


Abstract
In combined PET/CT imaging, functional data provided by 18F-FDG increase diagnostic accuracy over conventional PET and CT in a variety of malignancies. The question to be raised is: how much is CT needed in PET/CT imaging? Discussion: In stand-alone CT imaging, contrast agents are applied to aid differentiation of anatomic structures, improve lesion localization, and support lesion characterization. Based on our experience, the most important benefit when applying CT contrast agents in PET/CT imaging relates to more precise anatomic localization of pathology by differentiation of the lesion from its surrounding structures on CT. This benefit must be considered most profound in the head and neck as well as the abdomen and pelvis, where delineation of pathology from muscles, vascular structures, or the intestine is critical. CT contrast agents can be of additional value in tumors with only mild or no increase in 18F-FDG uptake by supporting lesion detection and characterization. The complementary role of CT contrast agents and molecular contrast for PET/CT imaging is addressed in this review. The authors provide specific indications as to which contrast-enhanced CT data provide additional diagnostic value. Conclusion: Functional contrast aids lesion detection and characterization, whereas morphologic contrast improves lesion localization. CT contrast agents and PET tracers do not compete but rather are complementary in combined PET/CT imaging.
Dual-modality PET/CT imaging systems permit the combined acquisition of functional and morphologic datasets within a single examination (1). Although the collection and interpretation of CT image sets represent a core competency of radiologists, PET imaging clearly falls within the realm of nuclear medicine. Based on our experience at the University Hospital of Essen, Germany, operating a combined PET/CT system mandates close collaboration between nuclear medicine and radiology to assure optimization of imaging protocols for both imaging components.
For the radiologist, advantages over simple contrast-enhanced CT arise from the additional functional data offered by PET. Several studies comparing 18F-FDG PET and CT for staging different malignant diseases have determined a benefit of PET over CT when assessing metastases to regional lymph nodes (N stage) and distant organs (M stage) (2,3). For the nuclear medicine physician, the additional availability of CT data offers precise anatomic background information. Previous studies have shown an increase in diagnostic accuracy when correlating PET images with morphologic data for determination of the correct site of malignancy (4,5). This additional CT information may be even more valuable when using highly specific tracers that reveal no anatomic background information.
The question of interest to both the radiologic and nuclear medicine communities is: how much CT will be required in combined PET/CT imaging? Do we need oral and intravenous CT contrast agents or is 18F-FDG the new radiologic contrast agent that will eliminate the need for conventional CT contrast? This review addresses the complementary roles of oral, intravenous, and molecular contrast for PET/CT imaging and provides specific indications as to which contrast-enhanced CT data provide additional diagnostic value.
CT CONTRAST PROTOCOLS
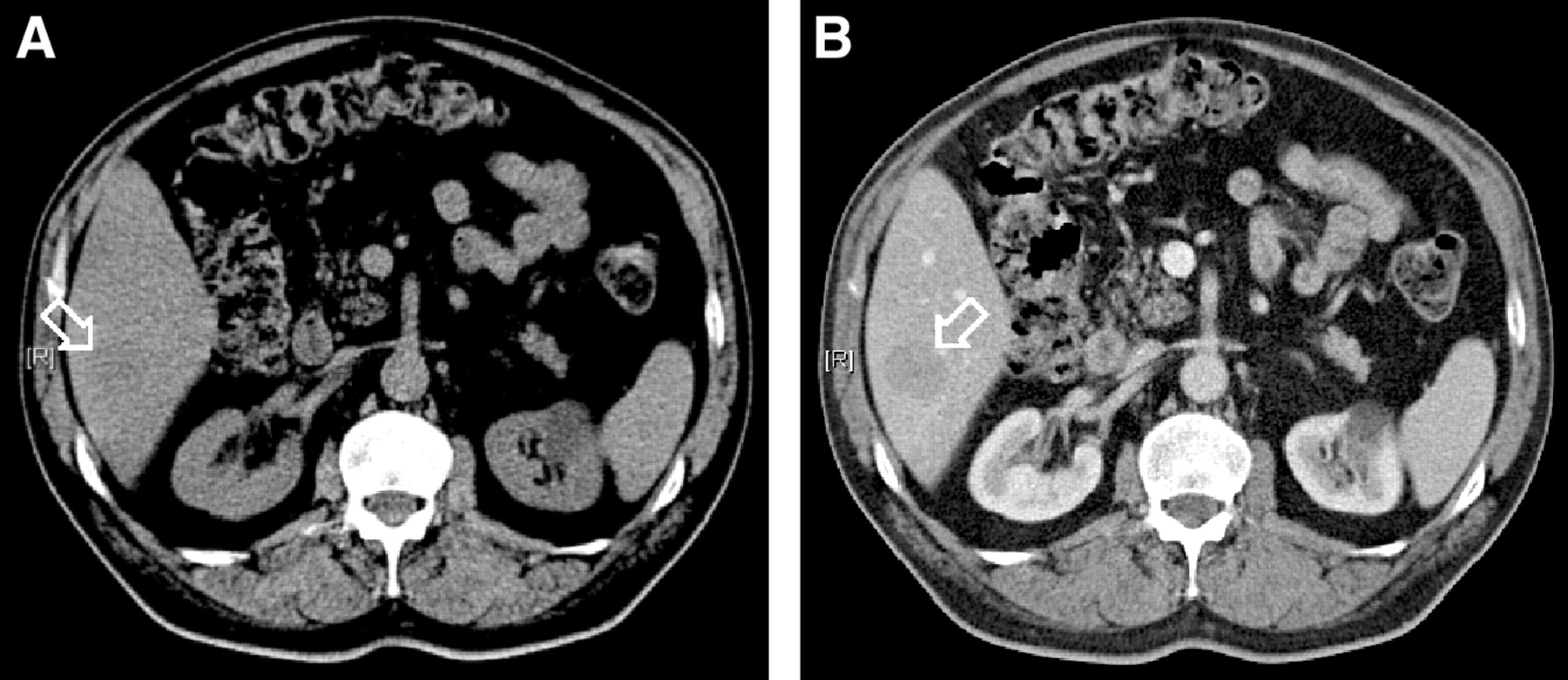
Studies comparing contrast-enhanced with nonenhanced CT protocols in the experimental setting as well as in standard radiology practice have demonstrated a substantial benefit of the contrast-enhanced approach over the nonenhanced protocol (6–13) (Fig. 1). In an experimental evaluation, Violante et al. (11) showed an increase in accuracy for detection of liver lesions (6 mm in size) from 63% to 90% when applying intravenous contrast agents. Burgener et al. (8) reported increased accuracy of contrast-enhanced images as compared with nonenhanced images when assessing infiltration of pelvic malignancies into adjacent structures. Summarizing the available literature, benefits arise from the following advantages provided by intravenous and oral CT contrast agents: (1) improved delineation of anatomic structures, (2) increased sensitivity for detection of pathologic lesions, and (3) improved accuracy in lesion characterization.
