


Abstract
Molecular imaging with 18F-FDG PET has been proven useful in the management of colorectal cancer. 18F-FDG PET plays a pivotal role in staging before surgical resection of recurrent colorectal cancer and metastases, in the localization of recurrence in patients with an unexplained rise in serum carcinoembryonic antigen levels, and in the assessment of residual masses after treatment. Currently, there is increasing interest in the role of 18F-FDG PET beyond staging. The technique appears to have significant potential for the characterization of tumors and for the prediction of prognosis in the context of treatment stratification and early assessment of tumor response to therapy. This systematic review provides an overview of the literature on the value of 18F-FDG PET for monitoring and predicting the response to therapy in colorectal cancer. The review covers chemotherapy response monitoring in advanced colorectal cancer, monitoring of the effects of local ablative therapies, and preoperative radiotherapy and multimodality treatment response evaluation in primary rectal cancer. Given the added value of 18F-FDG PET for these indications, implementation in clinical practice and systematic inclusion in therapeutic trials to exploit the potential of 18F-FDG PET are warranted.
Colorectal cancer was the third most common cancer in men and women in 2008 and is the third leading cause of cancer-related deaths in the United States. Although colorectal cancer incidence rates decreased from 1998 through 2004, this cancer continues to be a major health problem worldwide. About 148,800 cases of colorectal cancer are expected to be newly diagnosed in the United States in 2008, the cumulative lifetime risk is approximately 5%, and the current 5-y survival rate approaches 66% (1). The prognosis for patients with this disease has improved substantially, mainly because of earlier detection and the introduction of effective systemic (chemo)therapeutic agents (2–4).
Molecular imaging with 18F-FDG PET has been shown to be useful in the management of colorectal cancer. 18F-FDG PET already plays a pivotal role in staging before surgical resection of locally recurrent cancer and metastases, in the localization of recurrence in patients with an unexplained rise in serum carcinoembryonic antigen levels, and in the assessment of residual masses after treatment. This diagnostic tool seems to be very promising for therapy stratification as well (5,6).
Currently, there is growing interest in the role of 18F-FDG PET beyond staging, in particular, for the prediction of tumor response to therapy. Hence, the number of clinical applications for 18F-FDG PET in colorectal cancer continues to increase. This systematic review discusses the emerging role of 18F-FDG PET in the prediction and evaluation of responses to treatment, such as monitoring chemotherapy responses in advanced colorectal cancer, monitoring responses after local ablative therapy of liver metastases, and monitoring radiotherapy and multimodality treatment responses in primary rectal cancer.
SEARCH STRATEGY AND LITERATURE SELECTION CRITERIA
Data for this review were identified by searches of PubMed, MEDLINE (OvidSP), EMBASE (OvidSP), and the Cochrane Library up to December 2008 with the search terms reported by Mijnhout et al. (7) for identifying clinical 18F-FDG PET studies and the following 2 groups of search terms: “colorectal carcinoma” or “colorectal cancer” or “colon cancer” or “rectal cancer” or “rectal carcinoma” and “prediction” or “therapy monitoring” or “response monitoring” or “response.” Search results were evaluated for adequacy. Only articles in English were included. We omitted articles that merely dealt with staging before surgical resection of recurrent cancer and metastases, localization of recurrence in patients with an unexplained rise in serum carcinoembryonic antigen levels, and residual masses after treatment; with malignancies other than colorectal carcinoma or liver metastases of mixed primary origin; and with radiopharmaceuticals other than 18F-FDG. Descriptions of treatment responses without fixed outcome parameters (e.g., histologic or morphologic response, overall survival, or progression-free survival) were also omitted. References from included articles were checked for studies not retrieved by the search strategy. Abstracts, reports from meetings, editorial comments, and letters to the editor were excluded.
CHEMOTHERAPY RESPONSE MONITORING IN ADVANCED COLORECTAL CANCER
Tumor response to therapy is traditionally assessed by comparison of tumor sizes determined by morphologic imaging methods (CT) before and after treatment. According to the response evaluation criteria in solid tumors (RECIST), the current definition of tumor response is a decrease in the sum of the largest diameters of tumor lesions of at least 30% (8). The RECIST are widely accepted, but the correlation between morphologic tumor response and patient outcome is rather weak (9). Moreover, residual benign masses may persist, despite the fact that disease activity may have completely resolved after successful therapy.
18F-FDG PET yields data independent of associated structural characteristics and therefore allows the detection or monitoring of specific metabolic changes that are not associated with or that precede therapy-induced anatomic changes. The strength of 18F-FDG PET is that it permits whole-body imaging in a noninvasive way. In contrast to histopathologic analysis of biopsy material, 18F-FDG PET is not limited to the characterization of one or a few (sometimes very heterogeneous) target lesions; it can evaluate multiple tumor sites at the same time. Furthermore, serial scanning can be performed, allowing the measurement of functional changes over time during therapeutic interventions. PET not only can visualize (Fig. 1) but also can quantify 18F-FDG uptake and is able to provide several highly reproducible quantitative parameters of tumor glucose metabolism. However, the disadvantages of molecular imaging techniques (limited resolution and radiation burden) relative to techniques such as MRI should not be ignored. Therefore, these techniques should not be considered competitive but rather should be considered complementary because they aim to visualize and measure different processes in the human body.
