


Abstract
This study compared the diagnostic accuracy of 18F-FDG PET/CT with that of 18F-fluoride PET/CT in the detection of bony metastases in heightened-risk head and neck cancer patients. Methods: The study participants underwent 18F-FDG PET/CT and 18F-fluoride PET/CT within 2 wk of each another. Results: A total of 98 bony metastases were found in 18 of our 80 patients. 18F-fluoride PET/CT and 18F-FDG PET/CT showed similar lesion-based sensitivity (69.4% vs. 57.1%, P = 0.126) and areas under the curve (0.7561 vs. 0.7959, P = 0.149). Their combined interpretation demonstrated a significantly greater sensitivity and areas under the curve than that obtained with either modality alone (P < 0.001) in lesion-based analysis but not in patient-based analysis, with a treatment strategy change in 2 patients. Conclusion: 18F-fluoride PET/CT is a feasible modality for detecting bony metastases in patients with head and neck cancers, with similar sensitivity to 18F-FDG PET/CT. Their combined use may not be justifiable.
Distant metastases occur in 10%–30% of patients with advanced head and neck cancers (1). In these patients, accurate staging—including a survey of skeletal metastases—is crucial for selection of the appropriate therapy. The 99mTc-methylene diphosphonate (MDP) bone scan remains the current gold standard for skeletal staging in cancer patients. In May 2009, the halt in operation of National Research Universal in Canada contributed to a global 99mTc isotope shortage. Since then, the use of 18F-fluoride PET has gained attention. 18F-fluoride is superior to 99mTc-MDP in terms of both bone uptake and blood clearance (2). Because the current PET/CT systems offer high sensitivity and spatial resolution, the use of 18F-fluoride is being actively reevaluated. In comparative studies, the reported sensitivity of 18F-fluoride PET was higher than that of 99mTc-MDP bone scanning (94%–100% vs. 47%–78%) (3–5). One of the major drawbacks of 18F-fluoride PET or 99mTc-MDP bone scanning is a reduced sensitivity for detecting osteolytic bony metastases. In contrast, 18F-FDG PET/CT is superior to 99mTc-MDP bone scanning in the detection of osteolytic or bone marrow metastases (6,7). Because 18F-FDG PET/CT allows for the simultaneous assessment of local, regional, and distant sites of malignancy, there is active debate concerning the routine replacement of 99mTc-MDP bone scanning with 18F-FDG PET/CT for the detection of bony metastases (8,9).
Although the nuclear medicine community has begun to consider 18F-fluoride PET/CT as the next-generation bone scanning technique, its clinical usefulness in the era of 18F-FDG PET/CT is still a matter of debate. In this prospective study, we sought to compare the diagnostic accuracy of 18F-FDG PET/CT and 18F-fluoride PET/CT in the detection of bony metastases in head and neck cancer patients.
MATERIALS AND METHODS
Patients
This study was approved by the local ethics committee, and all patients provided written consent. We included patients with head and neck malignancies who presented with primary locoregional advanced disease, recurrent disease at locoregional sites, known disseminated disease other than in the bone according to conventional work-up findings, or unusual bone pain. Evaluations using 99mTc-MDP bone scanning, 18F-FDG PET/CT, and 18F-fluoride PET/CT were performed to determine the skeletal metastasis status. All scans were performed within 2 wk of each other.
18F-FDG PET/CT and 18F-Fluoride PET/CT
The 18F-FDG PET/CT protocol has been previously described (10). 18F-fluoride PET/CT was performed using a Discovery ST 16 system (GE Healthcare). The emission scan was initiated 50 min after an intravenous injection of 259 MBq (7 mCi) of 18F-labeled NaF. PET images were reconstructed using CT for attenuation correction with an ordered-subset expectation-maximization iterative reconstruction algorithm. 18F-fluoride PET scans included 8 bed positions (2-min acquisitions per bed position, 16-min total acquisition time) covering the skull, neck, arms, thorax, pelvis, and femora. Coronal, transverse, and sagittal sections and maximum-intensity projection images were documented in hard copy.
