


Abstract
On the basis of the high and consistent expression of prostate-specific membrane antigen (PSMA) in metastatic prostate cancer (PC), the goal of this study was the development, preclinical evaluation, and first proof-of-concept investigation of a PSMA inhibitor for imaging and therapy (PSMA I&T) for 68Ga-based PET and 177Lu-based endoradiotherapeutic treatment in patients with metastatic and castration-resistant disease. Methods: PSMA I&T was synthesized in a combined solid phase and solution chemistry strategy. The PSMA affinity of natGa-/natLu-PSMA I&T was determined in a competitive binding assay using LNCaP cells. Internalization kinetics of 68Ga- and 177Lu-PSMA I&T were investigated using the same cell line, and biodistribution studies were performed in LNCaP tumor–bearing CD-1 nu/nu mice. Initial human PET imaging studies using 68Ga-PSMA I&T, as well as endoradiotherapeutic treatment of 2 patients with metastatic PC using 177Lu-PSMA I&T, were performed. Results: PSMA I&T and its cold gallium and lutetium analog revealed nanomolar affinity toward PSMA. The DOTAGA (1,4,7,10-tetraazacyclododecane-1-(glutamic acid)-4,7,10-triacetic acid) conjugate PSMA I&T allowed fast and high-yield labeling with 68GaIII and 177LuIII. Uptake of 68Ga-/177Lu-PSMA I&T in LNCaP tumor cells is highly efficient and PSMA-specific, as demonstrated by competition studies both in vitro and in vivo. Tumor targeting and tracer kinetics in vivo were fast, with the highest uptake in tumor xenografts and kidneys (both PSMA-specific). First-in-human 68Ga-PSMA I&T PET imaging allowed high-contrast detection of bone lesions, lymph node, and liver metastases. Endoradiotherapy with 177Lu-PSMA I&T in 2 patients was found to be effective and safe with no detectable side effects. Conclusion: 68Ga-PSMA I&T shows potential for high-contrast PET imaging of metastatic PC, whereas its 177Lu-labeled counterpart exhibits suitable targeting and retention characteristics for successful endoradiotherapeutic treatment. Prospective studies on larger cohorts of patients are warranted and planned.
Besides radiopharmaceuticals that address metabolic processes, approaches focusing on disease-specific targets (1,2) are increasingly important for cancer diagnosis and treatment with radiopharmaceuticals. On prostate cancer (PC) cells, the cell surface enzyme prostate-specific membrane antigen (PSMA), also known as glutamate carboxypeptidase II or N-acetyl-l-aspartyl-l-glutamate peptidase, is highly upregulated, whereas it shows low or no expression in the normal prostate (3). PSMA expression correlates with the malignancy of the disease, being further increased in metastatic and hormone-refractory patients (4). As a consequence, PSMA has attracted attention as a target for molecular imaging and for targeted radioligand therapy, especially in metastatic castrate-resistant prostate cancer (mCRPC).
For imaging of PC, a variety of selective small-molecule PSMA inhibitors, labeled with a broad range of radionuclides for PET and SPECT, have been evaluated preclinically in recent years (5–13). Among these, 18F-DCFBC (N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-18F-fluorobenzyl-l-cysteine) (7), 123I-MIP-1072 ((S)-2-(3-((S)-1-carboxy-5-(4-iodobenzylamino)pentyl)ureido)pentanedioic acid) and 123I-MIP-1095 ((S)-2-(3-((S)-1-carboxy-5-(3-(4-iodophenyl)ureido)pentyl)ureido)pentanedioic acid) (9), Glu-NH-CO-NH-Lys(Ahx)-68Ga-HBED-CC (68Ga-PSMA-HBED-CC) (11), and 99mTc-MIP-1404 ((7S,12S,16S)-1-(1-(2-(bis(carboxymethyl)amino)-2-oxoethyl)-1H-imidazol-2-yl)-2-((1-(2-(bis(carboxymethyl)amino)-2-oxoethyl)-1H-imidazol-2-yl)methyl)-9,14-dioxo-2,8,13,15-tetraazaoctadecane-7,12,16,18-tetracarboxylic acid (12) have already been successfully applied in first patient PET or SPECT studies (14–17). Despite certain differences between these ligands in overall pharmacokinetics, all these compounds allow sensitive detection of PC lesions, thus improving imaging and therapy planning.
As long as the disease is restricted to the prostate, surgery and radiation therapy exhibit high efficacy (18) in therapy of PC. Treatment options for PC patients with metastatic disease are androgen-deprivation therapy and chemotherapy (19). However, these therapies cause potentially serious adverse effects. The calcium mimetic α-emitter 223Ra-radium dichloride (Xofigo; Bayer AG) was recently approved. Xofigo is indicated in patients with mCRPC that has spread to bones (improved overall survival by 3.6 mo) (20). Thus, there is a major need for additional therapeutic options for patients with soft-tissue metastasizing disease.
111In-capromab pendetide (ProstaScint; Cytogen Corp.) is a Food and Drug Administration–approved murine monoclonal antibody for radioimmunoscintigraphy in PC patients (21), which is directed against the intracellular domain of PSMA. To increase uptake and sensitivity (22), antibodies against the extracellular domain, for example, J591, its humanized analog huJ591, and a minibody version of huJ591, have been developed. For radioimmunotherapy, J591 was labeled with β emitters (90Y, 177Lu) and evaluated in patients with mCRPC (23). Patient survival could be prolonged for 9.9 mo using 177Lu-J591 (24).
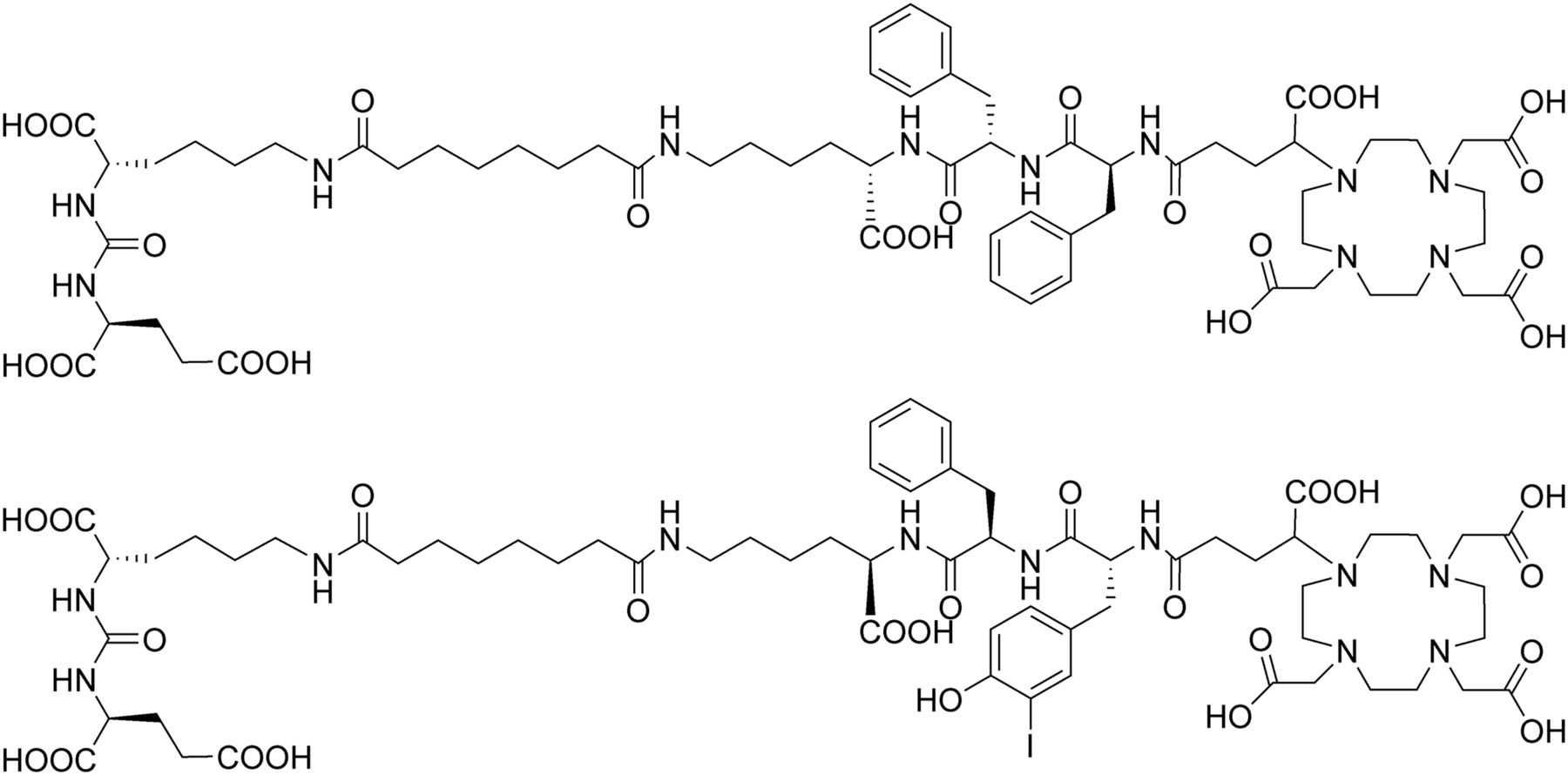
In a first step toward the development of small-molecule PSMA-targeting theranostics with fast pharmacokinetics and high PSMA affinity, we recently introduced (3S,7S)-29,32-dibenzyl-5,13,20,28,31,34-hexaoxo-37-(4,7,10-tris(carboxymethyl)-1,4,7,10-tetraazacyclododecan-1-yl)-4,6,12,21,27,30,33-heptaazaheptatriacontane-1,3,7,26,37-pentacarboxylic acid (DOTAGA-FFK(Sub-KuE) (13); Fig. 1; DOTAGA is 1,4,7,10-tetraazacyclododecane-1-(glutamic acid)-4,7,10-triacetic acid). In an initial study in patients with mCRPC (25,26), 177Lu-DOTAGA-FFK(Sub-KuE) administration led—in some patients—to a significant reduction in metastatic tumor load. In animal studies, higher metabolic stability and thus improved overall pharmacokinetics of PSMA inhibitors was achieved by substitution of the l-amino acid linker part (FFK) between the inhibitor and the chelator (13). Thus, the present study was focused on the further optimization of this second-generation theranostics tracer concept by exploiting the potential of the peptidic linker unit to enhance the PSMA affinity by increasing the lipophilic interaction of the tracer with the PSMA enzyme (8,27). To this aim, DOTAGA-(I-y)fk(Sub-KuE), termed PSMA I&T (for imaging and therapy; Fig. 1), was developed and evaluated in detail, both in vitro and in vivo. On the basis of the promising preclinical data obtained for 68Ga-/177Lu-PSMA I&T and to highlight the potential of 68Ga- and 177Lu-PSMA I&T, initial proof of concept in humans is described.

