


Abstract
The aim of this study was to determine if additional 18F-sodium fluoride PET/CT (NaF PET/CT) improves the prognostic accuracy in the initial staging of prostate cancer patients with normal bone scintigraphy undergoing prostatectomy. Methods: A prospective cohort study examined NaF PET/CT in intermediate- or high-risk prostate cancer with negative bone scintigraphy who were scheduled for prostatectomy. Biochemical response: PSA levels < 0.2 ng/mL at 6 wk and 6 mo postoperatively, PSA level ≥ 0.2 ng/mL was biochemical failure. Results: Eighty-one patients were included in the study; 75 patients (93%) achieved biochemical responses, 6 patients had biochemical failure. NaF PET/CT indicated bone metastasis in 1 patient (1.2%), was equivocal in 7 patients (8.6%), without bone metastases in 73 patients (90.1%). Eight patients with bone metastases or equivocal results on NaF PET/CT exhibited biochemical responses. All patients with biochemical failure had negative NaF PET/CT and bone scintigraphy for bone metastases. Conclusion: NaF PET/CT has no added value for bone staging in intermediate- and high-risk prostate cancer patients with normal bone scintigraphy results undergoing prostatectomy.
The European Association of Urology and National Cancer Comprehensive Network recommend bone scintigraphy for staging intermediate- and high-risk prostate cancer (PCa) patients (1,2). However, several studies have implied significantly improved diagnostic performance of 18F-sodium fluoride PET/CT (NaF PET/CT) over bone scintigraphy for the detection of bone metastases in PCa patients (3–5). The use of NaF PET/CT has been shown to change patient management by 12% when applied during initial staging (6). However, it remains to be shown whether the increased diagnostic performance afforded by NaF PET/CT correctly changes patient management and improves patient outcomes. We prospectively investigated whether additional NaF PET/CT improves the prognostic accuracy of the initial staging of patients with newly diagnosed, intermediate- and high-risk PCa without bone metastases on standard bone scintigraphy.
MATERIALS AND METHODS
Patients
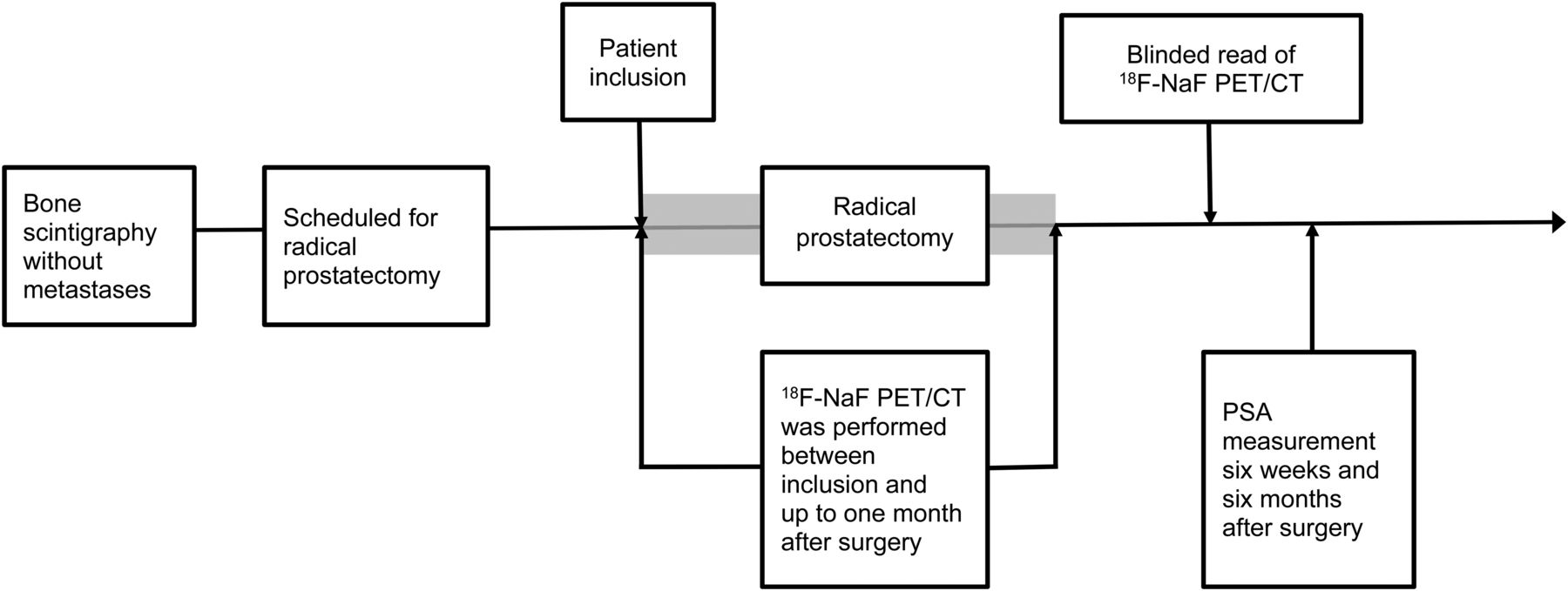
Consecutive patients from 2 sites were prospectively enrolled in this study. The recruitment period spanned from April 2015 to December 2016 (Regional Hospital West) and June 2015 to December 2016 (Aalborg University Hospital). During this time span, there were periods without patient screening due to limited scanner capacity or periods with scanner unavailability. The eligibility criteria were as follows: intermediate- or high-risk PCa according to the European Association of Urology classification (1), no bone metastases on standard bone scintigraphy reviewed by 2 readers according to institutional practices, no prior treatment for PCa, no history of malignancy other than PCa for 5 y before inclusion in the study, and planned radical prostatectomy (Fig. 1).
