


Abstract
In patients with locally advanced esophageal cancer, preoperative chemotherapy or chemoradiotherapy has been shown to improve outcome with respect to survival. Patients who respond to induction therapy have a significantly improved survival, compared with patients who do not respond to the therapy. However, surrogate markers that predict response or prognosis—especially early in the course of therapy—are not available in clinical routine. In patients with esophageal cancer, PET with the glucose analog 18F-FDG can be used for assessing response to therapy. Therapy response can be assessed with 18F-FDG PET and 18F-FDG PET/CT late, that is, after completion of therapy, and early in the course of therapy. In adenocarcinomas of the esophagogastric junction, 18F-FDG has been established and validated in several studies as a surrogate marker that allows prediction of response and prognosis, whereas in other studies 18F-FDG PET was not predictive of response and prognosis. The MUNICON study was an initial unicenter trial showing that a PET-guided treatment algorithm was feasible in patients with adenocarcinomas of the esophagogastric junction. The results of this study are important toward individualization of multimodal treatment. The use of 18F-FDG PET and PET/CT for therapy monitoring in esophageal cancer is the subject of intense discussion, underlining the need for randomized multicenter studies. From a methodologic point of view, the most important issue in therapy monitoring using 18F-FDG PET and PET/CT is the standardization of patient preparation, data acquisition and processing, and data interpretation, especially for prospective randomized multicenter studies. In conclusion, single-center studies investigating response assessment in patients with esophageal cancer have provided promising results. In the future, prospective randomized multicenter trials will have to be performed and research will address new imaging probes and innovative therapy regimens.
Esophageal cancer is among the 10 most common malignancies worldwide and is associated with a high mortality (1,2). Carcinomas of the esophagus represent a heterogeneous group of tumors with respect to epidemiology, etiology, and histopathology (3). Squamous cell carcinoma (SCC) occurs most frequently in the upper two thirds of the esophagus, with alcohol and smoking being the main risk factors. In the lower third of the esophagus and the esophagogastric junction, adenocarcinoma is more prevalent, and reflux and obesity are the most important risk factors. Adenocarcinoma originates from metaplastic epithelial cells in the esophagogastric junction that transform into an intestinal-type mucosal layer through irritation by gastric juice. Over the last few decades, the incidence and prevalence of esophageal adenocarcinoma have increased, and esophageal adenocarcinoma occurs increasingly more often than does SSC (4). Often, the tumors are locally advanced at the time of initial diagnosis because symptoms do not appear until late (T3–T4, N+, or M1). Preoperative assessment of prognostic factors is important in clinical management of the patients. Relevant pretherapeutic prognostic factors are local tumor invasion, locoregional lymph node stage, and distant metastases. Endoscopic ultrasound and CT represent the most widely used imaging modalities for the assessment of local tumor invasion and locoregional lymph node involvement. Locoregional lymph node stage is a strong prognostic factor: the number of lymph nodes, the location, and the size are strong predictors of survival. Noninvasive lymph node staging with conventional imaging modalities is rather limited. The sensitivity and specificity vary significantly among different studies and depend—among other factors—on the criteria used for the classification of regional lymph node involvement.
Precise pretherapeutic staging is important in choosing the best available therapy for the patient. It is crucial to be able to differentiate patients with locoregional disease from patients with systemic disease. In systemic disease, there is no curative option and the patients will receive palliative treatment (metastases in the celiac lymph nodes (M1a) are considered distant for tumors of the lower thoracic esophagus; metastases in the cervical lymph nodes are considered distant for tumors of the upper thoracic esophagus). Therefore, distant metastases have to be ruled out before initiation of therapy. 18F-FDG PET has a sensitivity and specificity of 67% (95% CI, 58%−76%) and 97% (95% CI, 90%−100%), respectively, in M staging of esophageal cancer (5).
After exclusion of distant metastases, the selection of the therapeutic regimen depends on the T stage. Localized tumors (T1/T2) have a high likelihood of R0 resection, and primary esophagectomy represents the most frequent therapeutic procedure.