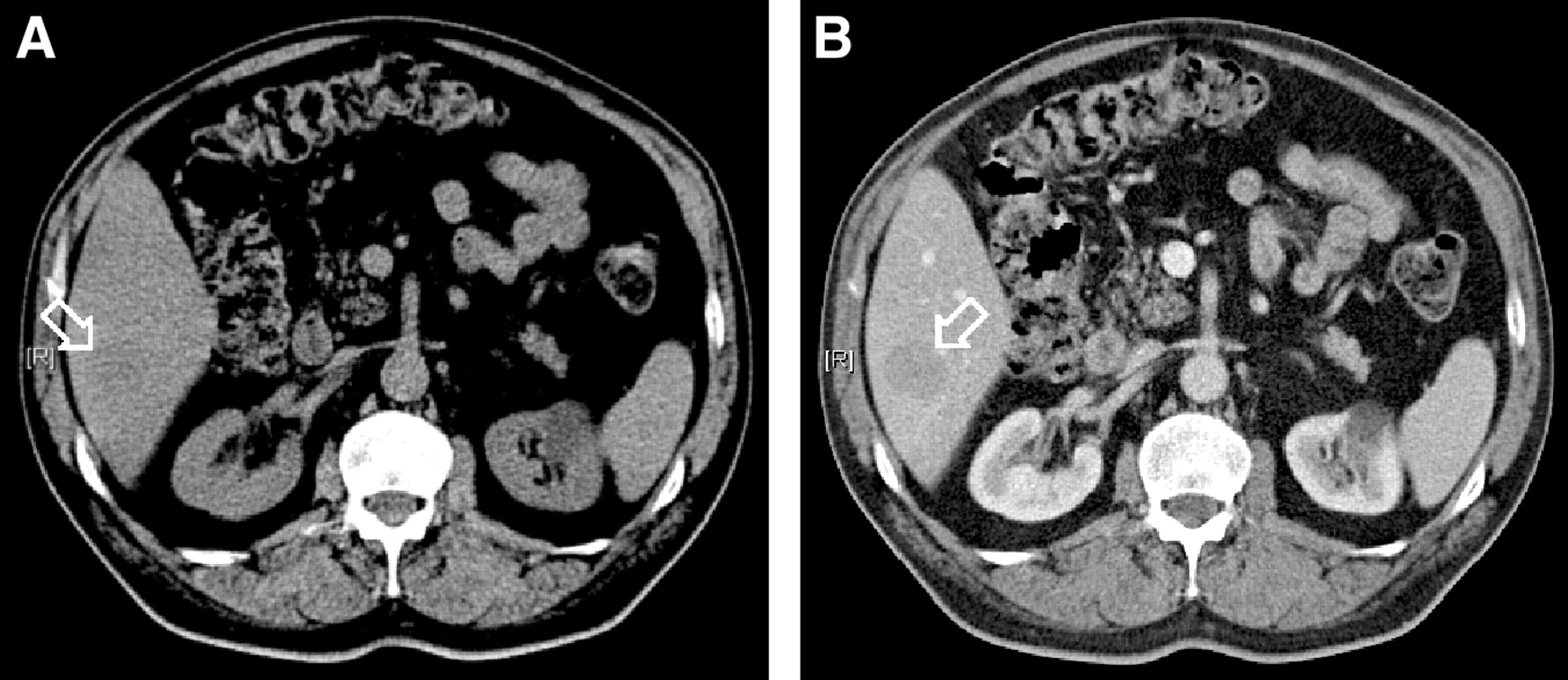
Hepatic metastasis on nonenhanced CT (A) and after application of 100 mL of an iodinated intravenous contrast agent (B). Lesion (arrows) was barely visible on unenhanced image but was clearly delineated after intravenous contrast administration.
Most CT protocols in daily radiologic routine, therefore, include contrast-enhanced images based on the application of oral and intravenous contrast agents. Oral contrast agents provide positive contrast by increase of CT attenuation (iodine, barium) or negative contrast by distension of the bowel (water-based contrast agents). Intravenous contrast agents are usually nonionic iodine-based substances. Contraindications for the application of intravenous contrast agents may arise from known allergic reactions to iodine-based contrast, hyperthyroidism, or impaired renal function. Barium must not be used in patients with known or suspected intestinal perforation/obstruction or in patients undergoing surgery of the intestine.
CT CONTRAST AGENTS IN PET/CT: TECHNICAL CONSIDERATIONS
CT Contrast Agents and PET Attenuation Correction
As a result of CT-based attenuation correction with a 2-step scaling algorithm (14) as implemented in currently available PET/CT scanners, PET attenuation can be overestimated in the presence of positive contrast agents (15–18). The resulting overestimation of the attenuation properties of contrast-enhanced structures at 511 keV may lead to image artifacts. These artifacts are correlated with Hounsfield units (HU) on CT images and appear as areas of apparently increased glucose metabolism in coregistration with areas of high contrast concentration (19). Because artifacts are found only in areas of high contrast concentrations, they rarely cause interpretation problems in the clinical setting.
Intravenous contrast artifacts are generally limited to the venous vessels carrying the undiluted contrast to the heart (19). Quantitative studies evaluating the effect of intravenous contrast agents in a canine model demonstrated only a modest effect on PET tracer quantification, with the maximal bias in parenchymal organs being 15% for the liver (18).
For clinically used concentrations of oral contrast agents, phantom measurements have found an overestimation of PET activity concentration of approximately 20% (16,20). However, Dizendorf et al. (17) reported only a 4% overestimation of the related standard uptake values (SUVs) when evaluated in clinical routine. Based on these results, the effect of oral CT contrast agents on the SUV seems to be negligible when the contrast agent is distributed homogeneously in the bowel. However, accumulation of positive oral contrast agents in the stomach, in patients with gastrointestinal stenoses, or in patients with compromised gastrointestinal motility may lead to a more severe increase in HU on CT, increasing inaccuracies in PET tracer quantification in such areas (16). Nonattenuation-corrected images can be used to solve cases of questionable image artifacts, because artifacts will be found only on attenuation-corrected data (Figs. 2 and 3).