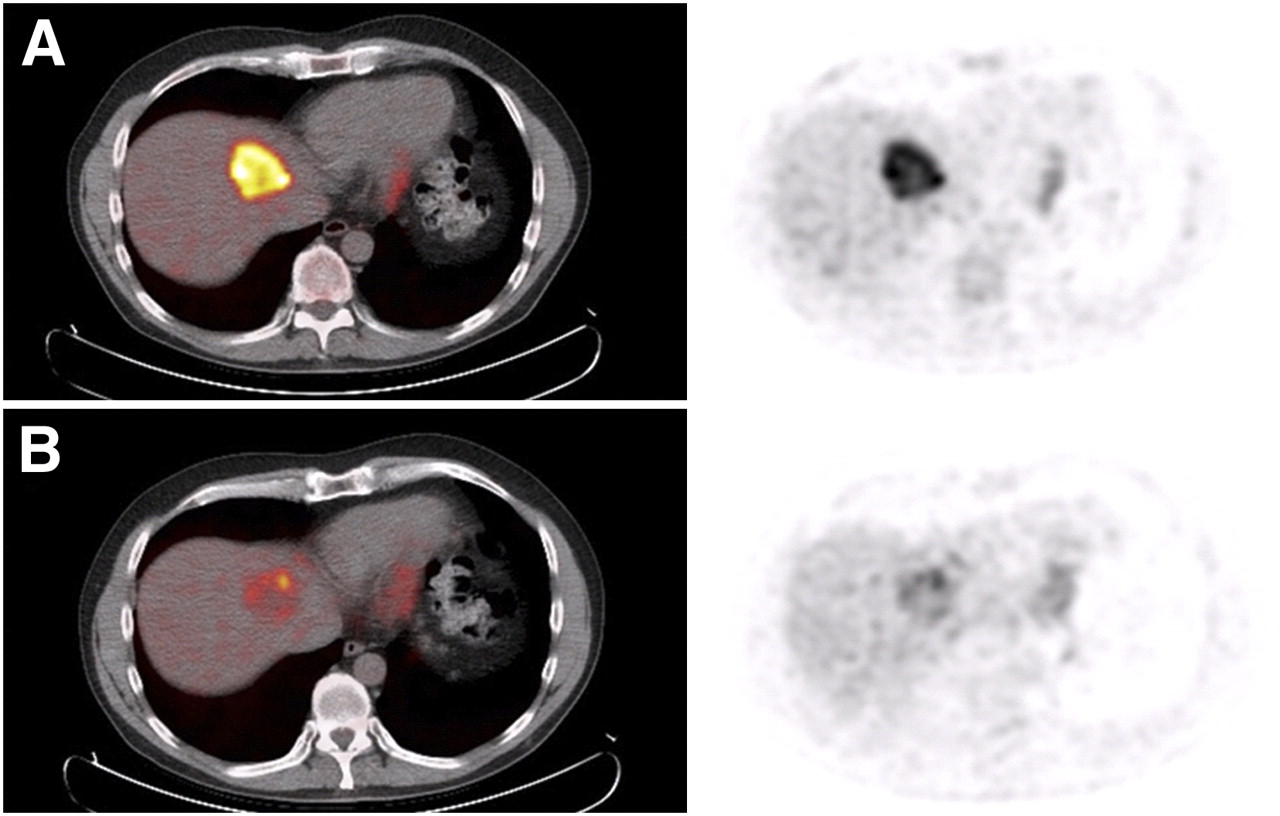
Typical example of colorectal cancer patient with nonresectable liver metastases that responded to chemotherapy. Relative to baseline (A), 85% decrease in MRglu was seen on 18F-FDG PET after 2 mo of chemotherapy (B). Transversal fused PET/CT scans are shown on left; transversal PET scans are shown on right. (Courtesy of Dr. W.V. Vogel.)
However, it is obvious that the introduction of targeted therapies, such as the angiogenesis inhibitor bevacizumab, requires new tools for monitoring therapeutic effects, because these agents exhibit a cytostatic effect rather than the cytoreductive effect of classic chemotherapy. These new agents inhibit the growth of new blood vessels in cancer tissue; this effect does not immediately lead to a decrease in tumor size and thus places new demands on imaging modalities. When anticancer treatment becomes more individualized, it is increasingly important to identify a response at earlier time points. Early identification of the lack of a response would prevent side effects, reduce the costs of futile treatment, and prevent delays in instituting a second-line, potentially effective, therapy.
Five studies (Table 1) reported the predictive value of 18F-FDG PET in patients treated with chemotherapy for nonresectable colorectal cancer liver metastases (10–14). As early as 1996, Findlay et al. (10) studied 18 patients before, at 1–2 wk after, and at 4–5 wk after 5-fluorouracil (5-FU) chemotherapy with or without interferon-α by using a nondedicated PET system with a limited resolution. Responding lesions showed a significantly greater reduction in 18F-FDG uptake, compared with the baseline value, than nonresponding lesions (−33% vs. −1%; P < 0.001). The 4- to 5-wk tumor-to-liver ratio was able to discriminate responders from nonresponders in both a lesion-by-lesion assessment and an overall patient response assessment with a sensitivity of 100% and specificities of 90% and 75%, respectively. A clear correlation was observed between the reduction in tumor glucose metabolism at 5 wk after the start of chemotherapy and treatment outcome; such a correlation was not observed at 1–2 wk after the start of treatment. These results showed the importance of the correct timing of 18F-FDG PET after the beginning of chemotherapy. The authors mentioned the so-called flare phenomenon that occurs at 1–2 wk after the initiation of chemotherapy and that can be observed as a marked increase in 18F-FDG metabolism in lesions that show a response later on.
Chemotherapy Response Monitoring in Advanced Colorectal Cancer
Bender et al. (11) showed that the flare phenomenon probably does not play a role as early as 72 h after the initiation of chemotherapy. Their preliminary results demonstrated that therapy-sensitive metastases show a reduction in 18F-FDG uptake after a single application of chemotherapy and that this effect can be quantified by PET and seems to be indicative of the final therapy outcome after the completion of an anticipated therapy cycle.
Dimitrakopoulou-Strauss et al. (12) studied 28 patients who were treated with second-line 5-FU–folinic acid–oxaliplatin (FOLFOX) therapy. Reference standards for the serial 18F-FDG PET studies were the clinical response data, according to the World Health Organization (WHO) classification. In contrast to the studies of Findlay et al. (10) and Bender et al. (11), that study investigated absolute standardized uptake values (SUVs) and kinetic parameters and not fractional changes between baseline and follow-up scans. Even the quantitative values from the first PET study (at baseline) were predictive with respect to therapy outcome. The so-called fractal dimension, a kinetic parameter that describes the heterogeneity of tissue time–activity data in tumors, produced the best results and correctly classified progressive disease and stable disease in 90% and 75% of cases at baseline, respectively.
