


Article Figures & Data
Figures
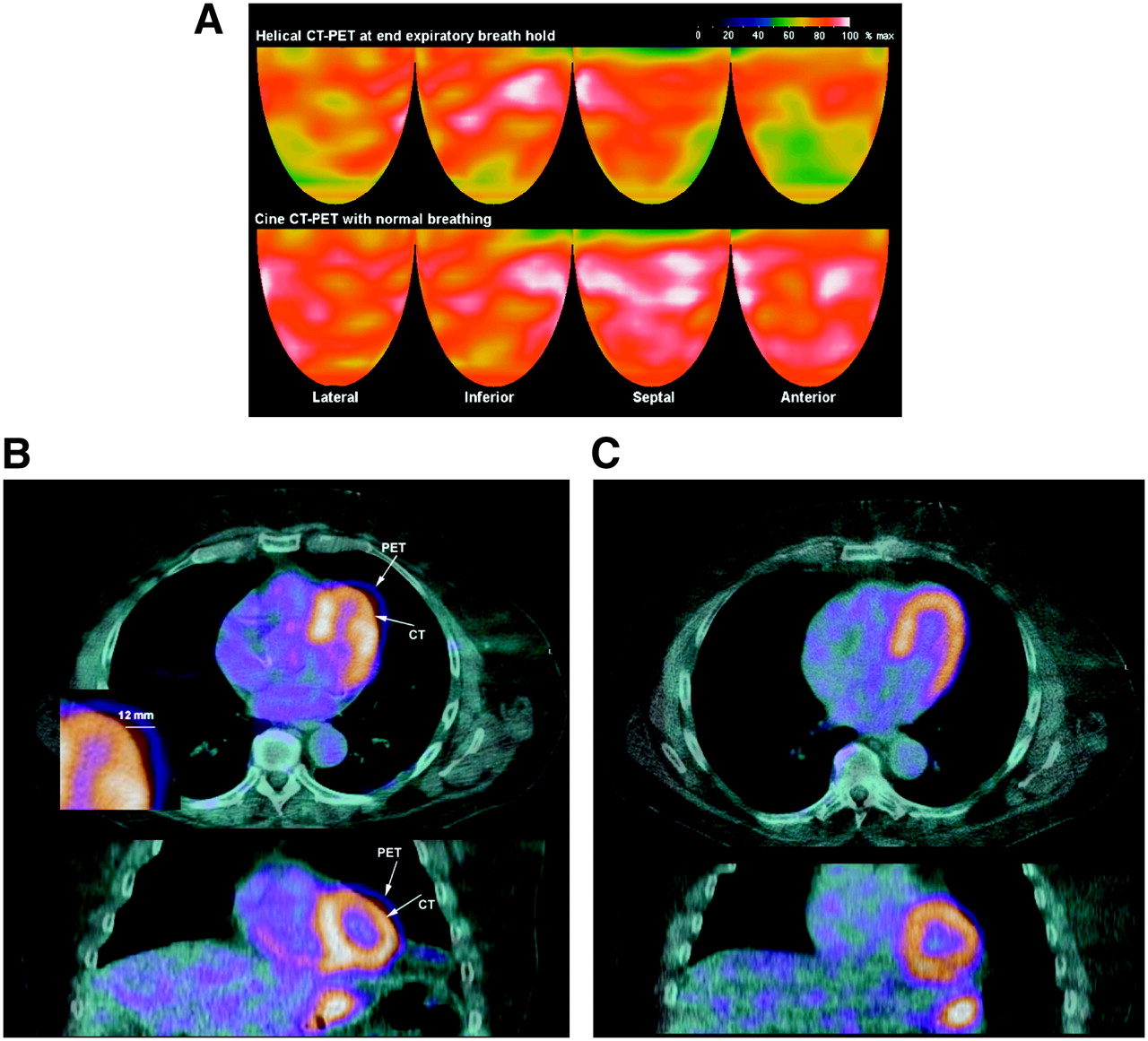
- FIGURE 1.
(A) Topographic 3D displays of helical CT PET with a mild-to-moderate anterior and lateral defect (top row) that is not present on cine CT PET (bottom row). White indicates the highest myocardial uptake of 82Rb, reflecting the highest myocardial perfusion, with red being the next highest and progressively lower perfusion indicated by color gradations from red to yellow, green, and blue. (B) For same patient as in A, misregistration on helical CT-PET fusion images in transaxial (top) and coronal (bottom) views. Arrows indicate heart borders on helical CT and PET emission images as unmatched, with region of misregistration corresponding to area of artifactual defect. Magnified inset illustrates quantification of misregistration in transaxial view—here, 12 mm—using an electronic caliper on the screen. (C) For same patient, cine CT-PET fusion images show good coregistration associated with no defect and a normal scan.
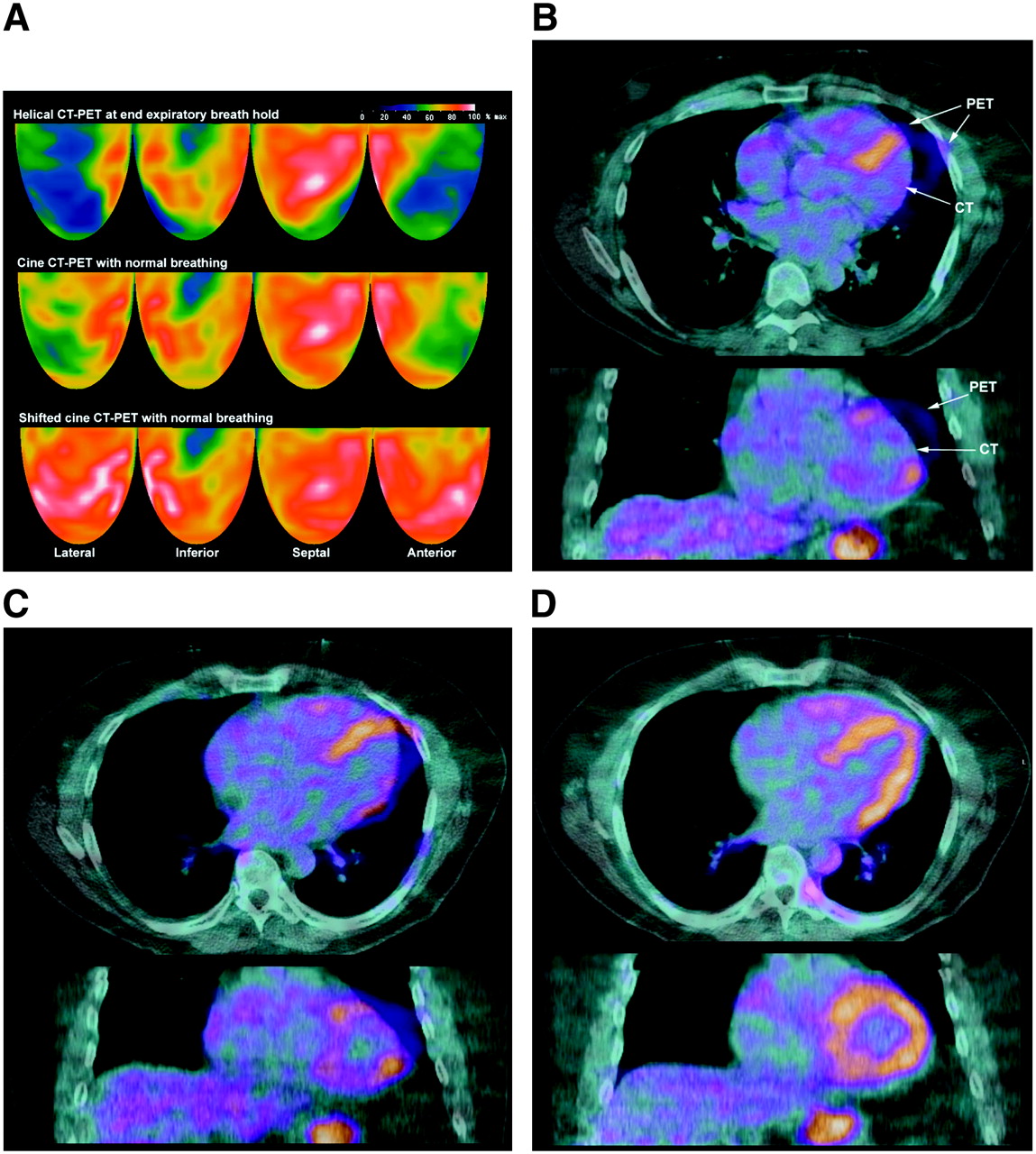
- FIGURE 2.
(A) Topographic 3D displays of helical CT PET with severe anterior, apical, lateral, and basal inferior defects (top row) that are also present but less severe on cine CT PET (middle row). Anterior, apical, and lateral defects normalize on shifted cine CT PET (bottom row). (B) For same patient as in A, helical CT-PET fusion images in transaxial (top) and coronal (bottom) views show marked misregistration. Arrows indicate heart borders on helical CT and PET emission images as unmatched, with region of misregistration corresponding to area of artifactual defect. (C) For same patient, cine CT-PET fusion images also show misregistration. (D) For same patient, shifted cine CT-PET fusion images with no misregistration associated with disappearance of artifactual anterior, apical, and lateral artifactual defects.
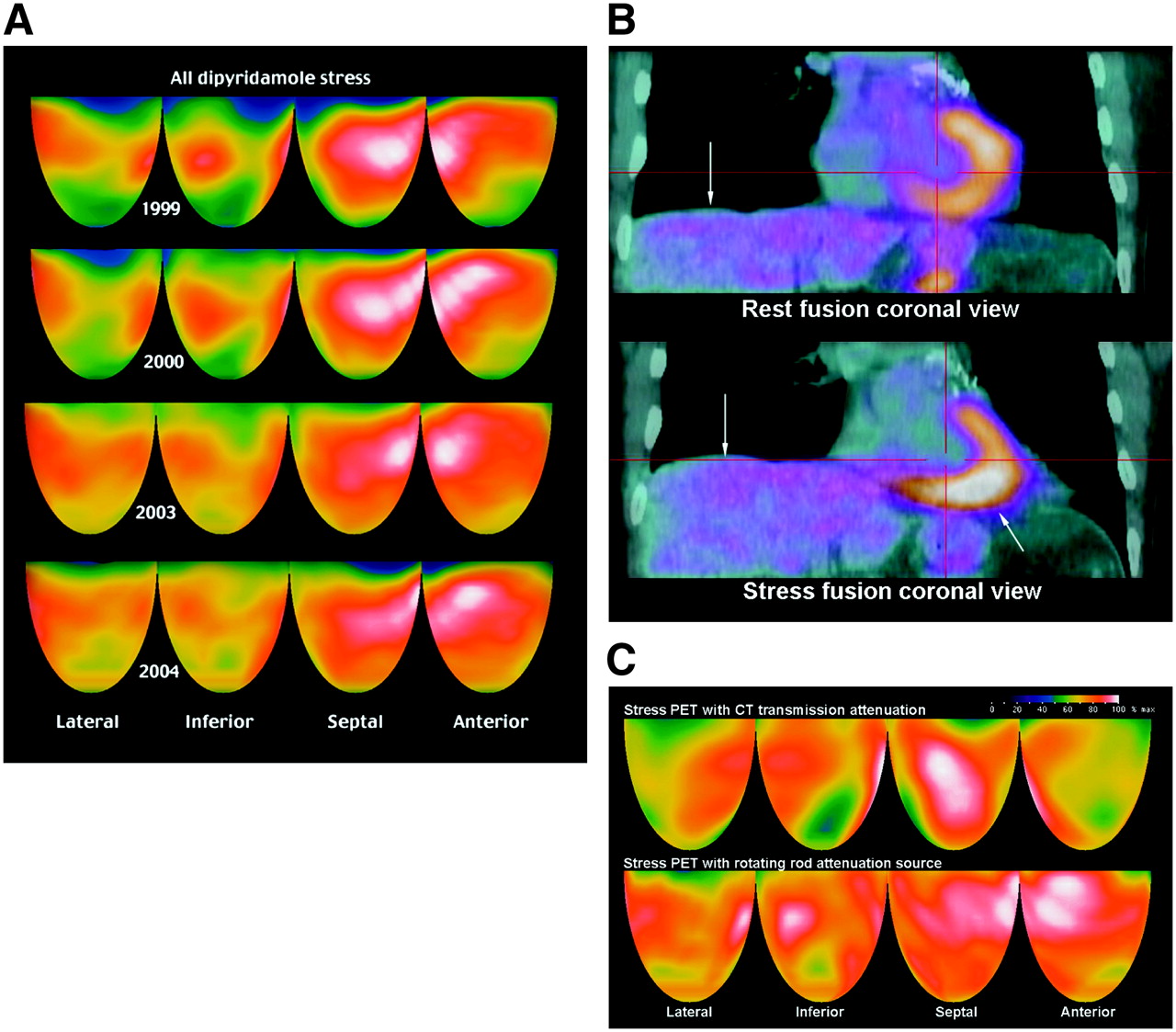
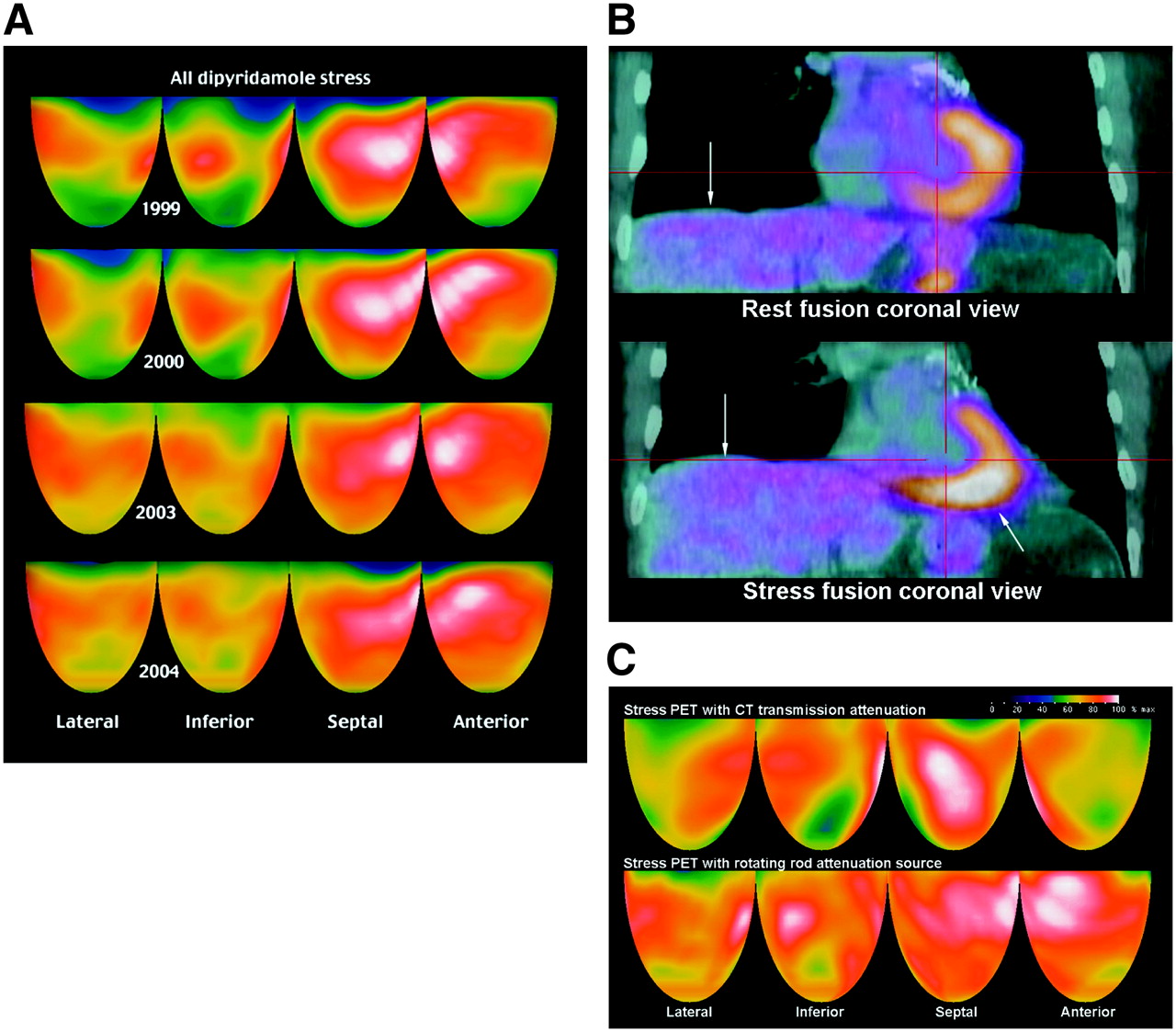
- FIGURE 3.
(A) Stress perfusion images at yearly intervals using a Positron PET scanner with rotating rod transmission source show progressive improvement on a strict lifestyle and medical regimen. (B) For same patient as in A, rest and stress helical CT-PET fusion images at follow-up in 2006 were acquired during normal breathing before cine CT was available. Diaphragm–heart mismatch (arrows) on stress fusion image caused attenuation overcorrection inferiorly and associated relative anterior defect on stress PET despite borders of heart being properly coregistered on both rest and stress perfusion images (see text). (C) For same patient, follow-up stress perfusion helical CT PET images in 2006. Diaphragm–heart mismatch on stress fusion image shown in B caused artifactual anterior, lateral, and inferoapical defects (top row) that disappeared on repeated stress scan using Positron PET scanner with a rotating rod attenuation transmission source (bottom row) and correct coregistration.
- FIGURE 4.
(A) Resting CT transmission image acquired over 29 s with normal breathing shows “motion layering” of CT scan (top row). Helical CT-PET fusion image demonstrates a corresponding notching of attenuation (arrows) and notched undercorrection of PET data. (B) For same patient as in A, corresponding rest–stress 3D topographic display has linear anterior and lateral artifacts (arrows) on rest emission scan caused by motion layering on resting CT scan, not present on stress scan. Mild inferior defect is not associated with any misregistration but is due to diffuse atherosclerosis of posterior descending coronary artery.


Tables
Transaxial misregistration (mm) Artifactual PET defects due to misregistration None Mild Moderate Severe Total ≤6 148 4 2 0 154 >6–10 7 22 19 2 50 >10 1 18 29 7 55 Total 156 44 50 9 259 χ2 P = 0.0000.
PET/CT (n = 122) Severity Size–severity % ≤ 2.0 SD % ≤ 2.5 SD Transaxial misregistration (mm) n NA 79.6 ± 3.1 0.1 ± 0.2 2.5 ± 3.1 0.8 ± 1.1 2.4 ± 2.4 19 Artifacts 73.9 ± 6.4 6.2 ± 14.6 8.6 ± 4.9 6.1 ± 4.9 11.7 ± 5.0 103 P for Δ 0.0000 0.0000 0.0000 0.0000 0.0000 Mild artifact 75.9 ± 3.9 1.8 ± 3.6 6.8 ± 3.9 3.9 ± 3.5 10.2 ± 3.8 44 P for Δ vs. NA 0.0003 0.0024 0.0000 0.0000 0.0000 Moderate artifact 74.2 ± 5.3 3.8 ± 5.3 9.3 ± 5.0 6.8 ± 4.7 12.1 ± 5.0 50 P for Δ vs. NA 0.0000 0.0000 0.0000 0.0000 0.0000 Severe artifact 62.9 ± 10.3 41.07 ± 31.1 13.9 ± 3.8 12.3 ± 4.8 16.5 ± 7.3 9 P for Δ vs. NA 0.0011 0.0043 0.0000 0.0001 0.0003 No or mild artifact 77.0 ± 4.1 1.3 ± 3.1 5.5 ± 4.2 2.9 ± 3.3 7.9 ± 4.9 63 Moderate or severe artifact 72.4 ± 7.4 9.5 ± 18.4 10.0 ± 5.1 7.7 ± 5.1 12.8 ± 5.6 59 P for Δ vs. no or mild 0.0001 0.0013 0.0000 0.0000 0.0000 NA = no artifacts.
All patients with perfusion defects outside 2 SD from healthy subjects on final stress PET/CT images, considered to be “real” defects, were excluded from quantitative analysis of misregistration artifacts in this table.
PET/CT scan Severity (% of maximum) Size–severity (% <60% maximum) % of LV <2.0 SD % LV <2.5 SD Transaxial misregistration (mm) Mean Δ cine vs. helical (mm) Diaphragm mm to CT 0 Mean Δ mm diaphragm All helical CT PET 74.2 ± 7.3 8.5 ± 17.5 8.2 ± 5.8 6.1 ± 5.6 8.34 ± 6.51 4.4 5.2 ± 15.8 3.3 All cine CT PET 77.6 ± 6.2 4.5 ± 11.6 5.1 ± 5.1 3.5 ± 4.7 3.93 ± 3.50 2.0 ± 15.4 n = 114, P for Δ 0.0000 0.0024 0.0000 0.0000 0.0000 0.0002 Helical CT PET with artifacts 73.7 ± 7.3 7.5 ± 17.6 8.7 ± 5.4 6.3 ± 5.3 11.87 ± 5.89 7.2 5.3 ± 16.9 2.6 Cine CT PET same patients 79.2 ± 5.0 1.2 ± 3.3 3.9 ± 3.8 2.2 ± 3.0 4.69 ± 3.67 2.7 ± 16.2 n = 67, P for Δ 0.0000 0.0038 0.0000 0.0000 0.0000 0.0334 LV = left ventricle.
Quantitative measurements of defects are for quadrant containing misregistration artifactual defect or for worst quadrant in absence of misregistration artifact.
- TABLE 4
Patients with Cine CT PET Having Worse Misregistration Artifactual Defects than with Helical CT PET Corrected by Shifting Cine CT Data
Cine CT PET worse than helical CT (8 patients) Severity (minimum quadrant average) Size–severity (% <60% maximum) Size (% ≤2.5 SD) Transaxial misregistration (mm) Helical CT PET 74.79 ± 3.60 1.72 ± 2.58 5.26 ± 4.49 8.39 ± 3.00 Cine CT PET 71.28 ± 5.45 9.64 ± 10.27 10.08 ± 5.57 12.44 ± 5.51 n = 8, P for Δ 0.0216 0.0284 0.0018 0.0751 Cine CT PET 70.29 ± 5.07 11.01 ± 10.27 10.88 ± 5.49 12.24 ± 5.93 Shifted cine CT PET 75.98 ± 6.10 4.05 ± 6.60 4.98 ± 5.77 2.71 ± 3.39 n = 7*, P for Δ 0.0043 0.0639 0.0047 0.0008 ↵* Quantitative shifted cine CT data were lost for 1 patient due to corruption of the header but with good saved images.
- TABLE 5
Patients with Slow Helical CT over 29 Seconds During Breathing Compared with Patients with Fast 4-Second Helical CT at End-Expiratory Breath-Holding
Comparison No artifacts Artifacts Total % artifacts Slow helical CT with breathing 106 39 145 27 Fast helical CT at end expiration 50 64 114 56 Total 156 103 259 40 χ2 P = 0.001.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Value of SiPM PET in myocardial perfusion imaging using Rubidium-82
- PET by MRI: Glucose Imaging by 13C-MRS without Dynamic Nuclear Polarization by Noise Suppression through Tensor Decomposition Rank Reduction
- Improving the Accuracy of Simultaneously Reconstructed Activity and Attenuation Maps Using Deep Learning
- Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC
- Routine Clinical Quantitative Rest Stress Myocardial Perfusion for Managing Coronary Artery Disease: Clinical Relevance of Test-Retest Variability
- Myocardial Blood Flow and Inflammatory Cardiac Sarcoidosis
- The Effect of Misregistration Between CT-Attenuation and PET-Emission Images in 13N-Ammonia Myocardial PET/CT
- Clinical Utility of Enhanced Relative Activity Recovery on Systolic Myocardial Perfusion SPECT: Lessons from PET
- Regadenoson Versus Dipyridamole Hyperemia for Cardiac PET Imaging
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Cardiac PET/CT Misregistration Causes Significant Changes in Estimated Myocardial Blood Flow
- Effective Dose of PET/CT in Informed Consent Forms
- Physiological Basis for Angina and ST-Segment Change: PET-Verified Thresholds of Quantitative Stress Myocardial Perfusion and Coronary Flow Reserve
- Impact of Unexpected Factors on Quantitative Myocardial Perfusion and Coronary Flow Reserve in Young, Asymptomatic Volunteers
- Cardiac Dedicated Ultrafast SPECT Cameras: New Designs and Clinical Implications
- Coronary Branch Steal: Experimental Validation and Clinical Implications of Interacting Stenosis in Branching Coronary Arteries
- Characterization of a Perirectal Artifact in 18F-FDG PET/CT
- Single-Phase CT Aligned to Gated PET for Respiratory Motion Correction in Cardiac PET/CT
- Decreased Perfusion in the Lateral Wall of the Left Ventricle in PET/CT Studies with 13N-Ammonia: Evaluation in Healthy Adults
- Nonrigid Versus Rigid Registration of Thoracic 18F-FDG PET and CT in Patients with Lung Cancer: An Intraindividual Comparison of Different Breathing Maneuvers
- Integrated positron emission tomography/computed tomography (PET/CT) in coronary disease
- Directions and Magnitudes of Misregistration of CT Attenuation-Corrected Myocardial Perfusion Studies: Incidence, Impact on Image Quality, and Guidance for Reregistration
- Does Coronary Flow Trump Coronary Anatomy?
- Cardiac Positron Emission Tomography
- Coronary Flow Reserve and Pharmacologic Stress Perfusion Imaging: Beginnings and Evolution
- Comparison of Myocardial Perfusion 82Rb PET Performed with CT- and Transmission CT-Based Attenuation Correction
- SPECT/CT
- Dual-Modality Imaging: Combining Anatomy and Function
- Reducing Radiation Dose in Rest-Stress Cardiac PET/CT by Single Poststress Cine CT for Attenuation Correction: Quantitative Validation
- Not All Randomized Trials Are Equal
- Reply: Attenuation Correction for Stress and Rest PET 82Rb Myocardial Perfusion Images
- Attenuation Correction for Stress and Rest PET 82Rb Myocardial Perfusion Images