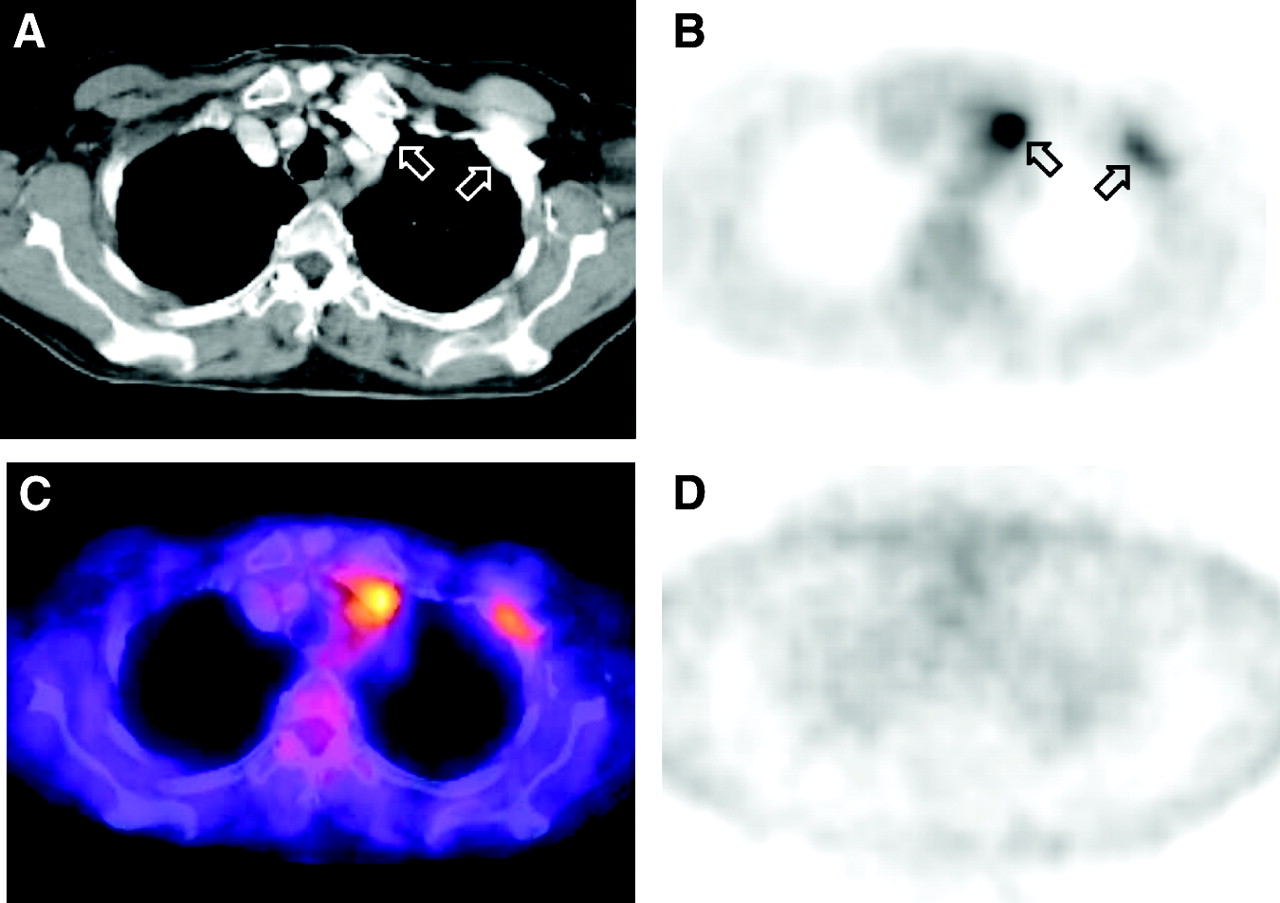
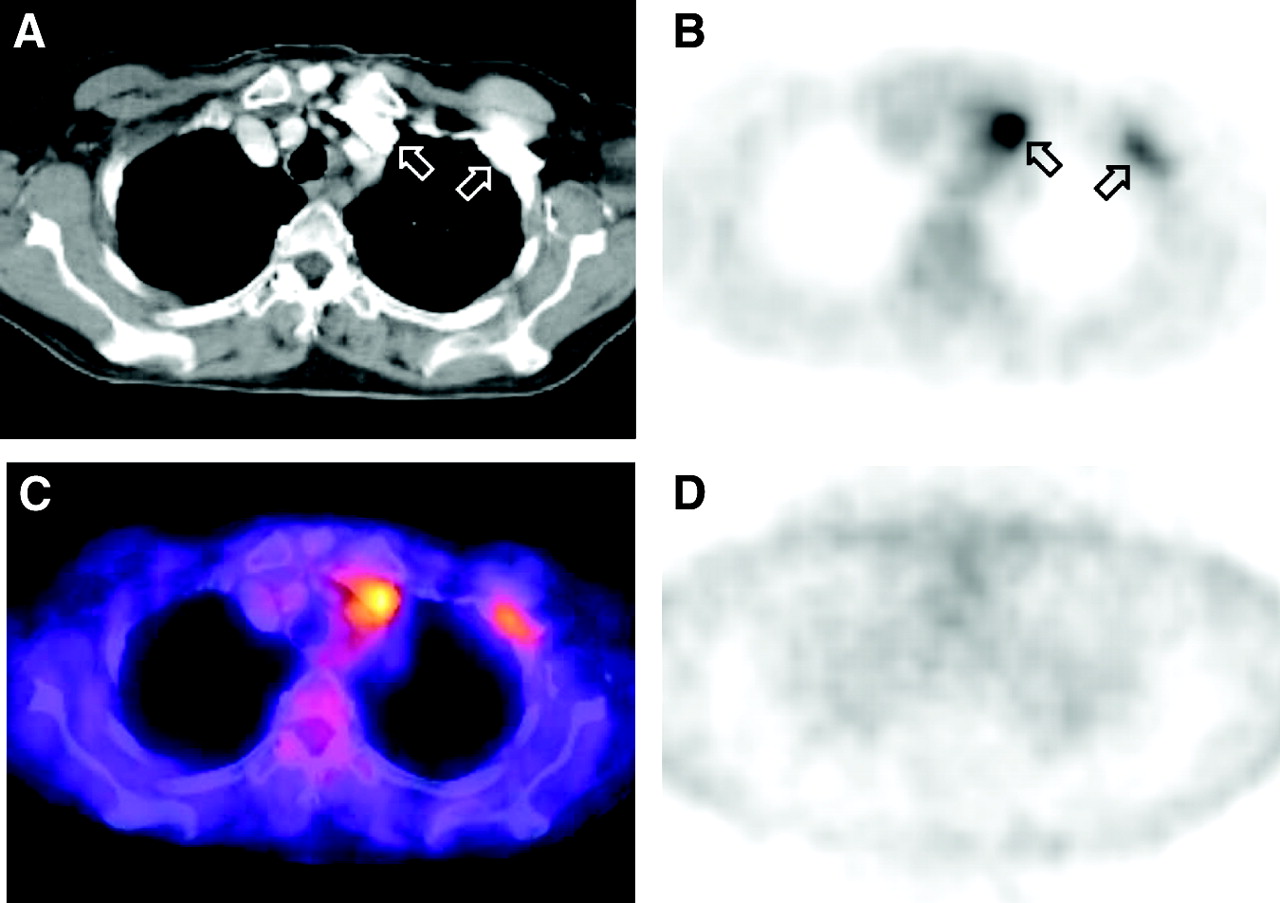
Image artifact in contrast-enhanced PET/CT studies. Bolus passage of intravenous contrast agent in left subclavian and brachiocephalic veins on CT (A, arrows) led to areas of apparently increased glucose metabolism on corrected PET (B, arrows). On fused PET/CT images, this area of apparently increased glucose metabolism correlated with high-density contrast in venous system on CT (C). PET image reconstruction without attenuation correction demonstrated homogeneous tracer distribution (D), demasking areas of apparently increased glucose metabolism as artificial.