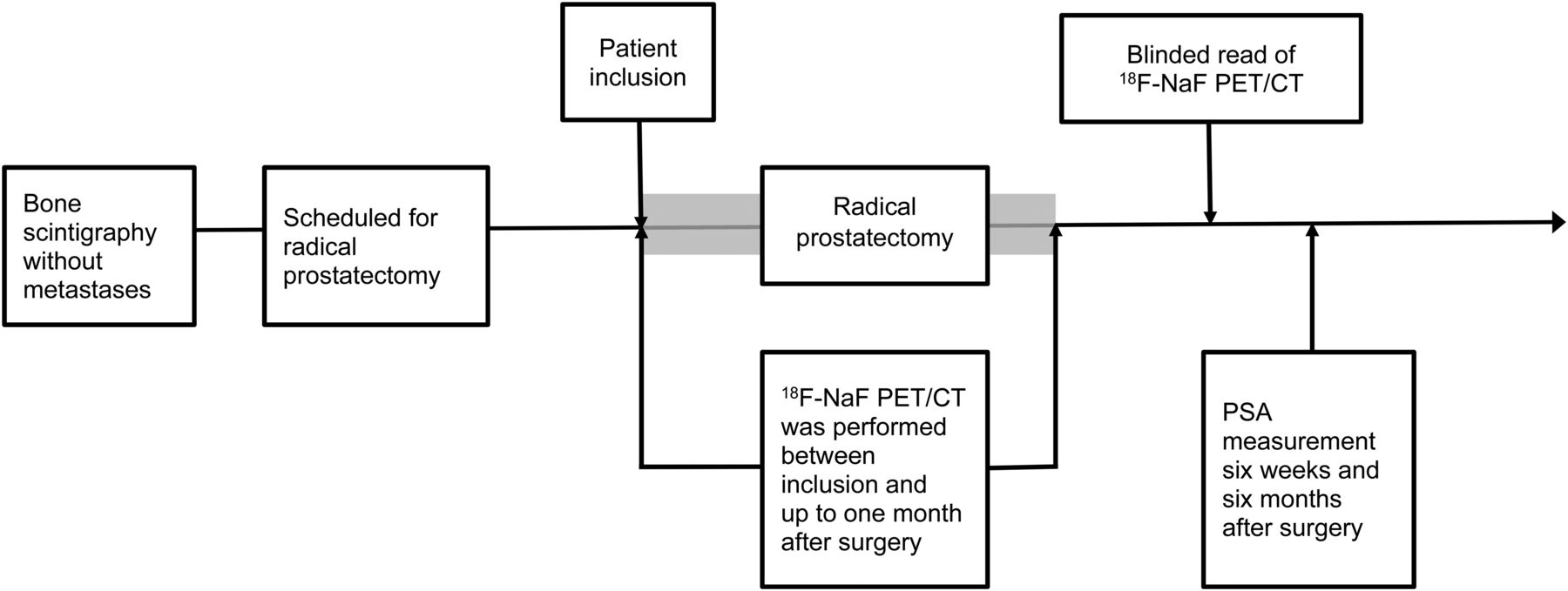
Outline of the study. Patients with negative standard imaging* who were undergoing radical prostatectomy were offered inclusion in the study. NaF PET/CT was performed between inclusion in the study and up to 1 mo after radical prostatectomy within the time span marked in gray. The results of the NaF PET/CT scan were unblinded 6 mo after radical prostatectomy. *Standard imaging consists of bone scintigraphy with/without SPECT/CT and diagnostic CT. RP = radical prostatectomy
NaF PET/CT
NaF PET/CT was performed in accordance with The Society of Nuclear Medicine and Molecular Imaging guidelines (7), in close conjunction with surgery (Fig. 1); the results of NaF PET/CT scans were not available to the treating urologist and were not used for clinical decision making.
