


Abstract
Radiolabeled prostate-specific membrane antigen (PSMA) ligands represent a true theranostic concept for diagnosis and therapy in patients with relapsed or metastatic prostate cancer. The aim of this study was to evaluate the response to and tolerability of a single dose of 177Lu-PSMA-617 in a large cohort of patients with metastatic castration-resistant prostate cancer (mCRPC). Methods: The data of 82 consecutive patients (median age, 73 y; range, 43–87 y) with mCRPC who received a single dose of 177Lu-PSMA-617 (mean, 5.9 ± 0.5 GBq) were retrospectively analyzed. Data were collected at baseline and 8 wk after therapy. 68Ga-PSMA-11 PET/CT was performed on all patients to verify sufficient PSMA expression. Bone, lymph node, liver, and lung metastases were present in 99%, 65%, 17%, and 11% of the patients, respectively. Tolerability and response were evaluated using hematologic parameters, renal scintigraphy, clinical data, and the prostate-specific antigen (PSA) level at baseline and 8 wk after therapy application. Results: Six patients died, and 2 patients dropped out because they were not willing to continue therapy and follow-up. The complete dataset of 74 patients was available for analysis. Forty-seven patients (64%) showed a PSA decline, including 23 (31%) with a decline by more than 50%. Thirty-five patients (47%) had stable disease: the change in their PSA level ranged from less than a 50% decline to less than a 25% rise. Seventeen patients (23%) had progressive disease: their PSA level rose by more than 25%. There were no significant changes in hemoglobin, white blood cells, creatinine, or tubular extraction rates indicative of toxicity. There was a significant but mild decrease in platelets, but the median value was still within the reference range. Conclusion: This retrospective multicenter analysis suggests that radioligand therapy with 177Lu-PSMA-617 is safe and well tolerated and has a considerable effect on PSA level. Therefore, it offers an additional therapeutic option for patients with mCRPC. These data may justify further prospective randomized studies to evaluate and prove the clinical benefit in terms of survival and quality of life.
Prostate-specific membrane antigen (PSMA) is a promising target in diagnostics and therapy of metastatic prostate cancer. In the last few years, there has been increasing evidence that PSMA imaging is valuable for diagnosis of recurrent and metastatic prostate cancer and, more recently, for preoperative staging of biopsy-proven prostate cancer patients to rule out distant metastases and evaluate the extent of intraprostatic disease (1–5).
With regard to the high PSMA expression on prostate cancer cells, especially in high-grade metastatic disease and castration-resistant prostate cancer, the possibility of using PSMA as a therapeutic target has been a topic of interest during the past decade (6–8). The first attempts at therapy using the 90Y-labeled monoclonal antibody CYT-356, which binds to the intracellular component of PSMA, did not have favorable results (6). Further study using the 177Lu-labeled monoclonal antibody J591 showed promising results in a phase II trial treating patients with progressive castration-resistant prostate cancer (7).
Introduced by the German Cancer Research Center in Heidelberg, PSMA-617 is a true theranostic agent in imaging and therapy of prostate cancer (9). In a first cohort of 10 patients, a single dose of 177Lu-PSMA-617 showed a low toxicity profile and a respectable effect on prostate-specific antigen (PSA) level (8).
The aim of this retrospective study was to evaluate the response to and toxicity of this novel therapeutic option in a large cohort of metastatic castration-resistant prostate cancer (mCRPC) patients, who were treated with a single dose of 177Lu-PSMA-617 as salvage therapy.
MATERIALS AND METHODS
Patient Population
The data of 82 consecutive patients (median age, 73 y; range, 43–87 y) with mCRPC were analyzed after treatment with a single dose of 177Lu-PSMA-617 in the nuclear medicine departments of the university hospitals of Bonn, Muenster, Cologne, and Aachen between December 2014 and November 2015. The mean administered activity was 5.9 ± 0.5 GBq. The patient data were analyzed retrospectively according to their response to the treatment and its tolerability.