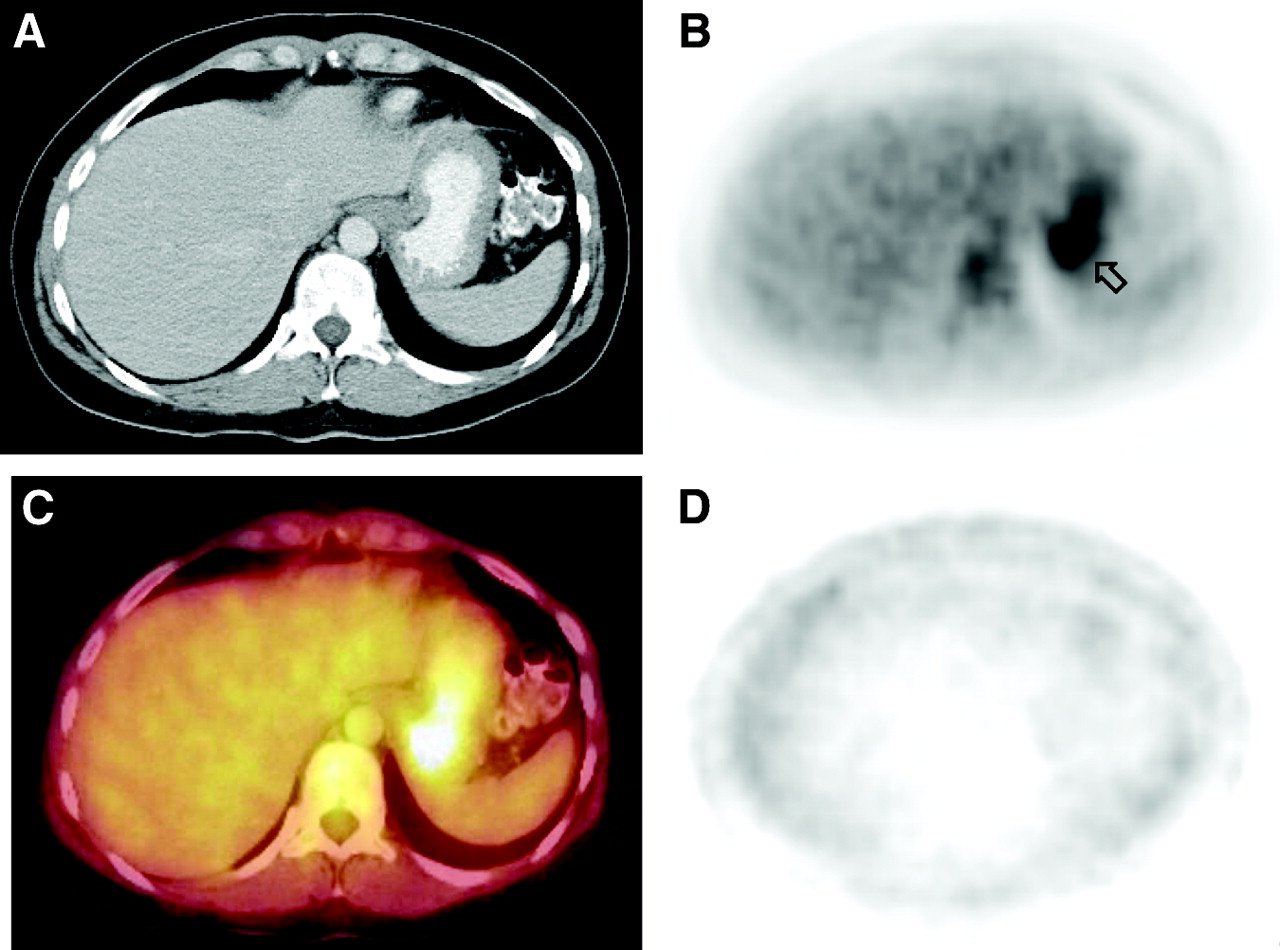
(A) Positive oral contrast agent (barium) in stomach on CT image. Area of apparently increased glucose metabolism on PET (B, arrow) corresponded to contrast-enhanced bowel lumen on PET/CT (C). (D) Homogeneous tracer distribution was seen on nonattenuation corrected PET images.
Several potential solutions have been proposed to deal with the effects of contrast agents on PET attenuation correction in PET/CT (15,21). A simple way to avoid contrast-induced artifacts with positive oral CT contrast agents is the use of a negative oral contrast agent for PET/CT imaging. These water-based contrast agents assure differentiation of bowel loops from surrounding structures by distending the bowel (Fig. 4). Unlike iodine or barium, they do not increase CT HU and, thus, cannot lead to artifacts or PET tracer quantification inaccuracies. To avoid absorption of the water in the gastrointestinal tract, different substances may be added. We routinely use a negative oral CT contrast agent based on a combination of water, 2.5% mannitol, and 0.2% locust bean gum (LBG). Mannitol increases bowel distension based on osmotic properties, and LBG avoids intestinal water absorption using a gelling action (22).

Good small-bowel distension on transverse CT image (A) with negative oral contrast agent containing water, 2.5% mannitol, and 0.2% locust bean gum. Both PET (B) and fused PET/CT (C) images were free of contrast-induced artifacts.
