


Abstract
Bone metastases are common in patients with advanced breast cancer. Given the significant associated morbidity, the introduction of new, effective systemic therapies, and the improvement in survival time, early detection and response assessment of skeletal metastases have become even more important. Although planar bone scanning has recognized limitations, in particular, poor specificity in staging and response assessment, it continues to be the main method in current clinical practice for staging of the skeleton in patients at risk of bone metastases. However, the accuracy of bone scanning can be improved with the addition of SPECT/CT. There have been reported improvements in sensitivity and specificity for staging of the skeleton with either bone-specific PET/CT tracers, such as 18F-NaF, or tumor-specific tracers, such as 18F-FDG, although these methods are less widely available and more costly. There is a paucity of data on the use of 18F-NaF PET/CT for response assessment in breast cancer, but there is increasing evidence that 18F-FDG PET/CT may improve on current methods in this regard. At the same time, interest and experience in using whole-body morphologic MRI augmented with diffusion-weighted imaging for both staging and response assessment in the skeleton have been increasing. However, data on comparisons of these methods with PET methods to determine the best technique for current clinical practice or for clinical trials are insufficient. There are early data supporting the use 18F-FDG PET/MRI to assess malignant disease in the skeleton, with the possibility of taking advantage of the synergies offered by combining morphologic, physiologic, and metabolic imaging.
The skeleton is the most common site for metastases from breast cancer, being affected in approximately 50%–70% of patients with relapse (1,2), and is the sole site of disease in 28%–44% (3,4). Skeletal metastases cause significant morbidity, including pain, fractures, hypercalcemia, and spinal cord compression; patients in whom disease is confined to the skeleton have the greatest risk of skeleton-related events (5). The median survival of patients with disease confined to the skeleton is relatively long compared with that of patients with visceral disease (2.2 y vs. 5.5 mo; P < 0.001) (3); therefore, cumulative morbidity and health care costs from bone metastases are high. With the arrival of effective novel therapies, it has become even more important to detect bone metastases at an early stage to minimize skeleton-related events and to allow the determination of a response as early as possible to limit toxicity and accelerate the therapeutic transition in nonresponding patients.
Imaging has always played a key role in the diagnosis of bone metastases in breast cancer and planar 99mTc-diphosphonate bone scanning (BS) remains widely used, its lack of specificity has been improved with the addition of SPECT and SPECT/CT. At the same time, there has been an increase in the use of other hybrid techniques for imaging of the skeleton (e.g., PET/CT) as well as whole-body MRI techniques, which have improved sensitivity. Despite improved accuracy in staging of the skeleton, evidence of efficacy and consensus regarding effective monitoring of a treatment response are lacking. Although radiographs have been used historically to determine a response by lesion resolution or sclerosis (6,7), this method has been recognized as being insensitive and may take at least 6 mo to yield a confident assessment of a response.
RECIST 1.1 (8) depends primarily on a change in longitudinal dimension in nodal and visceral disease. Only lytic bone metastases with soft-tissue masses of greater than 1 cm (an infrequent finding) are deemed measureable; although the use of BS, PET, or radiography for confirmation of a complete response is permitted, most bone metastases are not assessable. A more pragmatic approach involving a combination of imaging results from BS, CT, and radiography has been shown to provide a better prediction of progression-free survival and overall survival than World Health Organization criteria but has not yet gained wide acceptance (9). When these criteria were prospectively tested in 29 breast cancer patients with bone-only metastases, they were found to predict progression-free survival at 6 mo but not 3 mo, similar to the World Health Organization criteria (10).
The purpose of this review is to update the current status of imaging, particularly BS, 18F-FDG PET, and 18F-NaF PET, for detection and therapy response monitoring of bone metastases from breast cancer. Some potential future methods that show promise are also discussed.
PATHOPHYSIOLOGY OF BONE METASTASES
Paget suggested that metastases depend on cross talk between cancer cells (“seeds”) and specific organ microenvironments (“the soil”) (11). Bone marrow stromal cells attract tumor cells through the expression of chemotactic molecules and provide the tumor cells with an environment in which to grow. The abilities of cancer cells to adhere to bone matrix and to promote osteoclast maturation and activity are important in the development of bone metastases. Untreated bone lesions exist on a spectrum between predominantly osteoblastic (e.g., prostate cancer–related skeletal metastases) and osteolytic (e.g., myeloma), but breast cancer metastases can vary between the two or can be mixed in the same patient. The phenotypes have different effects on bones and may influence the selection of the optimal imaging modality for demonstrating the lesions.
In bone metastases that are predominantly osteolytic, parathyroid hormone–related protein, derived from cancer cells, stimulates production of the receptor activator of nuclear factor κB ligand; the latter leads to osteoclast maturation and bone resorption that outstrips attempts at osteoblastic bone formation and repair (12). Of relevance, a human monoclonal antibody to the receptor activator of nuclear factor κB ligand, denosumab, is currently being used in the treatment of cancer-related bone disease, and bisphosphonates exert some of their effect by inhibiting osteoclasts. Tumor cells can also secrete several growth factors that stimulate bone formation through increased osteoblastic activity (12). This primary osteoblastic activity may be indistinguishable on imaging from reactive and reparative osteoblastic activity that follows successful treatment of both osteolytic and osteoblastic bone metastases.
