, presumably because 18F-FDG is identifying marrow-based disease at an early stage (11). The precise localization of a metastasis in the skeleton may be important with regard to the extent of the metabolic response induced (12). 18F-FDG PET may also have an important role in the imaging evaluation of patients with bone and soft-tissue sarcoma, including guiding biopsy, detecting local recurrence in amputation stumps, detecting metastatic disease, predicting and monitoring response to therapy, and assessing for prognosis (13).
The arguments mentioned here advocate for the use of both 18F PET/CT and 18F-FDG PET/CT for the initial staging of patients with cancer. In this prospective pilot study, we combined 2 scans in a single imaging procedure. To date, no clinical attempts to combine 18F and 18F-FDG administration in a single PET/CT examination have been reported. Hoegerle et al. reported the use of combined 18F and 18F-FDG administration for PET more than a decade ago, when PET/CT was not available (14). In their study, the images obtained after combined administration were not compared with separate 18F and 18F-FDG images obtained from each patient. Also, Hoegerle et al. attempted to use the skeletal 18F uptake as a surrogate for anatomic localization of abnormal 18F-FDG in the absence of fused PET and CT. With the availability of PET/CT, a cocktail approach allows for a new strategy for patient management not previously possible.
We successfully separated the metabolic skeletal uptake and allowed interpretation of the 18F and 18F-FDG tissue distribution, even though the 2 tracers were administered at the same time. This approach is based on the eventual biodistribution of the 18F nearly exclusively to the skeletal structures. We also showed that visual analysis of the combined cocktail 18F/18F-FDG PET/CT scan results in reliable diagnosis, compared with interpretation of the separate 18F PET/CT and 18F-FDG PET/CT scans.
In terms of radiation exposure for the patients, a 99mTc-MDP bone scan exposes patients to approximately 4.2 mSv (420 mrem) of radiation, and an 18F-FDG PET/CT scan exposes them to approximately 26.5 mSv (2,650 mrem) (0.03 mSv/MBq [110 mrem/mCi]) from 18F-FDG and 10 mSv [1,000 mrem] from the low-dose CT). This equals a total of 30.7 mSv (3,070 mrem) for the bone scan and 18F-FDG scan together. The combination of 18F PET/CT and 18F-FDG PET/CT in a single examination will result in a total of 31.5 mSv (3,150 mrem) (0.03 mSv/MBq [110 mrem/mCi] from 18F-FDG, 0.03 mSv/MBq [100 mrem/mCi] from 18F, and 10 mSv [1,000 mrem] from the low-dose CT). The newest PET/CT scanners have increased sensitivity, and the dose of 18F-FDG can be decreased to 370 MBq (10 mCi), resulting in a total radiation exposure of 26 mSv (2,600 mrem) from the combined 18F/18F-FDG PET/CT scan. Thus, instead of patients having to get separate SPECT and PET/CT studies, usually on different days, this strategy allows for 1 combined PET/CT study with potentially more utility, lower costs, lower radiation dose, and much greater patient convenience.
One limitation of our study is the small number of patients included in this pilot phase and the selection bias toward patients with known cancers. To come to statistically sound conclusions regarding the appropriate indications for the combined 18F/18F-FDG PET/CT study, further prospective enrollment of patients is needed. Also, analysis of the 3 different PET/CT scans might not be fully independent because of the short interval between interpretation of the 3 scans of the same patient. In addition, none of the 14 patients received therapy with bone marrow–stimulating agents before imaging. Bone marrow–stimulating therapy induces intense 18F-FDG uptake in the skeleton (15) and may play a confounding role in the evaluation of the osseous structures on the combined 18F/18F-FDG scan. This particular instance of evaluation of response to therapy by combined 18F/18F-FDG PET/CT needs to be separately evaluated in future studies. The bone-mask technique has the limitation of possible inclusion of the soft-tissue component of a lesion that is contiguous with the bone surface. Thus, it is possible that soft-tissue lesions can be captured and displayed as skeletal disease. Further iterations of the software used, with careful analysis of edge detection, are warranted to address this issue.
CONCLUSION
Our pilot-phase prospective trial demonstrated the feasibility of combined administration of 18F/18F-FDG in a single PET/CT examination for detection of malignancy. The use of a single examination opens the possibility for improved patient care. Both visual analysis of the combined 18F/18F-FDG PET/CT scan and interpretation of the processed images were accurate in this selected population with known cancers, who had been referred for determination of the extent of disease before therapy. Larger prospective trials are needed for a better understanding of the precise indications for the combined 18F/18F-FDG PET/CT method and for refinement of the image-processing algorithm.
Acknowledgments
We thank Dr. Fred Chin in the Cyclotron Facility, Lindee Burton, and all the technologists in the Nuclear Medicine Clinic. This research was supported in part by NCI ICMIC CA114747 (SSG), and the clinical studies were supported in part by the Doris Duke Foundation and Canary Foundation.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 21, 2008.
- Accepted for publication December 24, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Sodium Fluoride PET: History, Technical Feasibility, Mechanism of Action, Normal Biodistribution, and Diagnostic Performance in Bone Metastasis Detection Compared with Other Imaging Modalities
- Nanobody-Facilitated Multiparametric PET/MRI Phenotyping of Atherosclerosis
- The Role of 18F-Sodium Fluoride PET/CT Bone Scans in the Diagnosis of Metastatic Bone Disease from Breast and Prostate Cancer
- Bone-Targeted Imaging and Radionuclide Therapy in Prostate Cancer
- Prospective Comparison of 99mTc-MDP Scintigraphy, Combined 18F-NaF and 18F-FDG PET/CT, and Whole-Body MRI in Patients with Breast and Prostate Cancer
- Semiquantitative Analysis of the Biodistribution of the Combined 18F-NaF and 18F-FDG Administration for PET/CT Imaging
- An Approach to Breast Cancer Diagnosis via PET Imaging of Microcalcifications Using 18F-NaF
- Combined 18F-Fluoride and 18F-FDG PET/CT Scanning for Evaluation of Malignancy: Results of an International Multicenter Trial
- Combined 18F-Fluoride and 18F-FDG PET/CT Scanning for Evaluation of Malignancy: Results of an International Multicenter Trial
- Proof-of-Concept Study of Monitoring Cancer Drug Therapy with Cerenkov Luminescence Imaging
- Correlation of Inflammation Assessed by 18F-FDG PET, Active Mineral Deposition Assessed by 18F-Fluoride PET, and Vascular Calcification in Atherosclerotic Plaque: A Dual-Tracer PET/CT Study
- SNM Practice Guideline for Sodium 18F-Fluoride PET/CT Bone Scans 1.0
- Combined 18F-FDG and Fluoride Approach in PET/CT Imaging: Is There a Clinical Future?
- Reply: Combined 18F-FDG and Fluoride Approach in PET/CT Imaging: Is There a Clinical Future?
- Combined 18F-FDG and Fluoride Approach in PET/CT Imaging: Is There a Clinical Future?