Radioligand therapy with 177Lu-PSMA-617 was performed as “compassionate use” according to the German Medicinal Drugs Act, AMG §13 2b. The decision to offer this treatment was made by the local interdisciplinary institutional tumor board. The prerequisite for salvage therapy was the absence of other therapeutic options: disease progression despite first- or second-line chemotherapy (docetaxel and cabazitaxel) or ineligibility for chemotherapy or 223Ra-dichloride. The patients also needed to have been previously treated with at least one of the new-generation hormone therapy drugs (abiraterone or enzalutamide). All patients consented to the 177Lu-PSMA-617 treatment in writing after receiving detailed information about it and its possible risks and side effects. Retrospective analysis was performed according to institutional ethical guidelines, and the requirement for separate informed consent for this analysis was waived.
Patient Preparation
68Ga-PSMA-11 PET/CT was performed before the therapy, using a previously described procedure (3,5), to demonstrate PSMA-positive metastatic disease and adequate PSMA expression in tumor lesions. In accordance with clinical standards, renal scintigraphy was also performed before the therapy, using a previously described procedure (10,11), to rule out obstructive disease and to evaluate kidney function. In cases of obstructive disease, the patients were referred to the local urologist to reduce the obstruction as much as possible.
Blood samples were drawn on the day of therapy (before tracer administration) and 8 wk afterward. The PSA level, alkaline phosphatase level, hematologic parameters, and kidney and liver status were determined at both time points. Additional blood samples were drawn by each patient’s general practitioner during the 8-wk follow-up, but because these data were incomplete they are not presented here.
Preparation of 177Lu-PSMA-617
PSMA-617 precursor was obtained from ABX GmbH. 177Lu was obtained from ITG Isotope Technologies and IDB Holland BV. The in-house production and labeling of 177Lu-PSMA-617 were in accordance with the German Medicinal Drugs Act, AMG §13 2b. The labeling procedures have been described in detail previously (8).