Chemical structures of DOTAGA-FFK(Sub-KuE), a first-generation tracer (upper), and PSMA I&T, a third-generation tracer (lower).
MATERIALS AND METHODS
General
All animal experiments were conducted in accordance with the German Animal Welfare Act (Deutsches Tierschutzgesetz, approval no. 55.2-1-54-2532-71-13). All human studies were approved by the institutional review boards of the participating medical institutions. Patients provided signed informed consent.
Synthesis and Radiolabeling
PSMA I&T and its gallium and lutetium complexes were synthesized according to a previously published protocol (13). The synthesis and a detailed description of the 68Ga- and 177Lu-labeling conditions are given in the supplemental data (supplemental materials are available at http://jnm.snmjournals.org). The radioiodinated reference ligand ((S)-1-carboxy-5-(4-(-125I-iodo-benzamido)pentyl)carbamoyl)-l-glutamic acid ([125I-BA]KuE) was prepared as described previously (13).
In Vitro Evaluation
The PSMA-positive LNCaP cells (300265; Cell Lines Service GmbH) were grown in Dulbecco modified Eagle medium/Nutrition Mixture F-12 with Glutamax-I (1:1) (Invitrogen) supplemented with 10% fetal calf serum. Cultures were maintained at 37°C in a humidified 5% CO2 atmosphere. One day before the experiment, cells were harvested using trypsin/ethylenediaminetetraacetate (0.05%/0.02%) in phosphate-buffered saline, centrifuged and resuspended in culture medium, counted, and seeded in 24-well plates.
Determination of PSMA Affinity
The determination of PSMA affinity (IC50) values was performed in a competitive binding assay using LNCaP cells (1.5 × 105 cells in 1 mL/well) and (125I-BA)KuE as radioligand as described previously (13). Quantification of the amount of free and bound activity was performed in a γ counter (Wallac 1480 WIZARD TM 3″; Perkin Elmer, Inc.). IC50 values were calculated using PRISM 6 software (GraphPad Software).
Cell Binding Kinetics
Cell binding and internalization kinetics were determined as reported (13). In brief, 1.25 × 105 LNCaP cells in poly-l-lysine–coated 24-well plates were incubated with radiolabeled PSMA I&T (0.2 nM for 68Ga- and 0.5 nM for 177Lu-labeled ligands) at 37°C for 5, 15, 30, and 60 min. The tracers were also incubated in the presence of 10 μM 2-(phosphonomethyl)pentane-1,5-dioic acid (PMPA) solution (blocking), and parallel experiments using the external reference ligand (125I-BA)KuE (0.2 nM) were performed. The amount of radioactivity in the supernatant, PSMA-specifically surface bound (incubation in 250 μL 10 μM PMPA for 10 min at 4°C), and in the cells (lysed with 250 μL 1 M NaOH) was quantified in a γ counter.
In Vivo Evaluation
Animal Model
To induce tumor growth, LNCaP cells (∼107 cells/200 μL) were suspended 1/1 in Dulbecco modified Eagle medium/Nutrition Mixture F-12 with Glutamax-I (1:1) and Matrigel (BD Biosciences) and were inoculated subcutaneously onto the right shoulder of CD-1 nu/nu mice (6–8 wk; Charles River Laboratories). After 2–4 wk (males) and 4–6 wk (females), respectively, tumors had reached 4–8 mm in diameter, and the animals were used for experiments.
Dual-Tracer Biodistribution Studies
Both 68Ga-PSMA I&T (4.7–6.3 MBq) and 177Lu-PSMA I&T (1.7–2.0 MBq) were coinjected into the tail vein of LNCaP tumor–bearing male mice under isoflurane anesthesia. The total injected peptide amount was kept constant at 0.2 nmol in all experiments. At 1 h after injection, the mice were sacrificed, the organs of interest were dissected, and the activity in weighed tissue samples was immediately quantified (68Ga). After the decay of 68Ga (next day), the quantification of 177Lu was performed in a γ counter.
Small-Animal PET Imaging
Imaging studies were performed on a Siemens Inveon small-animal PET scanner. For data analysis the Inveon Research Workplace software was used. Into the tail vein of female animals under isoflurane anesthesia, 14–18 MBq (0.2 nmol) of 68Ga-PSMA I&T were injected. Dynamic imaging was performed for 1.5 h after on-bed injection. Static images were recorded at 1 h after injection with an acquisition time of 15 min. Images were reconstructed using 3-dimensional ordered-subsets expectation maximum algorithm without scanner and attenuation correction.
Dosimetry Calculation
Female wild-type CD-1 mice were injected with 1.3–1.5 MBq of 177Lu-PSMA I&T (33.6–38.7 pmol) and sacrificed at 1, 6, 12, 24, 48, and 96 h after injection (n = 5, respectively). Organs of interest were dissected, and the activity in weighed tissue samples was quantified in a γ counter. Using the uptake data at different time points, we performed an extrapolation of the absorbed doses to humans. The dose extrapolation to humans involved the scaling of the time-integrated activity coefficients and the subsequent calculation of the absorbed doses from the animal biodistribution data using 2 different methods. Time-integrated activity coefficients were calculated using the software solution NUKFIT (28). The dose calculation was performed for a selected group of organs using OLINDA/EXM (version 1.1) (29). Details on the methodology used for extrapolating the mouse data to humans are provided in the supplemental data.
68Ga-PSMA I&T PET Imaging in Patients
The patient underwent PET/CT imaging (Biograph mCT PET/CT; Siemens Medical Solution AG) 60 min after intravenous administration of 133.2 MBq of 68Ga-PSMA I&T. CT and reconstruction details are given in the supplemental materials. Circular regions of interest were drawn around areas with increased uptake in transaxial slices for calculation of the maximum standardized uptake value (SUVmax). Regions of interest were automatically adapted to a 3-dimensional volume of interest with Syngovia (Siemens Medical Solutions) at a 40% isocontour.