CT Contrast Agents: Timing Issues
In our experience, optimization of contrast-enhanced CT protocols for PET/CT can be limited by currently available soft- and hardware. An optimized contrast protocol for CT needs to assure imaging of different body regions in region-specific phases of contrast enhancement (e.g., the thorax should be scanned in the arterial phase, whereas the upper abdomen should be imaged in the portal–venous phase). This goal cannot be achieved by a single whole-body CT spiral. To improve contrast enhancement of the CT component new soft- and hardware that allow CT acquisition to be split for optimized contrast enhancement will be required (Fig. 5). To avoid additional radiation exposure from a separate nonenhanced CT, this split CT spiral will have to serve for attenuation correction of PET. Some tumor entities require CT imaging in more than a single contrast-enhancing phase. Hepatocellular carcinoma, for example, typically demonstrates contrast enhancement in the arterial phase and, therefore, requires multiphase (arterial and portal–venous) CT imaging. Protocols offering acquisition of more than one CT spiral in combination with PET are desirable.

Split CT protocol to optimize contrast enhancement in each body region. Desired contrast enhancement is arterial in thorax, portal–venous in upper abdomen, venous in pelvis, and late-venous in neck and head. To meet these requirements, PET/CT scanners need to allow whole-body acquisition starting with thorax (scanned in caudocranial direction), followed by abdomen and pelvis (craniocaudal direction), and by neck and head (caudocranial scanning).
PET/CT PROTOCOLS: CT WITH OR WITHOUT CONTRAST?
Although the use of a radioactive tracer is essential for PET and PET/CT, there is controversy about the use of oral and intravenous CT contrast agents in dual-modality PET/CT. The main question when deciding on the potential application of CT contrast agents relates to whether the CT examination is to be diagnostic or nondiagnostic. Diagnostic CT requires full-dose acquisition and the application of oral and intravenous contrast agents to enhance lesion detectability, localization, and characterization. But do we really need diagnostic CT data as part of the PET/CT? One may argue that functional data from 18F-FDG (or other PET tracers) provide sufficient lesion-to-background contrast to assure lesion detectability and characterization. 18F-FDG, then, may, serve as “the new contrast agent for CT,” rendering conventional CT contrast agents superfluous. When assessing the value of CT contrast agents in combined PET/CT, their effects on lesion detection, lesion characterization, and lesion localization must be discussed.
Lesion Detection and Characterization in Tumor Staging
It is widely accepted that lesion detection in oncologic imaging is improved by the use of 18F-FDG PET when compared with CT imaging alone (3). Based on accurate image fusion, 18F-FDG PET/CT further increases staging accuracies for many malignancies as compared with PET alone, as well as with PET and CT viewed side by side. Lardinois et al. (23) reported additional diagnostic information from fused PET/CT compared with visual image correlation in 41% of patients with non–small cell lung cancer. The effect of additional lesion detection with PET/CT on patient management was not assessed in this study. Bar-Shalom et al. (24) found PET/CT to be of additional value over CT alone and PET alone in 49% of patients with different oncologic diseases. In this study patient management was altered by PET/CT in 14% of patients previously studied with PET and CT alone. Evaluation of PET/CT in non–small cell lung cancer in our clinic revealed a statistically significant benefit of fused images over the 2 imaging modalities alone when assessing the TNM stage. Improved staging with PET/CT had an effect on patient management in 15% of patients previously staged by PET alone and 19% previously staged by CT alone (25). Although data from our clinic included contrast-enhanced CT as part of the combined PET/CT, other studies used nonenhanced CT. Therefore, both contrast-enhanced and nonenhanced PET/CT seem to improve staging over conventional imaging. Data comparing diagnostic accuracies of contrast-enhanced with nonenhanced PET/CT with regard to lesion detection and characterization are not yet available.
Some malignant tumors, however, do not demonstrate increased 18F-FDG uptake or only express a mild increase in glucose utilization compared with surrounding tissues. If a tumor or its metastases turn out to be 18F-FDG PET–negative, the availability of diagnostic CT data from combined PET/CT can strongly improve lesion detection and characterization. By increasing attenuation differences between anatomic structures, lesion detection will be enhanced, and the pattern of contrast-enhancement can aid lesion characterization (6–11). Thus, application of CT contrast agents can increase CT performance beyond anatomic correlation and attenuation correction for PET (Fig. 6). Experiences with PET/CT at our hospital indicate a benefit in lesion detection and characterization in 11% of patients when using contrast-enhanced CT rather than nonenhanced CT data for combined PET/CT imaging. These data refer to a patient population with different oncologic diseases. However, it must be stated that in the majority of patients lesion detection and characterization are mainly based on functional data in 18F-FDG–avid tumors.
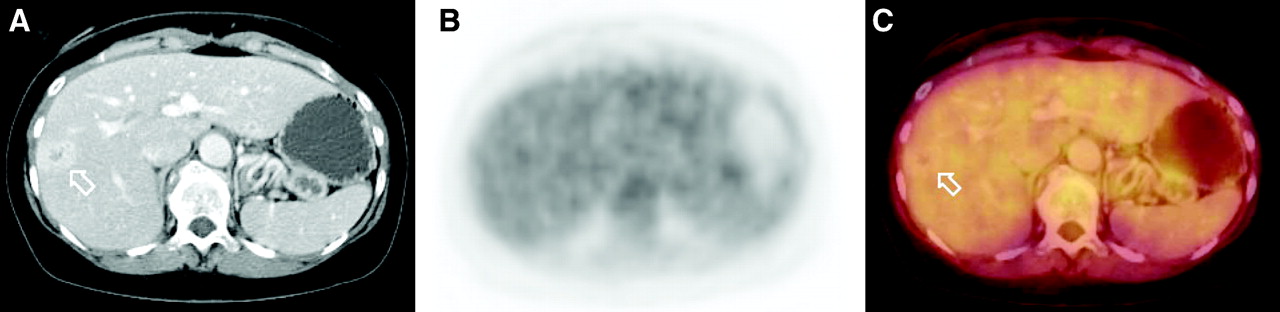
Hepatic metastasis from uveal melanoma in 58-y-old woman. (A) Contrast-enhanced CT clearly depicted lesion (arrow) in right liver lobe. (B) PET imaging was found to be negative for malignant disease. (C) Diagnosis of metastatic disease was based on CT data when evaluating fused images. Metastatic disease to liver was proven by histopathology.
