


Abstract
This study evaluated lesion mislocalization between PET and CT on PET/CT studies when CT instead of germanium is used for attenuation correction (AC). Methods: PET/CT scans were obtained for 300 clinical patients. Both CT and germanium scans were used to correct PET emission data. Cases were noted of suspected inaccurate localization of lesions on any of the 5 sets of images (PET using germanium AC [GeAC] fused and not fused with CT, PET using CT AC fused and not fused with CT, and PET with no AC [NAC]). Independent CT or MRI was used to determine true lesion locations. Results: Six of 300 patients (2%) had lesion mislocalization when CT was used for AC or fusion. True liver dome lesions were mislocalized to the right lung base on PET/CT, likely because of a respiratory motion difference between PET and CT. No mislocalization was present on NAC PET or non-CT-fused GeAC PET images. Conclusion: Serious lesion mislocalization on PET/CT studies may occur, albeit very infrequently, when CT is used for either AC or fusion.
Unique information on the metabolic and functional status of cancer lesions is provided by 18F-FDG PET, thus complementing morphologic imaging modalities. However, the lack of anatomic landmarks and limited spatial resolution of PET can make precise localization challenging, thus limiting optimal evaluation of some cancer patients.
Fusion of form and function can address these issues, has been performed on the brain using image-fusion software, and can be useful in other parts of the body (1). A similar but possibly more robust approach to image fusion is the use of combined PET/CT systems that acquire anatomic and functional information in the same examination (2). Furthermore, CT data are being used instead of 68Ge for PET attenuation correction (AC). CT acquisition time (<1 min) is shorter than 68Ge transmission acquisition time (18–30 min), thus improving patient comfort and scanner throughput (3). However, artifacts from using CT-corrected instead of germanium-corrected emission PET images are not yet well characterized. The purpose of this study was to evaluate the frequency and pattern of serious lesion mislocalization with PET/CT.
MATERIALS AND METHODS
Patient Population
Datasets were retrospectively examined for 300 sequential clinical patients who underwent PET/CT scans for known or suspected cancer.
Patient Preparation
After the patients had fasted for 4 h, 555 MBq of 18F-FDG were injected intravenously, and a 60-min uptake phase in a quiet room followed. The patients were allowed to breathe normally during image acquisitions and were not given specific breathing instructions.
PET/CT Scanning
18F-FDG PET was performed using a Discovery LS PET/CT system (General Electric Medical Systems, Waukesha, WI). CT was performed using a multidetector helical CT scanner. Acquisitions occurred at 5–7 bed positions and had the following parameters: 140 kV, 80 mA, 0.8 s per CT rotation, a pitch of 6, a table speed of 22.5 mm/s, coverage of 722.5–1,011.5 mm, and an acquisition time of 31.9–37 s. CT was performed before the emission acquisition. CT data were resized from a 512 × 512 matrix to a 128 × 128 matrix to match the PET data so that the images could be fused and CT transmission maps generated. No contrast material was given to the patients.
PET emission data were also acquired at 5–7 bed positions, typically from the base of the skull to the mid thigh (coverage of 722.5–1,011.5 mm, identical to the CT protocol). Melanoma patients had 2 acquisitions of emission data: one from the vertex of the head to the mid thigh, another from the mid thigh to the toes. Emission data were acquired for 5 min at each bed position (35 scanning planes, 14.6-cm longitudinal field of view, 1-slice overlap).
Image Reconstruction, Analysis, and Review
Images were reconstructed with an 8-mm gaussian filter using a 128 × 128 matrix. PET images were reconstructed using CT for AC (CTAC) with the ordered-subset expectation maximization iterative reconstruction algorithm (2 iterations, 28 subsets). Emission data were also reconstructed with germanium AC (GeAC) (data from a 3-min transmission). Both CT and germanium transmission scans were acquired and used to correct PET emission datasets. Cases of suspected mislocalization of lesions (i.e., when PET/CT fused images showed the lesion in a different organ or tissue from that shown on CT or MR images) on any of the 5 sets of PET images (PET using GeAC fused and not fused with CT, PET using CTAC fused and not fused with CT, and PET with no AC [NAC]) were noted as part of clinical image interpretation. Independent anatomic imaging modalities (CT or MRI) were used to determine the true location of lesions.
