


Abstract
The aims of the study were to evaluate the effects of oral contrast on apparent tracer activity measured with PET/CT when using CT attenuation correction and to report our initial experience in the use of oral contrast with PET/CT. Methods: Phantom studies with 18F activity and saline bags or syringes filled with barium or gastrografin of varying densities were performed using a PET/CT scanner (CT attenuation correction). In the study, 91 clinical patients received dilute oral contrast and were evaluated by whole-body 18F-FDG PET. Results: A phantom experiment with CT contrast (1.3% weight/volume [w/v] barium) showed a “cold” area in the cold stomach whereas a phantom with high-density barium (98% w/v) showed an artifactual focus of intense “activity” in the cold stomach. In clinical studies, stomach and right colon were opacified by CT contrast. Maximal measured contrast density was 239 Hounsfield units. Conclusion: High-density barium causes overestimation of tissue 18F-FDG concentration. Low-density barium does not cause significant artifacts and appears suitable for clinical use.
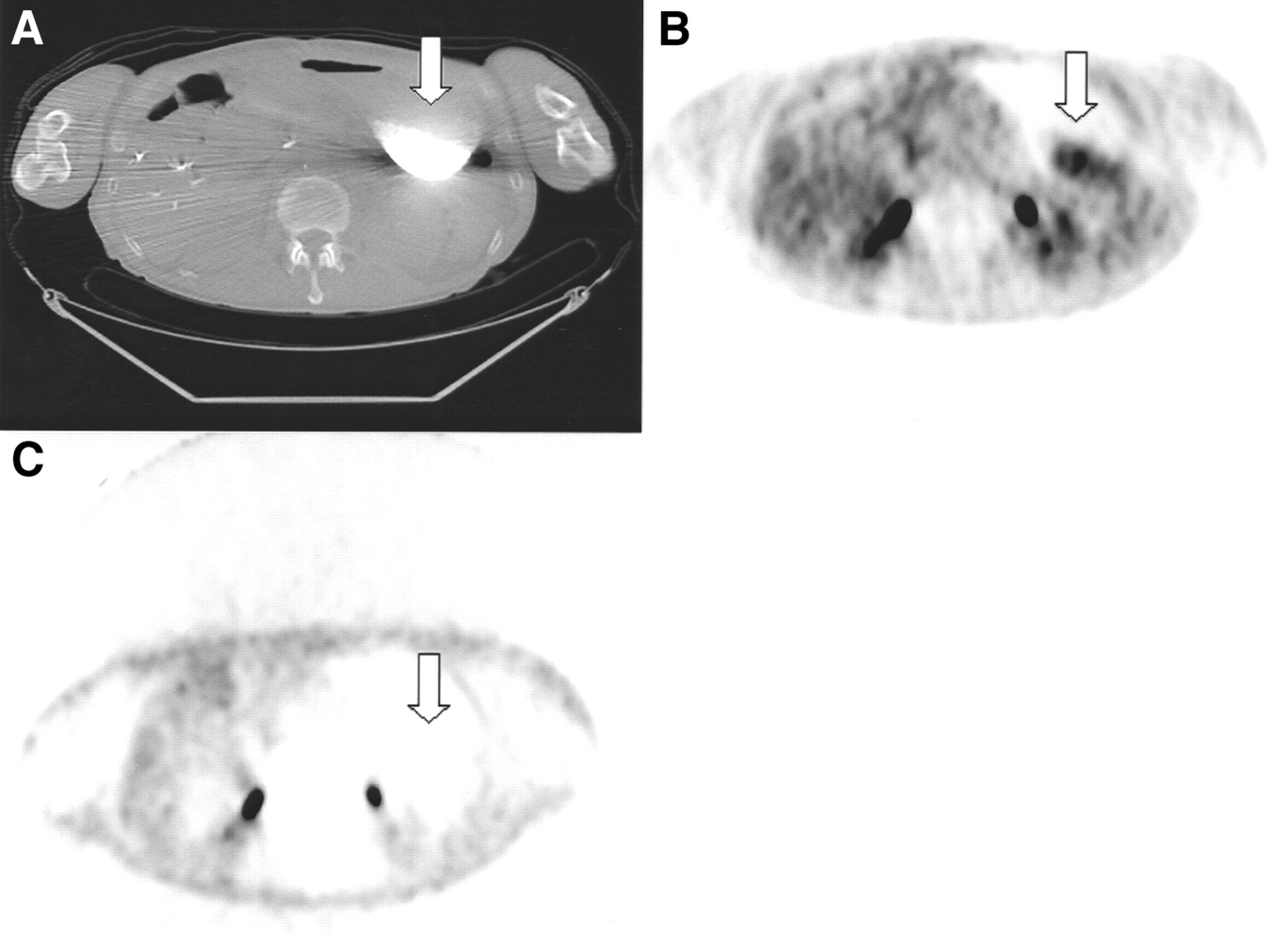
In CT scanning, the use of positive oral contrast has been shown to allow better definition of the bowel (1–3). Oral contrast might help in interpreting PET/CT images, allowing better discrimination between physiologic and pathologic abdominal uptake. Because artifactually increased activity in the presence of radiodense objects has been reported with CT attenuation correction (4), oral contrast is also a potential cause of artifacts on PET/CT in cases of overestimation of 511-keV photon attenuation and overcorrection of images. During our initial PET/CT experience, CT-corrected PET images in a patient who had consumed high-density barium for other purposes revealed an artifact of “increased” gastric activity that was unseen on the uncorrected images (Fig. 1).