In cases of locally advanced tumors (T3/T4, N+), surgery remains the mainstay of therapy, but evidence is growing that preoperative chemotherapy or chemoradiotherapy improves survival in patients with esophageal cancer (6–8). In a metaanalysis, Gebski et al. (7) showed that the hazard ratio for all-cause mortality with neoadjuvant chemoradiotherapy alone was 0.81 (95% confidence interval, 0.70–0.93; P = 0.002), corresponding to a 13% absolute difference in survival at 2 y (with similar results for SCC and adenocarcinoma). The hazard ratio for neoadjuvant chemotherapy was 0.90 (95% confidence interval, 0.81–1.00; P = 0.05), which is equivalent to a survival benefit of 7% (but no effect for SCC) (7). However, the metaanalysis by Gebski et al. was based on the results of numerous phase II and underpowered phase III clinical trials. In several recent studies, neoadjuvant chemoradiotherapy but not neoadjuvant chemotherapy has been shown to significantly improve overall survival in SCC (9–13). Nevertheless, chemoradiotherapy is a commonly used therapeutic approach for patients with SCC. In contrast, neoadjuvant chemotherapy is now widely accepted as a standard therapy in the treatment of locally advanced adenocarcinoma of the esophagus and esophagogastric junction (6–8). The rationale for neoadjuvant treatment might be a preoperative downsizing resulting in a higher R0 resection rate. Overall, the evidence to support downsizing is conflicting. Indeed, the Fédération Francophone de Cancérologie Digestive trial did show a significantly higher R0 resection rate after neoadjuvant chemotherapy (14). However, other trials, although positive for neoadjuvant chemotherapy, did not show a significantly higher R0 resection rate.
Neoadjuvant chemoradiotherapy for adenocarcinoma of the esophagus improves overall survival. In the metaanalysis by Gebski et al. (7), a similar survival benefit for neoadjuvant chemoradiotherapy and neoadjuvant chemotherapy was reported. Stahl et al. (15) observed a significantly higher response rate to neoadjuvant chemoradiotherapy than to neoadjuvant chemotherapy alone. However, the higher response to neoadjuvant chemoradiotherapy was accompanied by an increase of more than 10% in postoperative mortality.
Taken together, converging evidence reveals that patients undergoing neoadjuvant treatment and showing an objective tumor response have a better prognosis for survival than do those undergoing surgery alone. However, only 40%−50% of the patients respond to therapy. As a consequence, the patients who do not respond to therapy, may be compromised by toxic side effects and the delay caused by ineffective chemotherapy or chemoradiotherapy, and potentially have even biologically more aggressive tumors. Therefore, it is desirable to have a diagnostic test that allows noninvasive prediction of response so that responders can be differentiated from nonresponders early in the course of treatment, potentially enabling individualization of—that is, a change in—therapy in the nonresponding patients. No pretherapeutically available molecular markers predicting response or prognosis are available for esophageal cancer so far.
18F-FDG PET has shown promising results in assessing response to therapy and tumor control and in prognosis (16–18). Among these, assessment of early response to therapy has gained importance because it implies clinical consequences in the diagnostic management of patients. So far, almost all published studies on assessing therapy response in esophageal cancer have been performed with 18F-FDG PET. With the advent of PET/CT, which allows one to combine the structural information provided by helical CT with molecular imaging by PET, an almost simultaneous assessment of tumor morphology and metabolism over time has become possible (17). Changes in regional tumor metabolism may precede changes detectable by structural imaging (19). Moreover, PET/CT, by combining volumetric and metabolic measurements, may be even more accurate for assessing histopathologic tumor response in patients with advanced esophageal cancer. In general, 18F-FDG PET and 18F-FDG PET/CT studies to assess the response to therapy can be divided into 2 groups.
First, tumor response can be assessed after the completion of therapy. In this case, residual 18F-FDG uptake after therapy or changes in 18F-FDG uptake between the initial PET/CT scan and the posttherapy scan are correlated to postoperative histopathologic response, patient survival, or both. 18F-FDG uptake in patients responding to therapy should decrease to the background level, and residual 18F-FDG accumulation indicates viable tumor tissue in most cases. It is not necessary to perform a quantitative analysis.
Second, tumor response can be assessed early in the course of therapy (i.e., chemotherapy or chemoradiotherapy). 18F-FDG PET/CT will then take place before therapy, and a second scan is performed 2–4 wk after initiation of the first therapy cycle (often within the first cycle). Changes in 18F-FDG uptake between the pretherapeutic scan and the early follow-up scan are used to predict histopathologic response, and patient survival. The standardized uptake value is the most widely used 18F-FDG PET parameter, and in most studies, relative changes (%) are calculated to quantify metabolic response. Early in the course of treatment, metabolic activity in the tumor tissue most probably will have decreased in responders, but at the time of the second scan there will still be a considerable number of viable tumor cells, resulting in still significant 18F-FDG uptake.
ASSESSMENT OF RESPONSE LATE IN THERAPY
Several studies have evaluated the role of 18F-FDG PET in assessing response after completion of chemotherapy and chemoradiotherapy in patients with SCC and adenocarcinoma of the esophagus (Table 1).
18F-FDG PET and 18F-FDG PET/CT in Assessment of Response After Completion of Therapy for Esophageal Cancer
Brücher et al. (20) published results on 27 patients with SCC of the esophagus who underwent 18F-FDG PET before and after chemoradiotherapy. A threshold of 52% mean standardized uptake value (SUV) not only was a strong prognostic factor but also differentiated histopathologic responders from nonresponders with a sensitivity of 100% and a specificity of 55%. The authors showed that patients with a mean SUV decrease of less than 52% had a significantly shorter median survival than did patients with a maximum SUV decrease of more than 52% (8.8 mo vs. 22.5 mo, P < 0.0001). Flamen et al. (21) showed in 36 patients with esophageal cancer (27 cases of SCC and 9 of adenocarcinoma) that a decrease of more than 80% in the tumor-to-liver uptake ratio 3–4 wk after completion of neoadjuvant chemoradiotherapy predicted response with a sensitivity of 71% and a specificity of 82%. In a study by Downey et al. (22), 17 patients with esophageal cancer (14 cases of adenocarcinoma and 3 of SCC) underwent sequential 18F-FDG PET. The authors used a threshold of 60% for decrease in maximum SUV after the completion of chemoradiotherapy. A maximum SUV reduction of more than 60% was correlated with better 2-y disease-free survival (67% vs. 38%, P = 0.055). Swisher et al. (23) published results on 103 patients with histologically diagnosed adenocarcinoma (n = 90) and SCC (n = 13) and assessed the prognostic relevance of the 18F-FDG uptake after completion of neoadjuvant chemoradiotherapy. An SUV of 4 or more was the best predictor of long-term survival (P = 0.04; hazard ratio, 3.5). The 18-mo survival of patients with a postchemoradiotherapy SUV of 4 or more was 34%, compared with 77% for patients with an SUV of less than 4 (P = 0.01). The accuracy in predicting histopathologic nonresponse was 76%, and the corresponding sensitivity and specificity were 62% and 84%, respectively. However, the authors also demonstrated that PET failed to rule out residual microscopic disease, because 18F-FDG uptake in the tumor bed was not different between patients with no residual viable tumor cells and patients with up to 10% viable tumor cells. In another study, by Cerfolio et al. (24), 48 patients with esophageal cancer (41 cases of adenocarcinoma and 7 of SCC) underwent 18F-FDG PET/CT before and 3–4 wk after neoadjuvant chemoradiotherapy. 18F-FDG PET/CT predicted a complete response with a sensitivity of 87%, a specificity of 88%, and an accuracy of 88%. The authors compared 18F-FDG PET/CT, endoscopic ultrasound with fine-needle aspiration, and CT for predicting complete responders and concluded that, on the basis of their findings, 18F-FDG PET/CT was more accurate than endoscopic ultrasound with fine-needle aspiration (sensitivity, 20%; specificity, 94%; accuracy, 70%) and CT (sensitivity, 27%; specificity, 91%; accuracy, 71%). A study by Kim et al. included 62 patients with esophageal cancer for 18F-FDG PET assessment of late response to therapy (25). Complete metabolic response (reduction of maximum SUV > 80%) after completion of preoperative chemoradiotherapy correlated significantly with histopathologic response and predicted long-term outcome. Multivariate analysis revealed that complete metabolic response was significantly associated with better disease-free survival and overall survival (P = 0.006 and P = 0.033, respectively). Port et al. investigated the ability of 18F-FDG PET to predict clinical response, pathologic response, and survival in 62 patients with esophageal cancer (51 cases of adenocarcinoma and 11 of SCC) who were undergoing preoperative chemotherapy (26). Patients with a 50% or greater reduction in the maximum SUV of their primary tumor had significantly better disease-free survival than did patients with a less than 50% reduction in maximum SUV (median disease-free survival, 35.5 mo vs. 17.9 mo, respectively; P = 0.03). However, the authors also provided evidence that a complete absence of residual 18F-FDG uptake is not necessarily associated with a complete pathologic response. In a study published by Smithers et al. on 45 patients with adenocarcinoma of the esophagus, 18F-FDG PET was performed before treatment and 3–6 wk after completion of platinum-based chemotherapy (27). The authors found no correlation between the 18F-FDG PET response and the histopathologic response in their study cohort.
Taken together, most studies assessing late response to therapy for esophageal cancer have shown that the 18F-FDG PET signal after neoadjuvant therapy correlates with histopathologic response and long-term prognosis. However, the main drawback of late assessment is that it does not allow the therapy to be modified for patients not responding to it. One might speculate whether patients benefit from a change in therapy after a late response assessment. However, clinical trials are necessary to answer the question of whether further neoadjuvant or adjuvant chemotherapy or chemoradiation for 18F-FDG PET nonresponders improves the clinical outcome. So far, late response assessment has been able to give information only on the prognosis of patients. However, for locally advanced adenocarcinomas, surgery remains the mainstay of treatment. Consequently, the additional information provided by a late assessment is limited, especially as the histopathologic response will be known soon after PET. Therefore, an early assessment of response to therapy by PET with 18F-FDG has been proposed—but is not yet established in clinical routine—as a surrogate marker for predicting response and potentially allows a change in therapy early.
ASSESSMENT OF RESPONSE EARLY IN THERAPY
In esophageal cancer, several studies have used 18F-FDG PET to assess response to therapy early in the course of disease (Table 2).
18F-FDG PET and 18F-FDG PET/CT in Early Assessment of Response to Therapy for Esophageal Cancer
Weber et al. performed an initial study to monitor response to treatment with 18F-FDG PET early in the course of therapy in 40 patients (37 patients evaluable for therapy response assessment) with locally advanced adenocarcinoma of the esophagogastric junction (28). 18F-FDG PET was performed before the initiation of preoperative therapy and was repeated on day 14 of the first chemotherapy cycle. For the quantitative assessment of therapy response, a circular region of interest (diameter, 1.5 cm) was placed over the tumor in the slice with the maximum SUV in the baseline scan. In the second PET scan, the region of interest was placed at the same position as in the baseline study. The resected specimens were analyzed histopathologically. Tumor regression was assessed semiquantitatively according to a published scoring system from Becker et al. (29). All patients with less than 10% residual tumor cells (regression score, grade 1) were classified as responding. All other patients were classified as nonresponding.
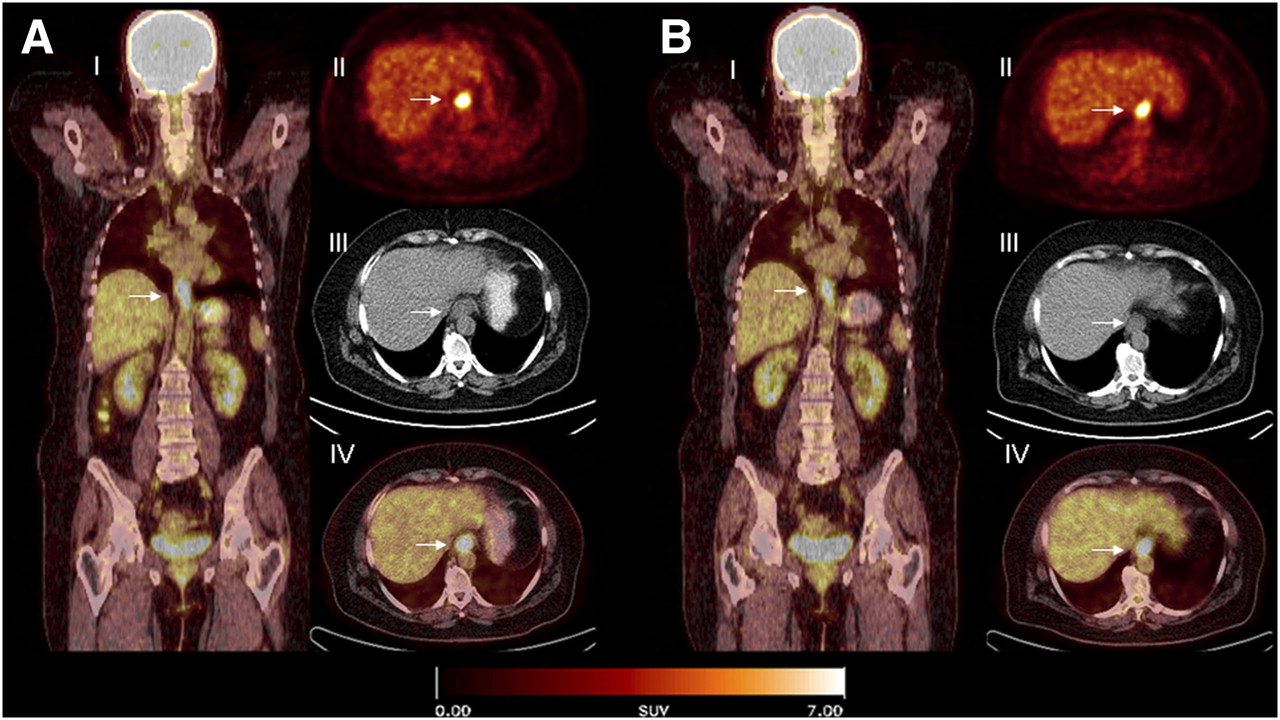
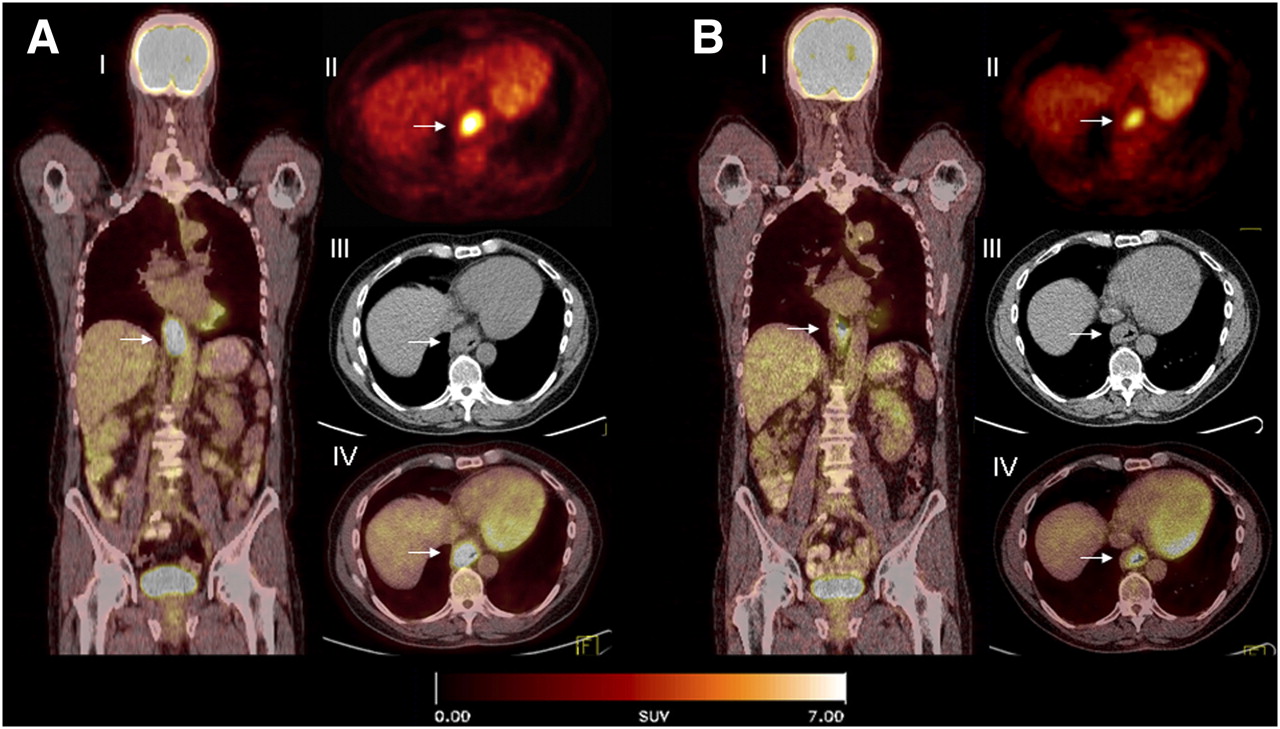
The authors showed that 18F-FDG PET allowed prediction of histopathologic response by metabolic response assessment as early as 2 wk after the initiation of platin-based chemotherapy. They established a metabolic threshold—defined as a reduction of more than 35% in baseline mean SUV—that allowed the prediction of clinical response with a sensitivity and specificity of 93% and 95%, respectively. The mean (±SD) 18F-FDG uptake (SUV) at baseline was 17.9 ± 8.1. Metabolic response was associated with a significantly longer time to progression (P = 0.01) and significantly longer overall survival (P = 0.04). Figures 1 and 2 show PET images for a metabolic nonresponder and a metabolic responder.

Coronal PET/CT (I), axial PET (II), CT (III), and PET/CT (IV) images of a patient with locally advanced adenocarcinoma of the esophagogastric junction (arrow) before (A) and 14 d after beginning (B) neoadjuvant chemotherapy. Fourteen days after initiation of neoadjuvant chemotherapy, tumor metabolic activity is marginally decreased (<35%). After completion of chemotherapy, more than 50% tumor cells were found in resected specimen.

Coronal PET/CT (I), axial PET (II), CT (III), and PET/CT (IV) images of a patient with locally advanced adenocarcinoma of the esophagogastric junction (arrow) before (A) and 14 d after beginning (B) neoadjuvant chemotherapy. Already 14 d after initiation of neoadjuvant chemotherapy, tumor metabolic activity is markedly decreased (>35%). After completion of chemotherapy, no viable tumor cells were found in resected specimen.
Wieder et al. used 18F-FDG PET to assess early response to chemoradiotherapy in 27 (23 underwent surgery) patients with SCC of the esophagus (30). Early metabolic response—defined as a reduction of more than 30% in baseline SUV—predicted histopathologic response with a sensitivity and specificity of 93% and 88%, respectively. Early changes in metabolic activity using this threshold were also a strong predictor of survival (P < 0.011). In a study by Gillham et al., early response assessment was performed on a study cohort of 32 patients with esophageal cancer (31). 18F-FDG PET failed to predict histopathologic response in that study. Schmidt evaluated the predictive and prognostic potential of 18F-FDG PET in 133 patients with advanced esophageal cancer. All patients received neoadjuvant chemoradiation. The authors did not find a correlation of SUV with histopathologic response and prognosis (32). Ribi et al. included 66 patients with advanced esophageal cancer in a multicenter trial. Less than a 40% reduction in 18F-FDG uptake predicted histopathologic response with a sensitivity of 70%, a specificity of 50%, and a negative predictive value of 70% (33). These 3 studies (31–33) had distinct differences from the studies by Weber et al. (28), Ott et al. (34), and Lordick et al. (35). First, metabolic response was assessed not at 2 wk after the initiation of the therapy but after only 1 wk of neoadjuvant chemoradiotherapy in the study by Gillham et al. (31), after 3–4 wk in the study by Schmidt et al. (32), and after the second cycle of chemotherapy in the study by Ribi et al. (33). Second, in all 3 studies (31–33), patients received chemoradiotherapy, which was not the case in the studies by Weber et al. (28), Ott et al. (34), and Lordick et al. (35), in which patients received induction chemotherapy. When radiotherapy is part of the regimen, nonspecific 18F-FDG accumulation in inflammatory lesions is of major importance for therapy monitoring. False overestimation of 18F-FDG uptake might occur in tumors with an inflammatory component or, more often, might be due to radiation-mediated inflammatory processes—which may persist from weeks to months—potentially influencing the assessment of changes in glucose metabolism during assessment of response to therapy (36).
Ott et al. (34) validated the metabolic threshold (a cutoff of a 35% decrease in mean SUV) established by Weber et al. (28) in a prospective study on 65 patients with locally advanced adenocarcinomas of the esophagogastric junction. Histopathologic response was predicted by 18F-FDG PET with a sensitivity of 80% and a specificity of 78%. The mean 18F-FDG uptake at baseline was 8.1 ± 3.4. The baseline SUVs in the study by Weber et al. (28) were normalized to body surface area and not body weight. Therefore, the absolute SUVs cannot be directly compared with those from the study by Ott et al. (34), which used SUVs normalized to body weight. After a median follow-up of 42 mo, the overall median survival of metabolic nonresponders was 18 mo, whereas median survival had not been reached for metabolic responders (P = 0.01). Metabolic responders had a significantly higher 3-y survival rate than did metabolic nonresponders (70% vs. 35%, P = 0.01). In the subgroup of completely resected (R0) patients, a multivariate analysis including ypT-category, ypN-category, and histopathologic response depicted metabolic response as the only predictor for recurrence (P < 0.018). The findings of these studies suggested that 18F-FDG PET could possibly be used to individualize treatment.
The unicenter MUNICON study was an initial trial to prospectively evaluate the feasibility and potential effect on prognosis of administering PET-response–guided chemotherapy to patients with locally advanced adenocarcinoma of the esophagus and the esophagogastric junction (35). By contrast, the studies of Weber et al. (28) and Ott et al. (34) established and validated the cutoff for metabolic response in the early prediction of response. In the MUNICON study, 110 patients were evaluable for metabolic response assessment. Metabolic responders (after 2 wk of induction chemotherapy) continued to receive chemotherapy for a maximum of 12 wk before undergoing surgery, whereas metabolic nonresponders discontinued chemotherapy after only 2 wk and were immediately resected. Of the evaluable 110 patients, 49% were classified as metabolic responders and 104 patients underwent resection. A histopathologic response was achieved in 58% of the metabolic responders. After a median follow-up of 2.3 y, median overall survival was not reached in metabolic responders, whereas median overall survival was 25.8 mo in nonresponders (hazard ratio, 2.13; P = 0.015). Median event-free survival was 29.7 mo in metabolic responders and 14.1 mo in nonresponders (hazard ratio, 2.18; P = 0.002). In the study by Ott et al. (34), the median recurrence-free period and overall median survival after continuing chemotherapy in metabolically nonresponding patients with similar tumor stages and similar preoperative chemotherapy were 10 and 18 mo, respectively. In the MUNICON study, the corresponding median recurrence-free period and overall median survival were 14.1 and 25.8 mo.
These results show satisfying sensitivities and specificities given that no other imaging modality or surrogate marker allows a more accurate early prediction of response to therapy. The response of tumors can be assessed by 18F-FDG PET as early as 2 wk after the initiation of the first chemotherapy cycle, whereas postsurgical parameters (i.e., ypT, R0) and histopathologic response can be determined only at 3–4 mo after the initiation of preoperative chemotherapy. Consequently, patients without a metabolic response after 2 wk of preoperative chemotherapy could receive an alternative therapy regimen early after the onset of preoperative chemotherapy. Furthermore, the fact that the negative predictive value is high is of major importance because patients who do not respond to treatment can be identified and a change in the therapy regimen can be considered. On the other hand, limitations also exist, such as the possible inflammatory changes that may influence the assessment of response. In addition, because of the partial-volume effect, tumor shrinkage due to therapy initiation may lead to underestimation of 18F-FDG uptake in the second 18F-FDG study and, in turn, to overestimation of the change in SUV.
Early assessment with 18F-FDG PET of the response to therapy in patients with locally advanced adenocarcinomas has shown promising results in single-center studies and should now be evaluated in randomized, prospective multicenter trials. Such trials are an important step toward possible implementation in clinical practice. Recently, a multicenter trial called Neoadjuvant Therapy Monitoring with PET and CT in Esophageal Cancer (NEOPEC) was launched as part of a randomized Dutch trial comparing neoadjuvant chemoradiotherapy for 5 wk followed by surgery, versus surgery alone. The neoadjuvant arm will include 150 patients from 6 centers within 3 y. Primary endpoints will be a difference in accuracy and in negative predictive value between 18F-FDG PET and CT. Moreover, a PET-guided treatment algorithm has proven to be feasible for patients with locally advanced adenocarcinomas (35) and should—in a next step—be validated and evaluated in randomized prospective multicenter trials (37). Identification of patients not responding to initial therapy is of great clinical interest because chemotherapy-induced side effects could be reduced and the costs of ineffective therapy avoided. However, it is still unclear whether a PET-guided treatment algorithm will result in a survival benefit. Although the MUNICON trial suggested that early discontinuation of chemotherapy in metabolic nonresponders had no negative consequences, that suggestion was from comparisons of this trial with previous trials by the same group. Therefore, randomized prospective multicenter trials are necessary to answer this question. Furthermore, so far only limited experience with therapy guided by PET assessment of early response has been obtained. Standardization of patient preparation, data acquisition and processing, and data interpretation is an important issue, especially for prospective randomized multicenter studies. Currently, the implementation of PET-guided treatment algorithms for treatment of patients with esophageal cancer is not recommended outside clinical trials.
Molecular imaging probes that reflect more specifically tumor biology might also represent a future approach to increase the accuracy of PET/CT prediction of response to therapy. For example, Westreenen et al. investigated the feasibility of imaging proliferation with 18F-FLT PET for the detection of esophageal cancer and compared 18F-FLT-PET with 18F-FDG PET in 10 patients (38). However, in that study the sensitivity of 18F-FDG PET was higher than that of 18F-FLT PET. Furthermore, the authors were not able to show a correlation between 18F-FDG and 18F-FLT uptake and the proliferation index (Ki-67).
Combining 18F-FDG PET/CT with biomarkers to more accurately predict response to therapy is also under investigation. Choi et al. investigated 51 patients with squamous carcinoma of the esophagus before curative surgery with 18F-FDG PET (39). Biopsies of tissue samples were stained for markers of angiogenesis (VEGF), proliferation, and intratumoral microvessel density. In a univariate analysis, survival was correlated with tumor stage, maximum SUV, tumor length, 18F-FDG PET–positive lymph nodes, proliferation index, angiogenesis, and intratumoral microvessel density. In a multivariate analysis, intratumoral microvessel density and VEGF expression proved to be independent prognostic factors additional to pathologic tumor stage and the number of 18F-FDG PET–positive lymph nodes. In a study by Westerterp et al. (40), 26 patients underwent 18F-FDG PET as well as biopsy of tissue samples, which were immunohistochemically stained for markers of angiogenesis (VEGF, CD31), glucose transporter-1, hexokinase isoforms, Ki-67, macrophages (CD68), and apoptosis (cleaved caspase-3). Glucose transporter-1 expression and tumor size were the only parameters that correlated with 18F-FDG uptake.
The past few years have seen progress emerge in the understanding of molecular pathways that are important in cancer biology. Several new molecular targets have been identified, and specific drugs targeting these molecular sites have subsequently been developed. Imaging of molecular targets is of high importance for the development of targeted drugs (41). In esophageal cancer, several new potential targets for a specific (targeted) therapy have been identified.
The 2 best-studied classes of targeted agents are the cell-growth inhibitors and the antiangiogenic drugs. In a recent trial by Di Fabio et al. (42), 18F-FDG PET showed a metabolic response in 60% of patients with gastric cancer and cancer of the esophagogastric junction after treatment with cetuximab (an anti–epidermal growth factor receptor monoclonal antibody) combined with the FOLFIRI regimen (folinic acid, fluorouracil, and irinotecan). Most importantly, median progression-free survival was significantly longer in metabolic responders (11 vs. 5 mo). Further upcoming targeted agents used in clinical trials include regulation of the inflammatory response, cell-cycle regulation, induction of apoptosis, and regulation of invasion and metastasis. Although early signs of activity have been reported for these drugs, it is too early for them to be implemented into standard therapy protocols. However, although limited experience exists in the evaluation of response to these new targeted agents, evaluation of early response seems especially attractive, to reduce the costs of these new, expensive agents. Besides the development of new drugs, the identification of biomarkers that can be used to select a specific therapy for a particular patient will also be necessary. Recently, the mutational status of kras in colorectal cancer has been shown to predict response to treatment with monoclonal antibodies directed against the epidermal growth factor receptor (43). Other biomarkers, such as FcgR polymorphisms (44) or ERCC1 (45), have also been shown to predict response to antibody treatment and chemotherapy with cisplatin. Therefore, future trials incorporating new drugs and biomarkers are necessary to further improve the clinical outcome of patients with esophageal cancer.
CONCLUSION
18F-FDG PET and 18F-FDG PET/CT can provide robust and reproducible criteria for assessing the response to therapy in esophageal cancer. PET-guided induction chemotherapy has been shown to be feasible in adenocarcinomas of the esophagogastric junction. However, the reported results are the subject of intense debate, underlining the urgent need for randomized multicenter studies with standardized protocols. Future research will have to address new imaging probes and innovative therapy regimens.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 24, 2008.
- Accepted for publication February 9, 2009.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial
- Repeatability of 18F-FDG Uptake Measurements in Tumors: A Metaanalysis
- Intratumor Heterogeneity Characterized by Textural Features on Baseline 18F-FDG PET Images Predicts Response to Concomitant Radiochemotherapy in Esophageal Cancer
- Early Repeated 18F-FDG PET Scans During Neoadjuvant Chemoradiation Fail to Predict Histopathologic Response or Survival Benefit in Adenocarcinoma of the Esophagus
- Assessing Tumor Response to Therapy