


Article Figures & Data
Figures
- FIGURE 1.
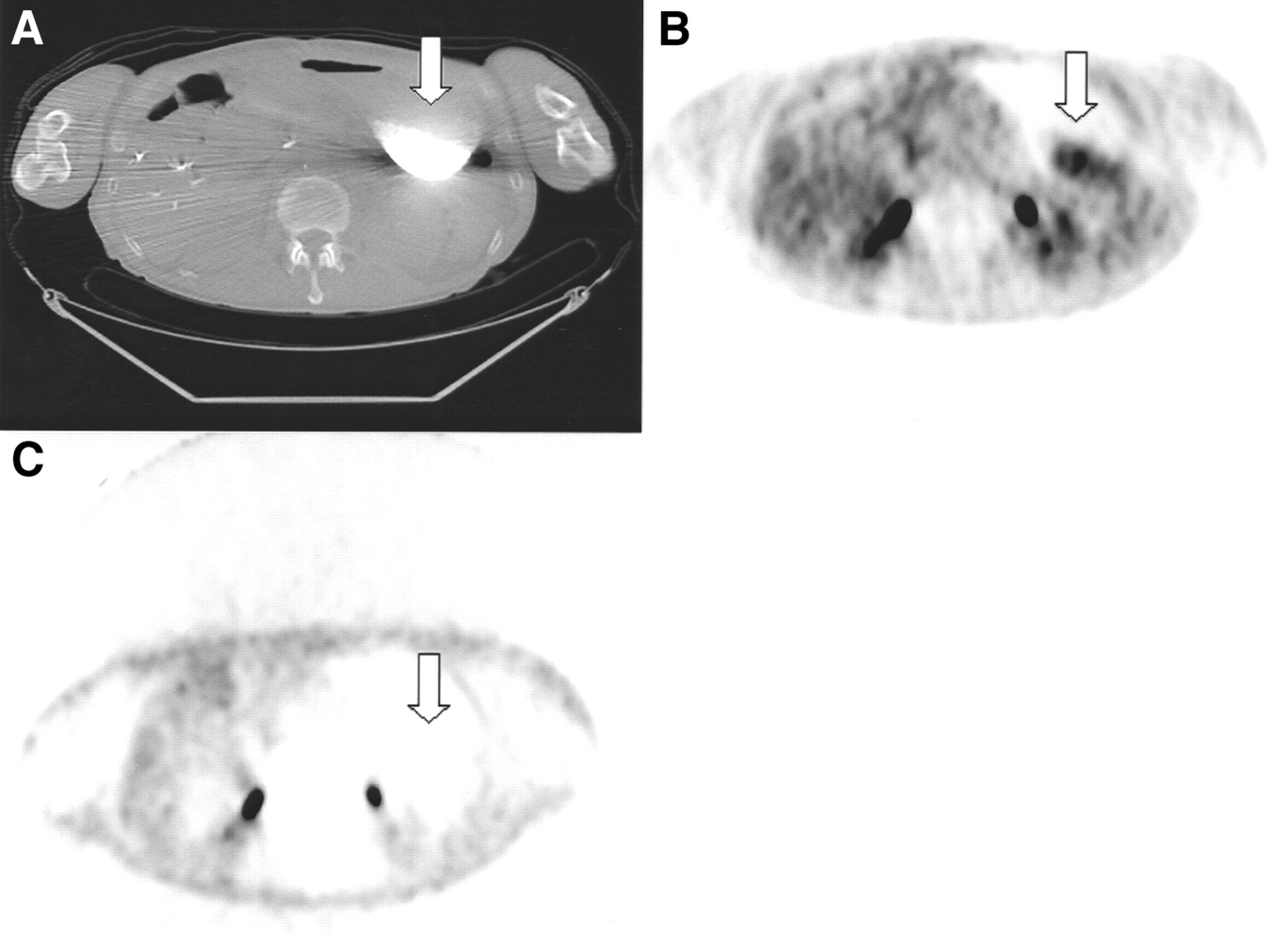
Sixty-year-old man with rising CA19-9 level and history of pancreatic cancer after therapy was evaluated by 18F-FDG PET for suspected tumor. Patient had ingested barium for upper gastrointestinal study 1 week before PET/CT study without additional contrast being administered. CT (A; arrow) showed residual, dense barium in distended stomach consistent with high-grade gastric outlet stenosis. CT attenuation-corrected PET emission images (B; arrow) showed area of increased activity in stomach corresponding to barium retention on CT (max CT Hounsfield units = 3,071). However, no increased uptake was seen in gastric lumen in nonattenuation-corrected images (C; arrow). SUVLEAN for high-activity gastric artifact was 5.31 maximum and 3.81 mean.