BONE SCINTIGRAPHY, INCLUDING SPECT AND SPECT/CT
BS has been used for decades as the primary method for staging and response assessment of skeletal metastases. Despite recognized limitations with regard to diagnostic specificity and both sensitivity and specificity in measuring a treatment response, BS remains in widespread use in clinical practice. Abnormal accumulation of 99mTc-labeled diphosphonates is related to changes in local blood flow and osteoblastic activity (13), events that are secondary in most bone metastases that are seeded in the bone marrow. Although BS is still considered a sensitive technique, methods that can detect tumor in the bone marrow, such as 18F-FDG PET and MRI, before osteoblastic activity is present—particularly in predominantly osteolytic disease—have been shown to be even more sensitive (14–18). The mechanism of accumulation means that the uptake of 99mTc-labeled diphosphonates is not specific for metastatic disease and may also make the differentiation of increased reparative osteoblastic activity after successful treatment (flare) from unresponsive progressive disease impossible for several months.
For staging of the skeleton, some improvements in sensitivity and specificity were observed when BS was augmented with SPECT (19–21). Further gains in sensitivity and, especially, in specificity and diagnostic confidence were apparent with SPECT/CT (22–25) because of the greater contrast resolution of SPECT coupled with the ability to reduce false-positive diagnoses of metastases through correlation with the morphologic appearance of lesions on CT.
For response assessment, the limitations of BS in defining response or nonresponse have been recognized for many years, with only 52% of responders showing scintigraphic improvement and 62% of nonresponders showing scintigraphic deterioration at 6–8 mo in an early study (26). The problem of the flare phenomenon, which makes the differentiation of progression from a temporary healing osteoblastic response to successful therapy difficult for 3–6 mo, has also been recognized for many years and has been described after chemotherapy and endocrine therapy in breast cancer (27,28). However, if serial scans confirm a flare, then a successful response can be predicted (29). Nevertheless, a time lag of 3–6 mo for accurate response evaluation from the start of treatment limits the utility of BS for response evaluation in routine clinical practice or as a progression endpoint in clinical trials, and we are not aware of evidence that shows an improvement through the addition of SPECT or SPECT/CT in such situations.
18F-NaF PET
18F-NaF was first described as a bone-specific tracer in 1962 (30), but not until the availability of modern PET and, subsequently, PET/CT scanners was it possible to take advantage of some of the superior physiologic and pharmacokinetic characteristics of this tracer compared with the 99mTc-based tracers used in conventional BS. The pharmacokinetics of 18F-NaF, including nearly 100% first-pass extraction into bone, negligible protein binding, and rapid renal excretion in hydrated subjects, allow early imaging of the skeleton—at less than 1 h after injection—with high contrast and spatial resolution (13). The mechanism of uptake into bone is similar to that of 99mTc diphosphonates, being related to local blood flow and osteoblastic activity, with rapid initial uptake and eventual incorporation into bone mineral as fluoroapatite.
Early studies showed the net clearance of 18F-NaF in breast cancer skeletal metastases to be 3–10 times greater than that in normal bone, with the ability to detect osteolytic and osteosclerotic metastases (31,32). PET and PET/CT studies in metastatic breast cancer have shown improved diagnostic accuracy compared with that of BS (33–37) or CT (38), and 18F-NaF PET/CT has shown higher diagnostic accuracy than 18F-NaF PET without the CT component (35). Similar improvements in diagnostic accuracy over that of BS with or without SPECT have been replicated in other cancers, including prostate cancer (39–41), lung cancer (42), renal cancer (43), bladder cancer (44), and hepatocellular carcinoma (45). Prospective studies with 18F-NaF for the detection of bone metastases are in progress (NCT00882609 (46) and NCT01930812 (47)). A National Oncology PET Registry trial assessed the impact of 18F-NaF PET/CT on the management of patients with cancer other than prostate cancer and included 781 patients with breast cancer (48). For the breast cancer patients, management changed for 24% of those with suspected first osseous metastasis and for 60% of those with suspected progression of osseous metastasis.
Although we are not aware of prospective data on the use of 18F-NaF PET/CT for the assessment of a treatment response in skeletal metastases from breast cancer, the feasibility of performing kinetic analysis of 18F-NaF uptake in metastases and normal bone in patients with breast cancer has been confirmed (49), and preliminary studies in metastatic prostate cancer have shown promise (50,51). A further National Oncology PET Registry trial assessed the impact of 18F-NaF PET/CT used for treatment monitoring and included 476 patients with breast cancer (52). The frequency of a change in the management plan for patients with breast cancer was 39.3%. Of note, there have been preliminary reports of a flare phenomenon with 18F-NaF PET after both chemotherapy and endocrine therapy in breast cancer; therefore, the timing of follow-up scans may be crucial (Figs. 1–3) (53,54).
