


Abstract
The incidence of malignancy associated with subcentimeter pulmonary nodules (micronodules) in patients with malignant disease has been reported to be as high as 58%. Thus, detection of small lung nodules is important for appropriate staging of lung cancer. Because of respiratory motion, small parenchymal lung lesions can be missed on CT acquired during shallow breathing. Micronodules are usually too small to be characterized reliably with 18F-FDG PET. We aimed to determine the incidence of missed pulmonary micronodules on PET/CT studies acquired during shallow breathing. Methods: The study included 142 consecutive cancer patients (62 male and 80 female; mean age, 54 y) who underwent whole-body PET/CT during shallow breathing and breath-hold CT of the chest during maximal inspiration. CT findings were reviewed independently, and noncalcified nodules missed on the shallow-breathing scan were evaluated for size, location, and metabolic activity. Results: Breath-hold chest CT detected an additional 125 parenchymal lung nodules (mean size, 3.4 ± 1.6 mm; range, 1−9 mm) in 48 (34%) of the 142 patients. In these patients, 3 nodules, on average, were missed during shallow breathing. In 18 patients (13%), micronodules were identified exclusively on breath-hold images. None of the missed nodules demonstrated 18F-FDG uptake. Conclusion: Acquisition of standard PET/CT chest images during shallow breathing is inadequate for comprehensive cancer staging.
The increasing use of PET/CT has led to the development of new imaging protocols to optimize fusion of PET and CT images. With current multidetector-CT technology, anatomic images of the chest or even the whole body can be acquired within seconds to minutes (1,2). Acquisition times for PET images, however, range from 7 min with lutetium oxyorthosilicate crystal–based technology (3,4) to more than 30 min for bismuth germanate crystal–based PET systems (5).
To optimize coregistration, both the CT and the PET portions of the examination are acquired during continuous shallow breathing (6–9). Respiratory motion does not significantly compromise the interpretation of PET images but does result in an unsatisfactory evaluation of the lung parenchyma on CT images. Subcentimeter nodules can be missed, and normal anatomic structures such as blood vessels can have an ambiguous appearance suggesting abnormality where there is none (10–12). The limited sensitivity of PET for subcentimeter lesions further limits the characterization of small pulmonary nodules (13,14).
The incidence of malignancy in subcentimeter pulmonary nodules (micronodules) of patients with known malignancy has been reported to range from 10% to 58% (15–18). Thus, identifying subcentimeter nodules has important implications for the staging and restaging of cancer and for establishing prognosis and initiating the most appropriate treatment.
The aim of the current study was to determine the incidence at which pulmonary micronodules are missed on PET/CT studies acquired during shallow breathing.
MATERIALS AND METHODS
Patient Population
This study included 142 consecutive patients (62 male and 80 female; mean age, 54 ± 28 y; range, 4−88 y) who underwent PET/CT between April 1 and June 30, 2004, and breath-hold CT of the chest during maximal inspiration. The PET/CT study was indicated for staging and restaging of various types of cancer (Table 1). The study complied with the regulations of the UCLA Institutional Review Board and of the Health Insurance Portability and Accountability Act.
Indications for PET/CT in the 142 Patients
Image Acquisition
PET/CT was performed using the Reveal RT scanner (CPS Innovations). This system combines a dual-slice-detector CT scanner (Somatom Emotion; Siemens Medical Systems) with an ECAT ACCEL PET scanner (Siemens/CPS Innovations).
While resting on a reclining chair, the patients received a 7.8 MBq/kg dose of 18F-FDG intravenously and drank 900 mL of barium sulfate. The imaging sequence began 60 min after tracer injection, after the patients had been placed on the scanner table in the arms-up position. We first obtained an initial scout scan to define the imaging field, followed by a low-dose (130 kVp, 35 mAs, 4-mm slice collimation, and pitch of 2) maximum-inspiration breath-hold CT scan of the chest. Immediately afterward, whole-body CT with intravenous contrast material was performed using the following parameters: 130 kVp, 120 mAs, 1-s tube rotation, 4-mm slice collimation, and bed speed of 8 mm/s (i.e., pitch of 2). This scan was followed by the PET emission scan, using a weight-based protocol as recently described (3,4). Scanning encompassed 6–8 bed positions (depending on patient height) from the mid thigh to the base of the skull.
