


Abstract
Trastuzumab with chemotherapy improves clinical outcomes in patients with human epidermal growth factor receptor 2 (HER2)–positive esophagogastric adenocarcinoma (EGA). Despite the therapeutic benefit, responses are rarely complete, and most patients develop progression. To our knowledge, this is the first report evaluating 89Zr-trastuzumab in HER2-positive EGA; here, we evaluate the safety, pharmacokinetics, biodistribution, and dosimetry 89Zr-trastuzumab. Methods: Trastuzumab was conjugated with deferoxamine and radiolabeled with 89Zr. A mean activity of 184 MBq was administered to 10 patients with metastatic HER2-positive EGA. PET imaging, whole-body probe counts, and blood draws were performed to assess pharmacokinetics, biodistribution, and dosimetry. Results: No clinically significant toxicities were observed. At the end of infusion, the estimated 89Zr-trastuzumab in plasma volume was a median 102% (range, 78%–113%) of the injected dose. The median biologic half-life T1/2β was 111 h (range, 78–193 h). The median biologic whole-body retention half-life was 370 h (range, 257–578 h). PET images showed optimal tumor visualization at 5–8 d after injection. The maximum tumor SUV ranged from no to minimal uptake in 3 patients to a median of 6.8 (range, 2.9–22.7) for 20 lesions in 7 patients. Dosimetry estimates from OLINDA showed that the organs receiving the highest absorbed doses were the liver and heart wall, with median values of 1.37 and 1.12 mGy/MBq, respectively. Conclusion: 89Zr-trastuzumab imaging tracer is safe and provides high-quality images in patients with HER2-positive EGA, with an optimal imaging time of 5–8 d after injection.
Gastric cancer is the fifth most common malignancy and among the leading causes of cancer death in the world (1). Human epidermal growth factor receptor 2 (HER2) is a transmembrane receptor that is overexpressed in approximately 20% of esophagogastric adenocarcinoma (EGAs) (2). Trastuzumab, an anti-HER2 monoclonal antibody, is the first Food and Drug Administration–approved targeted agent to treat patients with EGA that overexpresses HER2 (3). However, not all patients with HER2-positive EGA respond to trastuzumab (4). Furthermore, duration of response to trastuzumab-containing therapy is only 6.7 mo, and the basis of resistance in EGA is an area of investigation.
In patients with HER2 expression in tumors, the heterogeneity of HER2 expression within primary tumors and metastases as well as loss of HER2 expression while undergoing trastuzumab therapy are some factors that have been shown to contribute to therapeutic resistance (5). Furthermore, the extent of disease burden and presence of the primary tumor in the stomach has been shown to affect absorption, pharmacokinetics, and efficacy of trastuzumab and lapatinib (oral anti-HER2 tyrosine kinase inhibitor). An imaging agent that can noninvasively assess HER2 status and reflect functional effects of HER2-targeted agents in the primary tumor and metastases would help to elucidate these factors. Using 89Zr-trastuzumab in gastric cancer xenografts, we demonstrated that 89Zr-trastuzumab PET could delineate HER2-positive tumors and measure the pharmacodynamic effects of anti-HER2 therapy (6).
Previous reports with 89Zr-trastuzumab have focused on its ability to detect breast cancer (7), determine HER2 tumor heterogeneity (8), and identify patients likely to respond to HER2-directed treatments (9,10). Limited information is available on the pharmacokinetics and dosimetry of 89Zr-labeled antibodies in general (9–17), and no detailed data on the pharmacokinetics of 89Zr-trastuzumab have been published in peer-reviewed literature. Only recently has there been a report of 89Zr-trastuzumab dosimetry in breast cancer (18). To our knowledge, this is the first report evaluating 89Zr-trastuzumab in HER2-positive EGA; here, we evaluate the safety, pharmacokinetics, biodistribution, and dosimetry of 89Zr-trastuzumab.
MATERIALS AND METHODS
Patients
Eligible patients had a diagnosis of HER2-positive metastatic EGA. Other eligibility criteria included measurable or evaluable disease by RECIST (version 1.1), Karnofsky performance of 60% or greater, and adequate organ function. Exclusion criteria included ejection fraction of less than 50% and known hypersensitivity to trastuzumab. For patients receiving trastuzumab, a washout period of at least 14 d was recommended.
Study Design and Cohorts
This was a single-site, prospective open-label imaging protocol. The study was approved by the institutional review board and ethics committees at Memorial Sloan Kettering Cancer Center (MSK) (ClinicalTrials.gov identifier NCT02023996). All patients provided written informed consent. We report the results from the completed cohort 1, of 10 patients who underwent serial 89Zr-trastuzumab PET imaging (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org) to determine safety, biodistribution, pharmacokinetics, and dosimetry.
89Zr-Trastuzumab Drug Product
The 89Zr-trastuzumab was manufactured by the MSK Radiochemistry and Molecular Imaging Probes Core Facility in compliance with a Food and Drug Administration investigational new drug application. Clinical-grade trastuzumab (Herceptin; Genentech) was conjugated with p-SCN-Bn-deferoxamine (Macrocylics) chelator, followed by radiolabeling with 89Zr, a positron emitter with a 78.4-h half-life. The conjugation was performed using methodology previously described (19). The chelate-to-trastuzumab ratio was 1.03, as determined by the radioisotopic dilution method, with an antibody concentration of 10.6 mg/mL, determined by ultraviolet-visible spectroscopy, and antibody monomer content of 100%, determined by size-exclusion chromatography high-performance liquid chromatography. 89Zr-oxalate was also prepared in-house as previously described (20) and used to radiolabel desferrioxamine-trastuzumab as previously described (19,20). The 89Zr-trastuzumab final product had a radiochemical purity of more than 95%, endotoxin content of less than 5 EU/mL, and pH of 5.5–8.0 and was sterile. The median immunoreactivity was 94% (range, 86%–97%) (21).
Patient unit doses of approximately 185 MBq/3 mg of 89Zr-trastuzumab were mixed with nonradiolabeled trastuzumab to achieve a total mass of 50 mg. The total antibody mass of 50 mg was selected on the basis of the literature experience (7). A mean of 184 MBq (range, 182–189 MBq) was injected intravenously over approximately 5 min. Patients were monitored for 2 h after injection, and any adverse effects were graded using Common Terminology Criteria for Adverse Events (version 4).
Imaging
All patients underwent dedicated CT imaging as a reference standard a median of 9 d before (range, 29 d before or 3 d after) 89Zr-trastuzumab injection. Each patient underwent serial whole-body PET/CT scans from mid skull to proximal thigh. All scans were obtained on a Discovery STE PET/CT scanner (GE Healthcare) in 3-dimensional mode with attenuation, scatter, and other standard corrections applied and using iterative reconstruction. Images were acquired within 4 h of injection and at 1, 2–4, and 5–8 d after injection using 3, 4, 5, and 7–8 min per bed position, respectively. Low-dose CT scans were used for attenuation correction using an x-ray tube current of 10–80 mA.
Images were read by an experienced nuclear medicine physician who was aware of the patient’s history and conventional imaging. Localization in the tumor was defined as focal accumulation greater than adjacent background in areas in which physiologic activity was not expected. Volumes of interest were drawn on PET/CT images over normal liver, kidney, spleen, bone marrow, and lung using a dedicated workstation (Hermes Medical Solution or GE Healthcare AW server 2.0) and over selected tumor lesions confirmed on CT or 18F-FDG PET. SUVs normalized to lean body mass (SUVLBM) were determined.
Whole-Body and Serum Clearance Measurements
Whole-body clearance was determined by serial measurements of counting rate using a 12.7-cm-thick NaI(Tl) scintillation detector at a fixed 3 m from the patient. Background-corrected geometric mean counts were obtained after infusion and before first voiding, immediately after first voiding, and subsequently at the times of the PET scans. Counting rates were normalized to the immediate postinfusion value (taken as 100%) to yield relative retained activities (in %).
Blood samples were obtained at approximately 5, 15, 30, and 60 min and 2 h after injection and on subsequent days of each PET scan (n = 8). Aliquots of serum were counted using a well-type detector (Wallac Wizard 1480 γ-counter; Perkin Elmer). The measured activity concentrations were converted to percentage injected activity per liter.
The whole-body probe data and the serum activity concentration data were fit with monoexponential or biexponential functions using SAAM software (22). These data were used to determine cumulated activity per unit administered activity (i.e., residence time) for whole-body and serum. Serum data were also used to determine pharmacokinetic parameters, including concentration at 0 time, median biologic half-life T1/2β, volume of distribution of central compartment, area under the curve (AUC), and systemic clearance. The total percentage injected activity initially present in the serum was estimated by multiplying the percentage injected activity per liter in serum at concentration at 0 time by the patient’s estimated plasma volume determined from a nomogram (23).
Normal-Tissue Dosimetry
Image-derived SUVLBM were converted to activity concentration per unit mass (kBq/g). The AUCs were estimated by trapezoidal integration with the contribution of the terminal portion calculated by extrapolation from the last measured value using the faster of apparent terminal clearance rate or physical decay. Subsequently, whole-organ AUCs were estimated by multiplying the activity concentration AUC by organ mass and residence time derived by dividing the AUC by injected activity. Values of standard male/female organ masses were taken from the OLINDA/EXM software (24). If the actual body mass was more than 15% greater than the standard value, organ masses were rescaled. The assigned patient mass was the minimum of actual patient mass or a calculated maximum effective mass as previously described (25).
The residence time for cardiac contents was calculated by multiplying the serum value (in h/L) by the standard or patient mass–rescaled value of heart contents volume and by (1−measured hematocrit). The residence time for red marrow was calculated as described by Sgouros et al. (26). The residence time for the remainder of the body was derived by subtracting all the individually estimated residence times for normal organs from the whole-body residence time. Absorbed radiation doses to various normal organs were estimated using OLINDA/EXM software.
Statistics
Descriptive statistics include median or mean and SD. Comparison between groups was done using the paired t test. Statistical analysis was performed with SigmaStat 3.5 (Systat Software Inc.).
RESULTS
Patients
Ten consecutive patients with histologically documented EGA were imaged (esophageal, n = 2; gastroesophageal junction, n = 7; and gastric, n = 1). Tumors were HER2-positive based on immunohistochemistry 3+ (n = 8) or 2+ with fluorescence in situ hybridization (FISH) amplification (n = 2). Their median age was 62 y (age range, 46–80 y); 8 were men and 2 women. Patients either were trastuzumab-naïve (n = 3) or were no longer being treated with trastuzumab for a median of 42 d (range, 35–156 d) with the exception of patient 5, who received trastuzumab within 15 d before 89Zr-trastuzumab.
Adverse Events
Two patients reported grade 1 chills during injection that resolved after diphenhydramine and acetaminophen. One patient had chills that did not require treatment, possibly related to 89Zr-trastuzumab administration. No other related adverse events were reported.
Pharmacokinetics
The pharmacokinetic parameters for 89Zr-trastuzumab are shown in Table 1. At the end of infusion, the estimated total activity in serum was a median of 102% (range, 78%–113%) of the injected dose, determined by multiplying the patients’ estimated plasma volume by the concentration in serum at the initial sampling time point. The serum volume of distribution of the central compartment was within a median of 3% (range, −10%–28%) of the estimated plasma volume. The median biologic T1/2β was 111 h (range, 78–193 h) (Supplemental Fig. 2A).
Pharmacokinetic Parameters for 89Zr-Trastuzumab
Biodistribution
Whole-body retention of activity was prolonged, with a median biologic half-time of 370 h (range, 257–578 h), as shown in Supplemental Figure 2B. Excretion in the urine in the first 1.7 h (range, 1.1–2.5 h) was minimal, with a median of 1.6% (range, −1.0%–7.6%). Whole-body excretion over a median of 120 h (range, 115–191 h) was a median of 21.3% (range, 16.7%–30.0%). In 7 of 10 patients, the gallbladder was visualized in the day-of-injection image but seldom in subsequent images. All patients had bowel visualization that moved over time, consistent with intraluminal content. Exactly how much of the total excretion was urinary versus bowel was not determined; however, bowel appeared to be the predominant route of excretion based on visual inspection.
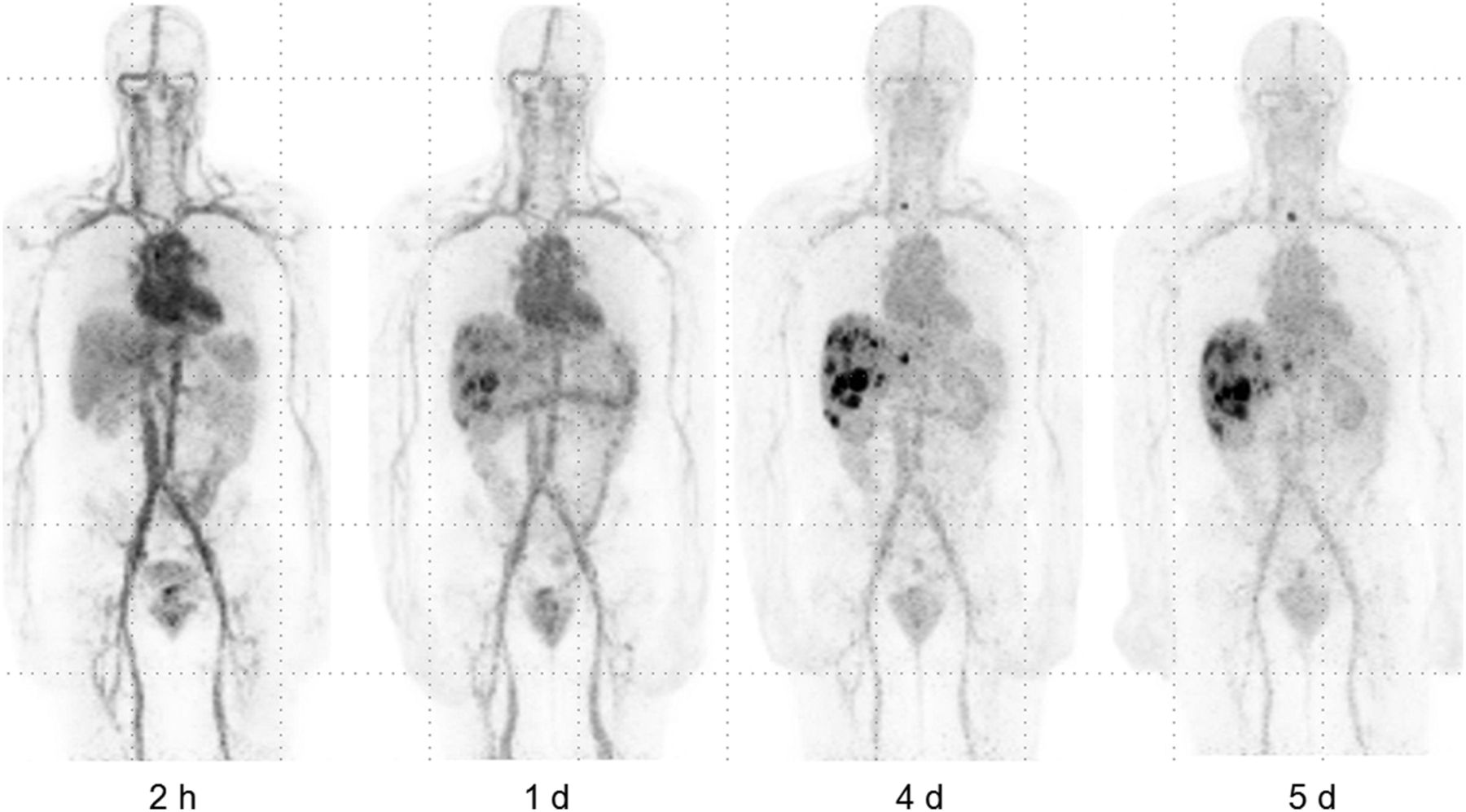
Optimal tumor visualization was generally obtained at the last imaging time point (5–8 d after injection), when most lesions were observed with the best contrast based on visual assessment by an expert reader and with the highest or near-highest SUVLBM-max (Fig. 1). The initial image primarily showed blood pool and rarely any tumor lesions. Tumor uptake typically increased over time, with the highest uptake most often seen at the last time point (Fig. 2). The highest tumor SUVLBM-max observed ranged from no uptake in any lesion in 2 patients to a median SUVLBM-max of 6.8 (range, 2.9–22.7) for 20 lesions in 7 patients with positive scan results, imaged between 115 and 191 h after administration. The time course of normal-organ uptake is shown in Figure 3A. The uptake in liver was relatively low and stable over time as was kidney (with the exception of the last time point representing a single patient). The uptake decreased continuously in the blood pool, lung, and spleen. A slight increase in organ-to-blood ratio was observed for liver, kidney, and bone marrow (Fig. 3B).

Patient 10 with EGA cancer metastatic to liver. Serial maximum-intensity-projection images are shown, after injection of 182.8 MBq of 89Zr-trastuzumab. All images are of good quality up to 5 d after injection (images set to same gray scale). Immediate postinjection images do not show tumor uptake. Images at 1 d after injection show uptake in metastatic liver lesions that increases over time and is well identified at 4 and 5 d after injection with SUVLBM-max of 22.7. Foci in upper mediastinal nodes are best seen at 5 d after injection. Blood-pool activity decreases over time. Activity in bowel is present at all time points. Minimal or no activity is seen in urinary bladder.
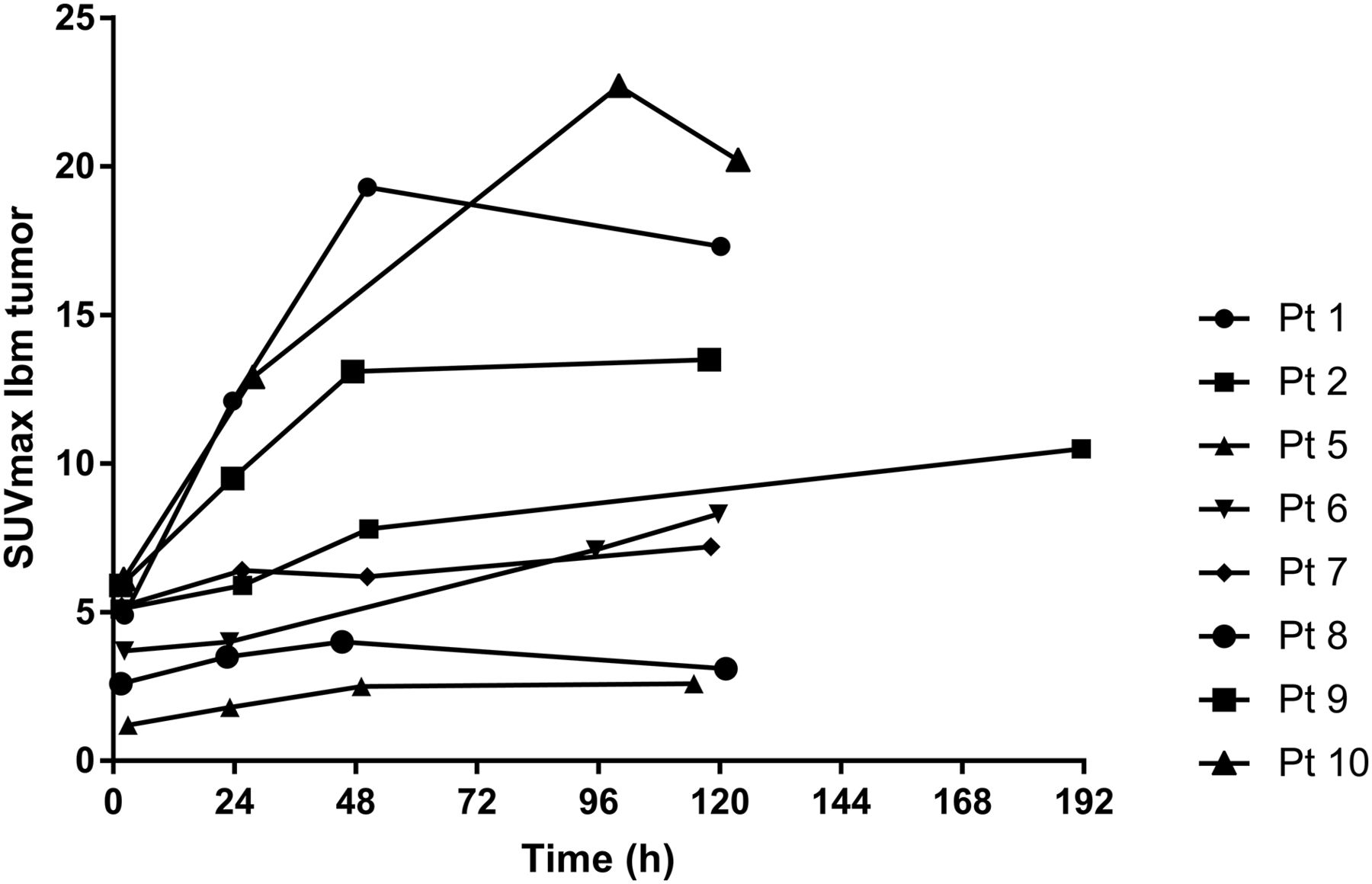
Volume of interest drawn over tumor lesions with highest uptake (SUVLBM-max [8 patients], with 89Zr-trastuzumab uptake usually increasing over time with highest SUVLBM-max typically at >48 h after injection).

(A) SUVLBM was determined by placing volume of interest over various organs and was averaged over all available time points (n = 10 for 2 h and 24 h, n = 9 for 48 h, n = 2 for 96 h, n = 10 for 120 h, and n = 1 for 192 h). SUVs were fairly stable over time for bone marrow, liver, and kidney, except for last time point. Slight decrease in SUVLBM was noted for spleen and lung, as was larger decrease in activity in blood. (B) Organ–to–blood-pool ratios showed fairly stable changes for spleen and lung over time, suggesting no concentration above blood pool. In contrast, liver, kidney, and bone marrow showed slight increase over time, suggesting some 89Zr accumulation in these organs.
Tumor Imaging
In 80% of imaged patients, accumulation of 89Zr-trastuzumab tracer was noted in sites of known disease. Focal areas of 89Zr-trastuzumab uptake were seen within known metastatic sites in the liver, lymph nodes, lung, and bone as well as remaining primary. No uptake was seen in 2 patients on 89Zr-trastuzumab PET. In patient 4, this was likely due to weak HER2 staining (immunohistochemistry 2+/FISH HER2/CEP17 3.4) and focal HER2 expression. In patient 3 with prior gastrectomy, whose primary tumor and biopsy-proven lung metastasis exhibited strong HER2 expression (immunohistochemistry 3+), 89Zr-trastuzumab PET failed to pick up small-volume recurrent disease in a 1.1 × 1.1 cm lung nodule and 1.9 × 1.3 cm retroperitoneal lymph node that were visualized on CT. The retroperitoneal lymph nodes were never biopsied or tested for HER2 overexpression. Patient 8 with very low uptake in bone lesions and no uptake in liver and nodal lesions was receiving chemotherapy at the time of imaging. Heterogeneity of tumor uptake within patients is shown in Supplemental Table 1, along with last trastuzumab therapy since this treatment may compete for tumor uptake.
Absorbed Dose to Normal Organs
The dosimetry estimates from OLINDA are shown in Table 2, indicating that the organs receiving the highest absorbed doses were liver, heart wall, kidney, lung, and spleen with mean values of 1.32, 1.12, 0.9, 0.81, and 0.8 mGy/MBq, respectively. The mean effective dose was 0.48 mSv/MBq.
Normal-Organ Absorbed Doses for 89Zr-Trastuzumab
DISCUSSION
Our data demonstrate for the first time that 89Zr-trastuzumab PET is specific for HER2-positive EGA and visualizes primary tumors and metastases with high contrast. Similar findings have been described previously in patients with breast cancer (7–10,18). 89Zr-trastuzumab PET has a potential advantage over single-site biopsies, as it can noninvasively assess variation in level of HER2 and target engagement in both the primary tumor and all sites of metastases simultaneously. 89Zr trastuzumab PET has already been used as a biomarker in the theranostic setting for breast cancer patients treated with trastuzumab emtansine antibody drug conjugate. In that setting, combining 89Zr-trastuzumab and 18F-FDG PET predicted response to treatment with trastuzumab emtansine (10). In addition, early changes in 89Zr-trastuzumab uptake in breast cancer metastasis after treatment with heat shock protein 90 inhibitor have correlated with CT changes in the size of lesions (9). Last, a preliminary report has suggested that breast cancer patients with prior HER2-negative biopsies may be identified as HER2-positive on imaging and selected for therapeutic intervention that they would not otherwise receive (8).
In this study, the biodistribution and imaging of 89Zr-trastuzumab in patients with EGA appeared visually similar to those in patients with metastatic breast cancer (7,8,18). Recent analysis of 89Zr-trastuzumab biodistribution in normal organs of women with breast cancer has been expressed as percentage injected dose (18), when our data in SUVLBM are converted to percentage injected dose using standard man body weight and organ volumes; we obtained uptake values in the same range (data not shown). A prior study with 89Zr-cmAb-U36 antibody in head and neck cancer (12) showed similar biodistribution and percentage injected dose in the liver, spleen, and kidney as previously described in breast cancer patients (18). In contrast, some antibodies have higher concentration in organs such as the liver (15,17,27) or spleen (16), which is probably due to cross-reactivity with antigen in these organs or the mass amount of antibody used. In our study, the uptake in the liver, kidney, and bone marrow showed little increase over time (Fig. 3A). When the ratios of these organs to blood pool was determined, there was evidence of slight accumulation of 89Zr above blood pool in the liver, kidney, and bone marrow (Fig. 3B), whereas the ratios in lung and spleen were flat, suggesting no concentration above blood pool (Fig. 3B).
Our dosimetric findings predominantly in men are in line with those described for 89Zr-trastuzumab in women, in whom the maximal absorbed dose was to the liver, kidney, spleen, and lung (18). Interestingly, for the few other 89Zr-labeled antibodies, the dosimetry in most normal organs is in the same range as for 89Zr-trastuzumab. The effective dose in our study of 0.48 mGy/MBq was comparable to 0.53, 0.36, 0.41, 0.61, and 0.41 mGy/MBq for cmAB-U36, hJ591, IAB2 M minibody, cetuximab, and rituximab antibodies, respectively (12,15–17,27). The major difference in organ dosimetry for these 89Zr-labeled antibodies is in the liver and spleen when antibodies cross-reacted with these tissues (15,16). It is possible that changing the mass of antibody administered (or if recent trastuzumab was administered) could result in not only differences in tumor targeting but also differences in biodistribution and dosimetry. This effect of antibody mass in organ dosimetry has been demonstrated with rituximab, where a preinjection of cold antibody will significantly decrease the dose to the spleen by blocking uptake (0.73 vs. 4.1 mSv/MBq).
We have previously reported that while localization can be achieved with shorter-lived positron-labeled 68Ga- or 64Cu-trastuzumab, their targeting is suboptimal (28,29), given the biologic half-life of intact antibody in the circulation for 89Zr-trastuzumab in this study (111 h). In our study, we concluded that the 5- to 8-d point offered the best imaging, similar to previous studies (7,18). Similar conclusions regarding optimal delayed imaging time with other 89Zr-labeled intact antibodies have been reported (12,17). Although studies have shown targeting of 111In-labeled trastuzumab (30), the advantage of 89Zr-trastuzumab is its ability to perform quantitative imaging with PET and the higher sensitivity and resolution of PET compared with single-photon emission tomography with 111In.
In this study, we administered approximately 185 MBq, resulting in good images even at 5–8 d after administration. Others have used approximately 37 MBq successfully, although they have pointed out limitations in imaging and defining volume of interest for delayed scans, especially in large patients and delayed times (7,12,14). Studies with 89Zr-trastuzumab using 62 MBq showed that delayed imaging could be adequately performed. On the basis of visual data from our images and prior reports, we believe that we will be able to decrease the administered activity significantly from 185 MBq and still obtain adequate images in patients with EGA (7,18).
Adverse events from 89Zr-trastuzumab administration were minor and similar to that observed previously with other 89Zr-labeled antibodies, for which grade 1 infusion reactions have been observed (9,12,17,27).
CONCLUSION
The current study demonstrates the feasibility of using 89Zr-trastuzumab to localize HER2-positive gastric cancer, raising the potential of using this reagent to select or identify patients with gastric cancer who are likely to respond to HER2-directed treatment. Additional patient accrual is ongoing to further categorize the heterogeneity of uptake and correlate imaging findings with response to HER2-directed therapies.
DISCLOSURE
Financial support for this study was provided by Mr. William H. and Mrs. Alice Goodwin and the Commonwealth Foundation for Cancer Research, The Center for Experimental Therapeutics of MSK, the Radiochemistry & Molecular Imaging Probes Core (NIH/NCI Cancer Center Support Grant P30 CA008748), the Ludwig Center for Cancer Immunotherapy at MSK, the Conquer Cancer Foundation (Career Development Award, to Yelena Y. Janjigian), the Department of Defense Congressionally Directed Medical Research Program (CA 150646, to Yelena Y. Janjigian, Jason S. Lewis, and Wolfgang A. Weber), and the Geoffrey Beene Cancer Research Center at MSK (to Jason S. Lewis). Yelena Y. Janjigian has received funding, or has pending grants or patents, from Boehringer Ingelheim, Bayer, Genentech, Bristol-Myers Squibb, Eli Lilly, Pfizer, and Merck. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Jing Qiao, Ariel Brown, and staff of the MSK Radiochemistry and Molecular Imaging Probe Core for labeling and dispensing the antibody. We also thank Rashid Ghani of the Nuclear Medicine Pharmacy, the Nuclear Medicine nurses Amabelle Lindo and Louise Harris for their help in patient management, RSA Abigail Boswell and CRM Bolorsukh Gansukh for their excellent support with patient flow and protocol management, the nuclear medicine technologists for their excellent technical assistance, and members of the Department of Medicine at MSK for patient referral. We thank Leah Bassity for her helpful suggestions in editing this manuscript and its submission to the journal.
Footnotes
↵* Contributed equally to this work.
Published online Jun. 21, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 7, 2017.
- Accepted for publication June 8, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Detection of HER2-Low Lesions Using HER2-Targeted PET Imaging in Patients with Metastatic Breast Cancer: A Paired HER2 PET and Tumor Biopsy Analysis
- 18F-BMS-986229 PET to Assess Programmed-Death Ligand 1 Status in Gastroesophageal Cancer
- First-in-Human Evaluation of Site-Specifically Labeled 89Zr-Pertuzumab in Patients with HER2-Positive Breast Cancer
- Immuno-PET and Targeted {alpha}-Therapy Using Anti-Glypican-1 Antibody Labeled with 89Zr or 211At: A Theranostic Approach for Pancreatic Ductal Adenocarcinoma
- Noninvasive Assessment of Human Epidermal Growth Factor Receptor 2 (HER2) in Esophagogastric Cancer Using 89Zr-Trastuzumab PET: A Pilot Study
- Click-to-Release: Cleavable Radioimmunoimaging with 89Zr-DFO-Trans-Cyclooctene-Trastuzumab Increases Tumor-to-Blood Ratio
- Preclinical Evaluation of 89Zr-Desferrioxamine-Bexmarilimab, a Humanized Antibody Against Common Lymphatic Endothelial and Vascular Endothelial Receptor-1, in a Rabbit Model of Renal Fibrosis
- Use of 64Cu-DOTA-Trastuzumab PET to Predict Response and Outcome of Patients Receiving Trastuzumab Emtansine for Metastatic Breast Cancer: A Pilot Study
- Influence of Fc Modifications and IgG Subclass on Biodistribution of Humanized Antibodies Targeting L1CAM
- 11C Dosimetry Scans Should Be Abandoned
- Towards integration of 64Cu-DOTA-Trasztusumab PET-CT and MRI with mathematical modeling to predict response to neoadjuvant therapy in HER2+ breast cancer
- Retooling a Blood-Based Biomarker: Phase I Assessment of the High-Affinity CA19-9 Antibody HuMab-5B1 for Immuno-PET Imaging of Pancreatic Cancer
- 89Zr-Immuno-PET: Toward a Noninvasive Clinical Tool to Measure Target Engagement of Therapeutic Antibodies In Vivo
- EGFR and MET Amplifications Determine Response to HER2 Inhibition in ERBB2-Amplified Esophagogastric Cancer
- PET Imaging of Receptor Tyrosine Kinases in Cancer
- First-in-Human Human Epidermal Growth Factor Receptor 2-Targeted Imaging Using 89Zr-Pertuzumab PET/CT: Dosimetry and Clinical Application in Patients with Breast Cancer