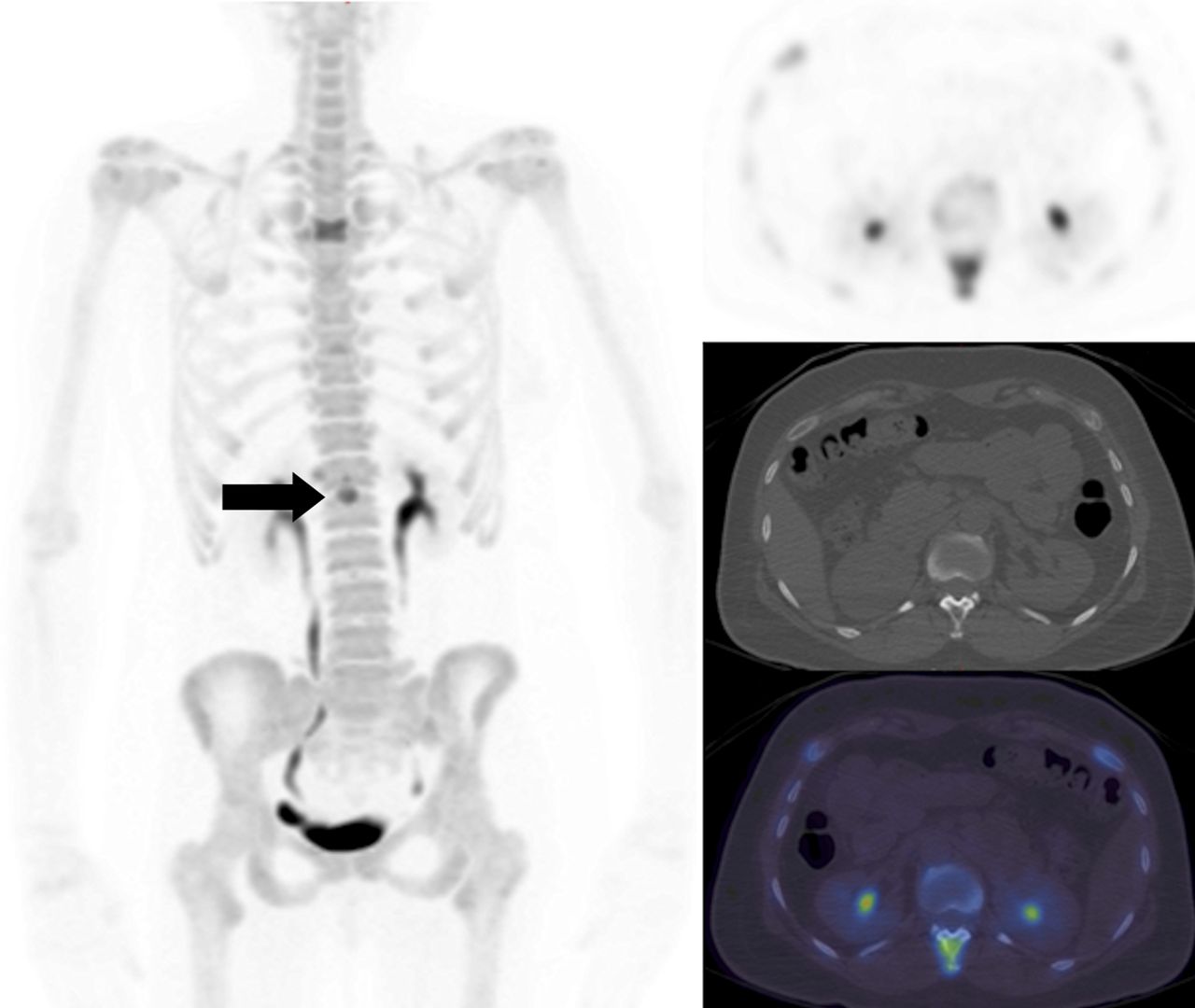
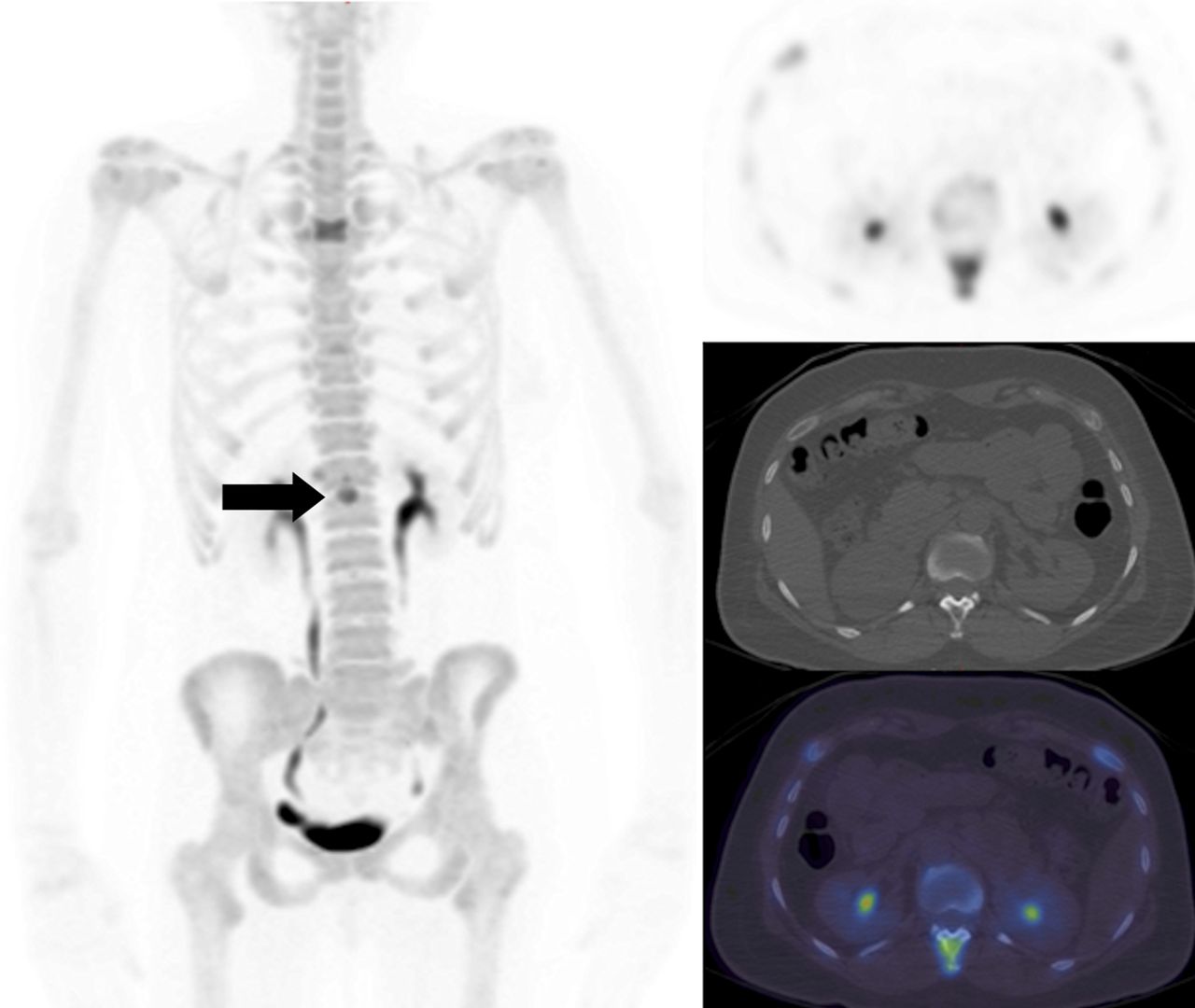
A 48-y-old woman with metastatic breast cancer. Maximum-intensity projection 18F-NaF (left) and axial 18F-NaF PET, CT, and fused PET/CT slices (right, from top to bottom) at level of T12 showing a metastasis in the spinous process (arrow). A further metastasis is visible at T4.