In a similar study, Dimitrakopoulou-Strauss et al. (13) examined the potential of serial 18F-FDG PET to predict the response to chemotherapy as reflected by individual survival times. It was shown that a combination of kinetic parameters from the first scan (at baseline) and the third scan (at 8 wk) provided the best results for classification into short- and long-term survival classes (defined as survival of <1 y and >1 y, respectively). The authors suggested that quantitative dynamic 18F-FDG PET should be used preferentially for chemotherapy response monitoring
A recent study (14) showed that 18F-FDG PET could be readily implemented without the need for complex dynamic imaging protocols. It was demonstrated that simplified measures (e.g., SUVs) can replace more complex quantitative measures (e.g., rate of metabolism of glucose [MRglu]). Dynamic 18F-FDG PET was performed before and at 2 mo (n = 50) and 6 mo (n = 19) after the start of treatment. There were increases in the rates of progression and death associated with the worst response as assessed by PET, as determined by Cox proportional regression analysis. The overall and progression-free survival data yielded significant predictive values at broad cutoff levels for changes in MRglu and SUV. It was concluded that the degree of chemotherapy-induced changes in tumor glucose metabolism in advanced colorectal cancer is highly predictive of patient outcome.
A noncomplex approach is advantageous over a full kinetic analysis approach because it will facilitate broad introduction into clinical practice and will improve patient compliance, which is an important feature of successful clinical trials. Another advantage of SUVs is that they can be calculated from static whole-body 18F-FDG PET studies, which depict all metastases. In dynamic scans, only one axial field of view, typically 15–20 cm, can be studied during dynamic data acquisition. Because metastatic lesions in different parts of the body may respond differently to chemotherapy, this features represents a principal advantage of SUV analysis over kinetic analysis.
An important observation is that chemotherapy-induced normalization of 18F-FDG uptake in liver metastases of colorectal cancer does not indicate a complete pathologic response (15–17). Tan et al. (16) found that, despite the absence of detectable metabolic activity above the background, viable tumor cells could still be found in 85% of lesions. In a subgroup of 7 lesions in which neoadjuvant chemotherapy resulted in both a complete metabolic response and a complete CT response (RECIST), histologic analysis revealed viable tumor cells in 6 lesions. A reduction in the number of viable tumor cells below the limit of detection may be an important reason why lesions are not seen by 18F-FDG PET after treatment. In addition, the relatively high level of 18F-FDG uptake in normal hepatic parenchyma makes it more difficult to detect lesions with a partial metabolic response resulting in uptake only slightly greater than that of the liver. Another factor may be the effect of chemotherapy on tumor cell 18F-FDG uptake. Chemotherapeutic agents may reduce 18F-FDG uptake by altering the glucose metabolism of tumor cells. Akhurst et al. (18) postulated that this change in 18F-FDG uptake after cytotoxic therapy is induced by a decrease in the activity of the key glycolytic enzyme hexokinase. Therefore, curative resection of liver metastases that demonstrate a complete metabolic response on 18F-FDG PET should not be omitted.
MONITORING RESPONSES AFTER LOCAL ABLATIVE THERAPY OF LIVER METASTASES
Complete surgical resection offers the best chance for cure in patients with colorectal liver metastases. However, because of the number or localization of liver metastases, complete resection with adequate tumor-free margins and adequate liver function reserve cannot be achieved in all patients. Local ablative techniques that result in intrahepatic tumor destruction have emerged as alternative treatment options, although positive effects on patients' survival remain to be established. These techniques include microwave tumor coagulation (19), laser-induced thermotherapy (20), injection of ethyl alcohol (21), cryosurgical ablation or cryotherapy (CSA) (22), and radiofrequency ablation (RFA) (23).
Different morphologic imaging techniques have been used to facilitate intraoperative localization. However, during the process of local ablation, the destruction process cannot easily be ascertained with intraoperative ultrasonography because of the hyperechogenicity that is induced within the treated area (24). Furthermore, evaluation with CT or MRI of residual tumor after the ablation procedure is hampered by a rimlike increase in contrast enhancement that occurs immediately after RFA and that resembles peripheral hyperperfusion. This area of contrast enhancement may interfere with the adequate detection of residual tumor (25). This problem can lead to either a delayed diagnosis of treatment failure or confusion between incomplete local ablative treatment and the occurrence of new metastases in regions adjacent to the treatment site.
Several studies (Table 2) have described the feasibility of 18F-FDG PET (Fig. 2) for the surveillance of patients with liver metastases (26–30). 18F-FDG PET appears to have great potential for identifying residual tumor very early after local ablative treatments. Earlier detection offers the opportunity to treat tumors again at an early stage, by either surgery or repeated local ablation in the case of an insufficient initial treatment result. A study performed at our own institute by Langenhoff et al. (26) demonstrated that 18F-FDG PET performed early after local tumor ablation provided additional information about efficacy by differentiating posttreatment changes from residual or recurrent malignant tumor. 18F-FDG PET results became negative in 51 lesions within 3 wk after local ablative therapy, meaning that 18F-FDG-accumulating liver metastases became photopenic. The 18F-FDG PET results for 5 lesions remained positive. A local recurrence was identified on CT during a mean follow-up of 16 mo for 4 of these lesions; the other lesion was found to be an abscess. Conversely, a local recurrence was not identified for lesions without 18F-FDG uptake on PET (negative predictive value, 100%). In all patients, 18F-FDG PET detected recurrence considerably earlier than CT (3.8 vs. 8.5 mo).