Lesion Localization in Tumor Staging
Based on an increase in 18F-FDG uptake, most malignant lesions can be distinguished clearly from background activity on 18F-FDG PET. An advantage of PET/CT compared with PET alone is the ability to accurately localize these lesions by providing intrinsic alignment of PET and CT datasets. On nonenhanced CT scans, however, differentiation of anatomic structures with similar density is frequently compromised (6–8). This can be only partially compensated for with 18F-FDG by increasing contrast between a lesion and its background. Differentiation of an area of physiologic 18F-FDG uptake from pathologic 18F-FDG utilization may be impossible if the area of increased glucose metabolism cannot be clearly localized within a specific morphologic structure. Thus, increased 18F-FDG uptake may be pathologic if fused with a lymph node or physiologic if coregistered with the bowel or stomach. Based on our experience, the availability of contrast-enhanced CT data improves confidence to accurately localize a PET-positive lesion in approximately 25% of patients. This advantage also relates to tumors with high 18F-FDG-uptake. Therefore, imaging protocols at our institution include contrast-enhanced data independent of the tumor type (26). The problem of lesion delineation and localization relates to all body regions, but it is most pronounced in the head and neck as well as the abdomen and pelvis. In the head and neck, intravenous contrast agents assure differentiation of malignant lesions from adjacent blood vessels, thyroid, salivary glands, and muscles (Fig. 7). In the abdomen and pelvis, intravenous and oral contrast agents are used to accurately delineate lesions adjacent to bowel loops, stomach, mesenteric and iliac blood vessels, and parenchymal organs (Fig. 8). In our experience, the availability of a diagnostic CT scan performed before the combined PET/CT examination rarely obviates the need for diagnostic CT data as part of the “diagnostic PET/CT” protocol. Separate CT scans frequently cover only a single body region rather than the same field of view as the whole-body PET/CT. When staging a patient for distant metastases, application of intravenous and oral contrast agents, therefore, is still required to provide adequate contrast enhancement in all body regions. A different approach, in which a low-dose and unenhanced PET/CT is performed and may be followed by a contrast-enhanced CT in equivocal findings, seems rather impractical for routine practice. For accurate fusion of the 2 examinations, the CT would have to be performed without repositioning of the patient. This demands that a physician be available for image assessment immediately after the PET/CT examination and would result in a lowering of patient throughput because of additional time requirements for image review.

Small lymph node adjacent to thyroid gland. (A) As result of contrast enhancement of thyroid after application of iodine-based intravenous contrast agent, hypodense lymph node (arrow) was clearly distinguished from thyroid parenchyma. Increased 18F-FDG uptake on PET (B) was accurately attributed to this lymph node rather than to thyroid gland (C). Without contrast enhancement, similar densities of parenchymal organs and lymph nodes frequently render differentiation of organ metastasis from adjacent lymph node metastasis difficult.

(A and B) On nonenhanced images, differentiation of lymph node from lesion (arrow) within stomach wall was not possible. (C and D) When applying intravenous contrast agents in a different patient, contrast enhancement of stomach wall was clearly distinguished from hypodense lesion adjacent to stomach wall, thus identifying lesion as abdominal lymph node (arrows).
The use of low-dose CT without contrast agents, however, can be considered as part of PET/CT in some applications. In patients undergoing follow-up studies to assess the effect of radiation therapy or chemotherapy, a nonenhanced CT scan with low-dose technique will be adequate after initial staging. Based on an effective dose of approximately 17 mSv from a diagnostic whole-body CT scan (head to upper thighs), this may be of particular relevance in younger patients undergoing potentially curative therapy. Table 1 summarizes different CT protocols in use for combined PET/CT at our institution.
Indications for CT Contrast Agents in Combined PET/CT
PET/CT FOR TREATMENT PLANNING AND FOLLOW-UP
Radiation Therapy
In radiation therapy planning, functional data provided by PET in combination with accurate anatomic localization alter the target volume when compared with CT alone (27,28) and provide additional information for monitoring of radiation therapy over that provided by viewing CT and PET side by side (29). When using PET/CT for radiation therapy planning and follow-up in 18F-FDG–avid tumors, CT data provide anatomic correlation for PET. No studies are currently available comparing contrast-enhanced and unenhanced PET/CT for target volume definition and follow-up. In our experience, the decision on contrast-enhanced versus nonenhanced CT depends strongly on the location of the tumor. As discussed previously, additional information derived from contrast-enhanced CT concerning lesion localization is most accentuated in the head and neck and in the abdomen and pelvis. Accurate differentiation of tumor tissue from adjacent organs is important to prevent inclusion of radiation-sensitive organs in the planning target volume. We, therefore, perform a contrast-enhanced CT as part of the PET/CT for therapy planning in these body regions. A nonenhanced CT, however, will still be required for dose calculation in these patients. In patients with thoracic tumors, PET/CT may be performed unenhanced for radiation therapy planning. Only when direct mediastinal tumor invasion is suspected will contrast agents be applied to improve delineation of potential vascular infiltration. Follow-up of patients undergoing irradiative therapy is mostly based on functional data provided by PET. Nonenhanced PET/CT, therefore, will be sufficient to differentiate responders from nonresponders.
Surgery
The benefits of PET/CT in planning for surgery are 2-fold. First, the decision as to whether the patient would benefit from an operation is based on the TNM stage. More accurate TNM staging by PET/CT has been shown to positively affect patient management with regard to choosing palliative or surgical/curative therapy (24,25). Second, accurate localization of a lesion will guide the surgeon to the pathology. To date, no data is available on the effects of accurate fusion of anatomic and functional data by PET/CT on surgical procedures. Both TNM staging and potential guidance of a surgeon to a lesion rely strongly on accurate lesion localization. PET/CT for surgical planning, therefore, is performed contrast enhanced at our institution.
Interventional Procedures
Guidance of biopsies and interventional procedures is generally based on morphologic imaging. Because many lesions are only poorly depicted on nonenhanced images, contrast-enhanced datasets are used for interventional planning before the needle is advanced into the lesion. Some lesions, however, are characterized by only poor vascularization. In these cases, additional 18F-FDG PET data can be of substantial benefit in assessing tumor size and defining viable tumor tissue.
Biopsy.
Most tumors are characterized by different types of tissue. Thus a single tumor may contain areas of well and poorly differentiated tumor cells as well as necrotic and viable tumor tissue. Depending on the biopsy site, this tissue heterogeneity can strongly affect histopathology. In cases of equivocal CT findings, 18F-FDG PET/CT can be used to differentiate viable tumor from necrosis. All patients referred to PET/CT for biopsy planning have already undergone contrast-enhanced CT imaging. Thus, the PET/CT will be performed unenhanced. It is important to emphasize that PET alone will not be sufficient in these patients, because accurate image fusion is mandatory to guide the interventional radiologist to the precise tumor region. Considering the higher cost of PET/CT compared with CT alone, the indication for PET/CT–guided interventions should be considered well. The accuracy of CT-guided needle biopsies has been found to range between 82% and 88% for typical indications such as liver tumors, lung nodules, or lymphoma (30–32). In accordance with these data, we have determined equivocal findings on contrast-enhanced CT in about 10% of patients undergoing biopsy. These patients undergo PET/CT–guided biopsy planning.
Interventional therapy.
The 2 main types of interventions are potentially curative interventional tumor therapy (e.g., radiofrequency ablation) and palliative procedures (e.g., chemoembolization of a liver tumor) (33–36). PET/CT offers support for both. Thermal tumor ablation based on either laser or radiofrequency represents a curative approach to tumor therapy. This mandates ablation of the entire tumor, which, in turn, requires accurate needle placement. Once the needle is placed in the center of the tumor, tumor destruction is achieved by applying thermal energy through an external power generator (35,36). If, however, the needle tip is not centralized within the tumor, thermal ablation may be incomplete, resulting in residual tumor cells in the periphery of the lesion. On morphologic imaging, needle placement is usually performed based on multiplanar reconstructions of ultrasound or CT images to assure a central needle position (37). We have determined a benefit of combined PET/CT over contrast-enhanced CT alone in half of all patients with respect to definition of viable tumor tissue and location (Fig. 9). Thus, PET/CT is performed instead of conventional contrast-enhanced CT in all patients before tumor ablation. Because no separate contrast-enhanced CT is performed, we use contrast-enhanced PET/CT data in all of these patients. Without regard to tumor histology, contrast enhancement is necessary in all patients preinterventionally to clearly visualize all vascular structures that may cause severe bleeding if injured during the intervention. All patients are also referred to PET/CT for follow-up examinations after interventional therapy, because integration of functional data has been shown to be more sensitive than morphology for detection of residual tumor or tumor recurrence (38,39) (Fig. 10).

Patient (56-y-old man) 1 y after local resection of hepatic metastasis. (A) Two hypodense lesions (arrow and arrowhead) were found on contrast-enhanced CT, but differentiation of viable tumor tissue from postoperative tissue alteration was not possible. (B) PET imaging demonstrated viable tumor tissue but without additional ability to accurately localize lesion within liver. (C) On fused PET/CT, lateral hepatic lesion was identified as local tumor recurrence (arrow), and medial lesion was caused by postoperative tissue alteration (arrowhead). (D–F) Radiofrequency ablation was selectively performed on lateral lesion, and complete tumor ablation was shown on postinterventional follow-up scan.

Patient (83-y-old man) with hepatocellular carcinoma of right liver lobe after transarterial chemoembolization. (A) On transverse contrast-enhanced CT image hyperdense chemoembolizing agents were visible, but differentiation of viable tumor tissue from normal liver parenchyma and necrotic tumor areas was difficult. PET image (B) clearly demonstrated residual viable tumor that could be accurately localized based on PET/CT data (C). By providing accurate anatomic localization of remaining tumor tissue, PET/CT aided further interventional planning.
Biopsies and therapeutic interventions do not have to be performed within the PET/CT unit. Interventions to critical parts of the body (close to large vessels or vulnerable organs) may require up to 60 min, which leads to an unacceptably long occupation of the PET/CT scanner. In these cases, the PET/CT can be performed shortly before the intervention. The PET/CT data are then transferred to a CT workstation, where they are fused manually with the CT data from the intervention to follow the placement of the biopsy needle in the context of the functional information (Fig. 11).
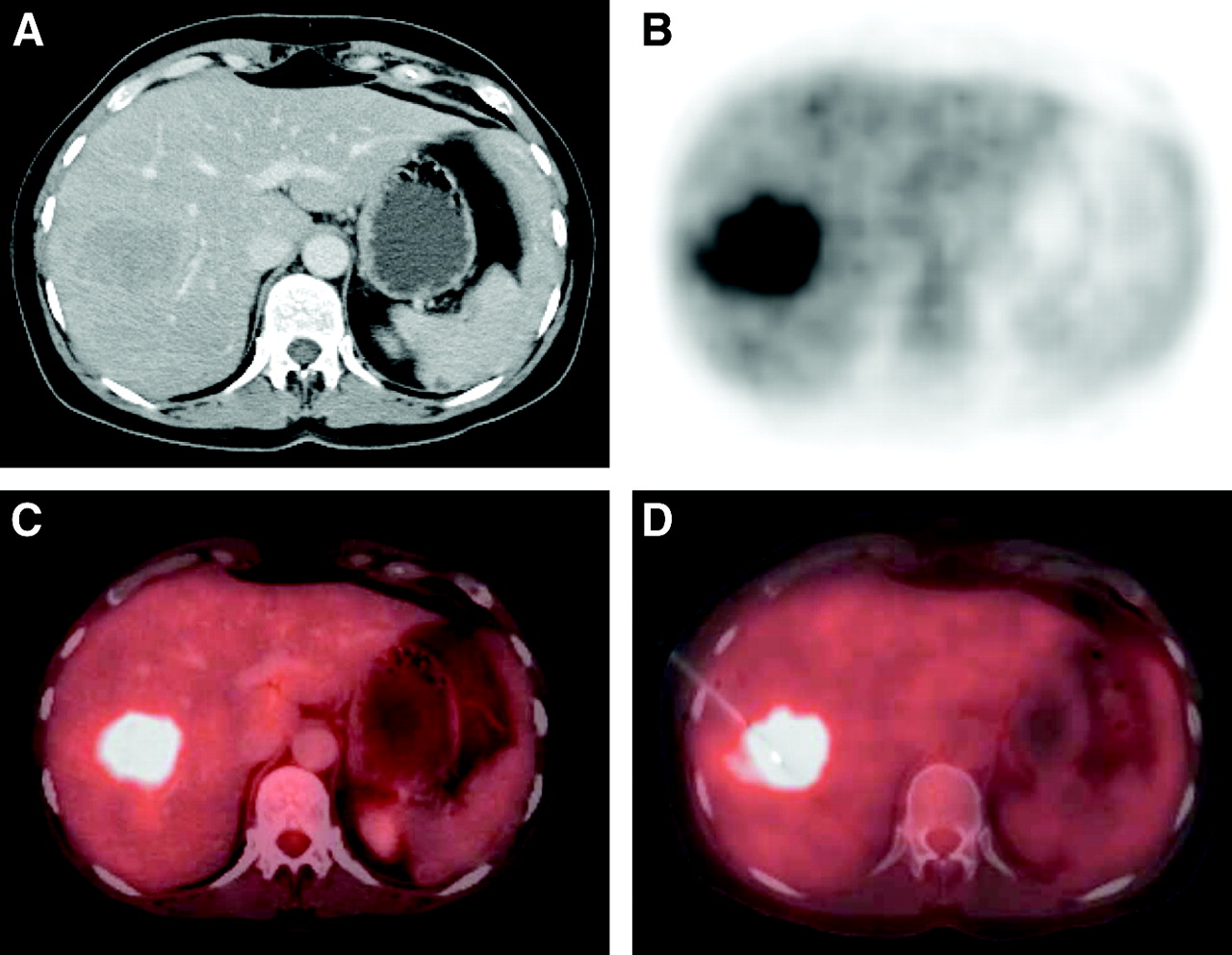
Hepatic metastasis in 47-y-old female patient with cancer of unknown primary. (A) Contrast-enhanced CT could not clearly distinguish between viable tumor tissue and normal liver parenchyma. (B) PET imaging demonstrated increased glucose metabolism. (C) Increased tracer uptake was accurately localized based on PET/CT images. (D) Additional manual fusion of PET/CT images with interventional images showed biopsy device to be within viable tumor tissue.
An unsolved issue with clinical PET/CT relates to the limited ability of 18F-FDG PET to differentiate regeneration and inflammation from tumor (40,41). Particularly in patients undergoing interventional procedures, regenerative tissue in the periphery of the induced necrotic area may be mistaken for residual or recurrent tumor (Fig. 12). A similar problem occurs when morphologic imaging is used to assess the effect of interventional therapy. Early arterial contrast enhancement in the periphery of the induced necrosis is typically found on CT and MR images. This type of enhancement is difficult to differentiate from residual tumor. Clinical and experimental studies addressing this issue are required to optimize PET/CT for biopsy and interventional therapy.

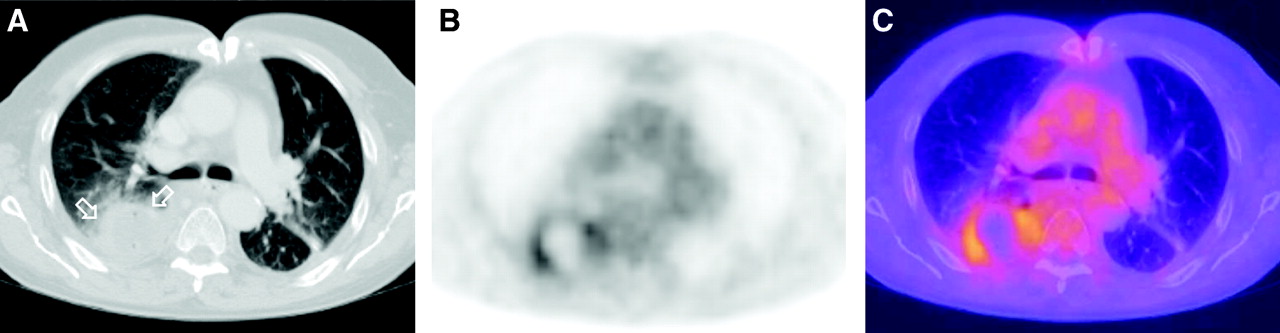
Patient (64-y-old man) 2 wk after radiofrequency ablation of pulmonary metastasis in right lower pulmonary lobe. (A) Round area of necrosis and hematoma (arrows) was found postinterventionally on CT. PET imaging demonstrated rim-like area of increased glucose metabolism (B) that correlated with periphery of necrotic zone on PET/CT (C). This increase in tracer uptake in periphery of lesion may have been result of tissue regeneration or viable tumor. Further follow-up in this patient revealed decrease in peripheral tracer uptake over time. Thus, increased peripheral glucose metabolism was found to be result of tissue regeneration rather than residual tumor.
CONCLUSION
Contrast-enhanced CT data as part of the combined PET/CT examination provide additional information when compared with nonenhanced PET/CT. Because CT data supply anatomic background for PET, the most important benefit relates to more precise anatomic localization of a pathology by differentiation of the lesion from its surrounding structures. By supporting lesion detection and characterization, CT contrast agents can be of additional value in 18F-FDG PET–negative tumors. Contrast-enhanced PET/CT can provide fully diagnostic morphologic and functional data in a single session, rendering additional diagnostic CT unnecessary. CT contrast agents and 18F-FDG, therefore, do not compete but rather complement each other in combined PET/CT imaging.
Acknowledgments
The authors would like to thank Sandra Pabst, RT; Bärbel Terschüren, RT; Lydia Schostok, RT; and Slavko Maric (RT) for their support with the acquisition of the PET/CT data. We gratefully acknowledge the substantial support of Hilmar Kuehl, MD, Jörg Stattaus, MD, Thomas Egelhof, MD, and Stefan P. Mueller (MD) in defining PET/CT imaging protocols.
Footnotes
Received Sep. 15, 2003; revision accepted Nov. 14, 2003.
For correspondence or reprints contact: Gerald Antoch, MD, Department of Diagnostic and Interventional Radiology, University Hospital Essen, Hufelandstrasse 55, 45122, Essen, Germany.
E-mail: gerald.antoch{at}uni-essen.de
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Performance of 18F-FDG PET/CT According to Delay After Treatment to Detect Subclinical Recurrence of Head and Neck Squamous Cell Carcinoma
- Diagnostic Contribution of Contrast-Enhanced CT as Compared with Unenhanced Low-Dose CT in PET/CT Staging and Treatment Response Assessment of 18F-FDG-Avid Lymphomas: A Prospective Study
- Pitfalls and Pearls of Wisdom in 18F-FDG PET Imaging of Tumors
- Techniques, Benefits, and Challenges of PET-MR
- Expert Opinions on Positron Emission Tomography and Computed Tomography Imaging in Lymphoma
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Role of PET/CT Scanning in Initial and Post-Treatment Assessment of Hodgkin Disease
- Dual-Modality Imaging: Combining Anatomy and Function
- Morphologic and Functional Changes in Nontumorous Liver Tissue After Radiofrequency Ablation in an In Vivo Model: Comparison of 18F-FDG PET/CT, MRI, Ultrasound, and CT
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Use of Positron Emission Tomography for Response Assessment of Lymphoma: Consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma
- Introduction
- Can PET/CT Replace Separate Diagnostic CT for Cancer Imaging? Optimizing CT Protocols for Imaging Cancers of the Chest and Abdomen
- PET/CT in Lymphoma: Prospective Study of Enhanced Full-Dose PET/CT Versus Unenhanced Low-Dose PET/CT
- Optimized Contrast-Enhanced CT Protocols for Diagnostic Whole-Body 18F-FDG PET/CT: Technical Aspects of Single-Phase Versus Multiphase CT Imaging
- Standard PET/CT of the Chest During Shallow Breathing Is Inadequate for Comprehensive Staging of Lung Cancer