Sixty-year-old man with rising CA19-9 level and history of pancreatic cancer after therapy was evaluated by 18F-FDG PET for suspected tumor. Patient had ingested barium for upper gastrointestinal study 1 week before PET/CT study without additional contrast being administered. CT (A; arrow) showed residual, dense barium in distended stomach consistent with high-grade gastric outlet stenosis. CT attenuation-corrected PET emission images (B; arrow) showed area of increased activity in stomach corresponding to barium retention on CT (max CT Hounsfield units = 3,071). However, no increased uptake was seen in gastric lumen in nonattenuation-corrected images (C; arrow). SUVLEAN for high-activity gastric artifact was 5.31 maximum and 3.81 mean.
The purpose of this study was to evaluate in phantom studies whether oral contrast could affect apparent PET tracer “activity” when using CT attenuation correction. We also assessed our initial clinical experience with oral contrast.
MATERIALS AND METHODS
Data Acquisition
Scanning was performed using a PET/CT scanner (Discovery LS; GE Medical Systems, Waukesha, WI). Emission data were acquired for 5-7 positions at 5 min per position and were reconstructed using CT for attenuation correction (ordered-subset expectation maximum algorithm). The parameters of the multidetector helical CT were 140 kVp, 80 mA, 0.8 s per CT rotation, pitch of 6, and 22.5 mm/s table speed. The conversion scale used to transform Hounsfield units (HU) into attenuation coefficients was described previously (5).
Phantom Studies
The first 2 experiments were performed with a phantom filled with 74 MBq 18F activity (0.24 mCi/mL) and a saline bag filled with CT oral contrast (READY CAT barium sulfate suspension, 1.3% weight/volume [w/v]; E-Z-EM Inc., Westbury, NY) and high-density barium (E-Z-HD barium sulfate suspension, 98% w/v; E-Z-EM Inc.), respectively (to simulate a contrast-filled stomach). In the third experiment, 8 syringes filled with varying concentrations (100%, 80%, 60%, 40%, 20%, 10%, 1%, and 0%) of MD-Gastroview (Mallinckrodt Inc., St. Louis, MO) were placed in a cylindric phantom containing 74 MBq 18F activity diluted with water (0.35 mCi/mL).
In all experiments, CT was performed, followed by emission and transmission scanning with 68Ge (3 min per position). Two datasets of PET images with 68Ge and CT-based correction and 1 without attenuation correction were reviewed by an experienced nuclear medicine physician using eNTEGRA software (ELGEMS, Haifa, Israel). Images were reviewed for abnormal uptake in the region of the stomach present on the attenuation-corrected images and absent on the noncorrected images. For the third experiment, a 1.91-cm2 region of interest (ROI) was used to measure the “activity” and contrast density for each syringe.
Patient Studies
A total of 108 clinical patients were evaluated retrospectively by whole-body 18F-FDG imaging after oral contrast utilization was initiated. Patients received 2 bottles (450 mL per bottle) of CT contrast (barium suspension; 1.3%) at least 10 min before receiving a 555- to 740-MBq 18F-FDG intravenous injection, followed by another bottle of contrast 40 min later.