Image Interpretation and Reference Standards
Two nuclear medicine physicians (with 11 and 32 y of experience in nuclear medicine practice) interpreted the 99mTc-MDP bone, 18F-fluoride PET, and 18F-FDG PET images. The 2 nuclear medicine physicians and a radiologist (with 33 y of experience in radiology practice) interpreted the 18F-fluoride PET/CT or 18F-FDG PET/CT images. Interpretation of all 99mTc-MDP bone, PET, and PET/CT images was masked and performed separately. Any discrepancy was resolved by consensus. The observers did not know the results of any other imaging studies. The delay between the interpretation sessions was more than 3 d, and the order of presentations was randomized.
The probability of malignancies was graded using a 5-point scoring system (0, no lesion; 1, definitely benign; 2, probably benign; 3, probably malignant; and 4, definitely malignant) (11). Bone lesions on 99mTc-MDP bone or PET images were categorized as benign when they appeared as hot osteophytes or when they were located around joints. Vertebral lesions were considered malignant when they involved either the entire vertebra or the posterior aspect of the vertebral body and pedicle (10,12,13). Rib lesions were categorized as malignant when they showed elongated uptake, but they were categorized as benign when they involved several ribs vertically. On the basis of the corresponding CT images from PET/CT scans, the corresponding lesions were reclassified as benign when they showed degenerative changes, fractures, or other reactive bone lesions. Any blastic bone marrow infiltration or cortical destruction associated with soft-tissue masses on CT images was considered to be malignant (14).
Patients were considered to have a bone metastasis if the bone lesion was positive on both the 18F-FDG PET/CT and the 18F-fluoride PET/CT examinations and if the patients exhibited a concordant clinical course of progression. For patients who had concurrent distant visceral metastasis, progressive findings from the imaging follow-up examinations were used as the reference standard. Histologic proof of bone metastasis was considered necessary only if it was critical for therapeutic decisions. Lesions that could not be classified were further evaluated by other radiologic techniques, when bone biopsy was not feasible. All our surviving patients were followed up for more than 6 mo.
Statistical Analysis
The sensitivity, specificity, accuracy, and negative and positive predictive values of 99mTc-MDP bone scanning, PET, and PET/CT for the detection of bone metastases were calculated and then compared with one another using the McNemar paired-sample test. Their diagnostic performance was assessed with receiver-operating-characteristic curves. The area under the receiver- operating-characteristic curve (AUC) was calculated for each technique and compared statistically. A 2-tailed P value of less than 0.05 was considered statistically significant.
RESULTS
Patients
Between January 2009 and June 2011, 80 patients were included. Because 99mTc was not available due to the global shortage of 99mTc from July 2009 to October 2010, only 47 patients were able to undergo 99mTc-MDP bone scans. As a result, the major focus of this study was shifted to a comparison of the diagnostic capacities of 18F-fluoride PET/CT and 18F-FDG PET/CT. The results of the 99mTc-MDP bone scans in 47 patients are described in Supplemental Tables 1 and 2 (supplemental materials are available online only at http://jnm.snmjournals.org).
Diagnostic Capability of 18F-Fluoride PET/CT and 18F-FDG PET/CT
Lesion-Based Analysis
A total of 403 bone lesions were detected. Ninety-eight lesions (24.3%) were malignant metastases, whereas 305 were benign (Table 1). 18F-fluoride PET/CT had a higher level of sensitivity and AUC than 18F-FDG PET/CT (Fig. 1), although these differences were not significant (P = 0.126 and 0.149, respectively). However, the sensitivity and AUC were significantly higher for the combined interpretation of 18F-fluoride PET/CT and 18F-FDG PET/CT than for either modality alone (P < 0.001, Fig. 2).