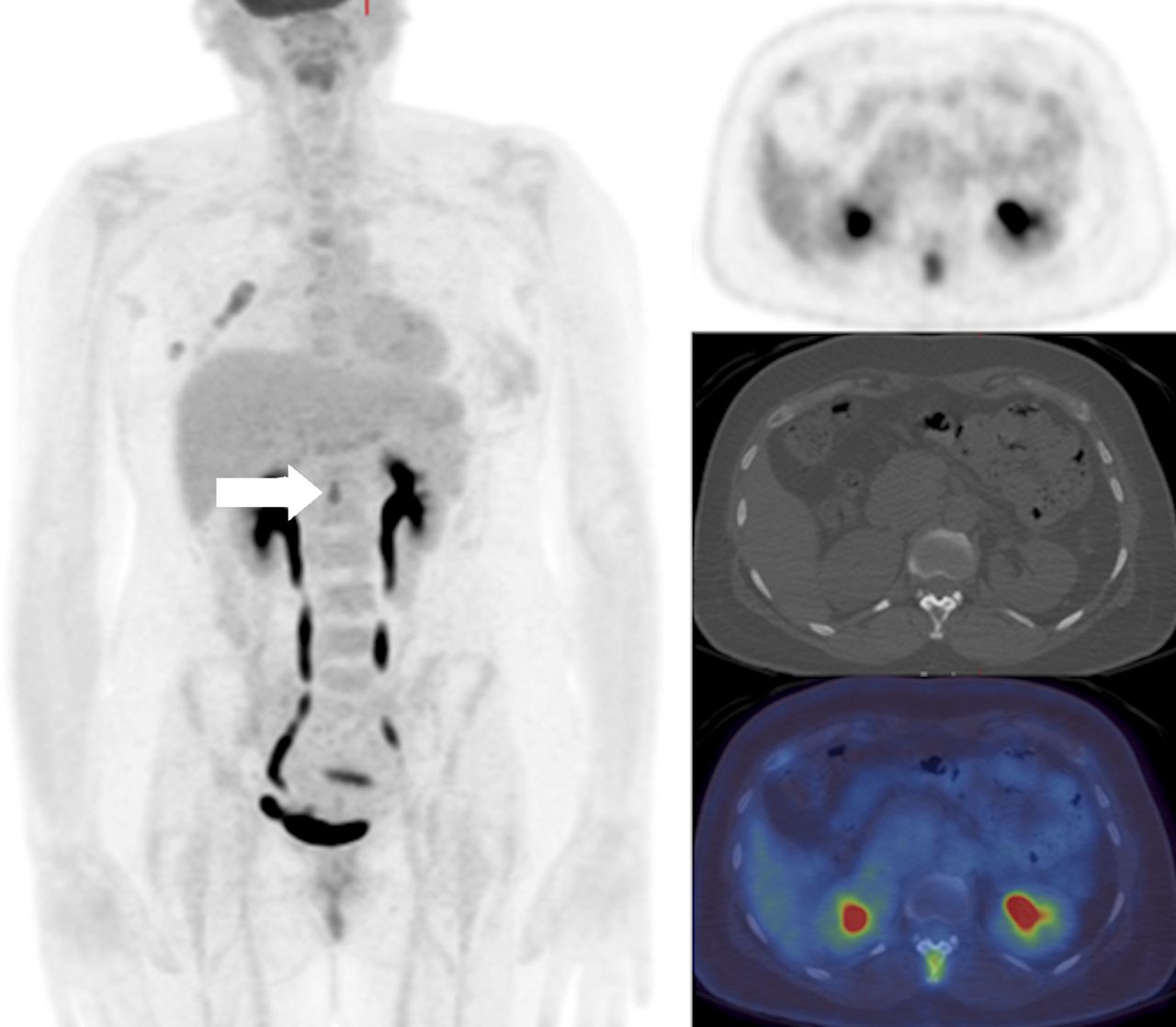
Maximum-intensity projection 18F-FDG PET/CT and axial 18F-FDG PET, CT, and fused PET/CT slices (right, from top to bottom) showing abnormal uptake in T12 spinous process (arrow) and at T4 in a 48-y-old woman with metastatic breast cancer (same patient as in Fig. 1).