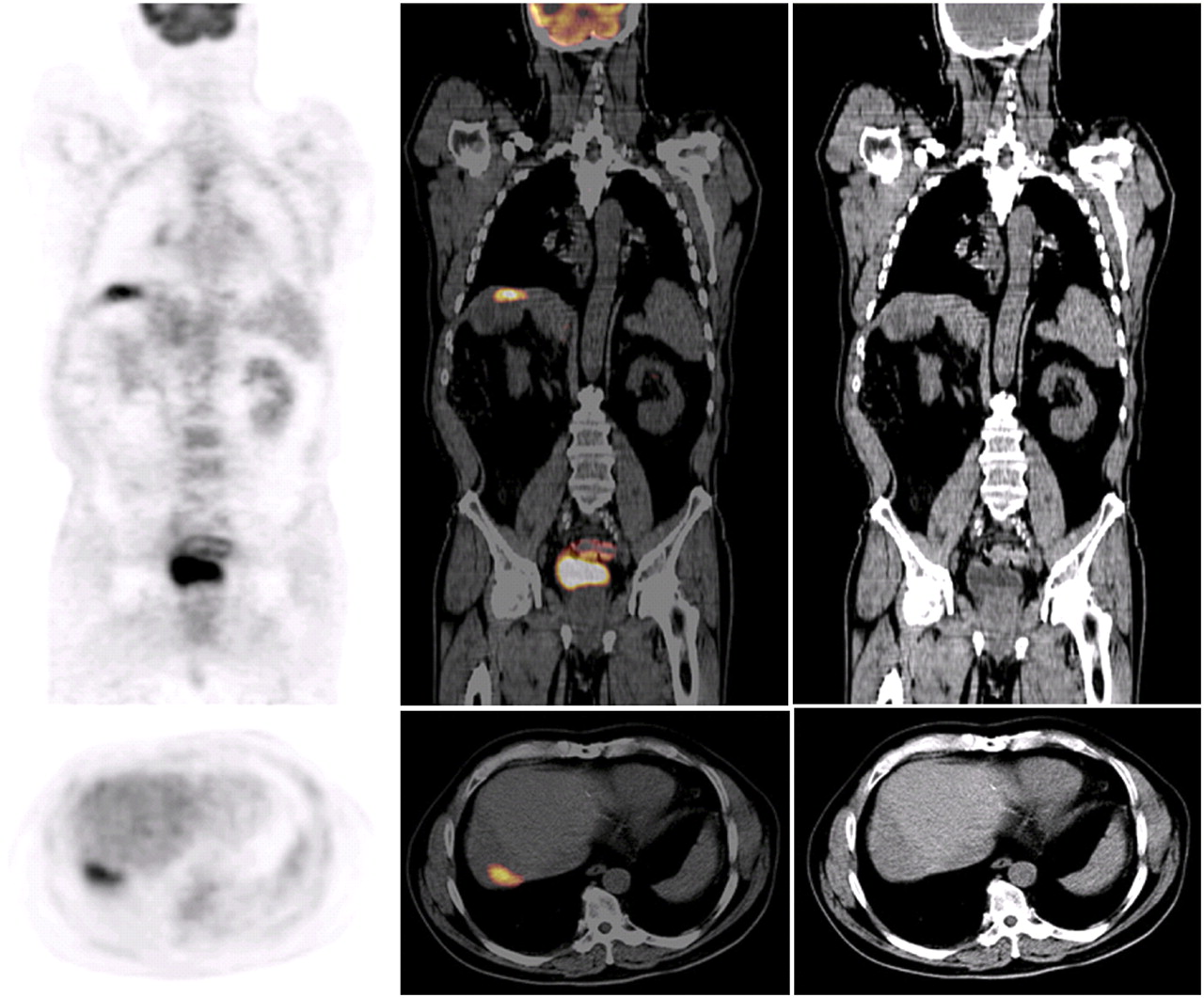
18F-FDG PET/CT 3 mo after radiofrequency ablation. Clear 18F-FDG accumulation revealed residual vital tumor tissue. Abnormalities on CT after 3 and 6 mo were interpreted as posttreatment effects, and tumor recurrence was diagnosed on CT after 9 mo. Upper row: coronal images; lower row: transversal images. From left to right: PET scans, fused PET/CT scans, and CT scans.
Response Monitoring After Local Ablative Therapy for Treatment of Colorectal Cancer Liver Metastases
Donckier et al. (28) performed 18F-FDG PET at 1 and 4 wk after local ablative treatment. They showed that 18F-FDG PET was accurate in monitoring the local effect of RFA because it recognized incomplete tumor ablation early, even when incomplete tumor ablation was not detectable by CT. After a median follow-up of 11 mo, none of 24 lesions without 18F-FDG uptake on PET after ablation showed the development of a local recurrence. In 4 patients, 18F-FDG PET at 1 wk and 1 mo revealed a peripheral hypermetabolic residue after RFA, whereas CT did not reveal residual tumor. In 3 patients, a local persistence of viable tumor cells was biopsy proven at reintervention. In the fourth patient, follow-up CT revealed the subsequent development of a local recurrence.
Joosten et al. (27) showed that CT after treatment did not predict local treatment failure, whereas 18F-FDG PET within 3 wk after local ablative treatment predicted 6 of 7 local recurrences in a study population of 43 patients with 104 ablated lesions. One local recurrence was detected on 18F-FDG PET 3 mo after treatment. The negative predictive value of 18F-FDG PET at 3 mo was 100%. Because 18F-FDG PET revealed 1 false-positive result because of focal infection, the positive predictive value was 88%. These results are in line with the findings of Denecke et al. (20). Among 54 lesions, they found 1 false-positive lesion 54 d after treatment, presumably caused by regenerative processes. One false-negative lesion among 6 examined was found within 3 d after treatment, probably because of a small volume of surviving tumor tissue.
Similar observations have been reported by Veit et al. (30). Their small study (n = 11) was the first to use integrated PET/CT. Four of 6 patients with residual tumor showed residual 18F-FDG accumulation at the ablative margin as early as 2 d after RFA. The accuracy for the detection of residual tumor directly after RFA was higher for PET/CT than for CT alone (68% vs. 47%). Although the number of patients was too small to draw definite conclusions, the authors pointed out some advantages of a short imaging interval after RFA and of the use of PET/CT for this indication over the use of PET or CT alone. They postulated that dual-modality PET/CT simplifies guidance for reinterventions and that a follow-up scan directly after RFA is ideal to shorten the time to a possible reintervention. The authors speculated that a follow-up scan should take place within 2 d after RFA, before tissue regeneration takes place (30). Tissue regeneration might cause rimlike tracer distribution at the ablative margin; in contrast, viable tumor residue results in an area of focally increased 18F-FDG uptake.