Assessment of Skeletal Metastasis by 18F-FDG PET/CT and18F-Fluoride PET/CT Based on Lesion Number

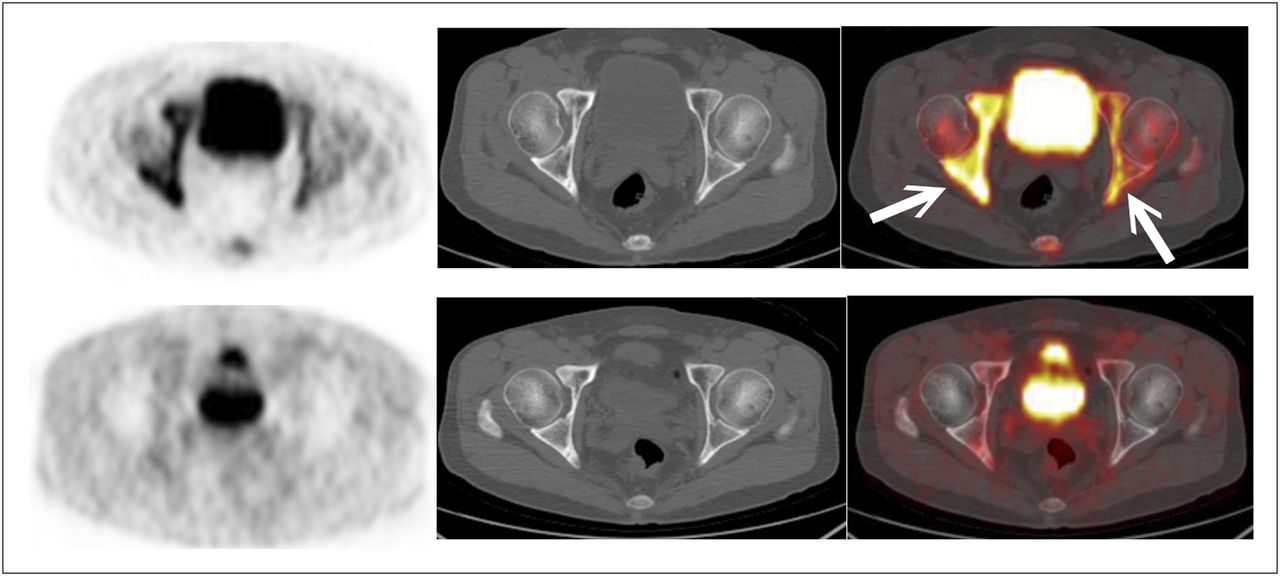
A 48-y-old man who presented with advanced tongue cancer. 18F-fluoride PET (top left) and PET/CT (top right) showed markedly increased bilateral uptake at acetabula (arrows), highly suggestive of bony metastases. Corresponding 18F-FDG PET (bottom left) and PET/CT (bottom right) images did not reveal abnormal uptake. MRI of pelvis confirmed presence of bony metastases.

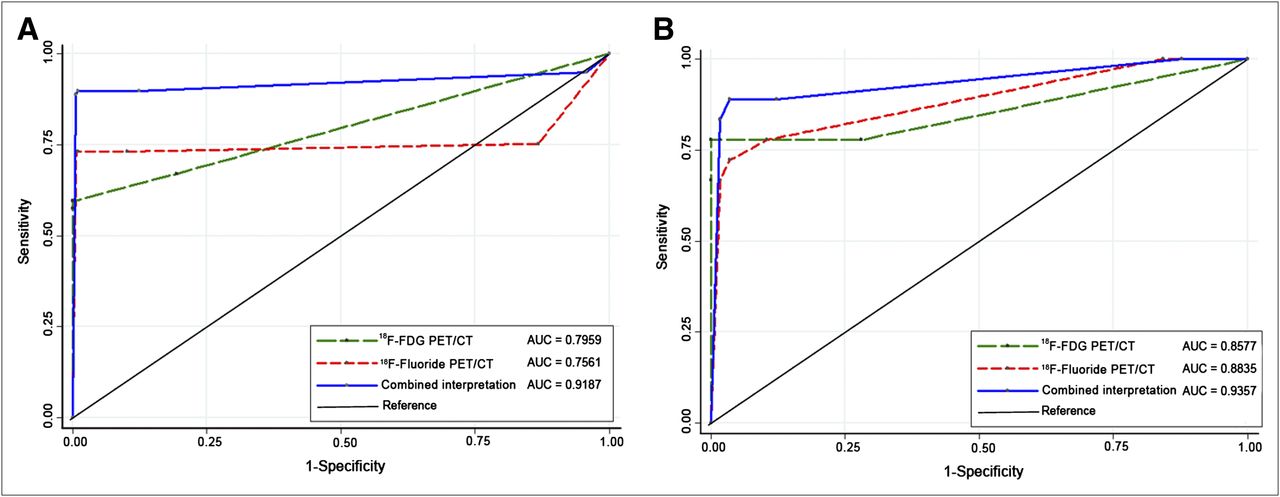
Comparison of AUCs for 18F-FDG PET/CT, 18F-fluoride PET/CT, and combined interpretation of both imaging modalities on lesion basis (A) and patient basis (B). In lesion-based analysis, combined interpretation yielded significantly greater AUC than did 18F-FDG PET/CT (P < 0.001) or 18F-fluoride PET/CT (P < 0.001) alone. In patient-based analysis, combined interpretation demonstrated moderately higher AUC than did 18F-fluoride PET/CT alone (P = 0.065). Difference between AUCs of combined interpretation and 18F-FDG PET/CT was not significant (P = 0.32). Differences between sensitivities of combined interpretation and 18F-FDG PET/CT and 18F-fluoride PET/CT were also not significant (P = 0.5 and 0.25, respectively).
Patient-Based Analysis
Eighteen patients were found to have bony metastases (22.5%, 18/80). The patient-based sensitivity of 18F-FDG PET/CT was similar to that of 18F-fluoride PET/CT (Table 2). The combined interpretation had a higher sensitivity and AUC than did either modality alone, but the difference was not statistically significant.
Assessment of Skeletal Metastasis by 18F-FDG PET/CT and18F-Fluoride PET/CT Based on Patient Number
Detection of Skeletal Metastases According to Bone Morphology
We then calculated the detection rates of bony metastases according to their morphologic changes on the corresponding CT images (Supplemental Table 3). For the 37 lesions with osteosclerotic changes on CT, 18F-fluoride PET/CT demonstrated a significantly higher detection rate than 18F-FDG PET/CT (Fig. 3) (91.9 vs. 43.2%, P = 0.01). In contrast, 18F-FDG PET/CT had a higher detection rate for osteolytic lesions (Fig. 4) (P = 0.31). For lesions with mixed osteosclerotic and osteolytic changes or without morphologic changes on CT images, the 2 imaging modalities had similar detection rates.
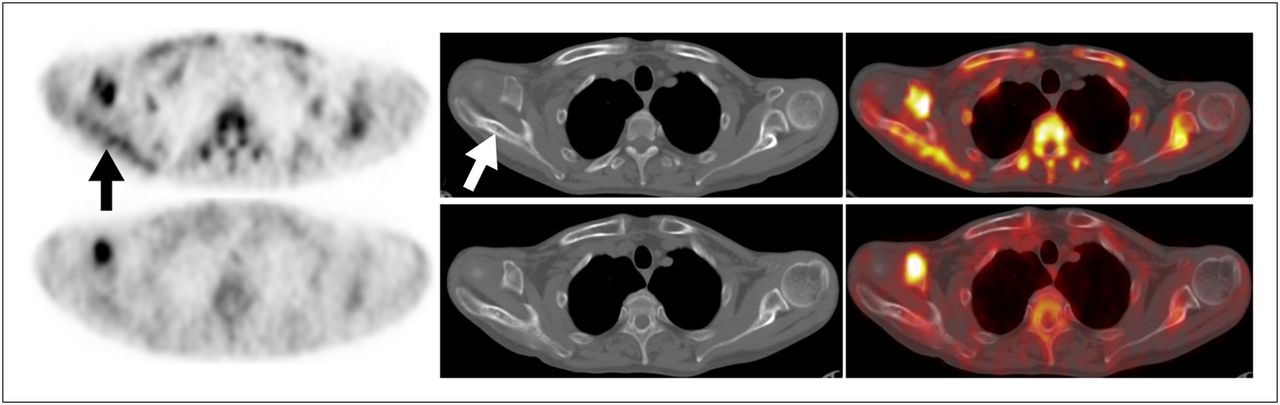
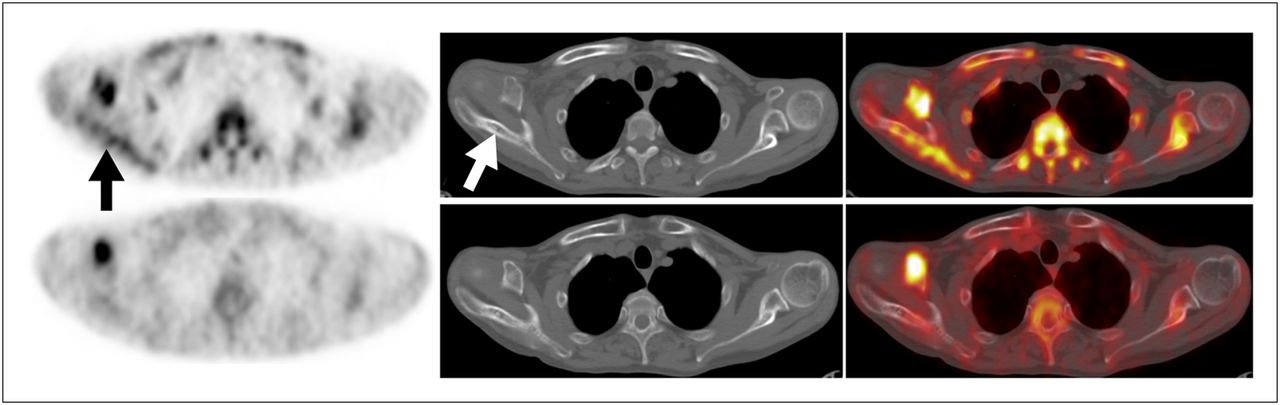
A 47-y-old patient with retromolar cancer and multiple bony metastases at vertebrae, thoracic cage, and extremity bones. 18F-fluoride PET (top left) and PET/CT (top right) showed abnormally increased uptake (arrows) at right scapula, with osteosclerotic changes on CT (top middle). Corresponding 18F-FDG PET (bottom left) and PET/CT (bottom right) did not reveal abnormal uptake at this metastatic site (B). Bone metastases progressed despite treatment, and patient died 6 mo later.

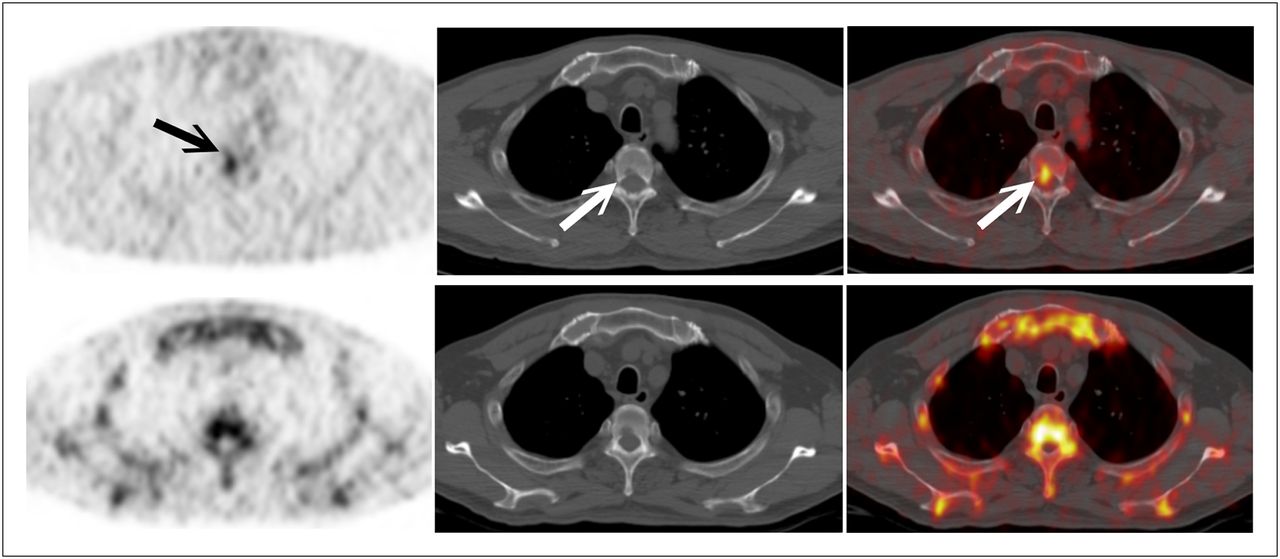
A 46-y-old man who presented with advanced buccal cancer and multiple bony metastases in vertebrae and ribs. 18F-FDG PET (top left) and PET/CT (top right) revealed focal area with abnormally increased uptake (arrows) in T4 vertebral body, corresponding to osteolytic lesion on CT (top middle). Osteolytic lesion was detected neither by 18F-fluoride PET (bottom left) nor by PET/CT (bottom right). Progressive bony metastatic disease was evident at follow-up despite use of systemic chemotherapy.