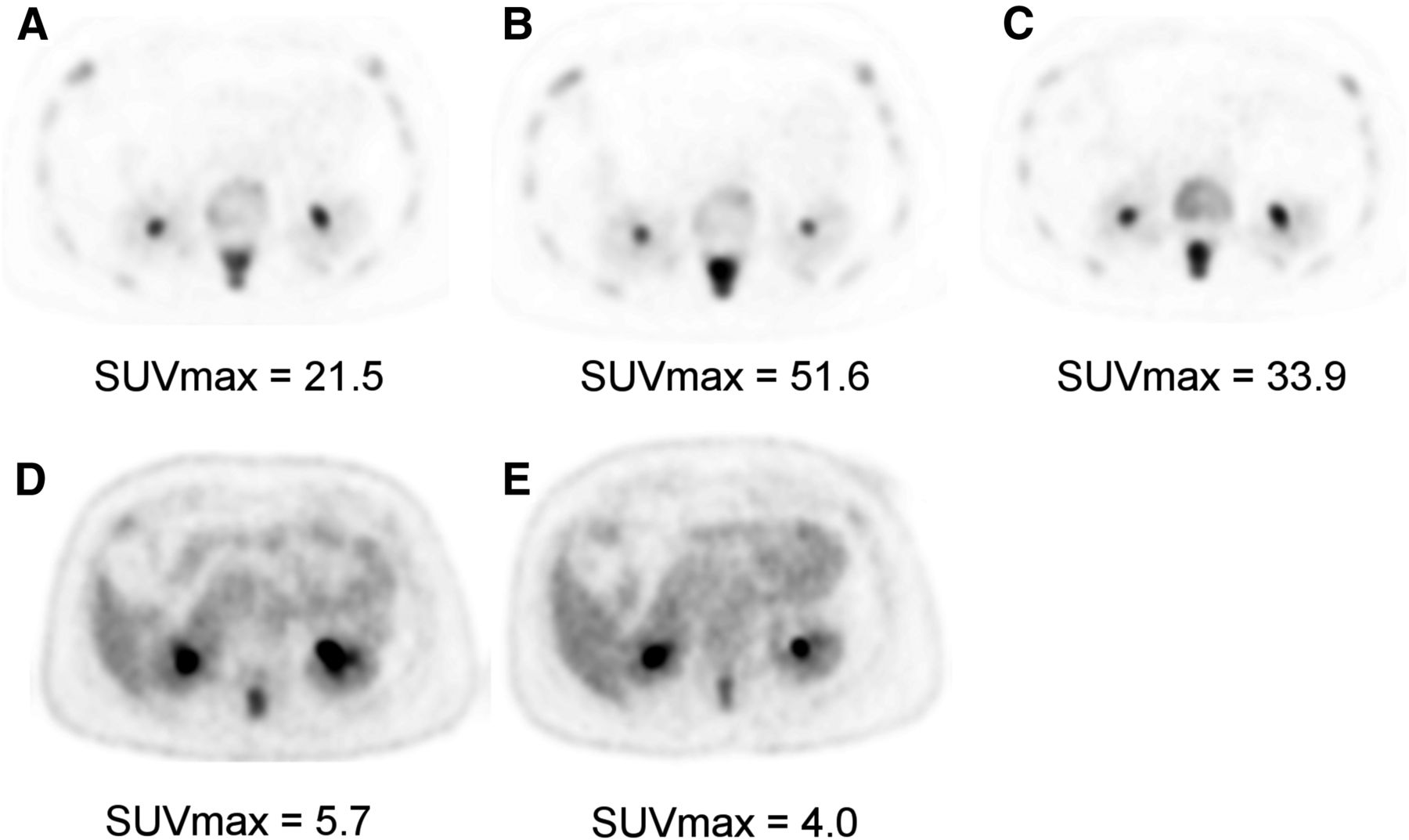
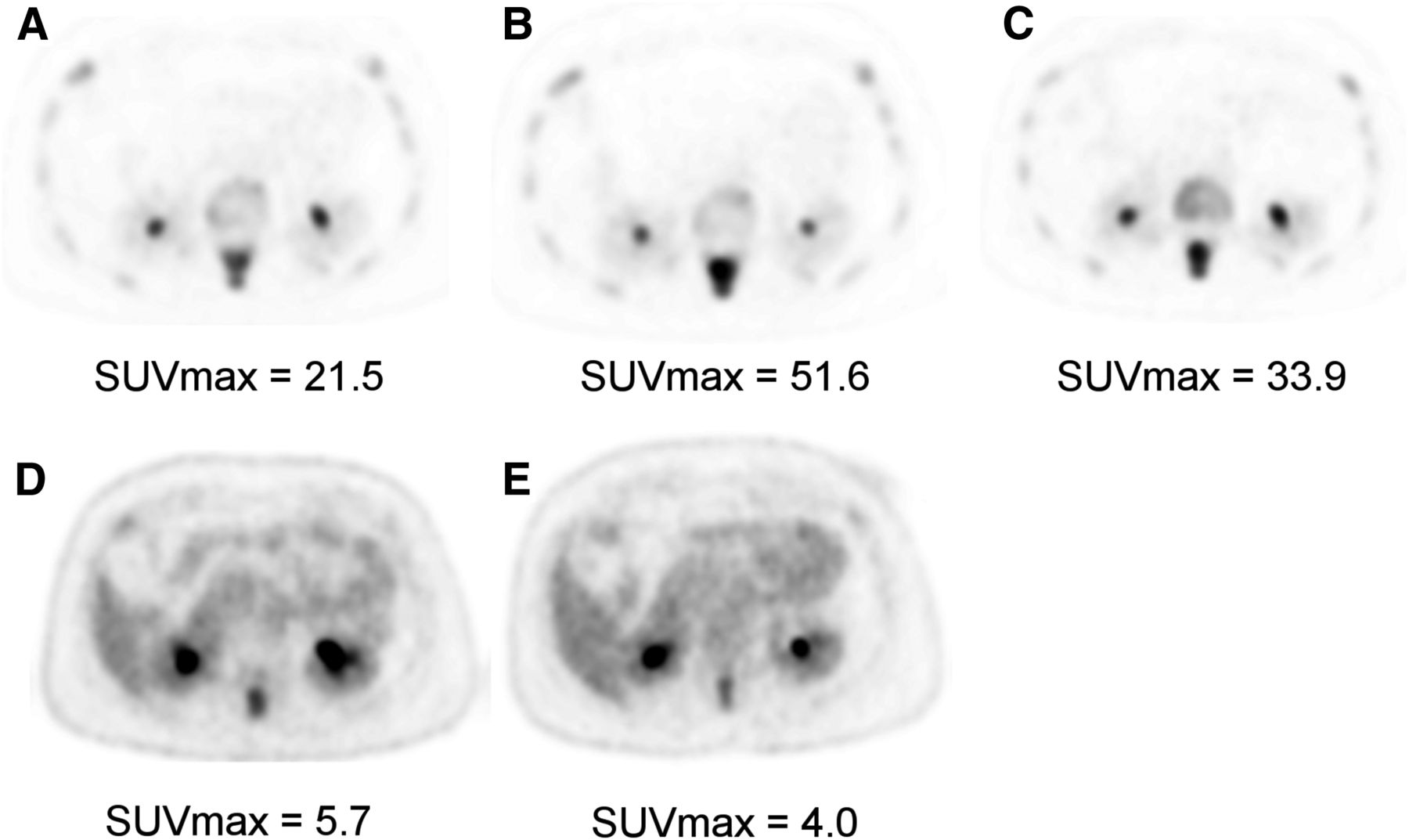
Axial slices at T12 showing 18F-NaF PET at baseline (A) and at 8 wk (B) and 12 wk (C) after commencement of endocrine treatment and equivalent 18F-FDG slices at baseline (D) and at 8 wk (E) in a 48-y-old woman with metastatic breast cancer (same patient as in Figs. 1 and 2). 18F-NaF PET at 8 wk shows significant increase in SUVmax, whereas 18F-FDG PET shows nearly 30% reduction in SUVmax. 18F-NaF PET at 12 wk shows decrease in SUVmax compared with that at 8 wk. This patient subsequently responded clinically, and scan sequences were interpreted as showing metabolic response with 18F-FDG PET at 8 wk but flare with 18F-NaF PET.
18F-FDG PET
The uptake of 18F-FDG in viable skeletal metastases is assumed to be predominantly within breast cancer tumor cells rather than osseous cells, such as osteoblasts or osteoclasts, thereby acting as a tumor-specific tracer rather than directly reflecting the altered bone microenvironment.
Several authors have reported lower sensitivity for 18F-FDG PET in osteoblastic lesions than in osteolytic lesions (15,17,55). Several factors may contribute to the reported differences in 18F-FDG avidity between osteoblastic and osteolytic metastases. Metastases that are inherently more biologically aggressive may show higher 18F-FDG uptake, with patients having a shorter overall survival than those with osteoblastic disease (17). The underlying histologic subtype may also be important; untreated invasive lobular carcinoma has been reported to show osteoblastic metastases with poor 18F-FDG uptake more frequently than invasive ductal or mixed subtypes (56). Previous treatment history is also important, as many 18F-FDG–negative skeletal metastases may appear sclerotic as a consequence of previous successful systemic therapy, rendering tumor cells nonviable—even though ongoing reparative osteoblastic activity, as seen with BS or 18F-NaF PET, may persist (57).
For detection of skeletal metastases and staging of cancer, 18F-FDG PET or PET/CT has shown higher sensitivity or specificity than BS in most reported studies (58,59) and metaanalyses (14,16,60). The improvement in sensitivity over that of BS may be due to the ability to detect metastatic tumor cells in the bone marrow before there is a sufficient osteoblastic effect to allow detection by bone-specific tracers. Gains in specificity may result from fewer causes of false-positive uptake of 18F-FDG than of nonspecific bone tracers in the skeleton.