Patient 1, 70 y of age, was diagnosed with PC in 2011, with an initial Gleason score of 10 (5 + 5). The patient had initially undergone palliative transurethral resection of the prostate, followed by androgen-deprivation therapy using abiraterone acetate. Further treatment with docetaxel plus prednisolone was initiated after development of mCRPC, with multiple bone metastases displayed by bone scan. The serum total prostate-specific antigen (PSA) level at the time of imaging was 10.1 ng/mL.
Endoradiotherapy of Patients Using 177Lu-PSMA I&T
Two patients with mCRPC were assessed before the 177Lu-PSMA I&T therapy by 68Ga-PSMA-HBED-CC PET/CT imaging (Biograph mCT Flow 64; Siemens Medical Solutions AG). Contrast-enhanced PET/CT was performed 1–5 d before endoradiotherapy and for follow-up at 65 ± 4 min after intravenous administration of 170 ± 23 MBq of 68Ga-PSMA-HBED-CC. Both patients with progressive mCRPC underwent therapy with 5.7 and 8.0 GBq of 177Lu-PSMA I&T, respectively, administered intravenously over 15 min. Complete blood counts, parameters of renal function (serum creatinine, blood urea nitrogen), and liver function (albumin, bilirubin, enzymes), as well as tubular extraction rate measured by 99mTc-mercaptoacetyltriglycine scintigraphy, were documented before and after therapy. Response to therapy was assessed by 68Ga-PSMA-HBED-CC PET combined with contrast-enhanced CT 8–10 wk after therapy. In addition, biochemical response was documented by means of PSA monitoring.
Patient 2 was a 68-y-old man with progressive metastatic prostatic adenocarcinoma (Gleason score 7) and multiple mediastinal lymph node metastases. The 54-y-old patient 3, with adenocarcinoma-of-the-prostate (Gleason score 9: 4 + 5) status after hormonal therapy and external-beam radiation therapy, presented with progressive mediastinal and retroperitoneal lymph node metastases and multifocal osseous lesions.
RESULTS
Synthesis and Radiolabeling
PSMA I&T was synthesized in accordance with the protocol described for DOTAGA-ffk(Sub-KuE) (13) and obtained in 32.4% yield (based on DOTAGA-(I-y)fk) and greater than 99% purity (220 nm).
For cell studies, manual 68Ga labeling of PSMA I&T (3 nmol) resulted in a specific activity of 250–300 GBq/μmol, whereas for animal studies fully automated 68Ga labeling (5 nmol) yielded 68Ga-PSMA I&T in specific activities of 80–120 GBq/μmol. For quantitative 177Lu complexation, 24.5 MBq of 177LuIII was reacted with a 4.5-fold molar excess of PSMA I&T, yielding 177Lu-PSMA I&T in specific activities of 27 GBq/μmol or more.
Tracers for patient application were prepared using a fully automated synthesis module and obtained in radiochemical yields of 67% ± 10% (non–decay-corrected) and radiochemical purities of 98% ± 2% (instant thin-layer chromatography silica gel; Varian). Calculated specific activities were 40.0 MBq/μg (37.8 GBq/μmol) for 68Ga-PSMA-HBED-CC and 13.6 MBq/μg (20.4 GBq/μmol) for 68Ga-PSMA I&T. For 177Lu-PSMA I&T, the radiochemical purity was 99.0% ± 1.0% as determined by reversed-phase high-performance liquid chromatography (LiChroCART 250-4, Lichrospher100, RP18; Merck), and specific activities of 40.0 MBq/μg (59.9 GBq/μmol) were achieved.
PSMA Binding Affinity
The affinity (IC50) of PSMA I&T and its natGa and natLu complexes toward PSMA (Table 1) was determined in a competitive binding assay using the human prostate carcinoma cell line LNCaP (1.5 × 105 cells/well, 1 h) at 4°C and (125I-BA)KuE (0.2 nM) as the radioligand.
IC50 Values Determined in Competitive Binding Assay
Compared with the second-generation DOTAGA-functionalized PSMA ligands (13), PSMA I&T contains a d-Phe-by-3-iodo-d-Tyr substitution in the peptidic linker unit (Fig. 1). To be able to assess the influence of this modification on PSMA affinity, data for DOTAGA-ffk(Sub-KuE) (13) are also included in Table 1. Metal complexation has only negligible effect on PSMA affinity of PSMA I&T. However, substitution of d-Phe by d-3-iodo-Tyr in the linker does have beneficiary influence in significantly improving PSMA affinity of the PSMA I&T constructs as compared with the second-generation DOTAGA analogs.
Internalization Kinetics
To investigate the impact of the increased affinity of 68Ga-/177Lu-PSMA I&T on ligand internalization and cell binding, LNCaP cells (1.25 × 105 cells/well) were incubated with the respective radioligands at 37°C for different time points up to 1 h. Experiments were performed in the absence (total binding) and presence of 10 μM PMPA (nonspecific binding), and a PMPA wash step (10 μM, 10 min, 4°C) was included to differentiate between specifically bound and internalized activity. To exclude an influence of interexperimental variations in cell count or cell viability on the absolute amount of bound/internalized tracer, the standard ligand (125I-BA)KuE was always assayed in parallel as an external reference, and its cellular uptake in the respective experiments was used for data normalization.
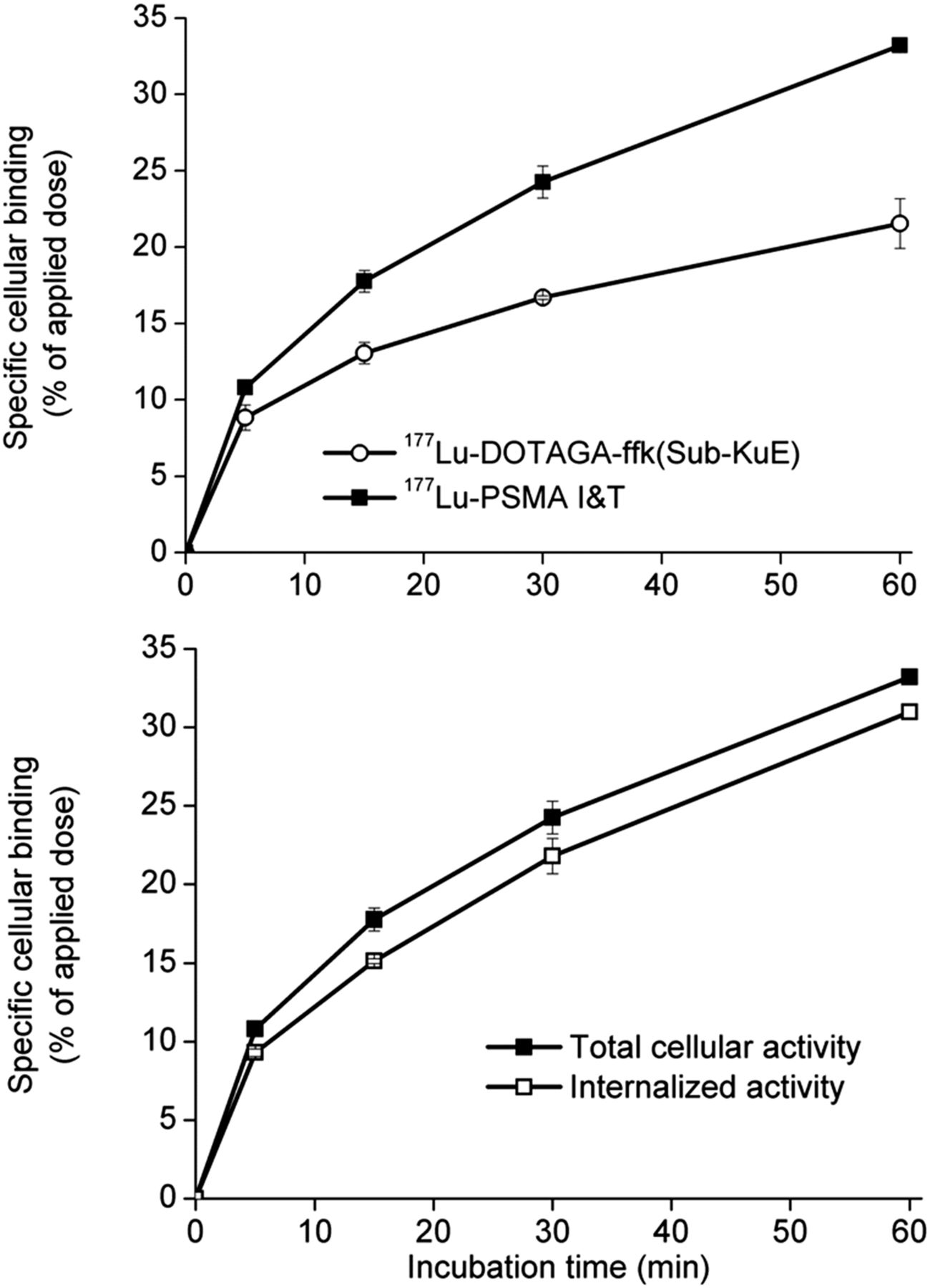
The upper portion of Figure 2 shows the ligand binding kinetics of 177Lu-PSMA I&T in comparison to 177Lu-DOTAGA-ffk(Sub-KuE). The internalization of all 68Ga- and 177Lu-labeled PSMA inhibitors investigated in this study was high and nearly identical. At all time points, 1%–3% of the total activity was bound to PSMA on the cell membrane (Fig. 2 [lower]), and less than 0.5% was nonspecifically bound. Although 177Lu-DOTAGA-ffk(Sub-KuE) showed only 44% ± 2% of the cellular uptake of the reference compound (125I-BA)KuE in a parallel experiment, internalization of 177Lu-PSMA I&T was increased to 76% ± 2% of that of (125I-BA)KuE. The same trend was observed for the respective 68Ga-labeled analogs, for which the transition from 68Ga-DOTAGA-ffk(Sub-KuE) to 68Ga-PSMA I&T led to an increase in internalization from 42% ± 2% to 59% ± 2% of (125I-BA)KuE internalization.