RESULTS
In our study, using CT for AC or for fusion did not cause visible lesion mislocalization in the vast majority of cases. However, 6 of 300 patients clearly had inaccurate localization of lesions when CT was used for AC or for fusion. Characteristics of cancer patients with mislocalized lesions are presented in Table 1.
Characteristics of Cancer Patients with Mislocalized Lesions
Although not systematically evaluated in this study, PET/CT fusion has improved our accuracy in localizing lesions for which exact localization would otherwise have been difficult (4).
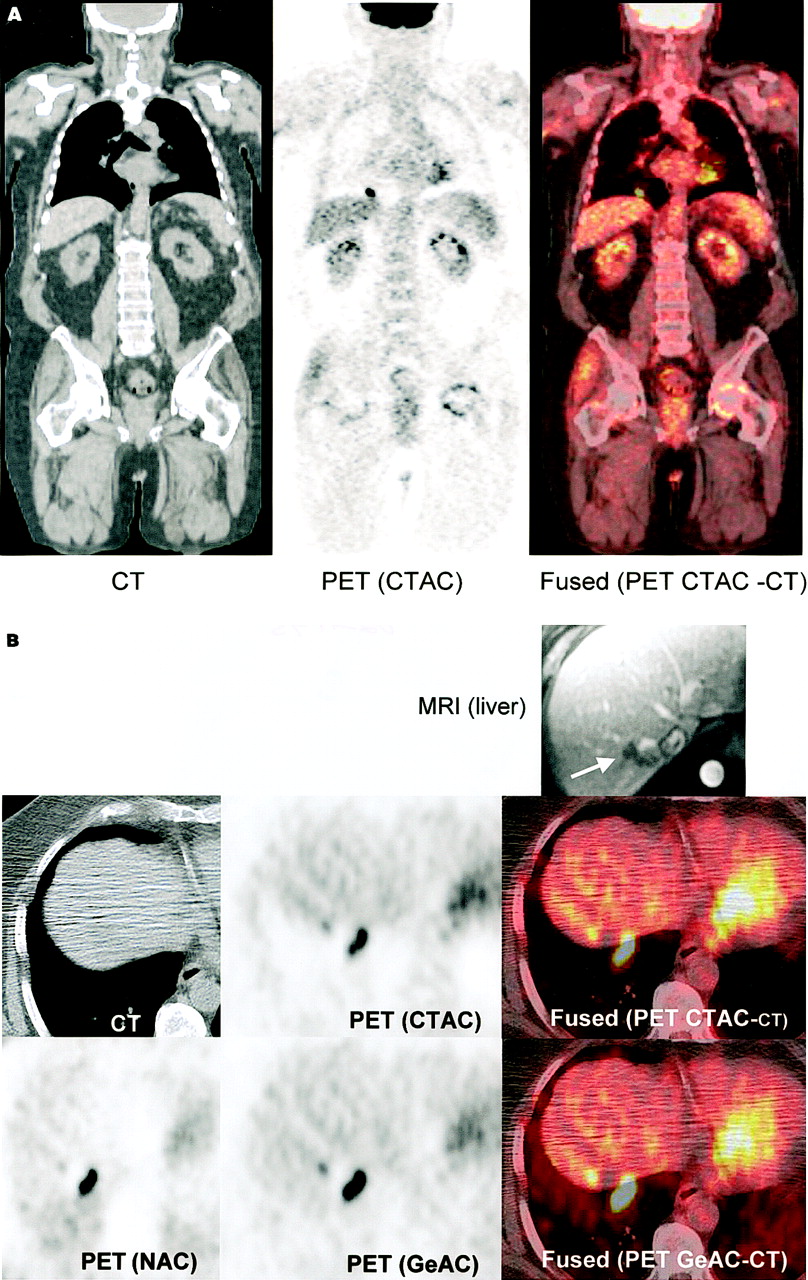
Figure 1 shows images of a 39-y-old woman with breast cancer, CT-proven liver metastases, and no lung lesion. Lesions are fused to the lung on PET/CT images (CTAC and GeAC PET images fused with CT) but are correctly localized in the liver on NAC and nonfused GeAC images. Figure 2 is an additional example of true, MRI-proven liver lesions mislocalized to the right lung base.
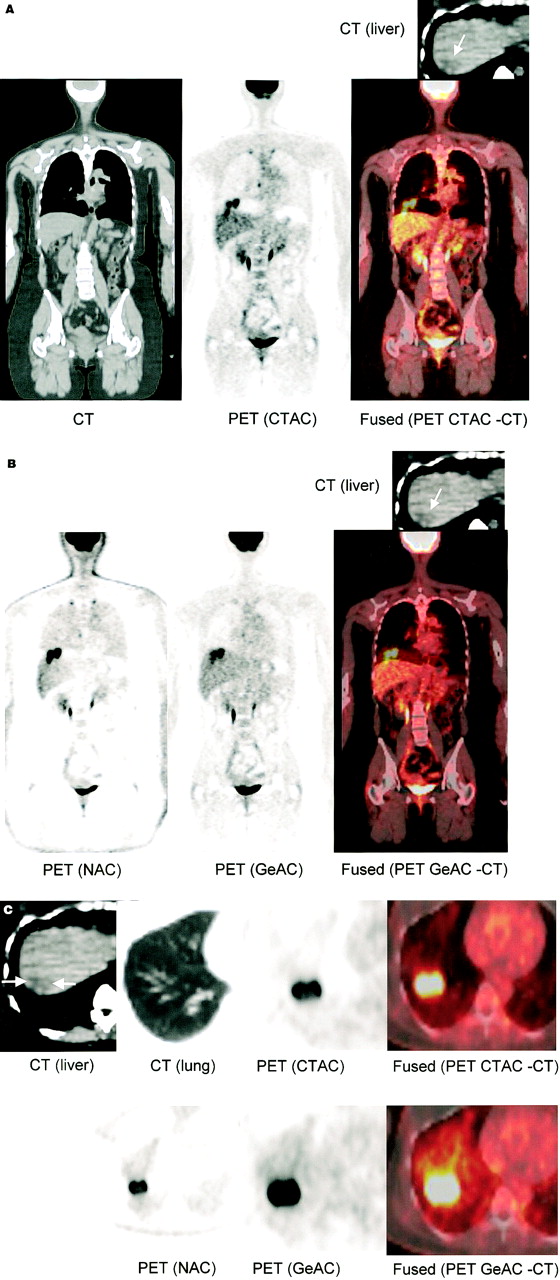
Coronal (A and B) and transaxial (C) CT images of 39-y-old woman with breast cancer and CT-proven liver metastases (arrows) but no lung lesion. Lesions are mislocalized to right lung base on fused PET/CT (using either GeAC or CTAC) but are in liver dome on NAC and nonfused GeAC images. Fused (PET CTAC-CT) = PET CTAC fused with CT; fused (PET GeAC-CT) = PET GeAC fused with CT.
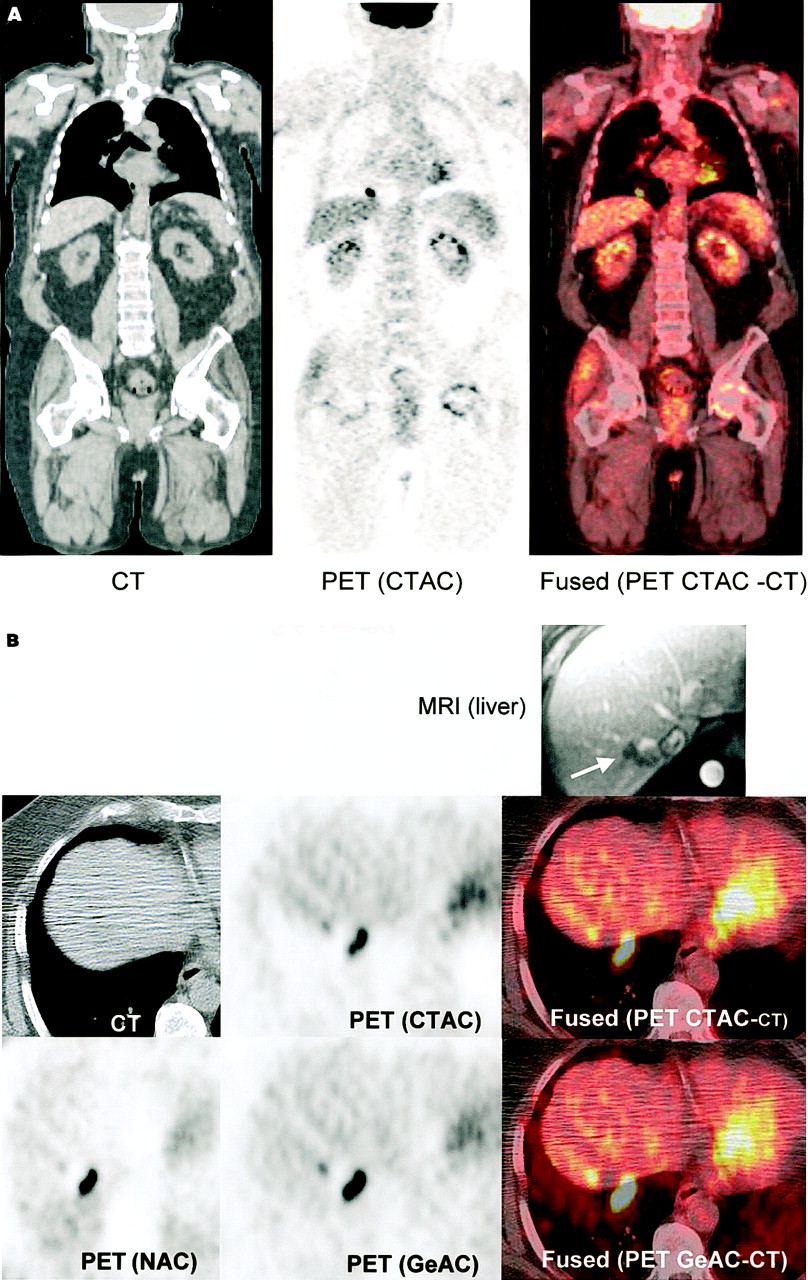
Coronal (A) and transaxial (B) PET/CT fusion images of 70-y-old man with colon cancer and MRI-proven liver metastases (arrow) but no lung lesions. Lesion is seen in right lung base, but no lung lesion is seen on CT; on both NAC and GeAC images without CT fusion, lesion was correctly localized to liver. Fused (PET CTAC-CT) = PET CTAC fused with CT; fused (PET GeAC-CT) = PET GeAC fused with CT.
DISCUSSION
Accurate image fusion potentially improves diagnostic accuracy (5). PET/CT transforms image fusion from a primarily research tool to everyday clinical practice. However, potential artifacts from using CT-corrected instead of 68Ge-corrected emission PET images and from fusing PET images to CT images have not been fully characterized. Examples of sources of coregistration errors in PET/CT systems include physiologic motion, such as breathing and cardiac motion, and nonphysiologic patient movement between the PET and CT studies. Problems from respiratory motion could be expected if differences in respiratory status exist between the 2 methods of AC. The potential exists for misalignment of PET and CT images acquired under different breathing conditions. PET scans require several minutes per field of view and the final image is an average of many breathing cycles, in contrast to the much shorter CT image acquisitions. Linear and transverse patient motion is avoidable, but respiratory motion probably is not, unless respiratory gating of PET is used.
In our study, curvilinear cold artifacts paralleling the dome of the diaphragm at the lung bases were frequently noted on PET/CT image acquisitions obtained at free tidal breathing. The degree of this artifact varied but was mild in most patients. This cold artifact was not present in GeAC images. This artifact was likely due to an inaccurate correction for photon attenuation at the lung base because of inconsistencies in the liver-lung interface between PET and CT acquisitions. Such inaccuracies could potentially lead to inaccurate quantitation of 18F-FDG uptake in this area. Furthermore, the inevitable difference in respiratory cycles between PET and CT images may potentially result in mislocalization if lesions are close to either side of the diaphragm.
Serious mislocalization from using CTAC instead of GeAC and from using CT for fusion has not previously been reported. In our study, PET images were corrected with both CT and germanium, thereby giving us a unique opportunity to study frequency and patterns of such possible mislocalization. Both CT and PET images were acquired during free tidal breathing. Clinically apparent mislocalizations were noted in 6 patients in whom true right liver dome lesions were mislocalized to the right lung base on PET/CT, likely because of respiratory motion. In those cases, mislocalization was not present on the GeAC PET images (Figs. 1 and 2) but was present when CT was used for AC or for fusion. When present, the degree of mislocalization was worst in the CT-fused CTAC PET images. Thus, respiratory motion causing PET and CT to image different configurations of the body was likely responsible for the artifacts. Such artifacts were not present in the NAC or the nonfused GeAC PET images. We believe that the overall frequency of lesion mislocalization does not warrant the use of special breathing protocols; however, respiratory gating may help in minimizing respiratory motion artifacts in PET/CT (6).
CONCLUSION
Serious lesion mislocalization in PET/CT may occur when CT is used for either AC or fusion. Respiratory motion can result in infrequent (2% in this study) but potentially serious lesion localization errors. PET/CT findings should be correlated with NAC images, GeAC images, or recent anatomic studies, particularly when lesions are at the lung bases or dome of the liver, to ensure proper lesion localization.
Footnotes
Received May 15, 2002; revision accepted Oct. 4, 2002.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, 601 N. Caroline St., Room 3223A, Baltimore, MD 21287-0817.
E-mail: rwahl{at}jhmi.edu
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improved Alignment of PET and CT Images in Whole-Body PET/CT in Cases of Respiratory Motion During CT
- Respiratory Motion Compensation for PET/CT with Motion Information Derived from Matched Attenuation-Corrected Gated PET Data
- Detection of Lung Cancer by FDG-PET Cancer Screening Program: A Nationwide Japanese Survey
- Generation of 4-Dimensional CT Images Based on 4-Dimensional PET-Derived Motion Fields
- Respiratory Motion Correction in Oncologic PET Using T1-Weighted MR Imaging on a Simultaneous Whole-Body PET/MR System
- Characterization of a Perirectal Artifact in 18F-FDG PET/CT
- 18F-FDG PET/CT for Image-Guided and Intensity-Modulated Radiotherapy
- Single 20-Second Acquisition of Deep-Inspiration Breath-Hold PET/CT: Clinical Feasibility for Lung Cancer
- Dual-Modality Imaging: Combining Anatomy and Function
- Latest Advances in Molecular Imaging Instrumentation
- Evaluation of Image Registration in PET/CT of the Liver and Recommendations for Optimized Imaging
- Deep-Inspiration Breath-Hold PET/CT: Clinical Findings with a New Technique for Detection and Characterization of Thoracic Lesions
- Artifacts from Misaligned CT in Cardiac Perfusion PET/CT Studies: Frequency, Effects, and Potential Solutions
- Reply: Adequate Evaluation of Image Registration in Hybrid PET/CT.
- Procedure Guideline for SPECT/CT Imaging 1.0
- Procedure Guideline for Tumor Imaging with 18F-FDG PET/CT 1.0
- Attenuation Correction of PET Images with Respiration-Averaged CT Images in PET/CT
- Concurrent PET/CT with an Integrated Imaging System: Intersociety Dialogue from the Joint Working Group of the American College of Radiology, the Society of Nuclear Medicine, and the Society of Computed Body Tomography and Magnetic Resonance
- Respiratory Gating for 3-Dimensional PET of the Thorax: Feasibility and Initial Results
- In Reply:
- PET/CT Today and Tomorrow
- Why Nearly All PET of Abdominal and Pelvic Cancers Will Be Performed as PET/CT
- Ahem, Blame the Daughter!
- PET/CT: Panacea, Redundancy, or Something in Between?