It has been postulated that coinjecting 18F-NaF and 18F-FDG may allow even better diagnostic accuracy than the injection of either tracer alone or consecutively (61–63). In a prospective multicenter study, separate 18F-FDG PET/CT and 18F-NaF PET/CT were compared with coinjected 18F-FDG/18F-NaF PET/CT in patients with various cancers. In the 39 breast cancer patients included in the study, the combined scan revealed more lesions than 18F-NaF PET/CT alone, and in 5 patients, lesions that were not visible on 18F-FDG PET/CT alone were revealed by the combined scan (63). In another study, soft-tissue lesion conspicuity was not adversely affected when a combined scan was used, and although skeletal lesion-to-background ratios were lower than those obtained with 18F-NaF alone, no skeletal lesions were missed on the combined scan (64).
There is accumulating evidence that 18F-FDG PET may have the advantage over conventional imaging of being able to determine a response or a nonresponse to systemic therapeutics more accurately and at an earlier time point, with the potential to limit toxicity and accelerate the therapeutic transition in nonresponders. However, as yet there is no evidence that these properties translate into improved outcomes in terms of skeleton-related events, time to progression, or overall survival.
Compared with morphologic changes in bone lesions on CT, progressive lesions become more lytic and 18F-FDG–avid, whereas increased sclerosis usually indicates a response but can also be seen with progression (65); such observations were also reported in a retrospective series (Figs. 4 and 5) (66). In another retrospective study, although both a change in the 18F-FDG SUVmax and increased sclerosis on CT predicted time to progression in a univariate analysis, only the change in the SUVmax remained predictive in a multivariate model (67). Therefore, 18F-FDG PET seems to be able to add specificity to a purely morphologic treatment response assessment of bone metastases in breast cancer.

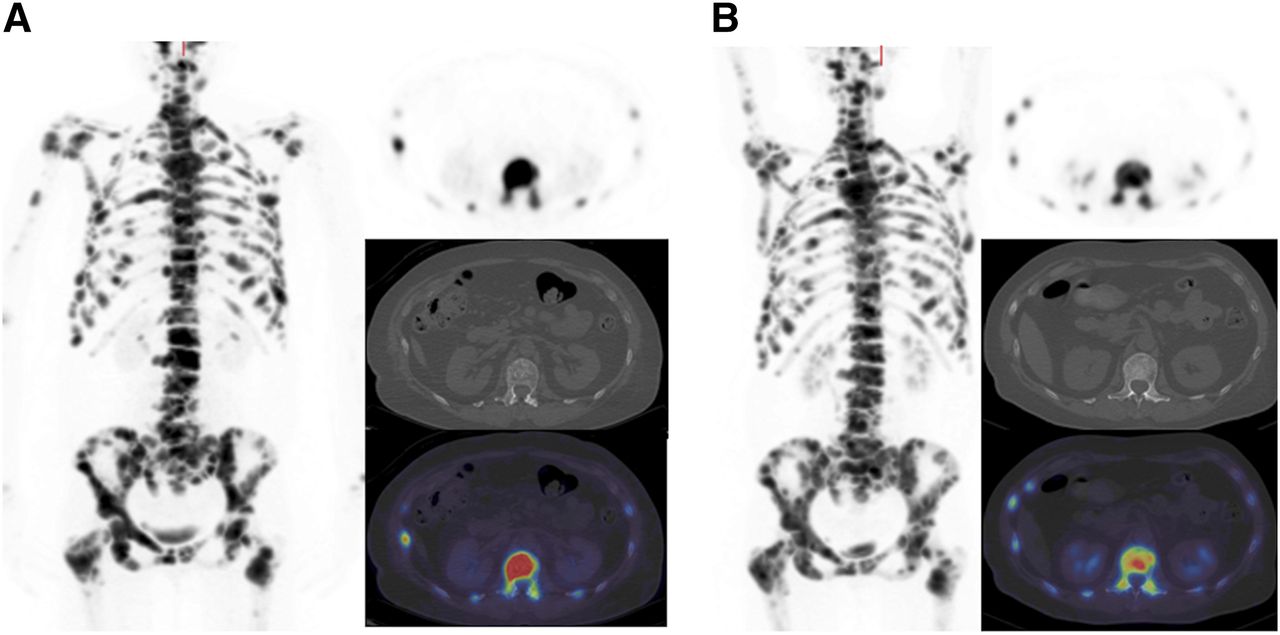
A 59-y-old woman with metastatic breast cancer. Maximum-intensity-projection 18F-NaF (left) and axial 18F-NaF PET, CT, and fused PET/CT (right, from top to bottom) at level of L1 at baseline (A) and at 8 wk (B) after commencement of endocrine therapy. Reduction in activity in all lesions was seen on 18F-NaF PET (L1 SUVmax decreased from 75.7 to 44.5).

Maximum-intensity-projection 18F-FDG PET/CT and axial slices at baseline (A) and at 8 wk (B) in 59-y-old woman with metastatic breast cancer (same patient as in Fig. 4). Marked metabolic response was seen on 18F-FDG PET (L1 SUVmax decreased from 9.5 to 3.3). Note increase in sclerosis in L1 on CT component.
Further studies have shown that changes in 18F-FDG SUVmax correlate with clinical and tumor marker response assessments (68) and are predictive of time to progression and time to skeleton-related events (69). A correlation between response or progressive disease on 18F-FDG PET and circulating tumor cell counts has also been observed (70). An 18F-FDG PET assessment was the only factor predictive of progression-free survival in a multivariate analysis, whereas estrogen receptor status was the only factor predictive of overall survival. In a prospective study of 22 patients (15 with bone metastases) receiving endocrine therapy for metastatic breast cancer, 18F-FDG PET/CT was performed at baseline and at 10 (±4) wk, and European Organization for Research and Treatment of Cancer PET response criteria were used (71). The authors reported statistically significant differences in progression-free survival but not overall survival between patients with progressive metabolic disease and patients who did not show progression (either responders or stable disease) (72).
OTHER MODALITIES
Whole-body MRI is now feasible in scan times of less than 1 h, and standard morphologic sequences (e.g., T1- and T2-weighted imaging and short-T1 inversion recovery imaging) are increasingly being combined with whole-body diffusion-weighted imaging. The signal from diffusion-weighted MRI (DW-MRI) depends on the rate of diffusion of water molecules, whereby tumors—which are typically hypercellular—show restricted diffusion compared with normal tissues. This property can be quantified, with the apparent diffusion coefficient representing the rate of signal loss with increasing diffusion weighting (73,74). The apparent diffusion coefficient typically increases with successful therapy as a result of cytotoxicity, reduced cellularity, and loss of cell membrane integrity, allowing water molecules to be more freely diffusible. Sclerotic lesions return a low signal on T1- and T2-weighted images and, because of fewer water molecules, are associated with lower diffusion signal and apparent diffusion coefficient. Therefore, differentiating reparative sclerosis after successful treatment from progressive disease may remain difficult (75), as it is with BS, although others have not shown this effect to be significant in prostate cancer (76).
In metastatic breast cancer, DW-MRI has been reported to be as sensitive as but less specific than 18F-FDG PET/CT, particularly in lymph nodes and the skeleton. These results indicate that the functional images from DW-MRI should not be read in isolation; correlation with morphologic assessment is required (77). A metaanalysis of studies of bone metastases from various cancers confirmed high sensitivity (90%) and specificity (92%) for whole-body MRI with diffusion-weighted imaging but lower specificity in studies in which DW-MRI was included (18).
One of the first comparisons of 18F-FDG PET/CT and PET/MRI in malignant skeletal disease, including 19 patients with breast cancer, reported similar lesion conspicuity and classification on PET but better anatomic delineation on MRI compared with CT (78). A systematic reduction in SUVs was noted in lesions and normal bone when PET/MRI was used; this issue is known to occur when MRI tissue segmentation methodology, which excludes cortical bone, is used for attenuation correction of PET data (79).
CONCLUSION
Although BS has served well for several decades, more recent advances in imaging have enabled several techniques to be used for staging of the skeleton with higher sensitivity and specificity. Some advances relate to hybrid imaging; for example, with SPECT/CT, PET/CT, and now PET/MRI, the high sensitivity of bone-specific or tumor-specific tracers can be complemented with the high spatial resolution and improved specificity of morphologic methods. At present, there are insufficient data to be able to determine which method provides the highest sensitivity for staging of the skeleton in breast cancer, but there is little doubt that the addition of CT in the form of BS with SPECT/CT and either bone-specific imaging with 18F-NaF or tumor-specific imaging with 18F-FDG and PET/CT improves diagnostic accuracy. It remains uncertain whether 18F-NaF or 18F-FDG alone is sufficiently sensitive for all subtypes of bone metastases or whether both tracers are required, possibly as a combination cocktail, to yield the highest sensitivity and specificity.
For monitoring of a treatment response, there are insufficient data to be able to recommend serial 18F-NaF PET/CT in breast cancer, and it is likely that the flare phenomenon—as recognized with BS for many years—will also be a problem for early response assessment within a few months of the start of systemic therapy. In contrast, accumulating evidence suggests that 18F-FDG PET/CT may be a good method for measuring a response early in the course of therapy, perhaps as early as 2 or 3 mo. Whole-body MRI is now feasible and practical, although there remain insufficient data specifically about routine use for breast cancer skeletal metastases; further work is required to understand how to optimally use DW-MRI and the apparent diffusion coefficient to measure a treatment response. It is tempting to think that the combination of morphologic, metabolic, and physiologic data that PET/MRI supply may provide a step forward in this clinical application where it is recognized that current methods are insufficiently sensitive and specific at early time points.
DISCLOSURE
We acknowledge financial support from the Department of Health (England) via National Institute for Health Research (NIHR) Biomedical Research Centre awards to Guy’s and St. Thomas’ NHS Foundation Trust in partnership with King’s College London and the King’s College London/University College London Comprehensive Cancer Imaging Centre funded by Cancer Research UK and the Engineering and Physical Sciences Research Council in association with the Medical Research Council and the Department of Health and a research grant from Breast Cancer Now. No other potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.
- 24.
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.
- 37.↵
- 38.↵
- 39.↵
- 40.
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- Received for publication August 3, 2015.
- Accepted for publication August 6, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Osseous sarcoidosis mimicking metastatic breast cancer
- Molecular Imaging of Bone Metastases and Their Response to Therapy
- Is Response Assessment of Breast Cancer Bone Metastases Better with Measurement of 18F-Fluoride Metabolic Flux Than with Measurement of 18F-Fluoride PET/CT SUV?
- Prospective Study of Serial 18F-FDG PET and 18F-Fluoride PET to Predict Time to Skeletal-Related Events, Time to Progression, and Survival in Patients with Bone-Dominant Metastatic Breast Cancer
- Molecular Imaging of Biomarkers in Breast Cancer
- Introduction and Overview