DISCUSSION
Since February 2011, the Centers for Medicare and Medicaid Services has been reimbursing for 18F-fluoride PET/CT bone scanning performed through the National Oncologic PET Registry. For this reason, 18F-fluoride PET/CT is considered as a potential substitute for 99mTc-MDP scintigraphy. In this prospective study, we found that 18F-fluoride PET/CT had a sensitivity and accuracy comparable to that of 18F-FDG PET/CT for the detection of bony metastases in patients with head and neck cancers, although each modality had its limitations. In the lesion-based analysis, 18F-fluoride PET/CT and 18F-fluoride PET demonstrated moderate sensitivities for detecting bony metastases. In previous studies, the sensitivity of 18F-fluoride PET for detecting bony metastases varied widely from 72% to 95% (3,15,16). Differences in the incidence of osteoblastic bony lesions or in the study design may account for such discrepancies. A recent metaanalysis found that the reported sensitivities of 18F-FDG PET in various types of tumors ranged from 45% to 95% (9). We have previously reported that 18F-FDG PET had a sensitivity of 70% for detecting bony metastases of nasopharyngeal carcinoma (13). In the current study, the patient-based sensitivity of 18F-FDG PET/CT for head and neck cancer was also approximately 70%. The wide range of reported sensitivities of 18F-FDG PET is probably due to different inclusion criteria or different avidities of 18F-FDG for various types of tumors.
During the process of bone metastasis, bone formation and destruction occur simultaneously; however, in blastic metastases, bone formation by osteoblasts predominates in the space created by bone destruction. For lytic metastases, bone destruction and tumor cell growth predominate in the bone resorption space (17). Nakai et al. (18) have shown that 99mTc-MDP bone scanning demonstrated a slightly higher sensitivity than 18F-FDG PET for the detection of osteosclerotic bony metastases in breast cancer patients. In our study, 18F-fluoride PET/CT demonstrated a significantly higher sensitivity than 18F-FDG PET/CT for the detection of sclerotic lesions. The study of Nakai et al. (18) also showed that 18F-FDG PET/CT had a significantly higher sensitivity than 99mTc-MDP bone scanning for lesions without visible morphologic changes on CT. However, our results indicate that 18F-FDG PET/CT and18F-fluoride PET/CT have similar detection rates. The discrepancies between our results and those of Nakai et al. may be due to our use of 18F-fluoride PET/CT instead of conventional 99mTc-MDP bone scanning. Therefore, the power of the osteoblastic activity-seeking tracer was evaluated more accurately and was not underestimated.
One should be aware of the problem of false positives when interpreting 18F-fluoride PET/CT images. Nonetheless, 18F-fluoride PET/CT showed fewer false-positive findings than conventional bone scanning in the detection of bony metastases (5,19). Besides, inappropriate treatment due to false-positive findings can be minimized via a thorough discussion of cases in a multidisciplinary tumor board.
Does the increased sensitivity from combined reading translate into a real clinical impact? We found that the additional use of 18F-fluoride PET/CT increased the bony metastasis detection rate by 16.6% in our patients treated with curative intent (primary advanced or recurrent locoregional cancer) (2/12, Supplemental Table 4). However, because of the small sample size, no firm conclusion about the clinical impact of combined imaging can be drawn.
CONCLUSION
The results of this pilot study indicate that 18F-fluoride PET/CT and 18F-FDG PET/CT have similar sensitivity and accuracy for detecting bony metastases of head and neck cancers, with 18F-fluoride PET/CT showing superiority for osteosclerotic metastases and 18F-FDG PET/CT showing superiority for osteolytic lesions. The limited clinical impact of combined PET/CT interpretation observed in this study does not seem to justify its routine use. More research is needed to further explore the clinical utility of the combined imaging.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This study was supported by grants (CMRPG370081-3) from Chang Gung University and Chang Gung Memorial Hospital, Taiwan. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 7, 2012.
↵* Contributed equally to this work.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 22, 2012.
- Accepted for publication June 20, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}