- FIGURE 2.
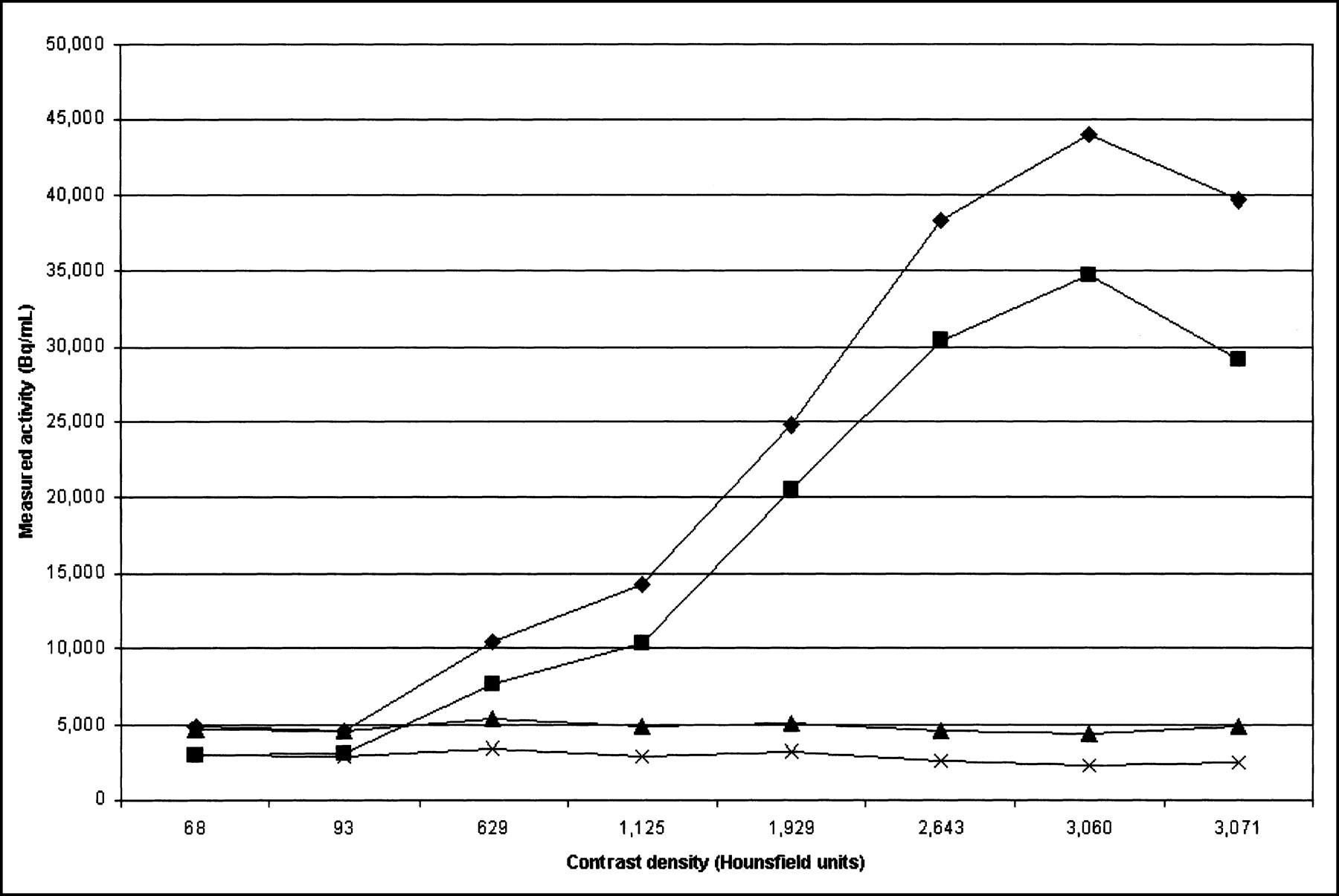
Phantom with syringes filled with variable concentrations of gastrografin, plotted as measured emission data activity (in Bq/mL) versus measured contrast density by CT (in Hounsfield units [HU]). Maximum (♦) and mean (▪) measured activity with CT attenuation correction, and maximum (▴) and mean (✖) measured activity with 68Ge attenuation correction are displayed. Drop in measured activity is observed for high-density contrast. In this region, “real density” is >3,071 HU, but the PET/CT system plateaus at this level. Thus, overcorrection in presence of high-density contrast also has plateau corresponding to 3,071 HU density. However, because of increased true attenuation as result of increasing “real” density, measured counts decrease, resulting in drop in curve.