Procedure for Evaluating NaF PET/CT
Two physicians, who before the evaluation of the first batch of study-related scans had clinical experience with 2,000+ and 2,500+ NaF PET/CTs, evaluated the NaF PET/CT scans. The observers were blinded to all clinical information, including the results of bone scintigraphy, except for the diagnosis of PCa. A consensus diagnosis was reached on a patient level as either no bone metastases, equivocal for bone metastases, or bone metastases present.
Clinical Data and Follow-up
Clinical data were retrieved from medical charts, pathology reports, and routine blood samples, including prostate-specific antigen (PSA) levels 6 wk and 6 mo after radical prostatectomy for all patients. Patients who achieved a PSA level < 0.2 ng/mL 6 wk and 6 mo after radical prostatectomy were defined as having a biochemical response and thus having no bone metastases (true M0) at the time of staging. Patients with a PSA level ≥ 0.2 ng/mL at 6 wk or at 6 mo after radical prostatectomy were categorized as having biochemical failure. Biochemical failure was not used to categorize true bone metastasis since elevated PSA levels could be caused by remnant PCa in other sites, for example, the prostatic bed or lymph nodes (8). Additional clinical and imaging follow-up focusing on bone metastases was conducted for 24 mo in patients with biochemical failure and in patients in whom NaF PET/CT was equivocal or suggested bone metastases.
Statistics
All variables were summarized using descriptive statistics (mean and range), and the proportions are provided along with the 95% confidence intervals. For the statistical analysis, STATA®11 (StataCorp LP, College Station, TX, USA) was used. This study was of an exploratory nature, and no formal sample size calculation was performed.
Approvals
This study complied with the Helsinki II Declaration and was approved by the local ethics committee (N-20140042) and the Danish Data Protection Agency. All patients provided informed consent to participate.
RESULTS
Patient Characteristics
Eighty-one patients were included in the study, and the majority had intermediate-risk PCa (Table 1). All patients were included at the time of staging except for 3 patients who had previously been in active surveillance. No patients received any systemic treatment for PCa before inclusion in this study or 6 mo after radical prostatectomy. A 6-mo follow-up after radical prostatectomy was available for all patients.
Patient Demographics and Clinical Characteristics
NaF PET/CT Findings and Outcome
NaF PET/CT showed bone metastasis in 1 patient (1.2%; 95% confidence interval: 0%–3.6%), equivocal findings in 7 patients (8.6%, 95% confidence interval: 2.5%–14.7%), and no pathologic findings in 73 patients (90.1%). At follow-up 6 mo after radical prostatectomy, 75 patients (93%) achieved a biochemical response, and 6 patients had biochemical failure. All 8 patients classified as having bone metastasis or equivocal results on NaF PET/CT had a biochemical response. The 6 patients with biochemical failure were NaF PET/CT negative for bone metastases (Table 2).
Diagnosis According to NaF PET/CT at Staging Compared with Outcome After Radical Prostatectomy
Follow-up
At 24 mo after radical prostatectomy, no bone metastases were identified in the group of patients with bone metastases or equivocal results on NaF PET/CT (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Likewise, no bone metastases were identified within 24 mo after radical prostatectomy in the group of patients with biochemical failure (Table 3).
Patients with PSA ≥ 0.1 ng/mL 6 Wk or 6 Mo After Radical Prostatectomy
DISCUSSION
NaF PET/CT has been introduced as a promising diagnostic method for assessing skeletal metastases, but studies of patient outcomes are scarce. In this study, NaF PET/CT did not improve outcomes in patients without metastases identified on standard bone scintigraphy.