Image Reconstruction
CT images were reconstructed using conventional filtered backprojection, at 3.4-mm axial intervals to match the slice separation of the PET data. PET images were reconstructed using iterative algorithms (ordered-subsets expectation maximization: 2 iterations and 8 subsets) to a final image resolution of 8.8 mm in full width at half maximum. Attenuation was corrected by mapping the CT Hounsfield units to the linear attenuation coefficients as previously described (19,20).
The low-dose breath-hold CT scan of the chest was reconstructed using conventional filtered backprojection at 5-mm axial intervals.
Image Analysis
The 142 patients were identified retrospectively. The 2 sets of CT studies (shallow breathing and breath hold) were analyzed prospectively and by consensus by 2 radiologists and 1 nuclear medicine specialist who were unaware of the patient's history and other imaging findings. The viewing station of a picture archiving and communication system was used for review of the CT images. Syngo software (Siemens) was used for review of the fused images. CT scans were presented to the readers in a random and unpaired sequence. All noncalcified nodules missed on the shallow-breathing scan were evaluated for size (largest diameter) and location. 18F-FDG uptake was assessed visually and was defined as positive if greater than the level of the surrounding lung tissue.
RESULTS
A total of 160 noncalcified lung nodules smaller than 1 cm were detected on CT scans acquired during shallow breathing.
Breath-hold CT detected 125 additional noncalcified lung nodules smaller than 1 cm in 48 (34%) of 142 patients. In 18 of these 48 patients (i.e., 13% of the study population of 142 patients), 38 small lung nodules were detected only on the breath-hold CT scan, with an average of 2 nodules missed on the images acquired during shallow breathing. Eighty-seven additional nodules (an average of 3 nodules missed on the images acquired during shallow breathing) were detected in 30 of these 48 patients in addition to nodules seen in the shallow-breathing images.
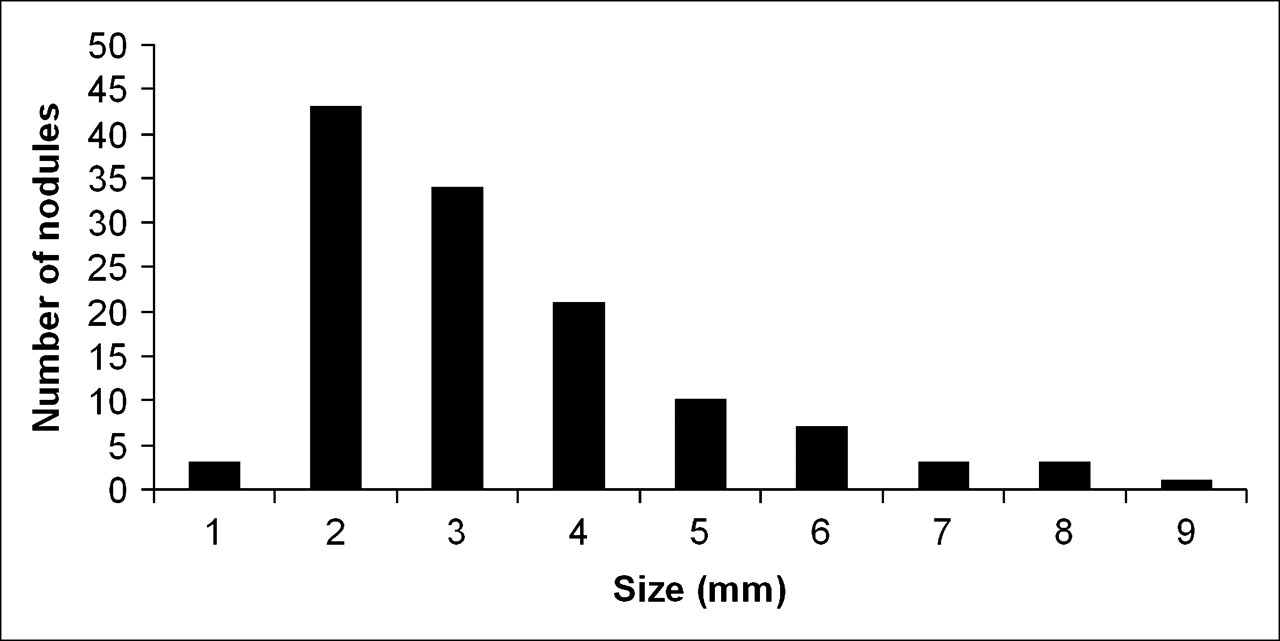
The size of the missed nodules ranged from 1 to 9 mm (Figs. 1–3⇓⇓) and averaged 3.4 ± 1.6 mm. The left lower lobe of the lung was the most frequent location at which nodules were missed (Table 2). None of the missed nodules demonstrated 18F-FDG uptake.
Distribution of the 125 Nodules Missed on Shallow-Breathing CT

Size distribution of nodules missed on shallow-breathing CT.

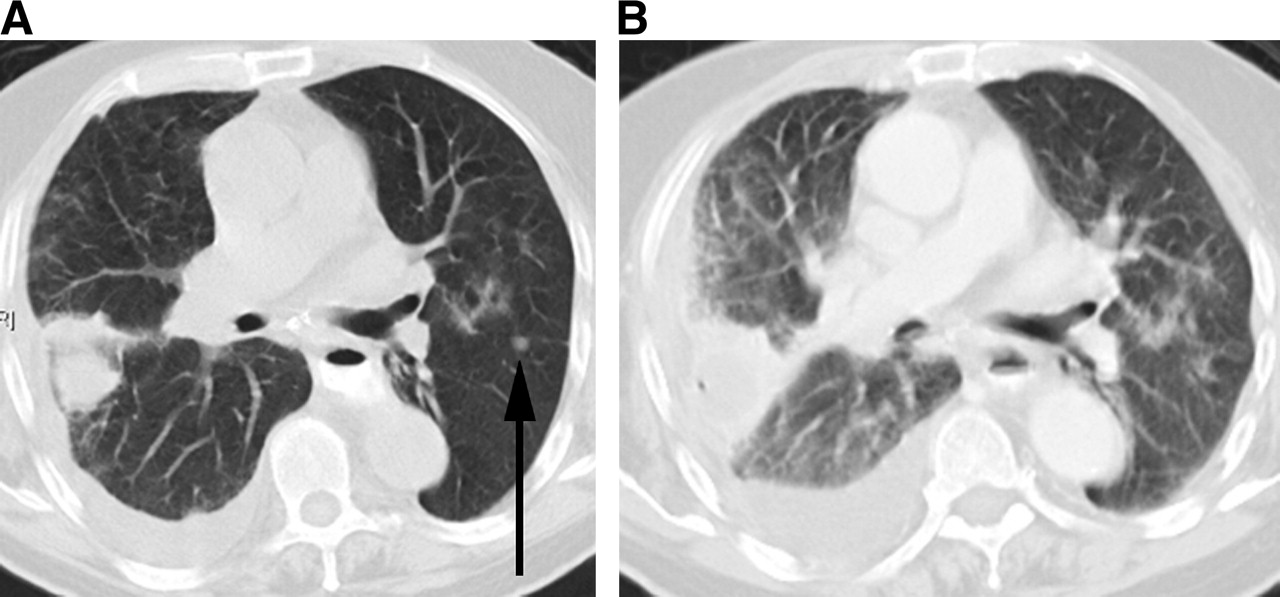
A 7-mm nodule (arrow) seen on maximum-inspiration CT (A) and missed on shallow-breathing CT (B) in left lower lobe of lung in patient with lung cancer.

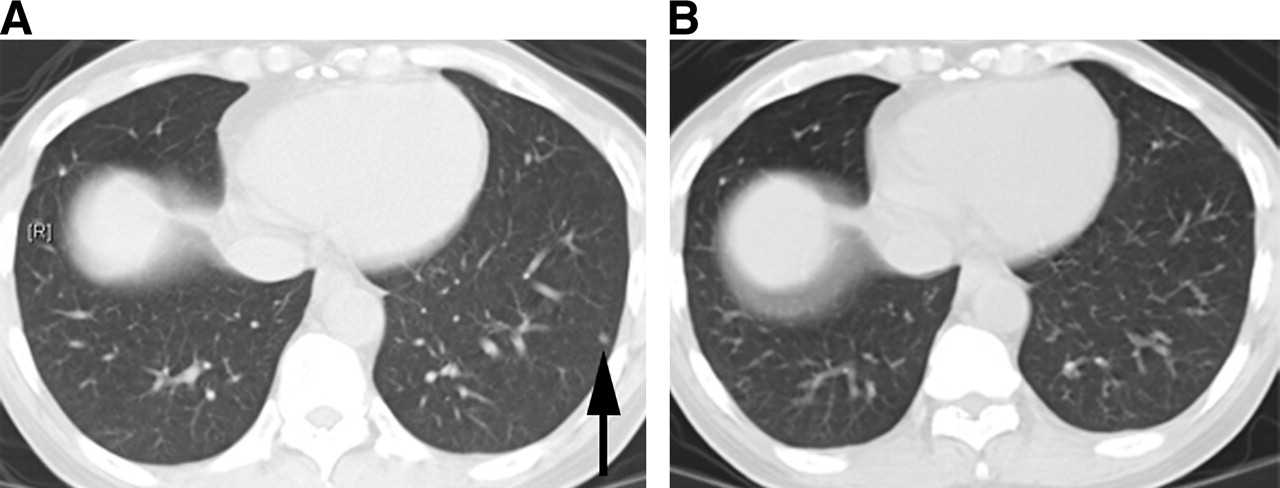
A 4-mm nodule (arrow) seen on maximum-inspiration CT (A) and missed on shallow-breathing CT (B) in left lower lobe of lung in patient with pancreatic cancer.
DISCUSSION
Significance of Micronodules
The prevalence of malignancy in micronodules detected on screening CT of the chest appears to be low, and there has been extensive debate over what constitutes the optimal management of incidentally detected small lung nodules (21–23). However, the incidence of malignancy associated with micronodules in the oncologic population has been reported to range from 10% to 58% (15–18) and probably depends on the underlying malignancy (24,25). In clinical practice, however, the statistical likelihood that a certain cancer will metastasize to the lung will be of only limited value for decisions on an individual patient's management. It is therefore prudent at least to adopt a strategy of close follow-up, even in patients with underlying malignancies that are only rarely associated with lung metastases.
Six of the 18 patients with micronodules that were detected only on the breath-hold studies did have significant metastatic disease elsewhere in the body. Conversely, 12 (66.6%) of the 18 patients had no evidence of other metastatic disease. In these patients, the detection of micronodules would have changed patient management, resulting in close follow-up of the micronodules.
How Much CT?
The results of our study have important implications for diagnosis, treatment, and prognosis. PET/CT is increasingly being proposed for use as a single, comprehensive modality for staging and restaging of cancer. Yet how much CT is needed is still a matter of controversy. Some have proposed that all CT should be done with intravenous contrast material (26), whereas others (27) have questioned the necessity of this approach.