Therapy Administration
To reduce 177Lu-PSMA-617 uptake in the salivary glands, they were cooled with cold packs from 30 min before the injection until 4 hours after the injection.
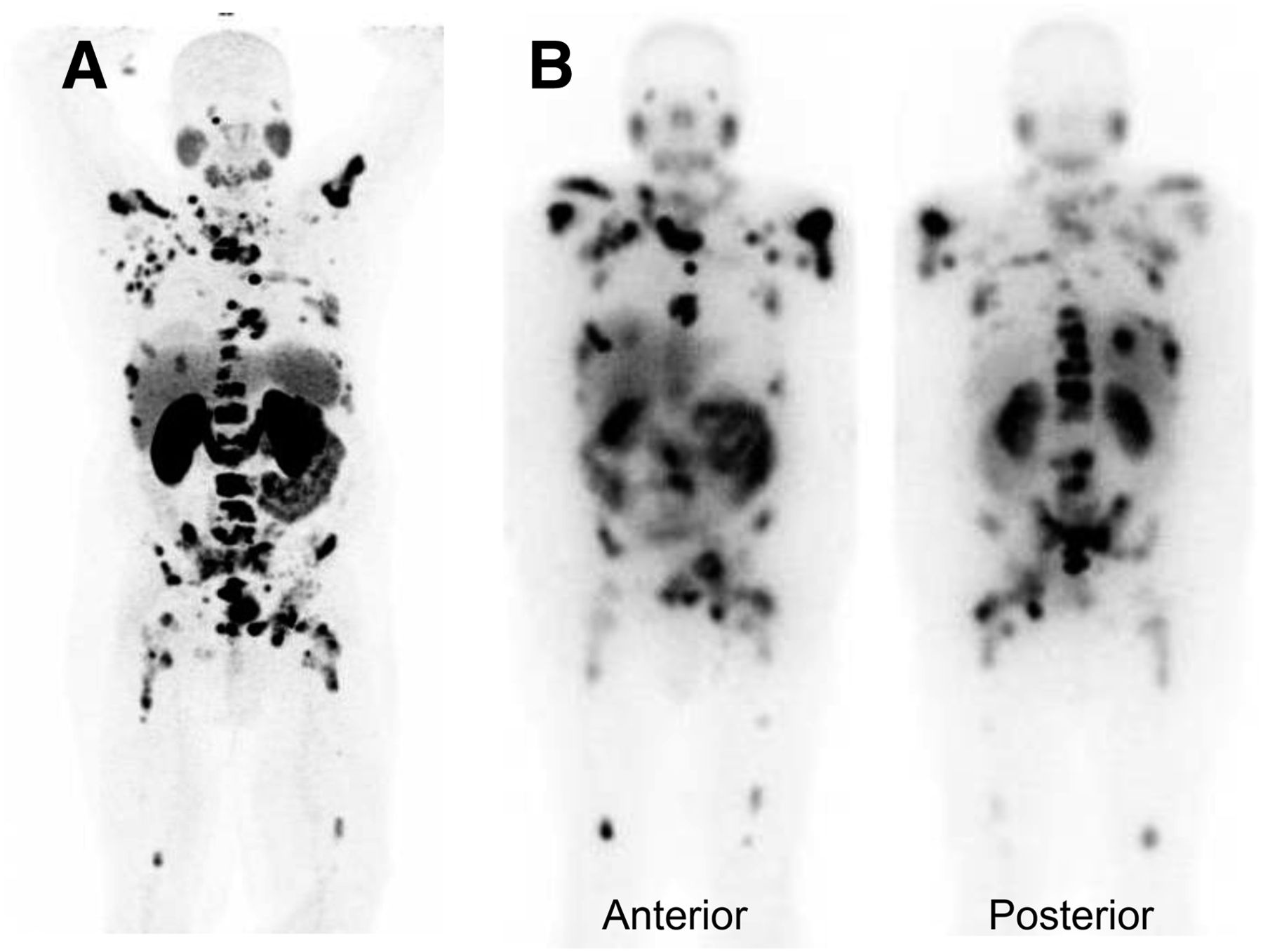
Nearly 6 GBq of 177Lu-PSMA-617 (mean, 5.9 ± 0.5 GBq) were injected intravenously as a slow bolus within 30–60 s followed by at least 1,000 mL of Ringer solution or isotonic NaCl solution. Immediately afterward and at 10 min, 24 h, and 48 h afterward, whole-body scintigraphic imaging was performed to document uptake and retention of 177Lu-PSMA-617 in tumor lesions. The images showed high 177Lu-PSMA-617 uptake within the metastatic lesions that had been seen on the pretherapeutic 68Ga-PSMA PET images (Fig. 1).

(A) Maximum-intensity-projection 68Ga-PSMA PET image showing multiple bone and lymph node metastases. (B) Posttherapeutic planar scintigraphic images showing high 177Lu-PSMA-617 uptake within lesions corresponding to those seen on PET image.
Evaluation of Response and Toxicity
Changes in PSA level were considered the main indicator of response. Although these changes were not confirmed by the second measurement recommended by the Prostate Cancer Working Group 2 criteria (12), we used those criteria as guidance for response evaluation. A PSA decline by 50% or more was considered a response, a change in PSA level ranging from less than a 50% decline to less than a 25% rise was considered stable disease, and a PSA rise by more than 25% was considered progressive disease. Therapy-induced changes in alkaline phosphatase level were also analyzed.
The Eastern Collaborative Oncology Group (ECOG) performance status was documented at baseline and 8 wk after therapy. Toxicity-attributed side effects and hematologic changes were documented according to version 4.0 of the Common Toxicity Criteria for Adverse Events.
Statistical Analysis
SPSS Statistics (version 23; IBM Inc.) was used for analysis. The descriptive statistics are reported as median and range when applicable. Wilcoxon signed rank testing was performed to determine the significance of differences between median values. A P value of less than 0.05 was considered significant.
RESULTS
Six patients died because of extensive disease, and 2 patients dropped out because they did not wish to be referred for further evaluation and therapy. The data of 74 patients were available for analysis. Patient characteristics at baseline, including extent of metastatic disease and prior therapies, are given in Table 1. Most patients (99%) had bone metastases; 84% of those patients were highly compromised by disseminated, multifocal bone metastases.
Patient Characteristics at Baseline
Eighty-one patients were formally castration-resistant and had received antiandrogen therapy before the 177Lu-PSMA-617 therapy. Only one patient did not receive antiandrogen therapy, because at baseline he had non–hormone-active neuroendocrine prostate cancer and a very low PSA level.
The initial ECOG score was 0 or 1 for 72% of the patients, 2 for 25.6%, and 3 for 2.4%. After 8 wk the ECOG scores had not significantly changed, having improved by 1 point in 2 patients and worsened by 1 point in 4 patients. Among the patients who died during follow-up, the initial ECOG score was 1 or 2. Of those patients, 3 died at 4 wk after the therapy, 1 died at 5 wk, 1 at 10 wk, and 1 at 11 wk. All had extensive metastatic disease, including diffuse bone metastases, and a history of multimodal therapies. To our knowledge, there was no association between the 177Lu-PSMA-617 therapy and the death of these patients.
Response
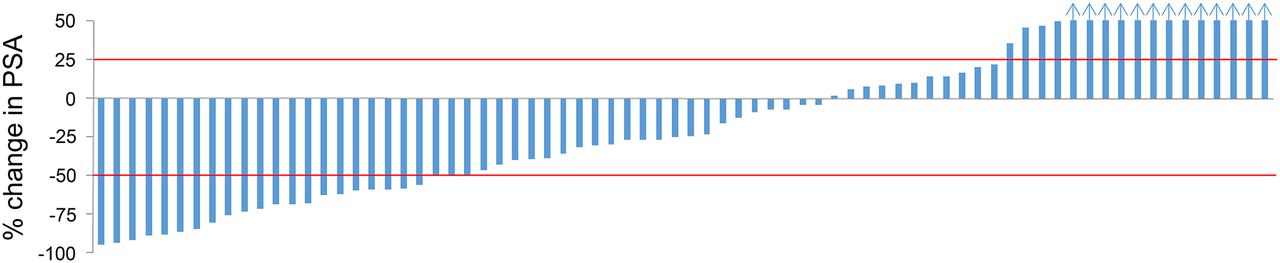
Forty-seven patients (64%) showed a decline in PSA; of these, 23 (31%) had a decline by more than 50%. Thirty-five patients (47%) had stable disease: the change in their PSA level ranged from less than a 50% decline to less than a 25% rise (Fig. 2). Progressive disease as indicated by more than a 25% rise in PSA occurred in 17 patients (23%). According to these results, 58 patients (78%) may have benefited from the 177Lu-PSMA-617 therapy. The median level of serum alkaline phosphatase showed a non–statistically significant decrease from 179 U/L (range, 38–1,607 U/L) to 159 U/L (range, 37–1,299 U/L).
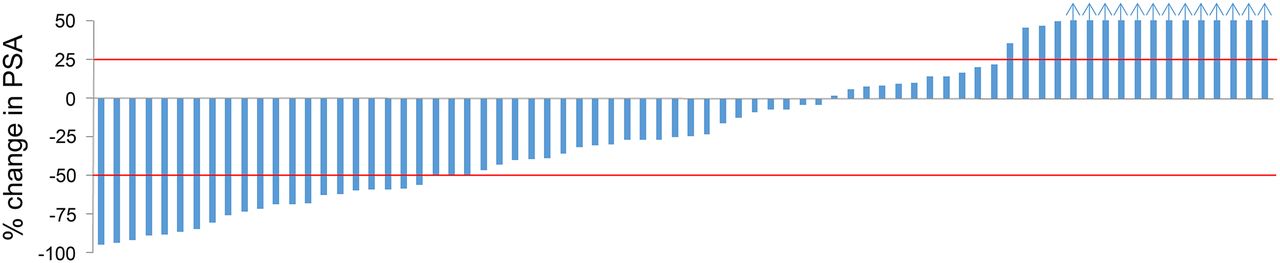
Waterfall curve showing percentage change in PSA values. In cases of PSA progression, maximum values ≥50% are scaled to 50%. Blue arrows represent patients with PSA increase ≥ 50%.
Toxicity
The toxicity results according to version 4.0 of the Common Toxicity Criteria for Adverse Events are given in Table 2. No serious adverse events occurred during therapy administration or hospitalization.
Adverse Events According to Common Toxicity Criteria for Adverse Events, Version 4.0
There were no significant changes in the median values for hemoglobin, white blood cells, creatinine, or liver parameters. At 8 wk, the platelet count had decreased significantly from baseline but was still within the reference range. Ten patients received a transfusion of erythrocyte concentrate before the therapy because of the extent of their skeletal metastases. Only 2 patients still needed an erythrocyte transfusion after the therapy.
The renal parameters did not change significantly: median creatinine decreased from 0.86 to 0.85 mg/dL, and median tubular extraction rate decreased from 218 to 214.
Xerostomia caused by previous chemotherapy was reported by 4 patients (4.8%) before the 177Lu-PSMA-617 therapy. After the therapy, a mild (grade I) xerostomia was reported by 7 patients, 3 of whom experienced it for only a short time. Permanent therapy-related xerostomia did not occur.
Diarrhea did not occur in any patient. Eight patients had nausea at baseline because of their prior therapies and general poor condition. Only 1 patient (1.4%) reported nausea at 8 wk after the therapy, and it was mild.
DISCUSSION
Targeted radioligand therapy is a favorable and elegant method of treating various kinds of tumors in a selective and individualized fashion that produces lower uptake in uninvolved tissue and thus fewer side effects. Glutamate carboxypeptidase II—now frequently called PSMA—is a membrane-bound metallopeptidase whose expression is highest in prostate cancer tissue (13). Therefore, PSMA is an ideal target for radioligand therapy.
In the present study, we evaluated the tolerability of and response to a single dose of 177Lu-PSMA-617 in a large cohort of patients in a multicenter setting.
In a phase II study that targeted the extracellular component of PSMA with a single dose of the 177Lu-labeled monoclonal antibody J591, Tagawa et al. (7) showed a PSA decline by 50% or more in 10.6% of patients and a PSA decline by any amount in 59.6% of patients. These results were in line with a prior phase I study by Bander et al. showing similar results with the same radioligand: a PSA decline by 50% or more in 11% of patients (14). By contrast, our study using a single 6-GBq dose of 177Lu PSMA-617 demonstrated a PSA decline by 50% or more in 31% of patients and a PSA decline by any amount in 64% of patients. According to our response criteria, 47% of the patients experienced stable disease and 78% of the patients may have benefited from the 177Lu-PSMA-617 therapy. Further studies evaluating response according to the Prostate Cancer Working Group 2 criteria (12) are needed to confirm these data.
In a first case series of 10 patients receiving a single dose of 177Lu-PSMA-617 (8), we demonstrated PSA declines by 50% or more and 30% or more in 50% and 70% of patients, respectively, as well as a low toxicity profile.
A study by Zechmann et al. using a 131I-labeled PSMA ligand showed a 50% or greater decline in PSA in more than 60% of patients (15).
More recently, Baum et al. (16) presented the results of a single-center study of 56 patients receiving a varying number of cycles (up to 5) of 177Lu-labeled PSMA imaging and therapy. A valuable response was found: a PSA decline by 50% or more in 58.9% of patients and progressive disease in 12.8% of patients. The authors presented only the results overall, not the results for the different numbers of cycles. In addition, the study was on an inhomogeneous group of patients, and the authors mention that their study was limited by the absence of pretherapeutic patient selection criteria. Our current study selected a homogeneous group of patients according to the criteria of having very advanced metastatic disease and either needing salvage therapy after previous treatment or being ineligible for the established mCRPC therapies.
All these publications showed respectable but variable response rates. The variation in response may have been due to the difference in β-energy between 131I and 177Lu or, especially, to differences in patient selection criteria such as extent of metastatic disease and prior treatments.
In a phase II therapy study using 177Lu-labeled monoclonal antibody J591, all patients developed reversible thrombocytopenia, and grade 4 thrombocytopenia occurred in 46.8% of the patients (7). In the present study, no grade 4 or 5 thrombocytopenia was observed, and grade 3 thrombocytopenia occurred in only one patient (Table 2). There were no changes in hematologic parameters indicative of toxicity, and although there was a mild but significant decline in the median platelet count, it was still within the reference range. Studies are needed to further evaluate these hematologic results for radioligand therapy.
The data on tolerability and hematologic toxicity presented here support the impression given by prior published data (8,15,16) by showing a low toxicity profile and high tolerability in patients with advanced metastatic disease.
The available dosimetry data for 177Lu-PSMA-617 therapy (17) indicate that uptake is highest in the salivary glands and kidneys but that the absorbed doses are not critical and therefore should not have much effect on function. Our study confirmed the results of prior studies (8,16) by showing no permanent xerostomia and no nephrotoxicity related to the therapy.
The major limitation of this study was its retrospective design. Further prospective randomized trials are needed to evaluate response in earlier stages of metastatic prostate cancer before this therapy can be considered as an addition to or replacement for approved therapies such as abiraterone or enzalutamide. In addition, future studies have to evaluate variables affecting or predicting response to 177Lu-PSMA-617.
CONCLUSION
This retrospective multicenter analysis suggested that radioligand therapy with 177Lu-PSMA-617 is safe and well tolerated and has a considerable effect on PSA level in patients with advanced mCRPC. Further studies are needed to evaluate response and toxicity after several therapy cycles and to determine the optimal number of cycles not only for salvage therapy but for use as an additional therapy in earlier stages of mCRPC.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the radiochemistry groups at all involved nuclear medicine departments for highly reliable production of 177Lu-PSMA-617 and 68Ga-PSMA-11.
Footnotes
Published online Apr. 7, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 7, 2016.
- Accepted for publication March 14, 2016.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development and Preclinical Evaluation of [211At]PSAt-3-Ga: An Inhibitor for Targeted {alpha}-Therapy of Prostate Cancer
- 177Lu-EB-PSMA Radioligand Therapy with Escalating Doses in Patients with Metastatic Castration-Resistant Prostate Cancer
- 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients with a Single Functioning Kidney
- Is the Vision of Radioligand Therapy for Prostate Cancer Becoming a Reality? An Overview of the Phase III VISION Trial and Its Importance for the Future of Theranostics
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- A Single Dose of 225Ac-RPS-074 Induces a Complete Tumor Response in an LNCaP Xenograft Model
- Repeated 177Lu-Labeled PSMA-617 Radioligand Therapy Using Treatment Activities of Up to 9.3 GBq
- Establishing 177Lu-PSMA-617 Radioligand Therapy in a Syngeneic Model of Murine Prostate Cancer
- Dual-Target Binding Ligands with Modulated Pharmacokinetics for Endoradiotherapy of Prostate Cancer
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- 177Lu-PSMA Radioligand Therapy for Prostate Cancer
- Why Targeting of PSMA Is a Valuable Addition to the Management of Castration-Resistant Prostate Cancer: The Urologists Point of View
- Preclinical Evaluation of 18F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- Predictors of Response to Radioligand Therapy of Metastatic Castrate-Resistant Prostate Cancer with 177Lu-PSMA-617
- From NETTER to PETTER: PSMA-Targeted Radioligand Therapy
- German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients