


Abstract
Vascular endothelial growth factor (VEGF), released by tumor cells, is an important growth factor in tumor angiogenesis. The humanized monoclonal antibody bevacizumab blocks VEGF-induced tumor angiogenesis by binding, thereby neutralizing VEGF. Our aim was to develop radiolabeled bevacizumab for noninvasive in vivo VEGF visualization and quantification with the single γ-emitting isotope 111In and the PET isotope 89Zr. Methods: Labeling, stability, and binding studies were performed. Nude mice with a human SKOV-3 ovarian tumor xenograft were injected with 89Zr-bevacizumab, 111In-bevacizumab, or human 89Zr-IgG. Human 89Zr-IgG served as an aspecific control antibody. Small-animal PET and microCT studies were obtained at 24, 72, and 168 h after injection of 89Zr-bevacizumab and 89Zr-IgG (3.5 ± 0.5 MBq, 100 ± 6 μg, 0.2 mL [mean ± SD]). Small-animal PET and microCT images were fused to calculate tumor uptake and compared with ex vivo biodistribution at 168 h after injection. 89Zr- and 111In-bevacizumab ex vivo biodistribution was compared at 24, 72, and 168 h after injection (2.0 ± 0.5 MBq each, 100 ± 4 μg in total, 0.2 mL). Results: Labeling efficiencies, radiochemical purity, stability, and binding properties were optimal for the radioimmunoconjugates. Small-animal PET showed uptake in well-perfused organs at 24 h and clear tumor localization from 72 h onward. Tumor uptake determined by quantification of small-animal PET images was higher for 89Zr-bevacizumab—namely, 7.38 ± 2.06 %ID/g compared with 3.39 ± 1.16 %ID/g (percentage injected dose per gram) for human 89Zr-IgG (P = 0.011) at 168 h and equivalent to ex vivo biodistribution studies. Tracer uptake in other organs was seen primarily in liver and spleen. 89Zr- and 111In-bevacizumab biodistribution was comparable. Conclusion: Radiolabeled bevacizumab showed higher uptake compared with radiolabeled human IgG in a human SKOV-3 ovarian tumor xenograft. Noninvasive quantitative small-animal PET was similar to invasive ex vivo biodistribution. Radiolabeled bevacizumab is a new tracer for noninvasive in vivo imaging of VEGF in the tumor microenvironment.
Several factors are involved in the development and growth of tumors. Angiogenesis, the forming of new blood vessels, is one of these factors. New vasculature allows tumor cells to execute their critical growth by supplying the tumor with nutrients and oxygen, enabling disposal of metabolic waste products and providing a route for metastatic spreading (1,2). An important factor involved in angiogenesis is vascular endothelial growth factor A (hereafter referred as VEGF) (3). VEGF consists of at least 4 splice variants, containing 121, 165, 189, and 206 amino acids (3). It is produced by tumor cells and induces tumor neovascularization (4–7).
Overexpression of VEGF occurs in many human tumor types, which makes VEGF a rational target for antiangiogenic therapy (8–11). This has led to interest in blocking the signaling of VEGF in human tumors. Antibodies binding to this ligand and its receptors, and chemical molecules that can block the tyrosine kinase function of VEGF receptors, have been developed (12).
The drug that is currently most widely used in the clinic is the humanized monoclonal antibody bevacizumab. It blocks VEGF-induced endothelial cell proliferation, permeability, and survival, and it inhibits human tumor cell line growth in preclinical models (8,13–15). The likely mechanism is that bevacizumab binds to VEGF—both soluble and bound to the extracellular matrix—and thereby prevents VEGF binding to its receptors, blocking the biologic pathways induced after VEGF binding. Bevacizumab is approved for clinical use in metastatic colon carcinoma and non–small cell lung cancer (16,17). Approval for several other tumor types is expected soon.
Despite the success of antiangiogenic therapy, a large percentage of patients does not benefit from this targeted therapy. Currently, it is impossible to predict which patient will benefit from antiangiogenic therapy. Reasons for treatment failure may be that the target for the drug is not present or that the drug may not reach the target. Tumor cells produce VEGF, which can lead to paracrine effects in the microenvironment. VEGF121 is freely soluble, whereas VEGF165 is secreted, though a significant fraction remains localized to the extracellular matrix, such as VEGF189 and VEGF206 (18). This will most likely lead to locally high VEGF levels. It is currently impossible to evaluate these local VEGF levels (19). Noninvasive measurement of VEGF in the tumor might give insight to the available target for VEGF-dependent antiangiogenic therapy and thus assist in tumor response prediction. To allow in vivo VEGF imaging, we set up bevacizumab labeling with the relatively new long-lived PET isotope 89Zr and the widely available single γ-emitting isotope 111In (20–23).
In the present study, we describe the development and the in vivo evaluation of 89Zr-bevacizumab and 111In-bevacizumab in a tumor-bearing mouse model and compare noninvasively obtained in vivo 89Zr-bevacizumab and 89Zr-IgG imaging quantification data with ex vivo biodistribution data.
MATERIALS AND METHODS
Conjugation and 89Zr Labeling of Bevacizumab and Control IgG
Bevacizumab (Avastin, 25 mg/mL; Roche) and human IgG (Immunoglobuline I.V.; Sanquin) conjugation and labeling were performed as described previously by Verel et al. (22). Human IgG served as an aspecific control antibody. Briefly, bevacizumab and IgG were purified from other excipients by ultrafiltration (Vivaspin-2; Sartorius) and diluted in water for injection to 5 mg/mL. Hereafter, conjugation of purified bevacizumab and IgG was achieved using N-succinyldesferrioxamine B-tetrafluorphenol (N-sucDf-TFP; VU Medical Center). The ester and the antibodies (bevacizumab and human IgG) were conjugated at room temperature for 30 min at pH 9.5–9.7 (0.1 mol/L Na2CO3; Bufa) with 1.5–2.5 chelate groups per antibody molecule. After conjugation, the mixture was set to pH 4.2–4.4 (0.1 mol/L H2SO4; University Medical Center Groningen [UMC Groningen]), and 50 μL of 25 mg/mL ethylenediaminetetraacetic acid (EDTA; Calbiochem) were added. The solutions were incubated 30 min at 35°C and again purified by ultrafiltration, diluted in water for injection (5 mg/mL), and stored at −20°C.
Labeling was performed with 89Zr (half-life = 3.27 d) produced by Cyclotron BV, which was delivered as 89Zr-oxalate dissolved in oxalic acid (1 M oxalic acid, 2 GBq/mL, 4 GBq/μg 89Zr, 99.9% radionuclidic purity). In brief, the 89Zr-oxalate solution was set at pH 3.9–4.2 and mixed for 3 min and was adjusted to pH 6.7–6.9 with 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES; Sigma-Aldrich) buffer. N-sucDf-bevacizumab was added and incubated for 45 min at room temperature.
Conjugation and 111In Labeling of Bevacizumab
Bevacizumab was conjugated with the chelator 2-(4-isothiocyanatobenzyl)-diethylenetriaminepentaacetic acid (ITC-DTPA; Macrocyclics) according to Ruegg et al. (24) with 2 or 3 chelate groups per antibody molecule. Briefly, 5 mg purified bevacizumab were adjusted to pH 9.2–9.5 (50 mmol/L Na2CO3, pH 9.5; Bufa) and 50 M excess ITC-DTPA was added. After a 1-h incubation at room temperature, the reaction mixture was purified by ultracentrifugation with ammonium acetate (50 mmol/L; UMC Groningen), pH 5.5, to eliminate the excess unconjugated ITC-DTPA. Purified conjugated bevacizumab was diluted (5 mg/mL) in ammonium acetate and stored at −20°C. Labeling was performed with 1 mg of purified ITC-DTPA-bevacizumab, which was allowed to react with 50 MBq of 111InCl3 (370 MBq/mL, >1.85 GBq/μg 111In, 99.9% radionuclidic purity; Tyco Health Care) for 1 h at room temperature. Glassware, materials, and solutions used for the conjugation and labeling procedures were sterilized, pyrogen-free, and metal-free.
Quality Control of 89Zr-Bevacizumab, 111In-Bevacizumab, and 89Zr-IgG
The radiochemical purity of the radiolabeled antibodies was determined by size-exclusion high-performance liquid chromatography (SE-HPLC), trichloroacetic acid protein precipitation (TCA) (89Zr-antibodies), and instant thin-layer chromatography (ITLC) (111In-bevacizumab) to differentiate the labeled product from aggregates and unlabeled 89Zr and 111In.
The HPLC system used consisted of a Waters 1500 series manual injector with a 20-μL injection loop (Rheodyne 7725i injector; Milford), a Waters 1525 binary HPLC pump, a Waters 2487 dual-wavelength absorbance detector, and an in-line radioactivity detector made of a sodium iodide crystal coupled to a multichannel analyzer (Ortec). Chromatograms were analyzed using the Breeze software (Waters). A Superdex 200 30/300 GL size-exclusion column (Amersham Biosciences) was used. The mobile phase consisted of phosphate-buffered saline ([PBS] 140 mmol/L NaCl, 9 mmol/L Na2HPO4, 1.3 mmol/L NaH2PO4; pH = 7.4; UMC Groningen) containing 10% methanol and 23 g/L NaCl. The flow was 0.75 mL/min and the UV-detector wavelengths were set to 220 and 280 nm. The column performance was tested using a reference Bio-Rad gel-filtration standard. The retention time of bevacizumab was 16.7 min. TCA precipitation was performed by mixing equal amounts of water for injection, 20% trichloroacetic acid, and 3 μL 89Zr-bevacizumab reaction solution. The mixture was centrifuged and the radiochemical purity was determined by separation of the protein fraction and supernatant. The radioactivity in the fractions was measured by an LKB-1282-Compu-gamma-system (LKB Wallac).
ITLC was performed on silica gel strips using 0.15 mol/L citrate buffer (pH 6.0) as the mobile phase. Radioactivity was determined by an ITLC scanner (VCS-101; Veenstra Instruments).
In Vitro Evaluation of Radiolabeled Compounds
The stability of 89Zr-bevacizumab, 89Zr-IgG, and 111In-bevacizumab was determined by storing the final product (1 mg, 50 MBq) in 1 mL ammonium acetate (50 mmol/L) at 4°C and in 1 mL human serum (UMC Groningen) at 37°C for 7 d. SE-HPLC, TCA, and ITLC procedures were performed 24, 72, and 168 h after labeling.
The binding properties for VEGF of 89Zr-bevacizumab, 111In-bevacizumab, and 89Zr-IgG were evaluated using a VEGF-coated enzyme-linked immunosorbent assay, comparable with the method described by Collingridge et al. (25). Briefly, recombinant human VEGF165 (catalog no. 293-VE/CF; R&D systems) was used as the target antigen and coated to Nunc-Immuno BreakApart plates (NUNC). Recombinant human VEGF165 was diluted in PBS to a concentration of 5 μg/mL. The solution was adjusted to pH 9.2–9.5 (50 mmol/L Na2CO3). Fifty microliters were added to the wells, incubated overnight at 4°C, and then blocked with 1% human serum albumin (HSA; Sanquin) in PBS. After blocking, the plates were washed with 0.1% polysorbate 80 (Sigma-Aldrich) in PBS. 89Zr-Bevacizumab, 111In-bevacizumab, and 89Zr-IgG solutions were diluted in PBS (concentrations, 1.0–1.0 × 106 ng/mL), added to the wells, and incubated for 2 h. Subsequently, the reaction solution was collected from the wells in 2 wash steps. Both the sustained radioactivity stacked to the antigen-coated wells and the collected reaction solution containing unbound radiolabeled antibody were measured by an LKB-1282-Compu-gamma-system. The percentage of binding was calculated as the fraction of radioactivity stacked to antigen-coated wells divided by the total amount of radioactivity added.
Competition experiments were performed by diluting bevacizumab standard solution (25 mg/mL) with PBS and adding an excess of unlabeled bevacizumab up to 500-fold. Glassware, materials, and solutions used for binding studies were pyrogen-free, metal-free, and coated with 2% HSA in PBS.
Cell Culture and Animal Studies
The human ovarian cancer cell line SKOV-3 was cultured in Dulbecco's modified Eagle medium (DMEM; UMC Groningen) with 4.5 g/mL glucose and 10% fetal calf serum. SKOV-3 cells were chosen because of identified high VEGF production in vivo (26). Before animals were inoculated, the SKOV-3 cells were harvested by trypsinization and resuspended in culture medium and Matrigel (BD Bioscience). In vivo imaging and biodistribution experiments were conducted using male athymic mice (HSD; Athymic nude-nu) obtained from Harlan Nederland. At 8 wk of age, the mice were injected subcutaneously with 1 × 106 SKOV-3 cells mixed equally with 0.1 mL Matrigel. Animals were used for in vivo studies when the tumor measured between 6 and 8 mm in diameter (±0.2 cm3), approximately 2–3 wk after inoculation.
All animal experiments were performed with isofluran inhalation anesthesia (induction, 3%; maintenance, 1.5%). 89Zr-Bevacizumab mice (n = 6) and 89Zr-IgG mice (n = 6) received an intravenous injection into the penile vein (3.5 ± 0.5 MBq, 100 ± 6 μg, 0.2 mL). Animals were imaged using a microPET Focus 220 rodent scanner (Siemens Preclinical Solutions USA, Inc.). Static images of 30-min acquisition time were obtained at 24, 72, and 168 h after injection. Images were corrected for scatter and attenuation. Thereafter, microCT images were made using a MicroCAT II system (Siemens). Images were reconstructed and 3-dimensional regions of interest were drawn within the microCT images and transposed into microPET images for quantification, using the AsiPro 6.2.5.0. software fusion tool (Siemens). The total injected dose was calculated by decay correction of the activity present at 24 h after injection in the animal, at which time the clearance of the injected antibodies is almost negligible. Data are presented as the percentage injected dose per gram tissue (%ID/g), assuming a tissue density of 1 g/cm3. Animals were sacrificed after the last scan (168 h), and organs and tissues were excised, rinsed for residual blood, and weighed.
A combined dose of 50% 111In-bevacizumab and 50% 89Zr-bevacizumab (2.0 ± 0.5 MBq each, 100 ± 4 μg in total, 0.2 mL) was injected intravenously into the penile vein of animals used for ex vivo biodistribution studies. Mice were sacrificed at 24 h (n = 5), 72 h (n = 5), and 168 h (n = 5) after injection. Organs and tissues were excised, rinsed for residual blood, and weighed.
Samples and primed standards were counted for radioactivity in a calibrated well-type LKB-1282-Compu-gamma-system and corrected for physical decay. Biodistribution samples were measured using dual-isotope counting programs for 89Zr and 111In, enabling comparison between 89Zr-bevacizumab and 111In-bevacizumab distribution. Tissue activity is expressed as the %ID/g.
All animal experiments were approved by the Animal Experiments Committee of the University of Groningen.
Immunohistochemistry
Frozen-embedded tumors were stained with antibodies against mouse CD31 (PEGAM-1; BD Pharmingen) and human IgG (Dako). Anti-CD31 staining was performed to determine the microvessel density in the tumors of mice that received 89Zr-bevacizumab or 89Zr-IgG. Microvessel density was scored in 3 areas, defined as hot spot areas with the maximum number of microvessels, by using a calibrated grid. Antihuman IgG staining was performed to obtain more detailed information about the localization of the tracers. The slides were examined at ×200 magnification.
Statistical Analysis
Data are presented as mean ± SD. Statistical analysis was performed using the Mann–Whitney test, version 12 (SPSS). P ≤ 0.05 was considered significant.
RESULTS
Radiolabeling, Quality Control
Labeling with 89Zr and 111In resulted in labeling yields of 98.0% ± 0.7% for 89Zr-bevacizumab and 96.6% ± 0.5% for 111In-bevacizumab and 95.4% ± 0.3% for 89Zr-IgG, without purification. Specific activity was 58 MBq/mg for 89Zr-bevacizumab and 50 MBq/mg for 111In-bevacizumab. No impurities were detected. These results demonstrate that bevacizumab and human IgG can be labeled with high labeling efficiency with 89Zr and 111In.
In Vitro Evaluation of Radiolabeled Compounds
89Zr-Bevacizumab, stored at 4°C in ammonium acetate and at 37°C in serum for 1 wk, displayed a small decrease (6%) in protein-bound radioactivity after 168 h. 111In-Bevacizumab and 89Zr-IgG showed an even smaller decrease (≤5%) in protein-bound radioactivity. The stability of the labeled products ensures optimal quantitative measurement and imaging during 1 wk.
Radiolabeled bevacizumab showed adequate VEGF binding, irrespective of the type of radiolabeling. Binding experiments of 89Zr-bevacizumab resulted in 54.0% ± 3.7% binding. A competition assay with excess unlabeled bevacizumab (≥500 fold) could almost completely block 89Zr-bevacizumab binding (<5%), comparable with 4%–8% nonspecific binding for 89Zr-IgG. Experiments with 111In-bevacizumab showed 56.9% ± 0.7% binding. Competition experiments with 50% radiolabeled and unlabeled bevacizumab (1:1) resulted in an approximately 50% decrease of the initial binding of radiolabeled bevacizumab, demonstrating almost equal binding characteristics of radiolabeled and unlabeled bevacizumab. These results ensure adequate VEGF binding by 89Zr- and 111In-bevacizumab.
Animal Studies
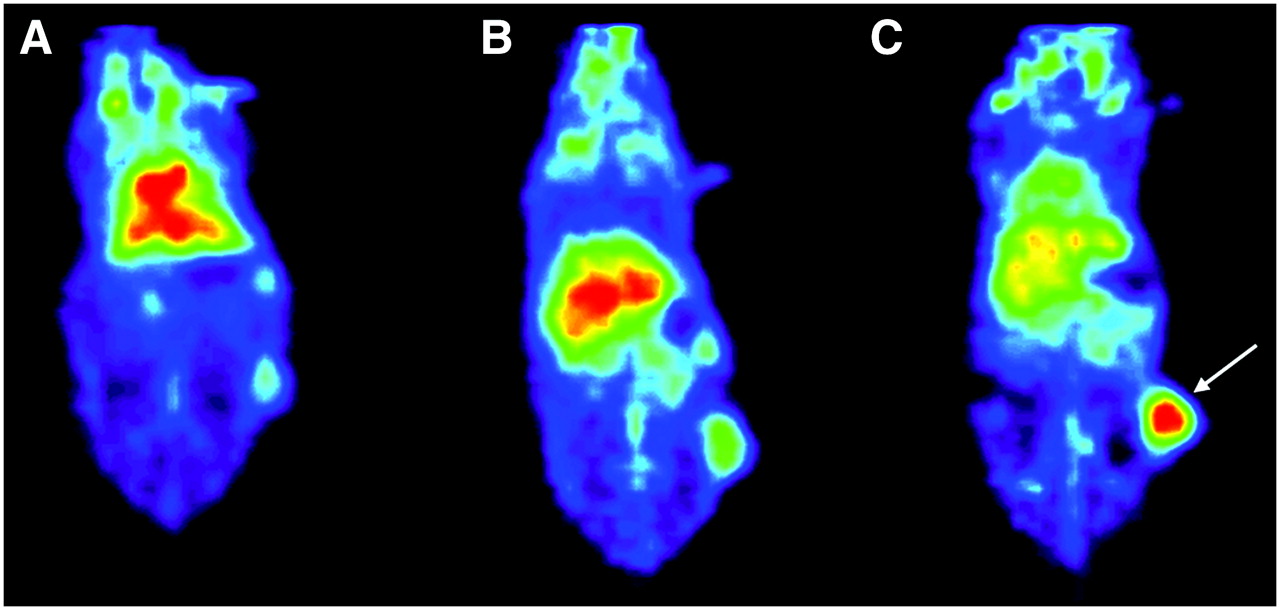
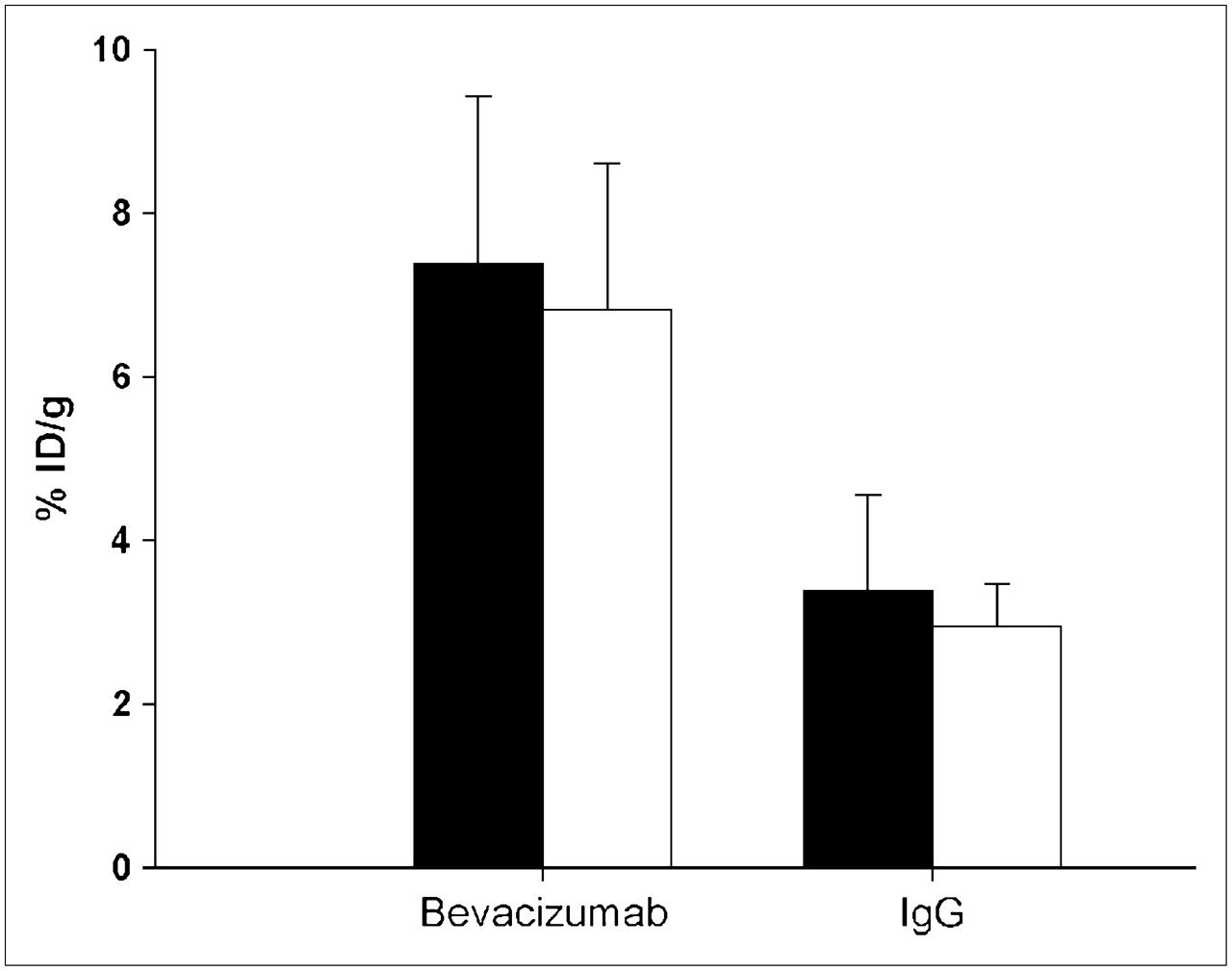
microPET and microCT fusion enabled excellent tumor visualization and quantification (Fig. 1). microPET images showed uptake in well-perfused organs and plasma at 24 h after injection, which declined at later time points. Increasing tumor-to-blood ratio resulted in clear tumor localization of 89Zr-bevacizumab from 72 h onward after injection (Fig. 2). In addition, uptake of 89Zr-bevacizumab was predominantly seen in liver and spleen. Quantitative measurement of 89Zr-bevacizumab in the tumor by microPET was significantly higher compared with human 89Zr-IgG—namely, 7.38 ± 2.06 %ID/g compared with 3.39 ± 1.16 %ID/g (P = 0.011) at 168 h after injection (Fig. 3). Similar results were seen in biodistribution experiments when tumors were excised and counted in a γ-counter: Tumor uptake was 6.82 ± 1.80 %ID/g for 89Zr-bevacizumab compared with 2.87 ± 0.48 %ID/g for human 89Zr-IgG (P = 0.006) (Fig. 3). Beside tumor uptake, ex vivo biodistribution experiments showed an equal organ distribution pattern for 89Zr-bevacizumab and 89Zr-IgG (Fig. 4), except for kidney uptake, which was significantly higher for 89Zr-IgG compared with 89Zr-bevacizumab (P = 0.004).

Coronal CT image (A) with clear subcutaneous localization of SKOV-3 tumor (arrow). Fusion of microPET and CT images (B) (168 h after injection) enables adequate quantitative measurement of 89Zr-bevacizumab in the tumor.

Coronal planes of microPET images 24 h (A), 72 h (B), and 168 h (C) after injection of 89Zr-bevacizumab. At 24 h, most uptake is in well-perfused organs. In time, relative uptake in the tumor (arrow) increases.
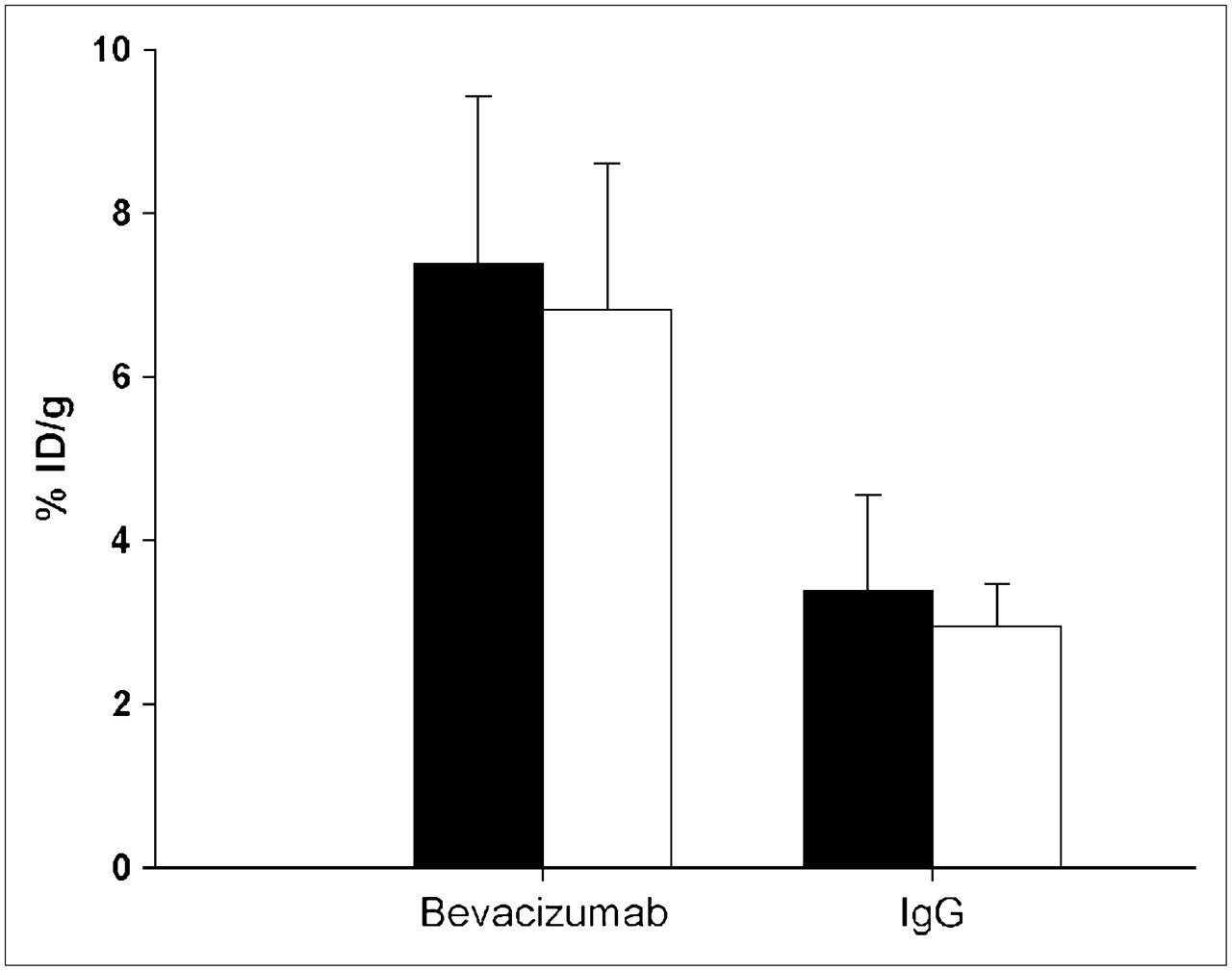
Comparison of tumor uptake of 89Zr-bevacizumab and control 89Zr-IgG as determined by noninvasive microPET imaging (▪) (n = 6) and by γ-counting of excised tumors (□) (n = 6) 168 h after injection. Data are presented as %ID/g ± SD, assuming a tissue density of 1 g/cm3.

Ex vivo biodistribution of 89Zr-bevacizumab (n = 6) (▪) and control 89Zr-IgG (n = 6) (□) 168 h after injection. Uptake of 89Zr-bevacizumab within the tumor is significantly higher than that of control 89Zr-IgG (P = 0.006). Data are presented as %ID/g ± SD. *P ≤ 0.05.
The ex vivo biodistribution for 89Zr-bevacizumab and 111In-bevacizumab was similar at 24, 72, and 168 h after injection (Table 1), demonstrating that both tracers could be used for VEGF imaging.
Ex Vivo Biodistribution of Mice Receiving 89Zr-Bevacizumab and 111In-Bevacizumab
Immunohistochemistry
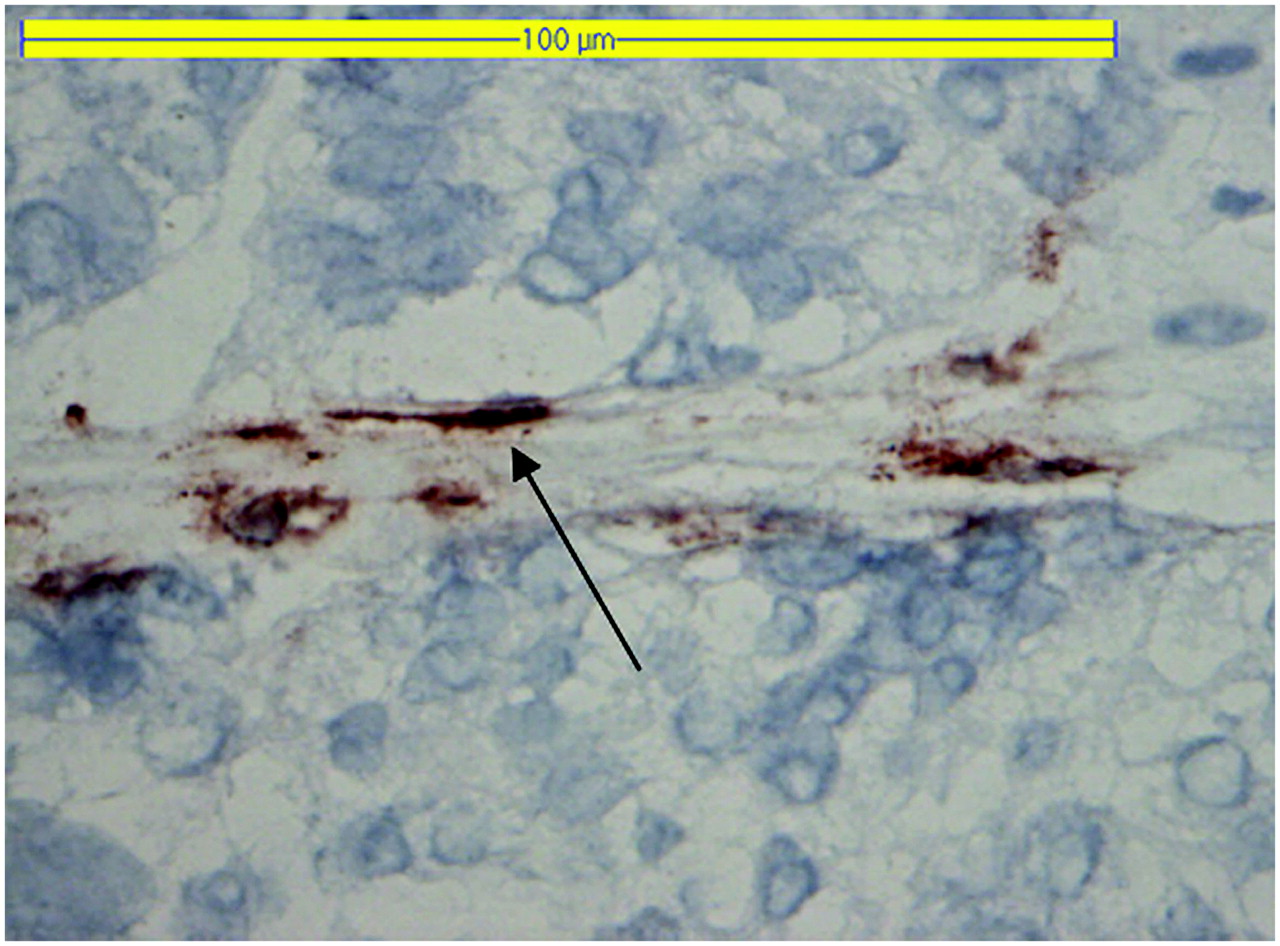
There was no difference in microvessel density or blood vessel distribution pattern between the tumors of the 89Zr-bevacizumab– and the 89Zr-IgG–injected mice. Antihuman IgG staining was seen primarily in the blood vessels of the tumor (Fig. 5).

Antihuman IgG staining (arrow) in a tumor slice from mice receiving 89Zr-bevacizumab.
DISCUSSION
89Zr and 111In labeling of bevacizumab resulted in high labeling efficiencies and adequate preservation of VEGF-binding properties. Tumor uptake of 89Zr-bevacizumab and 111In-bevacizumab were both significantly higher compared with that of the control 89Zr-IgG. Tumor uptake of 89Zr-bevacizumab and 111In-bevacizumab was already high at 24 h after injection, increasing in time with clear tumor visualization from 72 h onward after injection. These results demonstrate that radiolabeled bevacizumab is a potential new tracer for noninvasive imaging of VEGF in the microenvironment of the tumor.
Two human anti-VEGF antibodies, VG76e and HumMV833, have been used previously for noninvasive VEGF imaging (25,27). 125I- and 124I-labeled VG76e—an IgG1 mouse monoclonal anti-VEGF antibody that recognizes the 121, 165, and 189 isoforms of human VEGF-A—showed specific tumor targeting in a human fibrosarcoma xenograft mouse model. Maximum uptake was seen after 24 h, declining at 48 h after injection. These results are in contrast to our results, in which radiolabeled bevacizumab did not show tumor clearance up to 168 h after injection, which increases the available time for imaging. Jayson et al. (27) used 124I-HuMV833, a humanized monoclonal IgG4k antibody that binds VEGF121 and VEGF165, to perform PET studies on patients with various progressive solid tumors. Tumor uptake of 124I-HuMV833 was highly variable between and within patients. For example, there was high uptake of 124I-HuMV833 in an ovarian tumor and low uptake in a poorly vascularized metastasis from colon cancer. These differences may represent the variation in available target for the antibody between tumor types and lesions, which could have implications for anti-VEGF therapy (27). The monoclonal antibody bevacizumab that we used in this study, with high binding affinity to all VEGF-A isoforms and proven clinical effectiveness, is more attractive and accessible for this approach. Another point of application in the evaluation of anti-VEGF therapy could be VEGF-receptor imaging. Cai et al. described the development of VEGF-receptor imaging with 64Cu-DOTA-VEGF121 (DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid) (28). They showed that VEGF-receptor imaging with 64Cu-DOTA-VEGF121 corresponded with immunohistochemical analysis in a human glioblastoma-bearing mouse model. At this point, the correlation between levels of VEGF expression and VEGF-receptor expression is not elucidated. Therefore, in vivo VEGF-receptor imaging with 64Cu-DOTA-VEGF121 might facilitate the evaluation of VEGF-receptor expression, whereas radiolabeled bevacizumab could be used to evaluate VEGF levels. Both techniques could be complementary in the clinical evaluation of antiangiogenic therapy.
In the present study, we have shown that microPET and CT imaging, using 89Zr-bevacizumab, not only allowed imaging up to 168 h after injection but also enabled quantitative measurement of the tracer in the tumor. Tumor uptake values as assessed by noninvasive microPET quantification of 89Zr-bevacizumab were identical to uptake values as assessed by γ-counting of excised tumors, demonstrating the potential role of PET quantification beside in vivo visualization. The biodistribution of bevacizumab was investigated earlier by Lin et al. in rabbits with 125I-labeled bevacizumab; however, the uptake of bevacizumab was only investigated in normal tissues (29). The results were similar to our findings, with high uptake in heart and blood after 24 h, decreasing in time, and high uptake in liver and spleen at later time points. Our study additionally demonstrated that the tumor is a major compartment, besides plasma, liver, and spleen, in bevacizumab distribution.
We used 100 μg of 89Zr-bevacizumab for imaging and biodistribution studies. Smaller doses of bevacizumab could result in accelerated and increased clearance of 89Zr- and 111In-bevacizumab in the absence of IgG production by the nude mice (30). As a control, we used 89Zr-labeled human IgG to provide evidence that 89Zr-bevacizumab uptake is due to specific targeting in the tumor and is not caused by blood perfusion and passive diffusion within the tumor. Another frequently used approach to show specificity is blocking with an excess of the unlabeled agent (25). However, the use of an excess of unlabeled bevacizumab (up to 10-fold) could induce functional changes and, in this way, change the perfusion and uptake of radiolabeled bevacizumab in the tumor at later time points (31). Vascular changes after a single infusion of bevacizumab have been described earlier. Willett et al. showed a decreased microvessel density in rectal cancer patients already at 12 d after a single infusion of bevacizumab (31). To exclude that these effects were present in our study—due to 100 μg of radiolabeled bevacizumab—the microvessel density was determined in the tumors of the 89Zr-bevacizumab– and 89Zr-IgG–injected mice. There was no difference in microvessel density between the tumors of the 2 groups. These findings substantiate the result that high uptake of radiolabeled bevacizumab is due to specific targeting and not a result of vascular changes.
To obtain more detailed information with regard to the localization of radiolabeled bevacizumab (humanized IgG1 antibody) in the tumor, we performed antihuman IgG staining. Antihuman IgG was predominantly present in the blood vessels of the tumors. Cell-surface binding of antihuman IgG was not clearly evident. These results suggested that radiolabeled bevacizumab binds primarily to VEGF present in the blood vessels of the tumor. Binding to VEGF localized in the extracellular matrix of tumor cells could not be demonstrated.
In the present study, we used 2 isotopes for the development of radiolabeled bevacizumab. The PET isotope 89Zr has good characteristics for antibody imaging. The relatively long half-life of 3.27 d makes imaging possible—matching the pharmacokinetics of bevacizumab (half-life = 17–21 d)—combined with the advantages of high-resolution PET imaging. Borjesson et al. described the first clinical application of 89Zr, using labeled U36, an anti-CD44v6 antibody, to detect lymph node metastases in head and neck cancer patients (23). 89Zr will be commercially available soon. 89Zr might give a relatively high radiation exposure to patients, due to the high-energy, high-abundance γ-ray (909 keV, 99.9%) and low-abundance β+ (22%) emitted during the decay of 89Zr (32). However, the clinical dose for adequate 89Zr-bevacizumab PET has yet to be established. Increased sensitivity of new-generation PET cameras could further reduce the radiation exposure. As an alternative for PET, we also developed 111In-labeled bevacizumab for SPECT, as we described previously for trastuzumab, a HER-2 neu antibody (20). The ex vivo biodistribution results for 111In-bevacizumab were similar to those of 89Zr-bevacizumab. Both 111In-bevacizumab and 89Zr-bevacizumab can be used clinically for noninvasive in vivo VEGF imaging, although the feasibility of 111In-bevacizumab for in vivo quantification was not established by this study.
CONCLUSION
This study illustrates the potential of 89Zr-bevacizumab and 111In-bevacizumab as a specific VEGF tracer, with excellent in vivo quantitative measurement of 89Zr-bevacizumab. Noninvasive measurement of VEGF levels in the tumor could provide essential information in the evaluation of antiangiogenic therapy. This could lead to better understanding and patient-tailored therapy.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 28, 2007.
- Accepted for publication April 20, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radiolabeling Molecular Biomarkers of Invasive Pituitary Neuroendocrine Tumors: A Systematic Review
- 89Zr-3,2-HOPO-Mesothelin Antibody PET Imaging Reflects Tumor Uptake of Mesothelin-Targeted 227Th-Conjugate Therapy in Mice
- 89Zr-pembrolizumab biodistribution is influenced by PD-1-mediated uptake in lymphoid organs
- Development and Evaluation of Interleukin-2-Derived Radiotracers for PET Imaging of T Cells in Mice
- Probody Therapeutic Design of 89Zr-CX-072 Promotes Accumulation in PD-L1-Expressing Tumors Compared to Normal Murine Lymphoid Tissue
- A Distinct Advantage to Intraarterial Delivery of 89Zr-Bevacizumab in PET Imaging of Mice With and Without Osmotic Opening of the Blood-Brain Barrier
- Roadmap for the Development and Clinical Translation of Optical Tracers Cetuximab-800CW and Trastuzumab-800CW
- Near-infrared fluorescence molecular endoscopy detects dysplastic oesophageal lesions using topical and systemic tracer of vascular endothelial growth factor A
- PET Imaging of Receptor Tyrosine Kinases in Cancer
- Preclinical Development of CD38-Targeted [89Zr]Zr-DFO-Daratumumab for Imaging Multiple Myeloma
- Human Epidermal Growth Factor Receptor 3-Specific Tumor Uptake and Biodistribution of 89Zr-MSB0010853 Visualized by Real-Time and Noninvasive PET Imaging
- The Use of Microdosing in the Development of Small Organic and Protein Therapeutics
- Threshold Analysis and Biodistribution of Fluorescently Labeled Bevacizumab in Human Breast Cancer
- Predictive factors of response to mTOR inhibitors in neuroendocrine tumours
- Molecular Fluorescence Endoscopy Targeting Vascular Endothelial Growth Factor A for Improved Colorectal Polyp Detection
- PET/CT-Derived Whole-Body and Bone Marrow Dosimetry of 89Zr-Cetuximab
- 89Zr-Bevacizumab PET Visualizes Heterogeneous Tracer Accumulation in Tumor Lesions of Renal Cell Carcinoma Patients and Differential Effects of Antiangiogenic Treatment
- Everolimus Reduces 89Zr-Bevacizumab Tumor Uptake in Patients with Neuroendocrine Tumors
- Development of a Radiolabeled Irreversible Peptide Ligand for PET Imaging of Vascular Endothelial Growth Factor
- Early Assessment of Tumor Response to Gefitinib Treatment by Noninvasive Optical Imaging of Tumor Vascular Endothelial Growth Factor Expression in Animal Models
- In Vivo Visualization of MET Tumor Expression and Anticalin Biodistribution with the MET-Specific Anticalin 89Zr-PRS-110 PET Tracer
- 89Zr-Bevacizumab PET Imaging in Primary Breast Cancer
- Bevacizumab-Induced Normalization of Blood Vessels in Tumors Hampers Antibody Uptake
- Placental Growth Factor (PlGF)-Specific Uptake in Tumor Microenvironment of 89Zr-Labeled PlGF Antibody RO5323441
- Technetium-Bevacizumab in a Patient With Bone and Lung Metastatic Colon Adenocarcinoma
- Measurement of Tumor VEGF-A Levels with 89Zr-Bevacizumab PET as an Early Biomarker for the Antiangiogenic Effect of Everolimus Treatment in an Ovarian Cancer Xenograft Model
- Advances in Immuno-Positron Emission Tomography: Antibodies for Molecular Imaging in Oncology
- Nanobodies Targeting the Hepatocyte Growth Factor: Potential New Drugs for Molecular Cancer Therapy
- Molecular Imaging of Tumors with Radioactive Labeled Antibodies from Laboratory to the Clinic
- PET with the 89Zr-Labeled Transforming Growth Factor-{beta} Antibody Fresolimumab in Tumor Models
- Specific biomarkers of receptors, pathways of inhibition and targeted therapies: pre-clinical developments
- Intraoperative Near-Infrared Fluorescence Tumor Imaging with Vascular Endothelial Growth Factor and Human Epidermal Growth Factor Receptor 2 Targeting Antibodies
- Novel insights on imaging sex hormone-dependent tumourigenesis in vivo
- VEGF-PET Imaging Is a Noninvasive Biomarker Showing Differential Changes in the Tumor during Sunitinib Treatment
- Increase of Plasma VEGF after Intravenous Administration of Bevacizumab Is Predicted by a Pharmacokinetic Model
- 111In-Bevacizumab Imaging of Renal Cell Cancer and Evaluation of Neoadjuvant Treatment with the Vascular Endothelial Growth Factor Receptor Inhibitor Sorafenib
- 89Zr-DFO-J591 for ImmunoPET of Prostate-Specific Membrane Antigen Expression In Vivo
- Immuno-PET Quantitation of de2-7 Epidermal Growth Factor Receptor Expression in Glioma Using 124I-IMP-R4-Labeled Antibody ch806
- 89Zr-Bevacizumab PET of Early Antiangiogenic Tumor Response to Treatment with HSP90 Inhibitor NVP-AUY922
- Radiation Dosimetry of 89Zr-Labeled Chimeric Monoclonal Antibody U36 as Used for Immuno-PET in Head and Neck Cancer Patients
- Development and Characterization of Clinical-Grade 89Zr-Trastuzumab for HER2/neu ImmunoPET Imaging
- Disparity Between In Vivo EGFR Expression and 89Zr-Labeled Cetuximab Uptake Assessed with PET
- Multimodality Molecular Imaging of Tumor Angiogenesis
- Increased Metabolic Activity of Indolent Liver Metastases After Resection of a Primary Colorectal Tumor
- Immuno-PET: A Navigator in Monoclonal Antibody Development and Applications