When the lung parenchyma is assessed by CT alone, referring physicians expect the highest diagnostic quality, and breath-hold imaging sequences are considered the state of the art (10–12). Patients referred for PET/CT frequently undergo other imaging studies, including breath-hold CT of the chest. In these patients, an additional breath-hold CT scan of the chest as part of the PET/CT examination would not be necessary. However, the current study demonstrates the importance of breath-hold CT for a comprehensive assessment of cancer patients.
PET and Lesion Size
Because the spatial resolution of current PET scanners is approximately 6−8 mm (28), small lung nodules are not well characterized with 18F-FDG PET. A metaanalysis by Gould et al. found a high number of false-negative PET results for nodules smaller than 1 cm (13). In a more recent study by Nomori et al. looking at the performance of PET in small lung nodules, all malignant nodules smaller than 1 cm gave false-negative PET findings (14). These results were further supported by Crippa et al. (29), who reported a sensitivity of only 23% for detecting tumor-involved lymph nodes 5 mm or smaller in melanoma patients, despite the high glycolytic activity of this type of cancer. Thus, the sensitivity of PET for detecting cancer in small lesions is limited. Adding low-dose breath-hold CT of the chest represents a feasible approach to overcoming the limitations of current PET/CT protocols.
Radiation Dose
Depending on the examination parameters, CT of the chest can result in a radiation dose of up to 27 mSv (30). However, the additional radiation from low-dose CT of the chest amounts to less than 2 mSv (31). This seems a relatively small increment, with negligible additional risks, given that the dose received from whole-body PET/CT is approximately 30 mSv (32). Cancer patients usually undergo multiple radiologic procedures during the course of diagnosis, treatment, and follow-up. Because a single, comprehensive whole-body examination limits the need for additional radiologic examinations, the overall radiation dose received might actually be reduced. This consideration, together with the importance of accurate cancer staging and restaging, justifies the small additional exposure of patients to radiation.
PET/CT has replaced PET at most institutions. Optimal use of this technology requires close interaction between radiologists and nuclear medicine specialists not only in interpreting images but also in selecting image-acquisition protocols. We have demonstrated that low-dose breath-hold CT of the chest adds important diagnostic information.
Study Limitations
Insufficient follow-up data were available. Ideally, follow-up data would have provided information on the fate of the additional nodules detected on breath-hold CT. But the current study was not undertaken to determine the significance of pulmonary micronodules as detected by CT, because such studies have been done previously and have demonstrated that 18%–58% of such nodules represent metastatic disease [15–18]. The slice thickness (5 mm) chosen for low-dose breath-hold CT does not represent the optimum setting for the detection of small pulmonary nodules. However, the settings were chosen as a compromise between image resolution and radiation dose. High-resolution (1 mm) breath-hold CT might have led to the detection of additional nodules.
CONCLUSION
The current study demonstrates that maximum-inspiration breath-hold CT should be included with comprehensive whole-body PET/CT of cancer patients if no separate breath-hold chest CT is performed before PET/CT.
References
- Received for publication August 4, 2005.
- Accepted for publication October 31, 2005.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/MR Imaging in the Detection and Characterization of Pulmonary Lesions: Technical and Diagnostic Evaluation in Comparison to PET/CT
- Single 20-Second Acquisition of Deep-Inspiration Breath-Hold PET/CT: Clinical Feasibility for Lung Cancer
- 18F-FDOPA PET and PET/CT Accurately Localize Pheochromocytomas
- Deep-Inspiration Breath-Hold PET/CT of Lung Cancer: Maximum Standardized Uptake Value Analysis of 108 Patients
- Treatment Monitoring by 18F-FDG PET/CT in Patients with Sarcomas: Interobserver Variability of Quantitative Parameters in Treatment-Induced Changes in Histopathologically Responding and Nonresponding Tumors
- Dual-Modality Imaging: Combining Anatomy and Function
- Evaluation of Image Registration in PET/CT of the Liver and Recommendations for Optimized Imaging
- Deep-Inspiration Breath-Hold PET/CT of the Thorax
- Reply: Adequate Evaluation of Image Registration in Hybrid PET/CT.