- FIGURE 3.
Example of clinical value of oral contrast in patient with resected colorectal carcinoma evaluated with 18F-FDG PET for suspected recurrence. (A) Transverse CT image shows transverse colon with contrast (white arrow) and soft-tissue- density lesion adjacent to anterior abdominal wall (black arrow). (B) PET images with CT attenuation correction show focus of intense uptake in anterior abdomen (white arrow). (C) Fused PET/CT image shows that focus of uptake corresponds to soft-tissue mass (white arrow) and not to bowel. Diagnosis of peritoneal tumor implant was made. Patient underwent chemotherapy.


Tables
Opacification Stomach Small bowel Right colon Transverse colon Descending colon Rectosigmoid Adequate 88 90 80 64 31 13 Partial 0 0 2 2 7 9 Absent 3 1 9 25 53 69 Data are expressed as number of imaging studies in which opacification was achieved.
Parameter Stomach Small bowel Right colon Maximum 167.4 ± 8.9 156.6 ± 28 142.1 ± 46.2 (142–187) (100–209) (39–239) Mean 135.2 ± 7.7 104.1 ± 23.4 80.7 ± 34.7 (120–157) (64–148) (14–152) Results are expressed as Hounsfield units (mean ± SD). Values in parentheses are ranges. Scans from first 30 patients receiving oral contrast are included for these measurements. Maximum measured density was 239 in right colon.
Muscle SUVmax without oral contrast SUVmax with oral contrast 2-tailed P test Right mylohyoid 3.89 3.55 0.52 Left mylohyoid 3.5 3.59 0.85 Right cricoarytenoid 2.36 3.63 *0.03 Left cricoarytenoid 2.04 3.12 0.07 Interarytenoid 2.32 3.17 *0.05 Right strap muscle 1.38 1.75 0.1 Left strap muscle 1.21 1.63 *0.01 ↵* P < 0.05.
Two groups of patients were compared; the first 20 patients having received oral contrast and the last 20 patients imaged before oral contrast was introduced into routine clinical practice, excluding 2 patients with head and neck cancer, 1 with thyroid cancer, and 3 with previous neck irradiation.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Best Practices for 18F-Fluciclovine PET/CT Imaging of Recurrent Prostate Cancer: A Guide for Technologists
- Utility of positron emission tomography/CT in the evaluation of small bowel pathology
- Standards for PET Image Acquisition and Quantitative Data Analysis
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Diagnosis and Differentiation of Bronchioloalveolar Carcinoma from Adenocarcinoma with Bronchioloalveolar Components with Metabolic and Anatomic Characteristics Using PET/CT
- Dual-Modality Imaging: Combining Anatomy and Function
- Effective Methods to Correct Contrast Agent-Induced Errors in PET Quantification in Cardiac PET/CT
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Procedure Guideline for SPECT/CT Imaging 1.0
- Procedure Guideline for Tumor Imaging with 18F-FDG PET/CT 1.0
- PET/CT Imaging Artifacts
- Concurrent PET/CT with an Integrated Imaging System: Intersociety Dialogue from the Joint Working Group of the American College of Radiology, the Society of Nuclear Medicine, and the Society of Computed Body Tomography and Magnetic Resonance
- Do Implanted Pacemaker Leads and ICD Leads Cause Metal-Related Artifact in Cardiac PET/CT?
- An Analysis of the 18F-FDG Uptake Pattern in the Stomach
- Accuracy of Whole-Body Dual-Modality Fluorine-18-2-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography and Computed Tomography (FDG-PET/CT) for Tumor Staging in Solid Tumors: Comparison With CT and PET
- Why Nearly All PET of Abdominal and Pelvic Cancers Will Be Performed as PET/CT
- To Enhance or Not to Enhance? 18F-FDG and CT Contrast Agents in Dual-Modality 18F-FDG PET/CT
- Correction for Oral Contrast Artifacts in CT Attenuation-Corrected PET Images Obtained by Combined PET/CT
- PET/CT in Colorectal Cancer