PREOPERATIVE RADIOTHERAPY AND MULTIMODALITY TREATMENT RESPONSE EVALUATION IN PRIMARY RECTAL CANCER
With the exception of very early tumors that can be managed by local excision alone, the mainstay of therapy for rectal cancer is radical surgery. Total excision of the mesorectum has emerged as the surgical technique that can substantially reduce local recurrences. However, the risk of distant and local recurrences continues to threaten patients with rectal cancer. Patients with locally advanced rectal cancer are at the highest risk of failure of local treatment. Therefore, surgery alone is often not curative, and preoperative radiotherapy is required to achieve a radical resection and improve the local control rate (31). For locally advanced rectal cancer, neoadjuvant chemoradiation has been proven successful (32,33). Tumor responses to chemoradiotherapy, however, vary considerably. Some patients experience serious side effects, and not all patients benefit equally (34). Therefore, the surgical approach largely depends on a valid assessment of the preoperative extent of the tumor, particularly for distally located tumors or tumors that have been assessed as being nonresectable during primary staging.
The current standard method for discriminating responders from nonresponders is conventional histopathologic analysis, measuring the extent of the residual tumor. This method, however, is applicable only in a postoperative setting and consequently cannot be used for the preoperative selection of individualized surgery. First, accurate restaging to assess the success of neoadjuvant chemoradiation is critical because it can guide optimization of the surgical approach, such as sphincter-saving surgery in deep-seated tumors, less aggressive resection in minimally advanced tumors, or planning of intraoperative radiation therapy. Second, the correct assessment of responses and the identification of nonresponders may have clinically relevant consequences during the course of chemoradiation. These include the potential for individualized treatment, for instance, the escalation of preoperative treatment (e.g., increasing the radiation dose, adding regional hyperthermia, or using intraoperative radiation) or the addition of chemotherapeutic regimens after tumor resection. Therefore, there is an obvious need for reliable noninvasive methods suitable for the prediction of responses, especially complete pathologic remission.
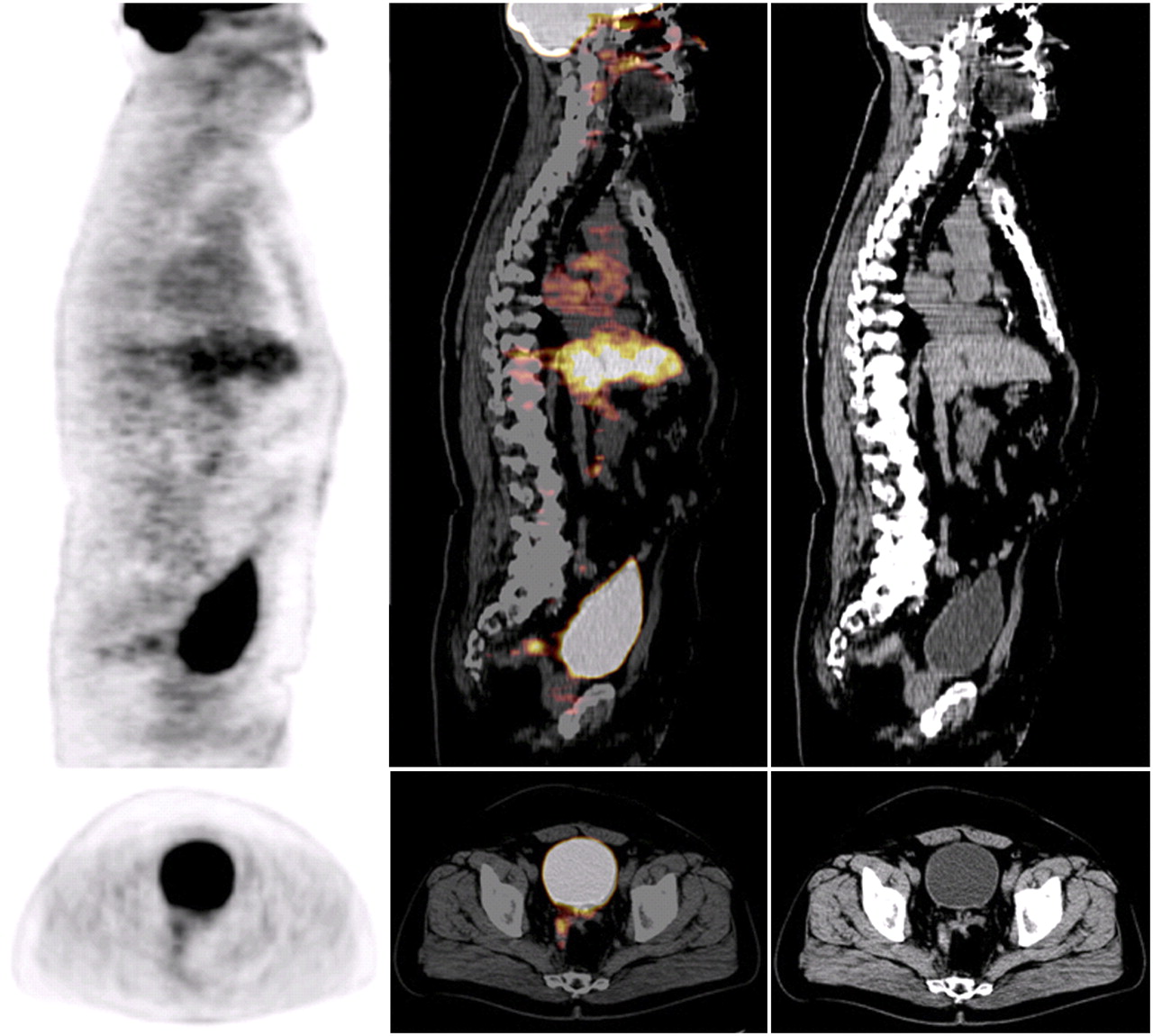
In the setting of routine clinical practice, mainly anatomically based imaging modalities, such as CT, MRI, and endorectal ultrasound, have been used. Two recent meta-analyses showed that these 3 imaging modalities are highly accurate in the staging of untreated tumors because of their ability to detect invasion in the perirectal fat or adjacent organ involvement (35,36). The situation is dramatically different when these imaging modalities are considered for the purpose of restaging after chemoradiotherapy, because their accuracies range from only 30% to 60%—accuracies that are clearly too low to support decisions regarding changes in the surgical approach (35–38). Conventional imaging modalities cannot distinguish fibrosis or scar from viable tumor cells in residual masses after chemoradiotherapy; therefore, these methods have a negligible impact on the prediction of pathologic findings (38,39). As a result, great demands are placed on imaging modalities that provide a combination of functional information (18F-FDG PET) and morphologic information (CT, MRI, and endorectal ultrasound) (Fig. 3). The introduction of integrated PET/CT scanners has shed new light on this issue.