Specific binding kinetics of 177Lu-PSMA I&T and 177Lu-DOTAGA-ffk(Sub-KuE) (upper) and specific binding and internalization kinetics of 177Lu-PSMA I&T at 37°C to LNCaP cells (lower). All data are expressed as mean ± SD.
Dual-Tracer Biodistribution Study
The biodistribution of 68Ga-PSMA I&T (0.1 nmol) and 177Lu-PSMA I&T (0.1 nmol) investigated in a dual-tracer experiment at 1 h after injection in LNCaP tumor–bearing CD-1 nu/nu mice is summarized in Table 2. Given their nearly identical physicochemical properties, both 68Ga- and 177Lu-PSMA I&T showed fast and rapid clearance from the circulation and virtually no background accumulation at 1 h after injection (Table 2). Interestingly, the increased PSMA-mediated internalization of 177Lu-PSMA I&T, compared with its 68Ga analog, was well reflected by an enhanced uptake in the PSMA-positive tissues—that is, lung, spleen, and a significantly (P < 0.05) higher kidney and tumor uptake. Therefore, tumor-to-background ratios for 177Lu-PSMA I&T are increased for almost all organs (Fig. 3).
Dual-Tracer Biodistribution (%ID/g) in LNCaP Tumor–Bearing CD-1 nu/nu Mice at 1 Hour After Injection (n = 4)

Tumor-to-organ ratios of dual-tracer biodistribution of 68Ga- and 177Lu-PSMA I&T at 1 h after injection in LNCaP tumor–bearing CD-1 nu/nu mice (n = 4). T/ = tumor-to-.
Small-Animal PET Imaging
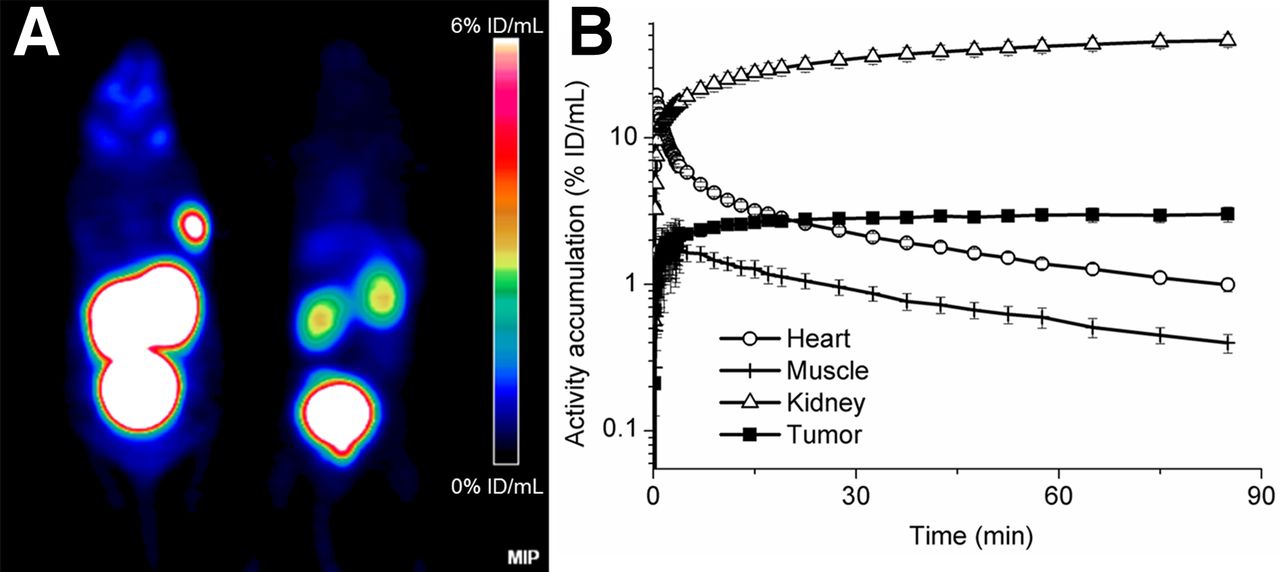
As shown on the PET images of LNCaP tumor–bearing CD-1 nu/nu mice at 1 h after injection, 68Ga-PSMA I&T primarily accumulates in the tumor xenograft and the kidneys, which were shown to be PSMA-specific (Fig. 4A). Fast renal excretion was confirmed by significant bladder activity. The time–activity curves (Fig. 4B) derived from dynamic PET data revealed fast uptake kinetics and retention of the tracer in kidney and tumor over the 1.5-h observation period, whereas the activity was rapidly washed out from nontarget tissues and compartments such as blood (region of interest over the heart) and muscle (linear decline in a logarithmic plot).

PET of LNCaP tumor–bearing CD-1 nu/nu mice. (A) Maximum-intensity projections (MIP) of static PET scans using 15.8 MBq of 68Ga-PSMA I&T (left) or 14.3 MBq of 68Ga-PSMA I&T coinjected with PMPA (8 mg/kg) (right). (B) Time–activity curves (logarithmic plot) for 68Ga-PSMA I&T (15.4 MBq) derived from dynamic small-animal PET data. ID = injected dose.
Dosimetry of 177Lu-PSMA I&T in Mice
Absorbed doses for 177Lu-PSMA I&T in humans were extrapolated from mouse biodistribution data using 2 alternative extrapolation methods (method 1 [M1] and method 2 [M2]). Details on the methodology, a list of the time-integrated activity coefficients for several organs of relevance for dosimetry (residence times), a full list of the corresponding absorbed doses, and information on the absorbed dose by β particles and photons are given in the supplemental data. The highest time-integrated activity coefficient was observed for the kidneys (M1, 8.3 h; M2, 5.8 h). For all organs, the total absorbed doses are summarized in Table 3 and were lower than 5.9 × 10−2 mGy/MBq (adrenals M1), except kidneys (2.4 mGy/MBq [M1] or 1.6 mGy/MBq [M2]). Unless more than 9.6 GBq (M1) or 14.4 GBq (M2) are administered to humans, the limiting kidney dose of 23 Gy could be exceeded.