The key findings, based on the concept of including NaF PET/CT findings in addition to negative bone scintigraphy findings, showed that NaF PET/CT did not show bone metastases in any patients with biochemical failure; this observation was correct in the present population because no bone metastases were detected after 24 mo of follow-up. Moreover, NaF PET/CT showed definite (n = 1) or unclear metastatic deposits in 7 patients, who all had postoperative PSA levels < 0.1 ng/mL that ruled out bone metastasis. Therefore, 1 patient could inappropriately have been deprived of curative treatment., the proportion of equivocal findings was 8.6%, which might seem high for experienced observers. However, the findings are consistent with previous studies conducted by Even-Sapir et al. (4), who reported that 7% of NaF PET/CTs were considered equivocal, and Löfgren et al., who reported 5% equivocal findings among experienced observers (9). In contrast, the proportion of equivocal findings (equivocal or probable) was 15% at the initial staging of PCa in the US National Oncology PET Registry study (6). Equivocal findings may lead to additional imaging and potentially lead to the improper withholding of treatment with a curative intent. In the present study, none of the equivocal findings were associated with biochemical failure. However, the present study also revealed that the likelihood of false positive NaF PET/CT findings was low, as emphasized by the narrow 95% confidence interval (0%–3.6%). The study did not allow any conclusions regarding if bone scintigraphy findings were added in patients with negative NaF PET/CT findings.
Previous studies investigating NaF PET/CT have primarily been dedicated to diagnostic test accuracy. In 2006, Even-Sapir demonstrated significantly improved diagnostic accuracy of NaF PET/CT in a head-to-head comparison with bone scintigraphy (4), whereas more recent diagnostic test accuracy studies have not entirely confirmed these results (9,10); in particular, false positive findings have been reported (5,11). NaF PET/CT has a high patient acceptance rate (12), and this technique may have an advantage over bone scintigraphy in terms of high patient throughput, thereby increasing patient capacity and the possibility of performing simultaneous contrast-enhanced CT as a “one-stop-shop” (13). Nevertheless, NaF PET/CT may be less cost-effective than bone scintigraphy (with or without SPECT/CT) (14), and access to a cyclotron and PET/CT scanner may be limited for various reasons.
The major focus in the US National Oncology PET Registry study was to document the impact of NaF PET/CT on patient management. A change in patient management was found in 12% of the patients (6); however, no evaluation of the appropriateness of the treatment changes was performed. Recently, Gauthé presented data showing the potential of NaF PET/CT to change patient management in 7% (2/27) of patients at initial staging (15). The changes in patient management induced by NaF PET/CT were considered appropriate at follow-up; however, no comparison to a standard PCa workup was conducted. These data are not in line with our findings.
The strength of the present study lies in the prospective design including a homogenous and representative group of newly diagnosed PCa patients eligible for radical prostatectomy. The present study had a true reference standard for the absence of bone metastases at the time of staging based on postoperative PSA levels, whereas the majority of studies on NaF PET/CT either focused on the detection rate without a proper reference or focused on the validation of bone metastases and not on the verification of a lack of bone metastases. The present design did not allow true verification of the localization of tumor cells in patients with biochemical failure (bone vs. nonbone); however, 24 mo of clinical follow-up and imaging did not reveal any false negative bone metastases.
In the present study, 7% of the patients had biochemical failure within 6 mo after radical prostatectomy. An investigation of biochemical recurrence at a later time point was not conducted. We retained this time frame to determine whether NaF PET/CT had potential to identify bone metastases not recognized on the initial bone scintigraphy before radical prostatectomy. This study did not allow for an evaluation of the false negative NaF PET/CT rate; thus, the lack of false negative NaF PET/CT in the present study cannot be generalized to other populations. Similarly, the present study represents a population with mainly intermediate-risk PCa suitable for surgery, and the findings cannot be extrapolated to high-risk or very high-risk populations.
CONCLUSION
NaF PET/CT did not provide any added prognostic value at the time of staging in patients with normal bone scintigraphy in terms of improved patient-related outcomes after radical prostatectomy.
DISCLOSURE
Helle D. Zacho received an unrestricted grant from the Danielsen Foundation. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTIONS: Does the use of 18F-sodium fluoride PET/CT (NaF PET/CT) in the initial staging of prostate cancer (PCa) improve the prognostic accuracy after radical prostatectomy in patients with normal bone scintigraphy?
PERTINENT FINDINGS: This was a 2-center, blinded, prospective cohort study of NaF PET/CT in 81 patients with intermediate- and high-risk PCa and negative bone scintigraphy who were scheduled for radical prostatectomy. Biochemical response was based on the postoperative PSA level. NaF PET/CT did not identify bone metastases in any patients with persistently elevated PSA levels after surgery but indicated bone metastases in 1 patient who had a PSA level < 0.1 ng/mL 6 mo after radical prostatectomy.
IMPLICATIONS FOR PATIENT CARE: NaF PET/CT has no added value in terms of prognostic accuracy after radical prostatectomy in patients with normal bone scintigraphy.
Footnotes
Published online May 30, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 22, 2019.
- Accepted for publication May 23, 2019.





{kind=link}