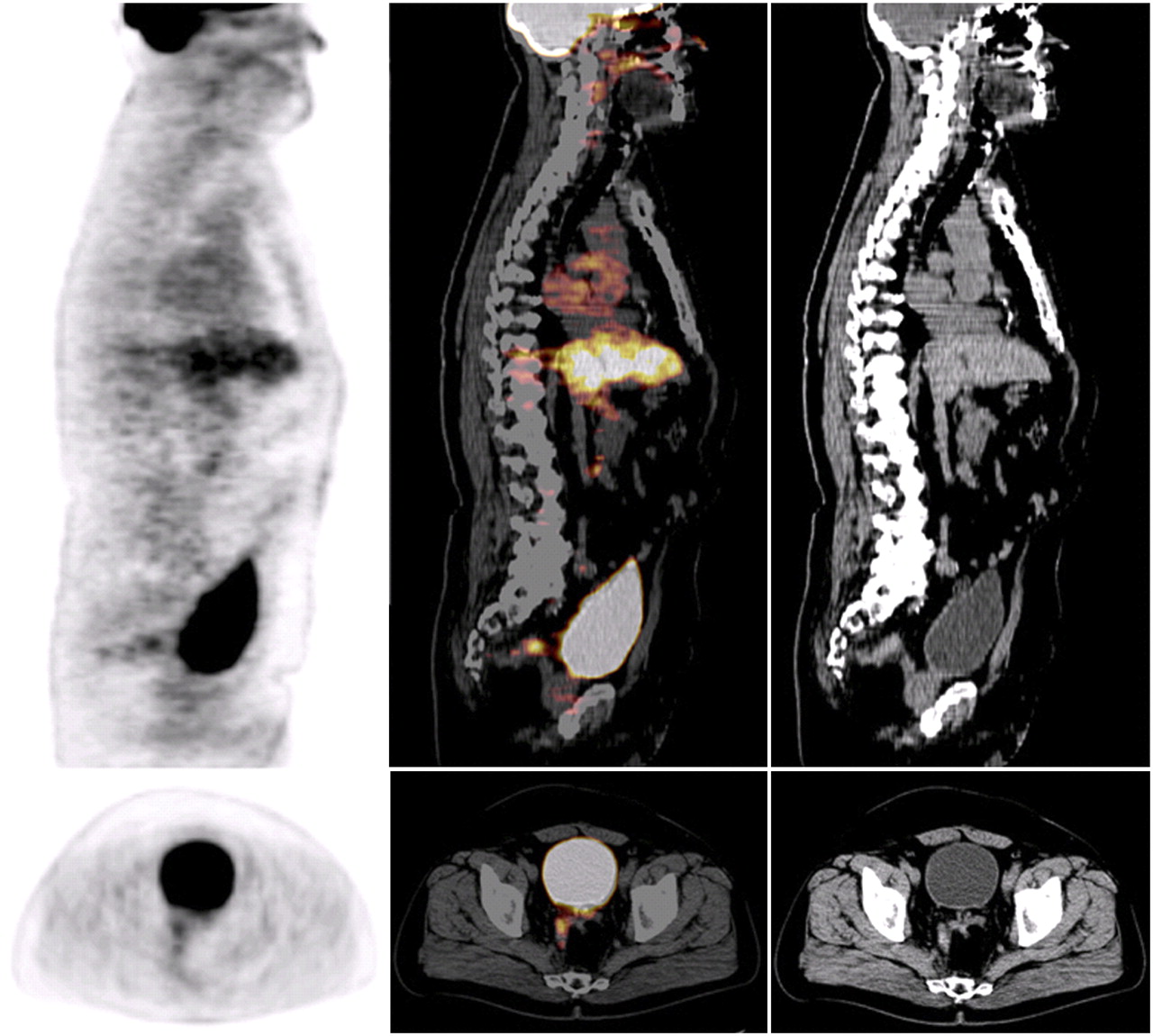
18F-FDG PET/CT of nonresponding patient with locally advanced rectal cancer that was treated with preoperative chemoradiation. In this preoperative study, tumor uptake was still present, and histopathologic analysis confirmed residual vital tumor tissue. Upper row: sagittal images; lower row: transversal images. From left to right: PET scans, fused PET/CT scans, and CT scans.
The first study (Table 3) that reported on metabolic response assessment after irradiation of nonresectable presacral recurrent rectal carcinomas was published in 1992 by Engenhart et al. (40) They noted a small but significant (P = 0.002) decrease in 18F-FDG uptake during treatment but concluded that it was still too early to use 18F-FDG PET for radiotherapy treatment monitoring because the effects of proliferation, repair, inflammation, and residual viable tumor cells on glycolytic activity had to be determined first. Several years later, Schiepers et al. (41) investigated the influence of induction radiotherapy on tumor biology in patients who had primary rectal cancer and were scheduled for elective surgery. A group treated with surgery alone was compared with a group treated with surgery after preoperative radiotherapy. The relationship between glucose use and cell kinetics was investigated. A 65% decrease in glucose use measured 2–3 wk after radiotherapy correlated with a reduction in tumor cell burden and cell death. The authors concluded that it was possible to discriminate successfully from unsuccessfully treated tumors as early as 2 wk after radiotherapy with an accuracy of 80%.