Image Analysis
One experienced reader performed image analysis using eNTEGRA software. Patient compliance with contrast ingestion and quantity of contrast were reviewed. The extent of bowel opacification was categorized as absent, partial, or adequate on the CT images. For the first 30 patients receiving oral contrast, density of contrast in the digestive tract was measured in HU using a manually drawn ROI. The maximum diameter in millimeters of the gastric lumen, evaluated in a transverse section of the midportion of the stomach, was then measured for CT and PET images. PET window levels were adjusted for each patient to those used for clinical interpretation (liver activity set to moderate gray intensity). A soft-tissue window (minimum = − 250 HU; maximum = +250 HU) was used for CT. The possible effect of oral contrast ingestion on neck muscle uptake was evaluated in 2 groups of 20 patients (with and without contrast) by measuring metabolic activity in several neck muscles using a circular ROI (6-pixel area).
RESULTS
Phantom Studies
The first experiment with CT oral contrast (1.3% w/v) showed a cold area in the region of contrast in the nonradioactive stomach for all 3 sets of images. The maximum density in the stomach was 182 HU.
The second experiment with high-density contrast showed a cold area in the region of the nonradioactive stomach in the noncorrected and 68Ge-corrected images. The CT-corrected images, however, showed an artifactual focus of intense “activity” with a maximal density measured at 3,071 HU in the nonradioactive stomach.
In the third experiment, 68Ge-corrected and noncorrected images showed the cold syringes in a uniform background. The CT attenuation correction produced similar expected “cold”-appearing images of the syringes containing 0% and 1% contrast, but the higher concentrations showed increasing levels of activity, with intense artifacts at >60% concentration (not shown). Figure 2 shows that the measured activity is progressively overestimated with CT attenuation correction at high HU using the commercial software.
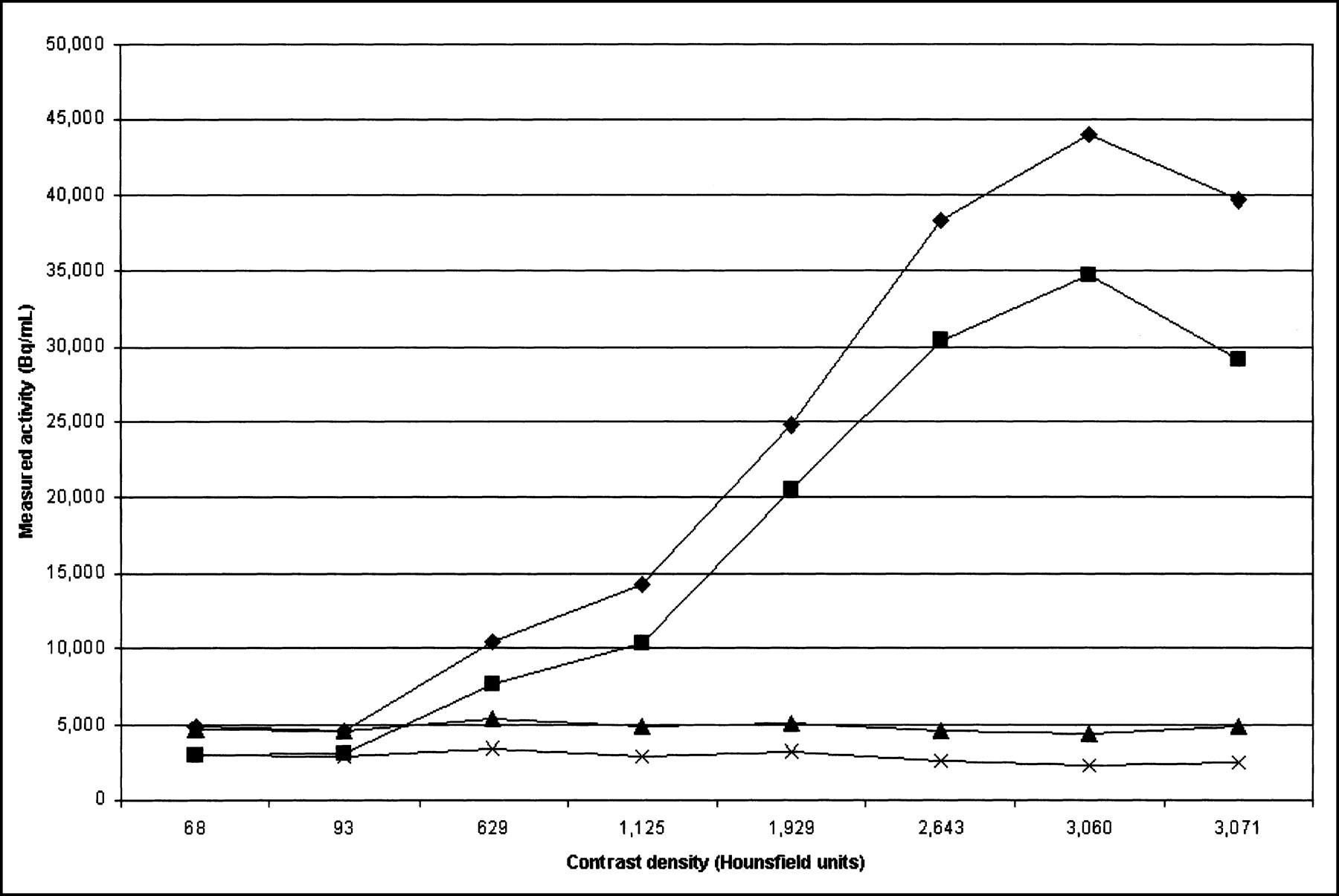
Phantom with syringes filled with variable concentrations of gastrografin, plotted as measured emission data activity (in Bq/mL) versus measured contrast density by CT (in Hounsfield units [HU]). Maximum (♦) and mean (▪) measured activity with CT attenuation correction, and maximum (▴) and mean (✖) measured activity with 68Ge attenuation correction are displayed. Drop in measured activity is observed for high-density contrast. In this region, “real density” is >3,071 HU, but the PET/CT system plateaus at this level. Thus, overcorrection in presence of high-density contrast also has plateau corresponding to 3,071 HU density. However, because of increased true attenuation as result of increasing “real” density, measured counts decrease, resulting in drop in curve.
Patient Studies
Of the 108 patients (84%), 91 received oral contrast. Of these, 75 patients received the full regimen of contrast and 16 received only part of the contrast because of inability to drink the entire volume. Seventeen did not receive any contrast because of the study indication (head and neck cancer [n = 11]) or refusal (n = 6). Details on bowel opacification are reported in Table 1. Measured oral contrast density in the digestive tract is reported in Table 2.
Extent of Bowel Opacification by Oral Contrast
Contrast Density Measured in Bowel in Patients Receiving CT Oral Contrast
The diameter of the stomach lumen measured on CT was significantly different (59.8 ± 20.6 mm) from that measured on PET emission images with CT attenuation correction (43.8 ± 23; P < 0.000001). Muscle activity tended to be higher in patients who received oral contrast than in those without contrast (Table 3). A systematic review of the diagnostic utility of oral contrast in enhancing the interpretation of PET/CT images (Fig. 3) will be reported subsequently. No obvious foci of artifactual “uptake” resulting from CT-based attenuation correction in the presence of CT oral contrast were found. There were thus no false-positive interpretations related to such potential artifacts.

Example of clinical value of oral contrast in patient with resected colorectal carcinoma evaluated with 18F-FDG PET for suspected recurrence. (A) Transverse CT image shows transverse colon with contrast (white arrow) and soft-tissue- density lesion adjacent to anterior abdominal wall (black arrow). (B) PET images with CT attenuation correction show focus of intense uptake in anterior abdomen (white arrow). (C) Fused PET/CT image shows that focus of uptake corresponds to soft-tissue mass (white arrow) and not to bowel. Diagnosis of peritoneal tumor implant was made. Patient underwent chemotherapy.
Muscle Uptake (SUVlean) Maximum With and Without Oral Contrast
DISCUSSION
The clinical case example and the phantom experiments clearly showed that high-density oral contrast can produce an artifact of apparent increased tracer uptake. The radiodensity of this dense barium is near that of metallic objects, which also can produce artifacts of increased activity on emission PET if CT-corrected emission data are used (4). These artifacts are likely caused by the energy differences between photons used for CT scanning and the 511-keV photons used for 68Ge transmission scanning. The use of low-energy photons for transmission imaging results in increased attenuation coefficients in the presence of materials of high atomic number (metallic objects, high-density contrast material) compared with the use of high-energy 511-keV photons. This increased attenuation for low-energy x-rays is caused by an increased probability of photoelectric interaction of low-energy photons with material of high atomic number. Mathematic algorithms ideally should scale the attenuation coefficients obtained with low-energy photons to the energy level of 511-keV photons. However, it appears that current and widely applied commercial scaling algorithms are not appropriate for high-density materials, causing an overestimation of attenuation coefficients in their presence and thus an overcorrection of the emission data that then produces an artifact of increased apparent tracer activity. The third phantom experiment shows that the CT attenuation correction algorithm produces an increasing overcorrection of the emission activity in the presence of increasing density of high- atomic-number contrast materials (Fig. 2). The overestimation of tracer activity begins to appear for materials as the measured density rises between 93 and 629 HU. The exact concentration threshold at which artifacts of increased activity can be expected will vary according to the material used for contrast and its quantity. No studies showed obvious artifacts from using oral CT contrast with 1.3% barium, as commonly used in CT contrast studies.
The density of CT oral contrast, with a maximum of 239 HU registered in patients, appears to be low enough not to produce a significant artifact. Therefore, artifacts of increased activity caused by CT oral contrast seem unlikely and were not observed in this study. However, if the concentration of the oral contrast in the lumen increases markedly as a result of significant water reabsorption, it is possible that artifacts of increased apparent tracer uptake will be observed. A limited time of around 1 h between CT oral contrast administration and CT acquisition may have limited water reabsorption and artifacts in our clinical patients.
The extent of gut opacification was adequate for most of the stomach, small bowel, and right colon but was adequate less frequently for the transverse, descending, and rectosigmoid colon. Nonopacification of the left colon is a lesser problem, because colon identification is often straightforward. Opacification of the small bowel is more relevant, because without contrast it is not always easy to delineate from other abdominal structures.
The size of the gastric lumen was smaller when measured by PET than by CT. A spatial misregistration could occur in this situation, and corrections for attenuation will be less accurate. Our comparison of contrast and noncontrast patient groups showed that muscle uptake in the head and neck is not substantially different globally in the contrast and noncontrast PET study groups. However, to avoid increased muscle uptake, we are not currently using oral contrast in head and neck cancer.
The diagnostic impact of oral contrast on PET/CT interpretation was not systematically evaluated in this study, because only contrast-enhanced CT was performed. However, oral contrast enhancement clearly facilitates small bowel identification, and qualitatively makes image interpretation easier with PET/CT.
CONCLUSION
Phantom studies demonstrated artifacts of increased apparent 18F-FDG uptake using CT-corrected PET if dense contrast was present. Phantom and patient studies using clinically practical CT oral contrast did not demonstrate such artifacts. CT oral contrast use has been implemented in clinical PET/CT practice and appears valuable in some instances.
Footnotes
Received May 24, 2002; revision accepted Oct. 4, 2002.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, Russell H. Morgan Department of Radiology and Radiological Sciences, Johns Hopkins Hospital, 601 N. Caroline St., Room 3223, Baltimore, MD 21287-0817.
E-mail: rwahl{at}jhmi.edu
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Best Practices for 18F-Fluciclovine PET/CT Imaging of Recurrent Prostate Cancer: A Guide for Technologists
- Utility of positron emission tomography/CT in the evaluation of small bowel pathology
- Standards for PET Image Acquisition and Quantitative Data Analysis
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Diagnosis and Differentiation of Bronchioloalveolar Carcinoma from Adenocarcinoma with Bronchioloalveolar Components with Metabolic and Anatomic Characteristics Using PET/CT
- Dual-Modality Imaging: Combining Anatomy and Function
- Effective Methods to Correct Contrast Agent-Induced Errors in PET Quantification in Cardiac PET/CT
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Procedure Guideline for SPECT/CT Imaging 1.0
- Procedure Guideline for Tumor Imaging with 18F-FDG PET/CT 1.0
- PET/CT Imaging Artifacts
- Concurrent PET/CT with an Integrated Imaging System: Intersociety Dialogue from the Joint Working Group of the American College of Radiology, the Society of Nuclear Medicine, and the Society of Computed Body Tomography and Magnetic Resonance
- Do Implanted Pacemaker Leads and ICD Leads Cause Metal-Related Artifact in Cardiac PET/CT?
- An Analysis of the 18F-FDG Uptake Pattern in the Stomach
- Accuracy of Whole-Body Dual-Modality Fluorine-18-2-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography and Computed Tomography (FDG-PET/CT) for Tumor Staging in Solid Tumors: Comparison With CT and PET
- Why Nearly All PET of Abdominal and Pelvic Cancers Will Be Performed as PET/CT
- To Enhance or Not to Enhance? 18F-FDG and CT Contrast Agents in Dual-Modality 18F-FDG PET/CT
- Correction for Oral Contrast Artifacts in CT Attenuation-Corrected PET Images Obtained by Combined PET/CT
- PET/CT in Colorectal Cancer