Total Absorbed Doses in Different Organs (mGy/MBq) after Application of 177Lu-PSMA I&T, Calculated by Both Methods
In addition, the effective dose per unit activity in kidneys was calculated. However, the quantity effective dose can be applied only to the description of stochastic radiation effects and organ-absorbed doses of less than 1 Gy. The extrapolated effective doses were 9.6 × 10−3 mSv/MBq (M1) and 7.4 × 10−3 mSv/MBq (M2), which corresponded to effective doses of 1.9 mSv (M1) and 1.5 mSv (M2) for an administered activity of 200 MBq.
68Ga-PSMA I&T PET Imaging in First Patient
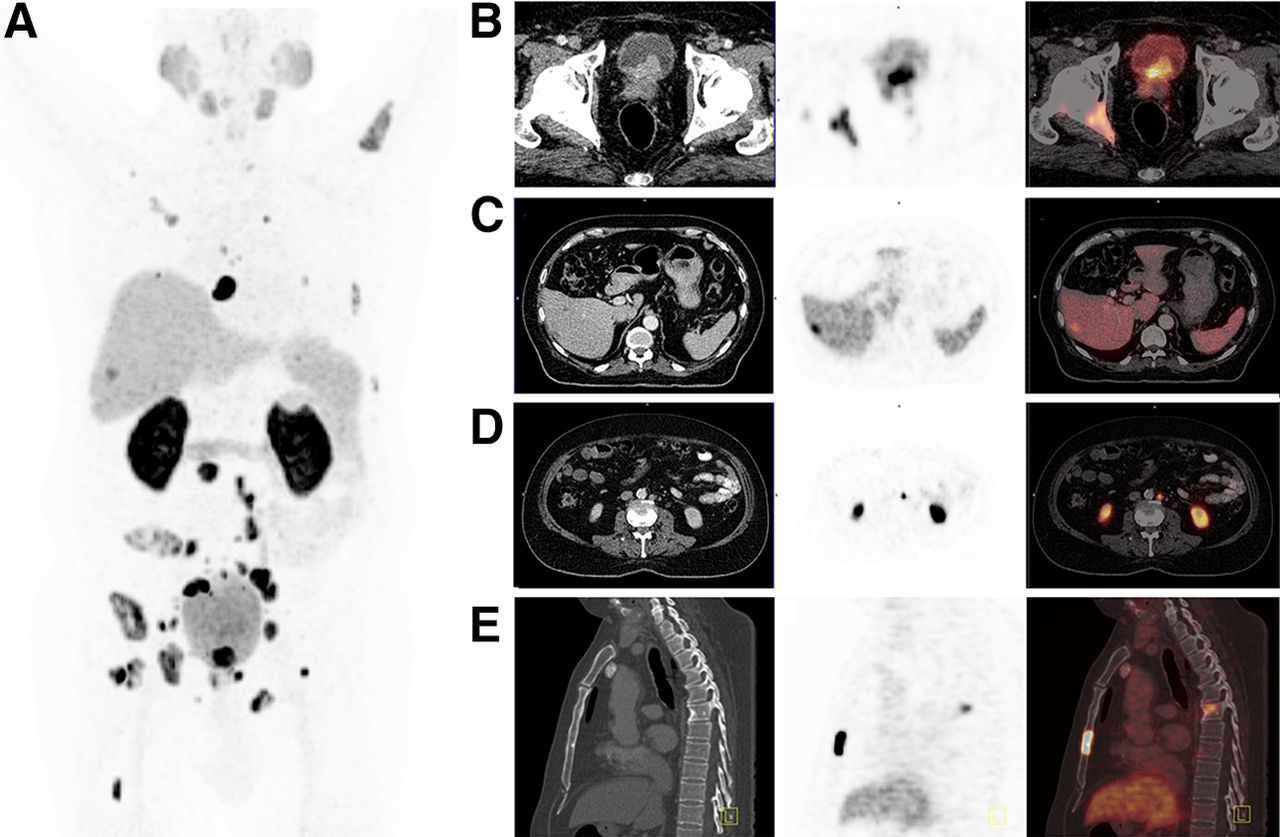
In a first patient with CRPC with multiple metastases 68Ga-PSMA I&T PET/CT revealed multiple bone, abdominal lymph node, and a liver metastasis (Fig. 5A). The primary prostate tumor (SUVmax, 65.1; Fig. 5B), as well as periprostatic tissue and urinary bladder invasion, was not concealed by radioactivity in the bladder. A 7-mm left perirectal lymph node showed an SUVmax of 15. The liver lesion (Fig. 5C), which was not known before PET scanning, showed an SUVmax of 10.9 and 2 cm in diameter. Further, a sclerosis in a sternal lesion, which had been barely visible in the CT image, exhibited a high 68Ga-PSMA I&T uptake (SUVmax,76.4; Fig. 5E). Multiple paraaortic and pelvic lymph nodes showed high contrast in 68Ga-PSMA I&T PET, as shown for an 8-mm paraaortic lymph node with an SUVmax of 39.4 in Figure 5D. Mean SUVmax of lymph node metastases was 26.4 (range, 7–80.4) and of bone metastases 52.8 (range, 22–76.5). The average 68Ga-PSMA I&T lesion-to-background ratio was 17.6 for lymph node metastases, 35.2 for bone metastases, and 20.7 for the liver metastasis. Background activity was determined in gluteal musculature (SUVmax, 1.5).

68Ga-PSMA I&T PET/CT of patient 1. (A) Whole-body maximum-intensity projection showing 1 liver lesion and multiple lymph node and bone metastases. (B) Transaxial slices show infiltration of soft-tissue mass with increased tracer uptake in urinary bladder and periprostatic tissue. (C) Transaxial slices revealing 68Ga-PSMA I&T uptake in right lobe of liver with hypodense lesion in corresponding CT slice. (D) Transaxial slices presenting small paraaortic lymph node with intense PSMA expression indicative of lymph node metastasis. (E) Sagittal reformatted CT reveals only minimal sclerosis of sternal bone metastasis with high 68Ga-PSMA I&T uptake. All slices are shown on CT (left), PET (middle), and fused PET/CT (right).
Besides the pathologic tracer accumulation, 68Ga-PSMA I&T showed a high uptake in the kidneys and salivary glands and low uptake in the liver, spleen, and proximal segments of the small intestine.
177Lu-PSMA I&T Therapy in Patients
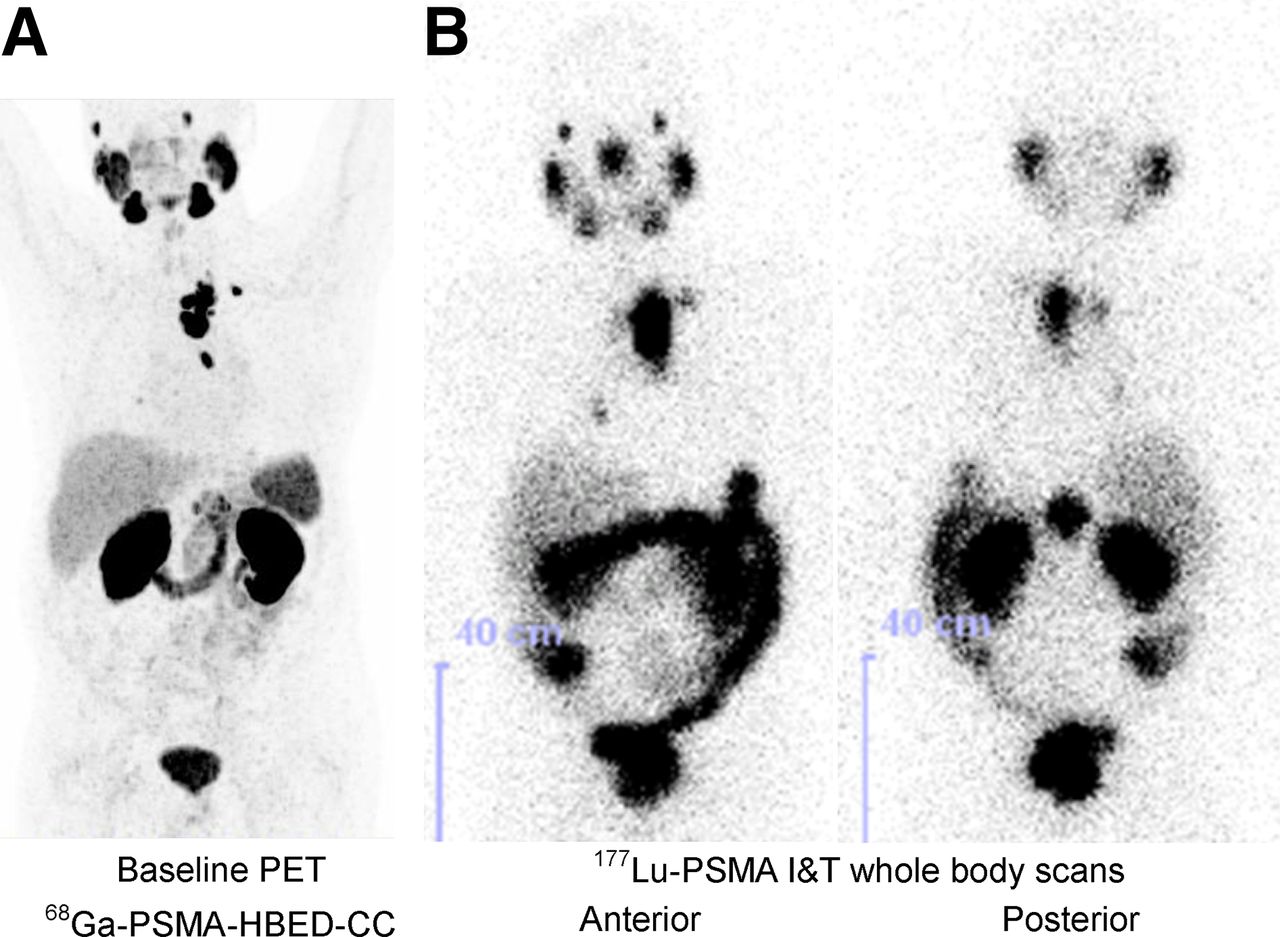
Two patients with mCRPC and multiple metastases in bone and lymph nodes, which had been confirmed by baseline 68Ga-PSMA-HBED-CC PET/CT, were treated with 177Lu-PSMA I&T. Therapy control was performed using 68Ga-PSMA-HBED-CC PET/CT to ensure comparability to data from the literature and an objective interpretation of the therapy outcome. The administered mass of PSMA I&T was 142 and 200 μg, and the administered activity was 5.7 and 8.0 GBq, respectively. In patient 2 (PSA, 54.2 ng/mL), the mediastinal lymph node metastases (SUVmax, 36.5, determined by 68Ga-PSMA-HBED-CC PET/CT) exhibited a high uptake of 177Lu-PSMA I&T (Fig. 6) on posttherapy planar and SPECT/CT images. Therapy was well tolerated, and no significant fall in blood counts, renal function (serum creatinine, tubular extraction rate), or any of the laboratory parameters was found. There was no adverse or clinically detectable pharmacologic effect. During early follow-up, no side effects were observed, particularly no dry mouth caused by activity in salivary glands.
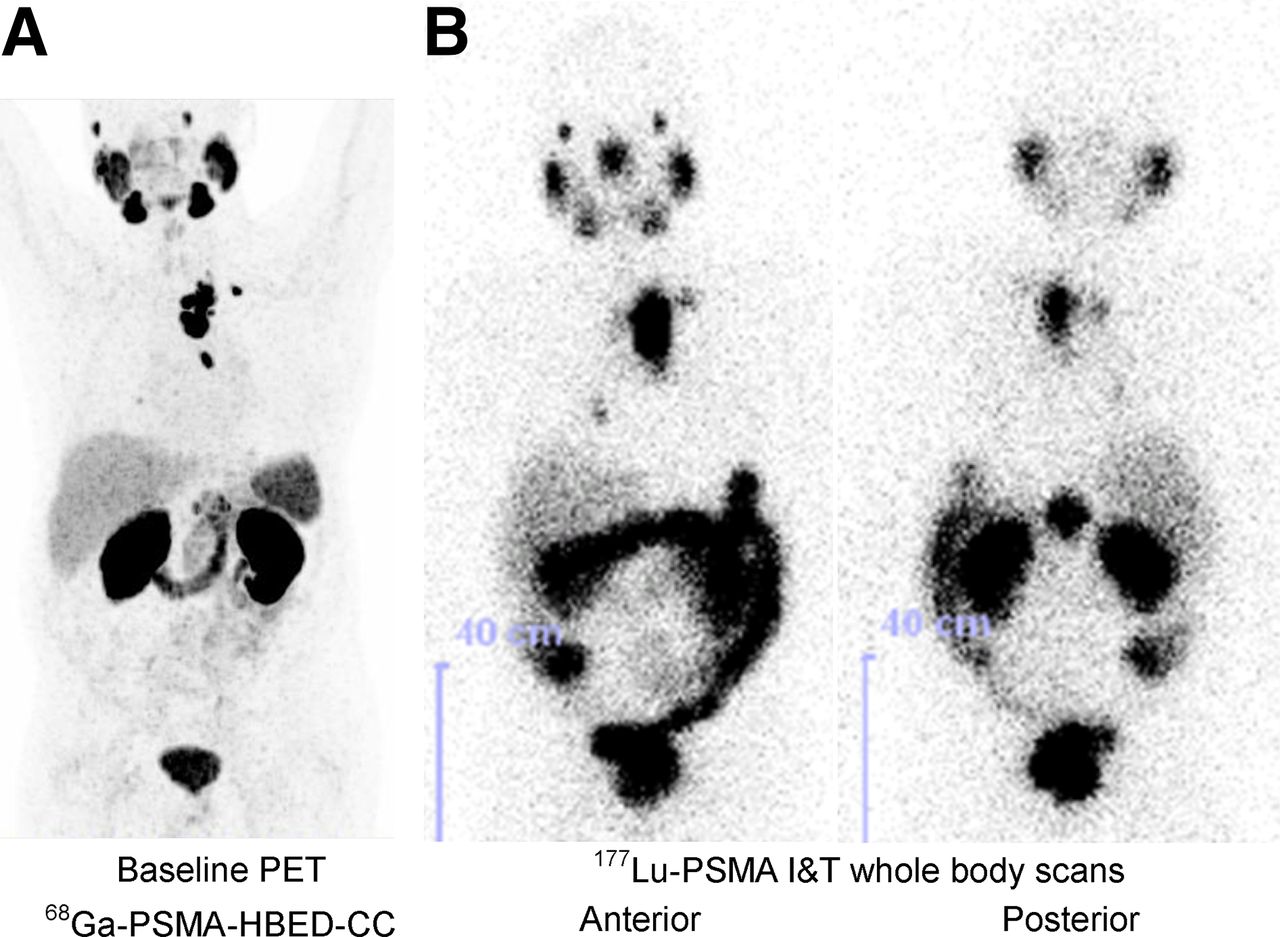
Patient 2. (A) Maximum-intensity projection of 68Ga-PSMA-HBED-CC PET/CT (164 MBq, 60 min after injection, left) showed intense tracer accumulation in mediastinal lymph node metastases. (B) Correspondingly, these mediastinal lymph nodes demonstrated high 177Lu-PSMA I&T uptake 47 h after therapy with 5.7 GBq of 177Lu-PSMA I&T.
The baseline 68Ga-PSMA-HBED-CC PET/CT scan in patient 3 (PSA, 40.2 ng/mL) demonstrated PSMA-mediated uptake in the primary tumor and multiple lymph node and bone metastases (Fig. 7A). The SUVmax of target lesions was 26.3 in the right paraaortic lymph node (transverse PET/CT image in Fig. 7A, upper), 25.2 in interaortocaval lymph node (Fig. 7A, middle), and 16.4 in the primary tumor in the prostate (Fig. 7A, lower). The patient underwent 1 therapy cycle with 8.0 GBq of 177Lu-PSMA I&T. Follow-up 68Ga-PSMA-HBED-CC PET/CT (Fig. 7B) 3 mo after 177Lu-PSMA I&T therapy revealed partial remission of many of the intense PSMA-positive metastases depicted by 68Ga-PSMA-HBED-CC PET/CT (SUVmax, 3.0, 3.5, and 5.1 in paraaortic, interaortocaval lymph node metastasis, and primary tumor, respectively) accompanied by a significant drop in the PSA to 0.7 ng/mL. Clinically, a symptomatic pain relief, especially on the left side of the chest, was reported.
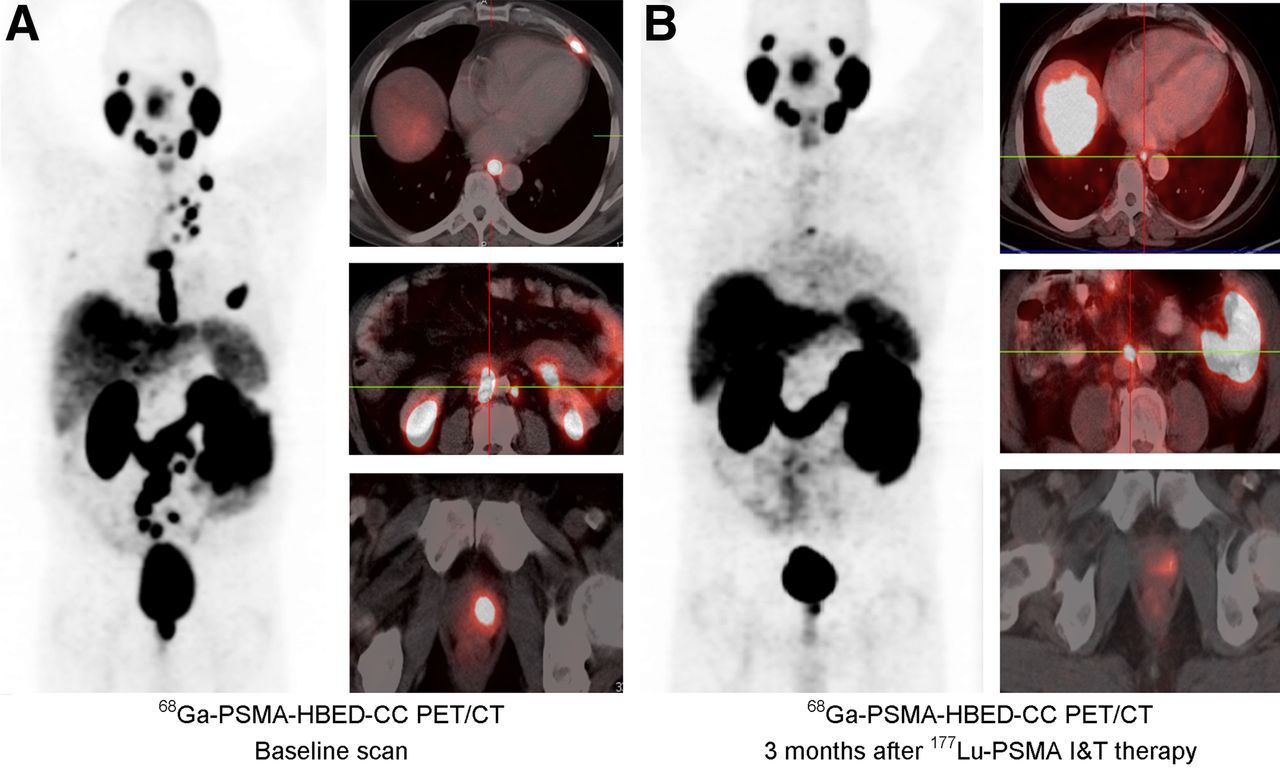
PET/CT in patient 3. (A) Baseline PET/CT 65 min after intravenous administration of 176 MBq of 68Ga-PSMA-HBED-CC. (B) Follow-up scan with 180 MBq of 68Ga-PSMA-HBED-CC (60 min after injection) performed 3 mo after 177Lu-PSMA I&T therapy (8.0 GBq).
DISCUSSION
In comparison to 18F-fluoromethylcholine, the urea-based PSMA inhibitor 68Ga-PSMA-HBED-CC (30) displays significantly improved diagnostic sensitivity and specificity. To meet the urgent need for a targeted therapeutic agent in the treatment of PC, first promising (urea-based) candidates for endoradiotherapy of PC have also been introduced and evaluated in first patient studies (25,26,31).
On the basis of the valuable results of this tracer class both in diagnostic imaging and in endoradiotherapy, the aim of this study was the development of a suitable PSMA-targeted theranostic concept, combining straightforward labeling procedures for clinical routine application with optimized PSMA-targeting characteristics. Previous studies leading to a first-generation theranostic agent (Fig. 1) have already demonstrated the beneficial effect of DOTAGA-for-DOTA substitution and of using an all-d-amino acid peptide linker on PSMA affinity and metabolic stability and thus uptake and clearance kinetics, respectively (13). Complementing these findings with the substitution of 1 of the d-phenylalanine residues in the peptidic linker by 3-iodo-d-tyrosine for an improved interaction of the tracer molecule with a remote binding site (27) led to PSMA I&T (Fig. 1). As anticipated, this modification resulted in an increased PSMA affinity of PSMA I&T and its natGa and natLu complexes, compared with their ffk analogs (Table 1), which is also reflected by an enhanced internalization efficiency of 68Ga-/177Lu-PSMA I&T into PSMA-expressing LNCaP cells. Interestingly, although the PSMA affinity of natLu-PSMA I&T is only marginally increased, compared with natGa-PSMA I&T, internalization of 177Lu-PSMA I&T into LNCaP cells is significantly enhanced. This improved targeting efficiency is reflected by an increased uptake of 177Lu-PSMA I&T in the LNCaP tumor xenografts and thus enhanced tumor-to-background ratios (Fig. 3). It also shows a nearly 2-fold-higher accumulation in lung, spleen, and kidney, all of which are tissues with documented PSMA expression (32). Compared with other promising PSMA-directed tracers, 68Ga- and 177Lu-PSMA I&T both show a tissue distribution pattern comparable to that of 68Ga-PSMA-HBED-CC (11,13) at the same time point. Although both compounds show enhanced blood activity levels and liver accumulation, compared with 99mTc-MIP-1404 (12), the extent of PSMA-unspecific activity retention in the blood and liver was significantly lower than 18F-DCFBC (7). This difference in retention is most probably the result of the excellent metabolic stability and comparably low plasma protein binding of 68Ga-/177Lu-PSMA I&T.
First clinical application of 68Ga-PSMA I&T in PET/CT successfully demonstrated multiple metastatic foci in different organs and tissues with high lesion-to-background ratios of 17.6–35.2 as early as 1 h after injection. Even very small (millimeter range) abdominal lymph node and small bone metastases showed high uptake and were easily detectable (Fig. 5). Comparable to previously reported data for 68Ga-PSMA-HBED-CC in PET/CT (14), low physiologic tracer uptake was observed in the liver (33), spleen (33), and intestine (3) and—to a higher extent—in the proximal tubules of the kidneys (3) and salivary glands (34), all of which are organs with documented moderate to high PSMA expression. However, the reasons for the observed high tracer uptake into salivary glands is still a matter of debate, because the PSMA expression level would suggest lower uptake.
Because there is presently no standardized way for extrapolating time-integrated activity coefficients from animal data to humans, we decided to apply 2 methods originally described by Sparks and Aydogan (35). Choosing 2 different ways of scaling provides an estimate of the extrapolation-related uncertainty in calculating absorbed doses to humans, as can be seen in Table 3. Overall, the agreement between the absorbed doses to the organs is acceptable. For most organs, the difference is less than ±45%. Major deviations caused by the different ways of extrapolating are for the intestines, pancreas, and uterus. If, for therapeutic applications, organs at risk need to be considered for a first-in-human study, one would apply the higher of both values as a conservative estimate of the organ-absorbed doses.
The extrapolated organ dosimetry for 177Lu-PSMA I&T shows that the highest absorbed dose per unit activity is expected in the kidneys. The values are about 1.1- to 1.7-fold higher than the corresponding values reported for 131I-MIP-1095 with 1.5 mGy/MBq (31) and for 177Lu-J591 with 1.4 mGy/MBq (23). For 90Y-J591 (23), a value of 4.5 mGy/MBq is reported, which is about 2 times higher than the extrapolated values for 177Lu-PSMA I&T. In addition, the calculated absorbed doses per unit activity for other organs (e.g., liver, spleen, heart wall, bone marrow) for 131I-MIP-1095 (31) and 177Lu-J591 (23) are at least 1 order of magnitude higher than the corresponding values for 177Lu-PSMA I&T. Of course the present extrapolated data need to be confirmed in a dosimetry study in patients, including an assessment of the absorbed doses to tumor lesions in patients.