(Preoperative) Multimodality and Radiotherapy Treatment Response Evaluation in Primary Rectal Cancer
Other studies, however, warned about confounding radiotherapy-induced effects on 18F-FDG uptake. On the one hand, they can be caused by the interference of inflammatory cells because approximately 25% of 18F-FDG uptake can occur in nontumor tissues, such as macrophages, neutrophils, fibroblasts, and granulation tissue (42,43). On the other hand, they can be caused by a short-lived reversible decrease in glucose metabolism attributable to the so-called stunning of tumor cells (44). The second phenomenon can mimic actual cytotoxic therapy effects, although only temporarily. These effects led Haberkorn et al. (45) to recommend that 18F-FDG PET studies should be postponed for 60 d after radiotherapy. Such a long interval, however, is not clinically feasible in a neoadjuvant setting. After the study of Haberkorn et al. (45), only a few studies of radiotherapy response monitoring were performed (40,41,46–48). Siegel et al. (47) studied metabolic responses to a short course of radiotherapy (Table 3). A significant reduction (40%) in SUVs was found as early as days 7–8 after the start of the short course of radiotherapy. At this short interval, however, no correlation was seen between the reduction in SUVs and the tumor regression grade. The results of most of the studies (41,46–48) implied a true radiation-induced reduction in glucose use because of tumor cell loss. These results call for systematic investigations of the required interval for radiotherapy response evaluation with 18F-FDG PET.
As shown in Table 3, 15 studies of multimodality treatment (chemoradiation with or without regional hyperthermia) response monitoring were performed (44,47,49–61). Several of these studies (44,50–52,58) compared metabolic and morphologic response evaluations. It was demonstrated that the reduction in SUVs was significantly greater in (histopathologically confirmed) responders than in nonresponders. 18F-FDG PET predicted therapy outcomes significantly better than endorectal ultrasound, CT, and MRI (44,50–52). In the study of Amthauer et al. (44), 18F-FDG PET had a sensitivity of 100% and a specificity of 86% when a minimum posttherapeutic SUV reduction of 36% was used to define a response. The positive and negative predictive values were 93% and 100%, respectively. Calvo et al. (50) showed that T downstaging was significantly correlated with absolute changes in the maximum SUV (SUVmax) of −3.3 and −1.9 for responders and nonresponders, respectively (P = 0.03). Guillem et al. (49) introduced the metabolic response parameter range in total lesion glycolysis (δTLG), an important variable that subsequently was also analyzed by Melton et al. (58). This parameter not only incorporates the difference in tumor activity between baseline (pre) and posttherapy (post) scans but also takes into account changes in tumor size (volume), as follows: δTLG = {[(SUVpost × volumepost) − (SUVpre × volumepre)]/(SUVpre × volumepre)} × 100%.
In a subsequent study, Guillem et al. (51) demonstrated (probably in the same patient population) that 18F-FDG PET was able to predict long-term clinical outcomes (51). The fractional change in tumor glucose use at 4–5 wk after the completion of chemoradiation was found to be the best predictor of recurrence-free survival. The mean percentage decreases in the SUVmax after a median follow-up of 42 mo were 69% for patients without recurrence and 37% for patients with recurrence (P = 0.004). Patients with a decrease in the SUVmax of ≥62.5% and a δTLG of ≥69.5% had significantly improved recurrence-free survival (P = 0.02 and P = 0.01, respectively), and patients with a δTLG of ≥69.5% also had significantly longer overall survival (P = 0.03). The pathologic response in this group of patients surprisingly was not a significant predictor of overall survival or recurrence-free survival. In that study, a minimal metabolic response of the primary tumor was shown to reflect unfavorable tumor biology, as evidenced by a predilection for distant metastatic disease, which resulted in poor overall survival. The metabolic response of a primary tumor probably reflects overall tumor behavior rather than a local response only (51).
Kalff et al. (56) graded response visually as complete, partial, or absent. After a median follow-up of 3.1 y, all 17 patients with a complete metabolic response were free of disease. Among the 10 patients with a partial metabolic response, only 6 were free of disease. All 3 metabolic nonresponders had died. Another study in which overall survival and disease-free survival were applied as outcome measures was performed by Capirci et al. (55). This (by far the largest) study showed that evaluation of the pathologic stage combined with 18F-FDG PET at restaging identified a subgroup of patients characterized by a good response to chemoradiotherapy and a more favorable prognosis. Cascini et al. (54) performed 18F-FDG PET at baseline, 12 d after the start of chemoradiotherapy (n = 33), and after the completion of chemoradiotherapy (n = 17). That study was one of 2 studies (47,54) in which 18F-FDG PET was evaluated at an earlier and perhaps more clinically relevant stage of treatment. As early as 12 d after the start of chemoradiation, responders were identified correctly by decreases in the mean SUV (SUVmean) (with a decrease of ≥52%, the accuracy was 100%) and SUVmax (with a decrease of ≥42%, the accuracy was 94%). Measurement of the SUVmean most likely better reflects the behavior of the entire tumor mass, in which the heterogeneity and the architecture of tumor cells (viable cells mixed with fibrosis or necrosis) must be considered.
In evaluations of the pelvic region (as in patients with rectal cancer), the fusion of metabolic imaging and morphologic imaging is especially advantageous for better lesion localization and thus for reducing interpretation pitfalls (such as those associated with nonspecific 18F-FDG uptake in the bowel lumen, cavity of the uterus, inflammatory processes, and muscles). Only a few studies were performed with an integrated PET/CT system (57–60). Capirci et al. (57) studied 44 patients at baseline and at 5–6 wk after the completion of chemoradiation and used the pathologic response as an outcome measure. When they used a decrease in the SUVmax of 66.2% as the cutoff value (identified by receiver operating characteristic curve analysis) for identifying a response to therapy, Capirci et al. (57) found 79.2% specificity, 81.2% sensitivity, 77% positive predictive value, 89% negative predictive value, and 80% overall accuracy. Kristiansen et al. (59) evaluated the predictive value of integrated PET/CT in primary rectal cancer. Because they administered contrast medium before performing both PET and CT, their results may have been influenced by attenuation correction artifacts on the PET scan, resulting in a low predictive value of this multimodality imaging approach (62–65).
Because the influence of contrast enhancement (in CT) on the calculation of SUVs has not yet been totally clarified, it is preferable to use non–contrast-enhanced CT data for attenuation correction to avoid small errors in attenuation correction factors when one is monitoring changes in SUVs with PET/CT (66). However, on this topic the current literature is controversial, and some authors believe that contrast-enhanced CT can be used for attenuation correction without any difficulty (67). Although it is not clear yet whether contrast-enhanced CT should be used for attenuation correction, it can still be used for image fusion to aid in the differentiation of anatomic structures, improve lesion localization, and support lesion characterization. It is remarkable that the confounding radiotherapy-induced effects discussed earlier have less impact on the results of 18F-FDG PET when it is combined with chemotherapy or regional hyperthermia. This finding implies that the nature of the combination of treatment modalities for neoadjuvant therapy is important in the timing of 18F-FDG PET evaluations. Further studies are required to ascertain the exact sequence of time-dependent (radio)biologic effects during neoadjuvant multimodality treatment.
Despite the fact that these 19 studies (Table 3) were very heterogeneous with respect to the methods applied for PET quantification, the evaluation interval, the metabolic response criteria, and the clinical endpoints (histology or survival), most of the studies showed that 18F-FDG PET is a significant predictor of therapy outcome.
CONCLUSION
Published data indicate that 18F-FDG PET has a high predictive value in the therapeutic management of colorectal cancer. This technique could be an asset for improving patient care by reducing the effort, costs, and morbidity associated with ineffective treatment in nonresponders. The available studies on chemotherapy response monitoring in advanced colorectal cancer and on preoperative radiotherapy and multimodality treatment response evaluation in primary rectal cancer indicate that 18F-FDG PET is a significant predictor of therapy outcome in both situations. In primary rectal cancer, 18F-FDG PET is applicable after neoadjuvant treatment in a preoperative setting (important for the preoperative selection for an individually tailored surgical approach) and correlates better with pathology than morphologic imaging modalities. Interestingly, when 18F-FDG PET is able to predict the final outcome, it may be used to guide adjuvant chemotherapy for rectal cancer after optimal neoadjuvant and local treatments. 18F-FDG PET could play a central role in optimizing the use of local ablative treatment of liver metastases because it recognizes, at early times, incomplete tumor ablation that is not detectable by CT. 18F-FDG PET could play a pivotal role in determining the need for further investigations and in guiding the reading of CT scans; the interpretation of the latter alone at early times after local ablative therapy appears to be difficult. Furthermore, 18F-FDG PET may be helpful in shortening the duration of early clinical trials assessing new antineoplastic agents. Therefore, therapy response assessment with 18F-FDG PET remains a very worthwhile research topic. The reported findings call for systematic implementation in randomized trials comparing PET-controlled strategies to adequately position 18F-FDG PET in treatment time lines.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.
- 65.↵
- 66.↵
- 67.↵
- Received for publication November 4, 2008.
- Accepted for publication January 28, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- SEARCH STRATEGY AND LITERATURE SELECTION CRITERIA
- CHEMOTHERAPY RESPONSE MONITORING IN ADVANCED COLORECTAL CANCER
- MONITORING RESPONSES AFTER LOCAL ABLATIVE THERAPY OF LIVER METASTASES
- PREOPERATIVE RADIOTHERAPY AND MULTIMODALITY TREATMENT RESPONSE EVALUATION IN PRIMARY RECTAL CANCER
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Signaling Pathways That Drive 18F-FDG Accumulation in Cancer
- Combined Metabolically Active Tumor Volume and Early Metabolic Response Improve Outcome Prediction in Metastatic Colorectal Cancer
- 18F-FDG PET/CT Is an Early Predictor of Pathologic Tumor Response and Survival After Preoperative Radiochemotherapy with Bevacizumab in High-Risk Locally Advanced Rectal Cancer
- 89Zr-anti-{gamma}H2AX-TAT but not 18F-FDG Allows Early Monitoring of Response to Chemotherapy in a Mouse Model of Pancreatic Ductal Adenocarcinoma
- Molecular Imaging to Plan Radiotherapy and Evaluate Its Efficacy
- Regulation of 18F-FDG Accumulation in Colorectal Cancer Cells with Mutated KRAS
- Comparison of EORTC Criteria and PERCIST for PET/CT Response Evaluation of Patients with Metastatic Colorectal Cancer Treated with Irinotecan and Cetuximab
- Primary Jejunal Adenocarcinoma Incidentally Diagnosed on Positron Emission Tomography/Computed Tomography in a Patient With Metastatic Colorectal Cancer: Suspicion of Lynch Syndrome and Effect on Therapeutic Management
- The Oncosurgery Approach to Managing Liver Metastases from Colorectal Cancer: A Multidisciplinary International Consensus
- Discovery and validation of small-molecule heat-shock protein 90 inhibitors through multimodality molecular imaging in living subjects
- Repeatability of 18F-FDG Uptake Measurements in Tumors: A Metaanalysis
- Desmoid tumour (aggressive fibromatosis) of the colon mimics malignancy on dual time-point 18F-FDG PET/CT imaging
- [18F]Fluorodeoxyglucose Positron Emission Tomography for Outcome Prediction of Mammalian Target of Rapamycin Inhibitor Therapy
- Assessing Tumor Response to Therapy