


Abstract
Vascular endothelial growth factor (VEGF)-A is overexpressed in most malignant and premalignant breast lesions. VEGF-A can be visualized noninvasively with PET imaging and using the tracer 89Zr-labeled bevacizumab. In this clinical feasibility study, we assessed whether VEGF-A in primary breast cancer can be visualized by 89Zr-bevacizumab PET. Methods: Before surgery, breast cancer patients underwent a PET/CT scan of the breasts and axillary regions 4 d after intravenous administration of 37 MBq of 89Zr-bevacizumab per 5 mg. PET images were compared with standard imaging modalities. 89Zr-bevacizumab uptake was quantified as the maximum standardized uptake value (SUVmax). VEGF-A levels in tumor and normal breast tissues were assessed with enzyme-linked immunosorbent assay. Data are presented as mean ± SD. Results: Twenty-five of 26 breast tumors (mean size ± SD, 25.1 ± 19.8 mm; range, 4–80 mm) in 23 patients were visualized. SUVmax was higher in tumors (1.85 ± 1.22; range, 0.52–5.64) than in normal breasts (0.59 ± 0.37; range, 0.27–1.69; P < 0.001). The only tumor not detected on PET was 10 mm in diameter. Lymph node metastases were present in 10 axillary regions; 4 could be detected with PET (SUVmax, 2.66 ± 2.03; range, 1.32–5.68). VEGF-A levels in the 17 assessable tumors were higher than in normal breast tissue in all cases (VEGF-A/mg protein, 184 ± 169 pg vs. 10 ± 21 pg; P = 0.001), whereas 89Zr-bevacizumab tumor uptake correlated with VEGF-A tumor levels (r = 0.49). Conclusion: VEGF-A in primary breast cancer can be visualized by means of 89Zr-bevacizumab PET.
Breast cancer is the most common cause of cancer-related deaths among women (1). The application of molecular imaging can visualize and potentially quantifies functional differences between tumor and normal cells. A molecular target of interest in this respect is vascular endothelial growth factor (VEGF)-A. VEGF-A is involved in the development and maintenance of tumor angiogenesis and is involved early during tumorigenesis. Various studies have reported overexpression of VEGF-A in the breast cancer microenvironment, compared with normal breast tissue (2–5). All VEGF-A splice variants are bound by the clinically used monoclonal antibody bevacizumab. When labeled with the PET isotope 89Zr, bevacizumab preserves its VEGF-A–binding properties. Thus, tracer dosages of radiolabeled bevacizumab can be used for tumor-specific, whole-body imaging of VEGF-A. In preclinical studies (6,7) and in a study in renal cell cancer patients (8), we have already shown an excellent tumor-to-background ratio with an optimum at 4 d after tracer injection when using 89Zr-bevacizumab. In the present clinical feasibility study, we used 89Zr-bevacizumab PET to provide proof of principle on whether VEGF-A imaging can be used for detection of primary breast tumors.
MATERIALS AND METHODS
Patients
Eligible patients had a histologically or cytologically confirmed adenocarcinoma of the breast and were scheduled for mastectomy or lumpectomy. Additional eligibility criteria included a minimum age of 18 y and World Health Organization performance status of no more than 2. In all patients, standard diagnostics consisted of mammography and ultrasonography. When needed to better define tumor extent, MR imaging was also performed. Exclusion criteria included pregnancy or lactation, prior radiotherapy in the involved area, major surgery within 28 d before initiation of the study, clinically significant cardiovascular disease, or prior allergic reactions to immunoglobulins. In premenopausal patients, a pregnancy test was performed to exclude pregnancy.
The study was approved by the Medical Ethics Committee of the University Medical Center of Groningen. This local committee was supervised by the Central Committee on Research Involving Human Subjects, which acts as the competent authority. All patients gave written informed consent. The trial is registered under clinicaltrial.gov number NCT00991978.
89Zr-Bevacizumab PET Imaging
Patients received 37 MBq of 89Zr-bevacizumab per 5 mg of protein as an intravenous bolus injection 4 d before PET scanning and were observed for allergic reactions for 1 h. The 5-mg dose of bevacizumab was chosen because this was the lowest possible dose that was reproducible during the labeling procedure. The same dose was used in a study with 111In-labeled bevacizumab, which visualized all known melanoma lesions (9). 89Zr has a decay half-life of 78.4 h, the mean β-energy is 395.5 keV, the positron branching fraction is 22.74%, and the main γ-emissions are 511 keV, 45.5%, and 909 keV, 99.04%. Clinical 89Zr-bevacizumab was produced as follows: reconstituted bevacizumab (Avastin; Roche) was conjugated with tetrafluorphenol-N-succinyldesferal-Fe (VU University Medical Center), purified, and stored at −80°C. Good manufacturing practice–produced 89Zr-oxalate (BV Cyclotron) was used for radiolabeling the conjugate. Quality control was performed to ensure radiochemical purity (>95%), antigen binding, and stability. PET/CT was performed with a Biograph mCT 64-slice PET/CT camera (Siemens). Scanning of both breasts and the axillary regions was performed in 2 bed positions with 5 min of imaging per bed position. In addition, a low-dose CT scan was performed and was used for attenuation and scatter correction. The patient was positioned prone with the breasts hanging. PET data were reconstructed with Siemens iterative reconstruction, involving 3-dimensional ordinary Poisson ordered-subsets expectation maximization without time-of-flight and point-spread-function methods. The settings used for reconstruction were 2 iterations and 8 subsets, a matrix size of 200, and a postprocessing filter of 10 mm, resulting in an effective resolution of 11 mm. For sentinel lymph node detection and SPECT imaging as standard of care, 100 MBq of 99mTc-labeled nanocolloid were administered 1 d before surgery. To avoid interference of SPECT imaging, a minimal interval of 3 half-life episodes of 89Zr-bevacizumab (11 d) was considered between the administration of 89Zr-bevacizumab and 99mTc-nanocolloid to allow for sufficient 89Zr isotope decay.
89Zr-Bevacizumab PET Analysis
Final image analysis was done by a nuclear medicine physician. Separate analysis of the mammography and ultrasonographic images was executed by a radiologist and compared with the PET images in collaboration with the nuclear medicine physician to confirm that the tumor location on both imaging modalities was identical. Uptake of 89Zr-bevacizumab in the tumor was quantified using AMIDE, A Medical Image Data Examiner software (version 0.9.3; Stanford University) (10). For the quantification of radioactivity within the tumor, 3-dimensional regions of interest were manually drawn around the tumor and axillary lymph node metastasis (if present). For determining the background also, uptake in the cardiac blood pool, normal breast (ipsi- and contralateral), and nipple was quantified. The data are presented as the maximum standardized uptake value (SUVmax). Furthermore, the images were analyzed for uptake of 89Zr-bevacizumab along the cytology or biopsy channel.
Enzyme-Linked Immunosorbent Assay (ELISA) to Detect VEGF-A
For quantification of VEGF-A expression in the surgical specimen, ELISA was performed according to the manufacturer instructions (Quantikine; R&D Systems). Three random samples were collected from the surgical specimen of the primary tumor, ipsilateral normal tissue, and nipple tissue. Tissue was lysed manually using mammalian protein extraction reagent (M-PER; Pierce). Thereafter, mixtures were centrifuged at 20,000g for 15 min and subsequently stored at −20°C until analysis. Results of VEGF-A measurement were normalized for the protein concentration of the same samples determined by the Bradford assay (11).
Tumor Histology and Immunohistochemistry
Tumor tissue of the surgical specimen was typed and graded according to the World Health Organization guidelines and the modified Bloom and Richardson guidelines, respectively. Immunohistochemistry for VEGF-A and Ki-67 was performed on tumors, ductal carcinoma in situ (if present), and normal breast tissue using paraffin-embedded slides. Slides were deparaffinized in xylene and rehydrated in ethanol. Endogenous peroxidase was blocked by incubation with 0.3% hydrogen peroxidase for 30 min. The primary antibodies rabbit anti-VEGF-A (A20-c152, 1:50; Santa Cruz Biotechnology), mouse anti-Ki-67 (1:300, clone MIB-1; DAKO), and mouse anti-CD31 (BD Pharmingen) were applied for 60 min, followed by suitable secondary antibodies, and immunostaining was visualized with 3′3-diaminobenzidine tetrahydrochloride. Counterstaining was performed with hematoxylin. All stainings were scored by 2 independent observers. VEGF-A was scored (negative/positive) at ×400 magnification. The proliferation index was calculated by counting of Ki-67–positive versus –negative cells in at least 5 high-power fields (×400). Microvessel density was scored in 5 areas defined as hot spots with the maximum number of microvessels.
Breast cancer molecular subtypes according to immunohistochemical profile were categorized as follows: luminal A (estrogen receptor [ER]–positive or progesterone receptor [PR]–positive and Ki-67 < 14%), luminal B (ER-positive or PR-positive and Ki-67 ≥ 14%), human epidermal growth factor receptor 2 (HER2)–enriched (ER-negative, PR-negative, and HER2-positive), and basallike (ER-negative, PR-negative, HER2-negative). Luminal B also included tumors that were ER-positive or PR-positive and HER2-positive (12).
Phantom Study
To define the detection limit of the PET/CT camera system, a breast simulation phantom study was performed. Breast-shaped phantoms were produced as described earlier (13,14). For tumorlike agarose inclusions, 2% agarose (Hispanagar) was suspended in Tris-buffered saline and heated to 70°C. Subsequently, 89Zr-oxalate was dissolved to a final concentration of 7,700 Bq/mL. Silicone molds were filled with the agarose mixture to create tumorlike inclusions ranging from 5 to 20 mm in diameter.
Breast phantoms were constructed with 2 tumorlike inclusions. PET imaging was performed on day 1 and every 3–4 d until visual disappearance of the lesions from the scan. Final image analysis was performed as stated above. The recovery coefficient was determined by calculating the ratio between the measured amount of 89Zr on the PET image and the inserted dose as measured by a dose calibrator, corrected for decay.
Statistical Analyses
Data are presented as a mean ± SD. Statistical analysis was performed using the paired t test or Wilcoxon signed rank test for paired data and the unpaired t test for unpaired data. Associations between parameters were evaluated using the Pearson correlation test (SPSS, version 19.0; IBM). A double-sided P value of less than 0.05 was considered significant.
RESULTS
Patient Characteristics
A total of 23 patients with 26 breast tumors was included. The patients had no history of prior malignancies. Two women had bilateral breast cancer, and 1 patient had 2 ipsilateral tumors. Patient and tumor characteristics are shown in Table 1. Breast tumors were detected with mammography (n = 22), ultrasound (n = 25), or MR imaging (n = 1). Histologic analyses showed invasive ductal carcinoma (n = 23), invasive lobular carcinoma (n = 2), and invasive tubular carcinoma (n = 1). Of the 25 available invasive cancers, 9 tumors were classified as luminal A breast cancer and 14 as luminal B. There was 1 basallike and 1 HER2-enriched tumor. Six patients had pathologically proven axillary lymph node metastases before surgery. In 3 additional patients, tumor cells were detected in the sentinel lymph node after surgery. In a patient with bilateral breast cancer, axillary lymph node involvement on one side was already known before surgery and was also detected in a sentinel lymph node of the opposite axilla.
Patient and Tumor Characteristics
89Zr-Bevacizumab PET
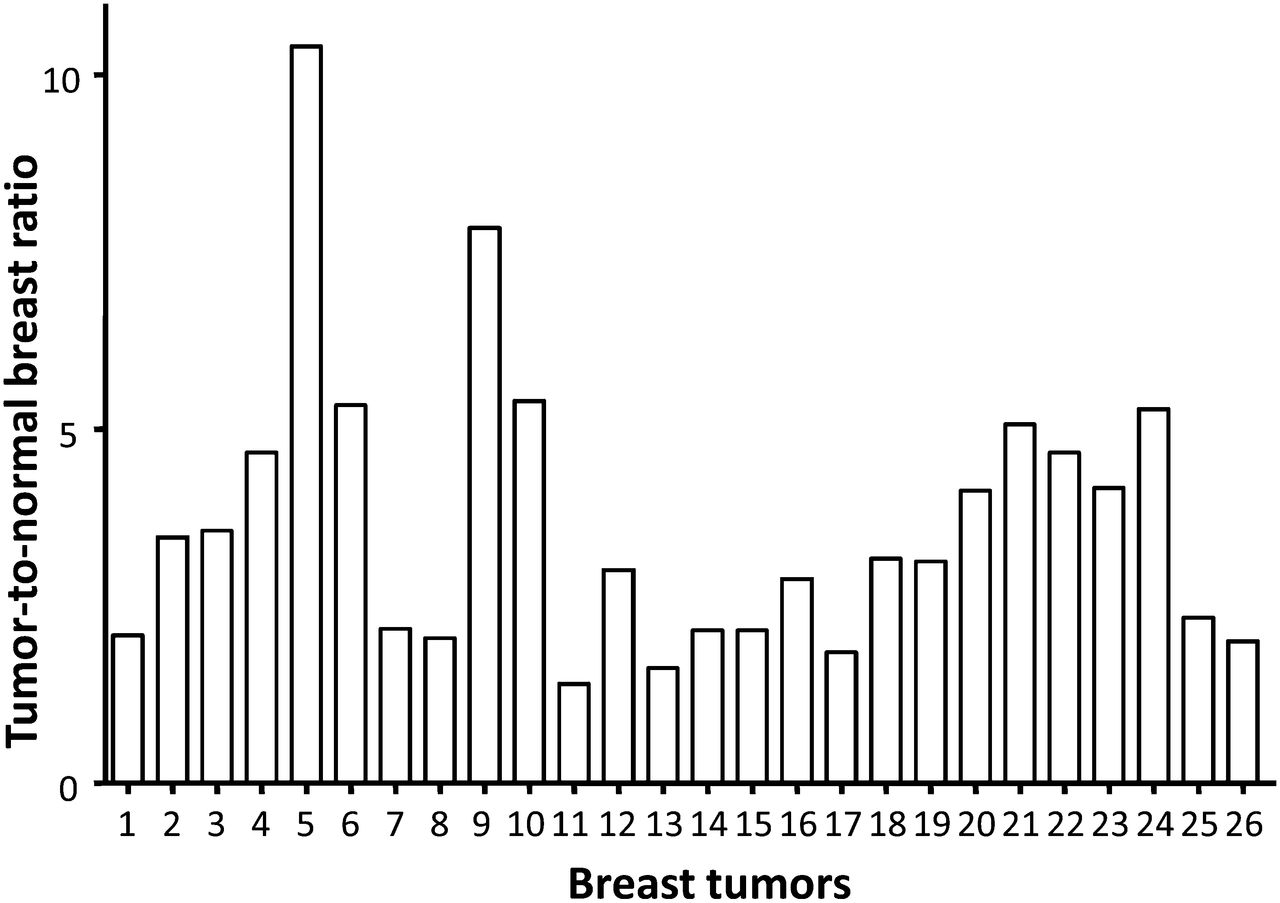
In this study, no adverse events were seen. 89Zr-bevacizumab PET imaging showed uptake in 25 of the 26 breast tumors (96.1%). Figure 1 shows a representative example. Uptake of 89Zr-bevacizumab was higher in breast tumors than in normal breast tissue (of both the ipsi- and contralateral breast); SUVmax was 1.85 ± 1.22 (range, 0.52–5.64) in breast tumors versus 0.59 ± 0.37 (range, 0.27–1.69) in ipsilateral normal breast tissue and 0.51 ± 0.26 (range, 0.20–1.12) in contralateral normal breast tissue (both P < 0.001) (Fig. 2A). There was similar 89Zr-bevacizumab uptake in normal tissue of both breasts (P = 0.88). The SUVmax of luminal A tumors was 1.28 ± 0.58, compared with 2.04 ± 1.08 in luminal B tumors (P = 0.06). In the patients with a basallike and HER2-overexpressing breast tumor, SUVmax was 0.52 and 5.64, respectively. The only breast tumor that did not show preferential 89Zr-bevacizumab uptake was an invasive ductal carcinoma with a diameter of 10 mm. Lymph node metastases (size range, 3–42 mm) were present in 10 axillary regions (of 9 patients); 4 of these lymph node–positive axillary regions were detected by PET (SUVmax, 2.66 ± 2.03; range, 1.32–5.68). On the basis of ultrasound and cytology, all 4 positive axillary regions were already known before surgery. 89Zr-bevacizumab PET detected none of 4 positive axillary regions with 1–3 lymph node metastases (pN1) and 4 of 6 positive axillary regions with 4 or more lymph node metastases (≥pN2). There were no false-positive readings, and there was no 89Zr-bevacizumab uptake along the cytology or biopsy tract.

Axial slices of 89Zr-bevacizumab PET from patient with primary breast tumor (1) and lymph node metastasis (2).

Analysis per patient (x-axis) showing ratio between 89Zr-bevacizumab uptake expressed as SUVmax in breast tumors vs. normal breast tissue.
Next to tumor visualization, there was slightly higher uptake in the nipples of both breasts than in the background in 20 of the 23 patients. The SUVmax of nipple tissue was 1.13 ± 0.59 (range, 0.47–3.02). This is lower than the SUVmax in tumor tissue (P = 0.01). The SUVmax in the blood pool on day 4 was 4.17 ± 1.07 (range, 2.97–7.05), which is 2.3- and 3.7-fold higher than in the tumors and nipples, respectively.
VEGF-A ELISA
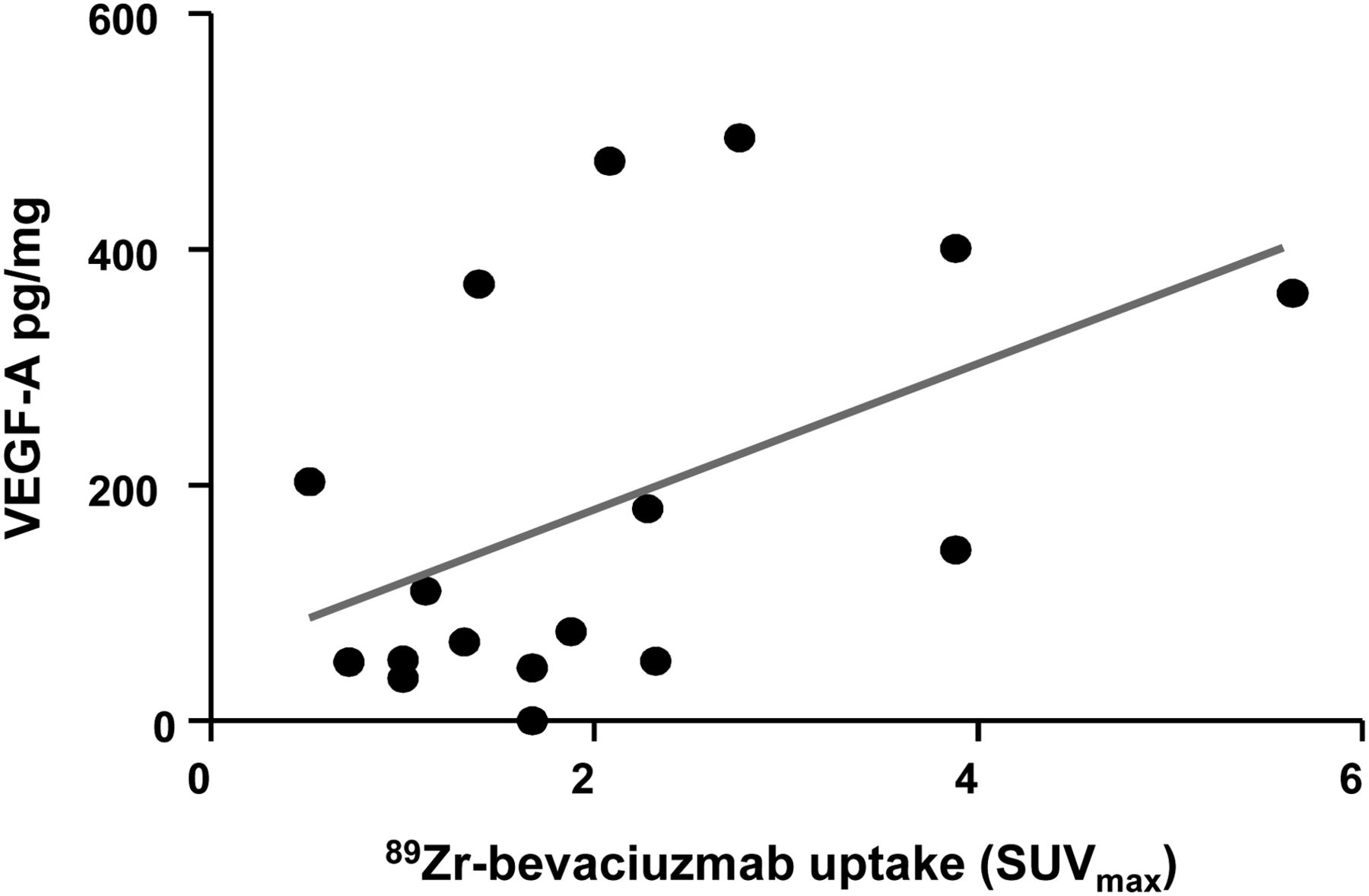
For VEGF-A ELISA measurements, surgical specimens of 17 breast tumors and 24 specimens of normal ipsilateral breast tissue were available. Pathologic examination of the tissue confirmed tumor in all macroscopic tumors. Mean tumor VEGF-A/mg of protein was higher (184 ± 169 pg) than in normal breast tissue (10 ± 21 pg, P = 0.001) (Fig. 2B). In the 10-mm tumor that was not detected by 89Zr-bevacizumab PET, 371 pg of VEGF-A per milligram of protein was measured. 89Zr-bevacizumab tumor uptake of the 89Zr-bevacizumab–detected tumors correlated with the VEGF-A protein level (Pearson r = 0.49, P = 0.04) (Fig. 3).
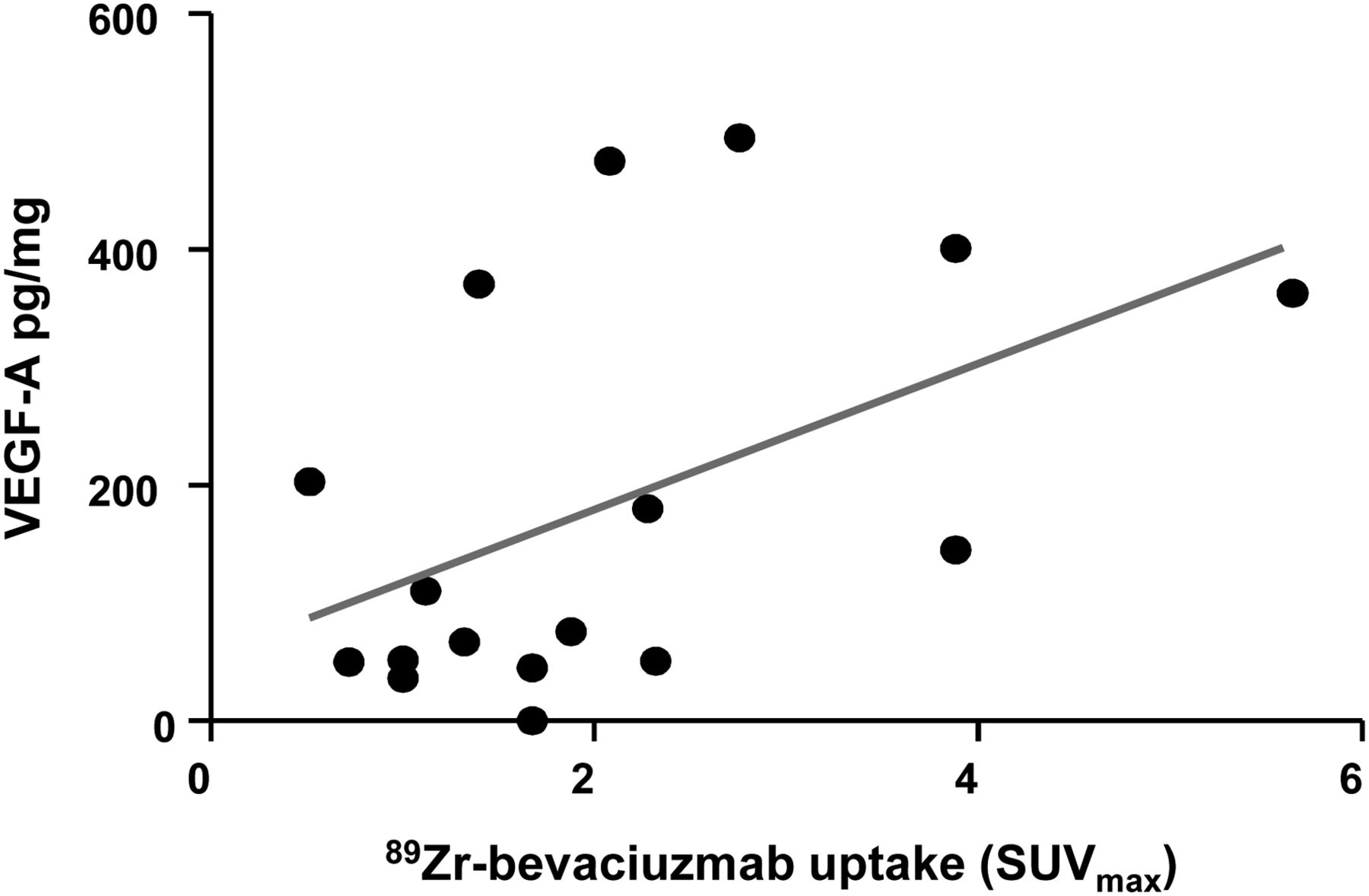
Correlation between 89Zr-bevacizumab tumor uptake (x-axis) and tumor VEGF-A (y-axis) levels as measured by ELISA (Pearson r = 0.49, P = 0.04).
In the 11 available nipple specimens (including both nipples from 1 patient with bilateral breast cancer), the VEGF-A level was 10 ± 13 pg per milligram of protein, which was not different from normal breast tissue (P = 0.96).
Immunohistochemistry
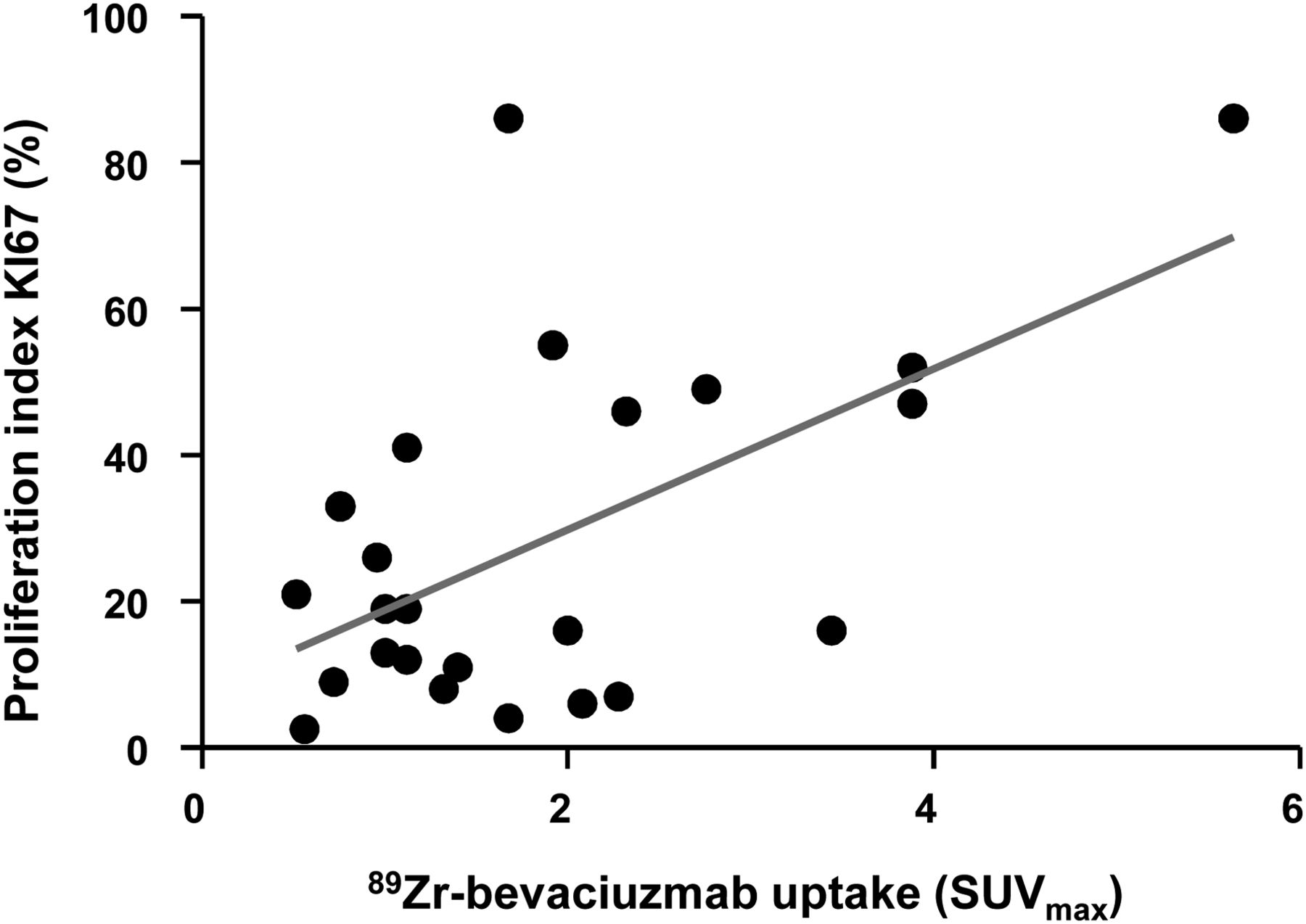
All available tumors (n = 25) showed positive staining for VEGF-A expression. VEGF-A expression in normal tissue was absent in 2 and present in 23 of the 25 operated breasts. Ductal carcinoma in situ was present in 10 patients and stained positively for VEGF-A in all cases. 89Zr-bevacizumab tumor uptake correlated positively with a mean proliferation index of 32.1 ± 24.3 (range, 6.0–86.0) (Pearson r = 0.55, P = 0.005) (Fig. 4). The microvessel density did not correlate with 89Zr-bevacizumab uptake (r = 0.10, P = 0.64).

Correlation between 89Zr-bevacizumab tumor uptake (x-axis) and proliferation index (y-axis) as measured with Ki-67 expression by tumor (Pearson r = 0.55, P = 0.005).
Phantom Study
All tumorlike inclusions were visible on day 1. The recovery coefficient was 73% for the smallest inclusion and 96% for the largest one. The last time point before visual disappearance was day 1 (5-mm inclusion), day 10 (10-mm inclusion), day 14 (15-mm inclusion), and day 17 (20-mm inclusion).
DISCUSSION
To our knowledge, this was the first clinical feasibility study with 89Zr-bevacizumab PET in breast cancer patients. Uptake of 89Zr-bevacizumab was visualized in 96.1% of the primary tumor lesions, and there was a relation with the level of VEGF-A in the tumor. This result provides proof that 89Zr-bevacizumab might be potentially valuable for biologic characterization of tumors and for prediction and evaluation of the effect of VEGF-A–targeting therapeutics.
VEGF-A is reported in several studies to be overexpressed in malignant breast tumors and in ductal carcinoma in situ (5,15), thus covering the full spectrum from early-stage breast cancer to more advanced stages. More frequent VEGF-A staining was found to be related to aggressiveness as assessed by VEGF-A staining in a study with 1,788 breast tumors (5). 89Zr-bevacizumab PET proved to be able to detect a broad range of VEGF-A expression levels. Quantitative tumor analyses showed a more than 10-fold difference between individual SUVmax measurements, suggesting large differences in VEGF-A tumor levels between patients, as was confirmed by the broad difference in VEGF-A measured by ELISA. Although there was a high visualization rate, the SUVmax of tumors and normal tissues did overlap in this study. Importantly, in individual patients SUVmax was always higher in tumor than in normal breast tissues. The higher VEGF-A ratio between tumor and normal breast as measured by ELISA than by PET might be explained by the fact that (in contrast to 89Zr-bevacizumab PET) ELISA also measures intracellular VEGF-A (16). Moreover, the resolution of the PET camera is 10 mm whereas ELISA and immunohistochemistry measure on the cellular level.
89Zr-bevacizumab uptake in the primary breast tumors was relatively low, compared with uptake in a series of 22 metastatic renal cell cancers in our institution (mean SUVmax, 1.85 vs. 10.1) (15). Antiangiogenic treatment has monotherapy activity in renal cell cancers but not in tumor types such as breast cancer (17,18). The difference in 89Zr-bevacizumab uptake, and therefore VEGF-A levels, is possibly related to this varying efficacy. 89Zr-bevacizumab might be potentially valuable for biologic characterization of tumors and for prediction and evaluation of the effect of VEGF-A–targeting therapeutics.
The failure to detect the tumor lesion 10 mm in diameter despite sufficient VEGF-A expression can be explained by the findings in our phantom study. Small lesions visually disappear much earlier on 89Zr-PET than do larger lesions. This effect might influence tumor uptake of 89Zr-bevacizumab measured by SUVmax. The observed effect of tumor size on PET detection is shared by 18F-FDG PET (19,20) but is larger in the case of 89Zr-PET. Because of the higher radiation dose per megabecquerel of 89Zr, a lower amount of activity was injected for 89Zr than for 18F-FDG. 89Zr has a smaller yield of positrons than does 18F, resulting in increased noise, and therefore 89Zr-bevacizumab PET images require more smoothing. This degrades resolution and increases size effects. Importantly, imaging with 89Zr-bevacizumab PET delivered no false-positive lesions.
Most patients had uptake of 89Zr-bevacizumab in the region of the nipple, whereas the VEGF-A level as measured with ELISA was low and equal to that in normal tissue. 89Zr has a long half-life of 78.4 h. When labeled to bevacizumab, a considerable amount of the tracer remains in the circulation. Therefore, uptake of 89Zr-bevacizumab in the nipple is likely to be due to high vascularization of the nipple, compared with normal breast tissue (21). In the tumor, the contribution of perfusion to increased 89Zr-bevacizumab uptake in the tumor is less likely to play a role, based on preclinical and clinical data. In a xenograft mouse model, we have shown that tumor accumulation of 89Zr-bevacizumab increases in time, whereas uptake in normal organs decreases (6). This increase in 89Zr-bevacizumab tumor accumulation over time was also shown in melanoma patients who underwent 111In-bevacizumab SPECT (9). In a human SKOV-3 ovarian tumor xenograft, there was higher uptake of 89Zr-bevacizumab than of 89Zr-IgG (6), indicating tumor-specific uptake. 89Zr-IgG PET in the patient setting is not possible because of radiation exposure concerns. This is also the limiting factor in using 89Zr-bevacizumab PET in healthy subjects as a negative control. However, the microvessel density did not influence 89Zr-bevacizumab uptake. Moreover, the relation between VEGF-A measured by ELISA and 89Zr-bevacizumab uptake in tumors and not in nipple tissue is in line with the preclinical finding that the tracer uptake is, in fact, tumor-specific.
The limiting factor for more general application of imaging with radionuclides is the radiation burden. In a study comparing the risks of radiation-induced cancer from mammography, molecular breast imaging, and positron emitting mammography, the cumulative cancer incidence is 15–30 times higher for positron emission mammography and molecular breast imaging than for mammography (22). The estimated radiation burden of 89Zr-bevacizumab-PET is 19 mSv per tracer injection, on the basis of extrapolation from 111In-bevacizumab data and a dosimetry study on 89Zr-U36, compared with 5.3 mSv for 18F-FDG PET (23–25).
To make optimal use of the tumor specificity of molecular imaging of VEGF-A while overcoming radiation issues, bevacizumab was also linked to the near-infrared fluorescent dye IRDye 800CW in our institution. This technique has already been tested in human xenograft–bearing athymic mice, detecting tumor lesions in vivo with high sensitivity and specificity. IRDye 800CW–labeled bevacizumab revealed submillimeter lesions with a clinical intraoperative fluorescence camera (26). Recently, we started a study with IRDye 800CW–labeled bevacizumab in early breast cancer (NCT01508572). The aim of this study is to determine the uptake of the VEGF-A–targeting fluorescent tracer in breast tumors, both during preoperative diffuse optical tomography and during surgery. This approach can potentially contribute to the development of a tumor-specific tracer.
CONCLUSION
In this first clinical feasibility study with 89Zr-bevacizumab PET in breast cancer patients, we have shown that uptake of 89Zr-bevacizumab was visible in most primary breast tumors and correlated with the protein level of VEGF-A in the tumor. These findings support use of VEGF-A imaging in breast cancer for future imaging purposes.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by the Dutch Cancer Society (grant RUG 2009-4273), the Dutch Pink Ribbon Foundation, and the foundation A Sister’s Hope (grant KP566481). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Arieke Prozée, Kees Meijer, and Marian Beernink for their assistance with patient inclusion in the trial and Tineke van der Sluis and Esther M.E. van Straten for their technical assistance.
Footnotes
Published online May 7, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 26, 2012.
- Accepted for publication January 28, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 89Zirconium-labelled girentuximab (89Zr-TLX250) PET in Urothelial Cancer Patients (ZiPUP): protocol for a phase I trial of a novel staging modality for urothelial carcinoma
- 89Zr-Immuno-PET: Toward a Noninvasive Clinical Tool to Measure Target Engagement of Therapeutic Antibodies In Vivo
- 89Zr-oxine labelling and PET imaging shows lung delivery of a cell/gene cancer therapy
- A Distinct Advantage to Intraarterial Delivery of 89Zr-Bevacizumab in PET Imaging of Mice With and Without Osmotic Opening of the Blood-Brain Barrier
- Near-infrared fluorescence molecular endoscopy detects dysplastic oesophageal lesions using topical and systemic tracer of vascular endothelial growth factor A
- PET Imaging of Receptor Tyrosine Kinases in Cancer
- Tracers for Fluorescence-Guided Surgery: How Elongation of the Polymethine Chain in Cyanine Dyes Alters the Pharmacokinetics of a Dual-Modality c[RGDyK] Tracer
- Pharmacokinetics, Biodistribution, and Radiation Dosimetry for 89Zr-Trastuzumab in Patients with Esophagogastric Cancer
- 89Zr-Lumretuzumab PET Imaging before and during HER3 Antibody Lumretuzumab Treatment in Patients with Solid Tumors
- The Use of Microdosing in the Development of Small Organic and Protein Therapeutics
- 89Zr-Bevacizumab PET: Potential Early Indicator of Everolimus Efficacy in Patients with Metastatic Renal Cell Carcinoma
- Tumor-Specific Uptake of Fluorescent Bevacizumab-IRDye800CW Microdosing in Patients with Primary Breast Cancer: A Phase I Feasibility Study
- 89Zr-Bevacizumab PET Visualizes Disease Manifestations in Patients with von Hippel-Lindau Disease
- ImmunoPET with Anti-Mesothelin Antibody in Patients with Pancreatic and Ovarian Cancer before Anti-Mesothelin Antibody-Drug Conjugate Treatment
- The Use of Novel PET Tracers to Image Breast Cancer Biologic Processes Such as Proliferation, DNA Damage and Repair, and Angiogenesis
- ADAPT, a Novel Scaffold Protein-Based Probe for Radionuclide Imaging of Molecular Targets That Are Expressed in Disseminated Cancers
- Antibody Positron Emission Tomography Imaging in Anticancer Drug Development
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- 89Zr-Bevacizumab PET Visualizes Heterogeneous Tracer Accumulation in Tumor Lesions of Renal Cell Carcinoma Patients and Differential Effects of Antiangiogenic Treatment
- A Modular Labeling Strategy for In Vivo PET and Near-Infrared Fluorescence Imaging of Nanoparticle Tumor Targeting
- 89Zr-trastuzumab and 89Zr-bevacizumab PET to Evaluate the Effect of the HSP90 Inhibitor NVP-AUY922 in Metastatic Breast Cancer Patients
- Everolimus Reduces 89Zr-Bevacizumab Tumor Uptake in Patients with Neuroendocrine Tumors
- Development of a Radiolabeled Irreversible Peptide Ligand for PET Imaging of Vascular Endothelial Growth Factor
- Glypican-3-Targeted 89Zr PET Imaging of Hepatocellular Carcinoma: Where Antibody Imaging Dares to Tread
- CNS Metastases in Breast Cancer: Old Challenge, New Frontiers