As its 68Ga analog, 177Lu-PSMA I&T shows high, specific and rapid uptake in all previously identified tumor lesions of the mCRPC patients included in this proof-of-concept study (Fig. 6). As expected, significant tracer uptake is also observed for the kidney, spleen, and salivary glands but also in the small intestine. This finding is consistent with the PSMA expression levels documented for these tissues (3,33,34); for example, 177Lu-PSMA I&T uptake in the small intestine most likely is the result of PSMA expression in human intestine (3), in which the physiologic function of PSMA is mediating folate absorption (36). On the basis of the high PSMA expression in the metastases of mCRPC (37) and the resulting high uptake of 177Lu-PSMA I&T in these lesions, therapeutically effective doses were delivered to the PC metastases resulting in impressive molecular treatment response. Besides concomitant subjective reduction of pain, both patients demonstrated objective clinical measures of improvement, such as a drop of PSA and reduction of disease burden as determined by 68Ga-PSMA-HBED-CC PET/CT (Fig. 7).
Because of the rapid renal washout and blood clearance of 177Lu-PSMA I&T, no side effects either in salivary glands or in kidneys or blood parameters were observed in either of the 2 treated patients, and treatment was well tolerated. In contrast, after endoradiotherapy with 131I-MIP-1095 (31) dry mouth and 1 case of mucositis were reported due to high salivary gland retention of the therapeutic agent. Thus, high contrast in PET imaging and therapeutic effectiveness with no detectable side effects qualifies 68Ga-/177Lu-PSMA I&T to be a valid choice for the theranostic management of PC.
CONCLUSION
68Ga-PSMA I&T is a PET tracer of high potential for the detection of metastatic PC and may be useful for stratification and follow-up of patients undergoing radioligand therapy with 177Lu-PSMA I&T (theranostics). In a proof-of-concept study 177Lu-PSMA I&T endoradiotherapy was feasible, safe, and effective in metastatic PC. Subsequent studies have to assess the optimal activity as well as the amount of peptide administered, potential kidney or salivary gland protection, and the need of repeated therapeutic interventions based on patient follow-up.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The research leading to these results has received funding from the Deutsche Forschungsgemeinschaft (DFG) under grant agreement no. SFB 824 project Z1. Jakub Simecek is an employee and Hans-Jürgen Wester is CEO of SCINTOMICS GmbH, Fuerstenfeldbruck, Germany. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Frauke Hoffmann and Simon Schmied for experimental assistance and Sybille Reder, Markus Mittelhäuser, and Marco Lehmann for small-animal PET imaging.
Footnotes
Published online Jun. 18, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 31, 2015.
- Accepted for publication June 2, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Evaluation of 177Lu-rhPSMA-10.1, a Radiopharmaceutical for Prostate Cancer: Biodistribution and Therapeutic Efficacy
- Albumin-Binding and Conventional PSMA Ligands in Combination with 161Tb: Biodistribution, Dosimetry, and Preclinical Therapy
- A Single-Arm, Low-Dose, Prospective Study of 177Lu-EB-PSMA Radioligand Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer
- 177Lu-PSMA-I&T for Treatment of Metastatic Castration-Resistant Prostate Cancer: Prognostic Value of Scintigraphic and Clinical Biomarkers
- Synthesis and Preclinical Evaluation of 177Lu-Labeled Radiohybrid PSMA Ligands for Endoradiotherapy of Prostate Cancer
- 177Lu-PSMA Therapy
- Prostate-Specific Membrane Antigen Radioligand Therapy Using 177Lu-PSMA I&T and 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: Comparison of Safety, Biodistribution, and Dosimetry
- Effects of 225Ac-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer: A Meta-Analysis
- First In Vivo and Phantom Imaging of Cyclotron-Produced 133La as a Theranostic Radionuclide for 225Ac and 135La
- The History of Prostate-Specific Membrane Antigen as a Theranostic Target in Prostate Cancer: The Cornerstone Role of the Prostate Cancer Foundation
- Bringing VISION to Nuclear Medicine: Accelerating Evidence and Changing Paradigms with Theranostics
- Reply: PSMA-Targeted Therapeutics: A Tale About Law and Economics
- PSMA-Targeted Therapeutics: A Tale About Law and Economics
- Synthesis and Preclinical Evaluation of a 68Ga-Labeled Adnectin, 68Ga-BMS-986192, as a PET Agent for Imaging PD-L1 Expression
- Comparative Preclinical Biodistribution, Dosimetry, and Endoradiotherapy in Metastatic Castration-Resistant Prostate Cancer Using 19F/177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T
- Dynamic 68Ga-PSMA-11 PET/CT for the Primary Evaluation of Localized Renal Mass: A Prospective Study
- Therapeutic Efficacy of a Bivalent Inhibitor of Prostate-Specific Membrane Antigen Labeled with 67Cu
- First Clinical Results for PSMA-Targeted {alpha}-Therapy Using 225Ac-PSMA-I&T in Advanced-mCRPC Patients
- Evaluation of an Automated Module Synthesis and a Sterile Cold Kit-Based Preparation of 68Ga-PSMA-11 in Patients with Prostate Cancer
- Radiohybrid Ligands: A Novel Tracer Concept Exemplified by 18F- or 68Ga-Labeled rhPSMA Inhibitors
- Prostate-Specific Membrane Antigen-Guided Surgery
- Development of Novel PSMA Ligands for Imaging and Therapy with Copper Isotopes
- 89Zr-Immuno-PET: Toward a Noninvasive Clinical Tool to Measure Target Engagement of Therapeutic Antibodies In Vivo
- 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients with a Single Functioning Kidney
- One-Step 18F-Labeling and Preclinical Evaluation of Prostate-Specific Membrane Antigen Trifluoroborate Probes for Cancer Imaging
- Clinical Outcomes of 177Lu-PSMA Radioligand Therapy in Earlier and Later Phases of Metastatic Castration-Resistant Prostate Cancer Grouped by Previous Taxane Chemotherapy
- Synthesis and Preclinical Characterization of the PSMA-Targeted Hybrid Tracer PSMA-I&F for Nuclear and Fluorescence Imaging of Prostate Cancer
- The Relevance of Dosimetry in Precision Medicine
- Molecular Imaging of Prostate Cancer: Choosing the Right Agent
- Low-Level Endogenous PSMA Expression in Nonprostatic Tumor Xenografts Is Sufficient for In Vivo Tumor Targeting and Imaging
- Initial Experience with Volumetric 68Ga-PSMA I&T PET/CT for Assessment of Whole-Body Tumor Burden as a Quantitative Imaging Biomarker in Patients with Prostate Cancer
- PSMA Ligands for PET Imaging of Prostate Cancer
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- Glu-Ureido-Based Inhibitors of Prostate-Specific Membrane Antigen: Lessons Learned During the Development of a Novel Class of Low-Molecular-Weight Theranostic Radiotracers
- 177Lu-PSMA Radioligand Therapy for Prostate Cancer
- 68Ga-PSMA Ligand PET/CT-based Radiotherapy for Lymph Node Relapse of Prostate Cancer After Primary Therapy Delays Initiation of Systemic Therapy
- Preclinical Evaluation of 18F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging
- Preclinical Evaluation and First Patient Application of 99mTc-PSMA-I&S for SPECT Imaging and Radioguided Surgery in Prostate Cancer
- Molecular Imaging and Therapy with a Purpose: A Renaissance of Nuclear Medicine
- 68Ga-PSMA PET/CT Detects the Location and Extent of Primary Prostate Cancer
- Evaluation of 68Ga-Glutamate Carboxypeptidase II Ligand Positron Emission Tomography for Clinical Molecular Imaging of Atherosclerotic Plaque Neovascularization
- (2S)-2-(3-(1-Carboxy-5-(4-211At-Astatobenzamido)Pentyl)Ureido)-Pentanedioic Acid for PSMA-Targeted {alpha}-Particle Radiopharmaceutical Therapy
- PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013
- Prostate-Specific Membrane Antigen-Targeted Radiohalogenated PET and Therapeutic Agents for Prostate Cancer
- 177Lu-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy of Metastatic Castration-Resistant Prostate Cancer: Safety and Efficacy
- Perspective on 177Lu-PSMA Therapy for Metastatic Castration-Resistant Prostate Cancer
- Pilot Comparison of 68Ga-RM2 PET and 68Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer