


Abstract
In murine models, resection of a primary tumor leads to increased vascularization and accelerated growth of metastases that previously had remained microscopic. To study such a potentially inhibitory effect of primary tumors on the outgrowth of distant metastases in humans, we assessed the metabolic activity of liver metastases by 18F-FDG PET before and after resection of primary colorectal tumors. Methods: Group A consisted of 8 patients with synchronous colorectal liver metastases who were scheduled for resection of their primary tumor. These patients underwent an 18F-FDG PET scan shortly before resection and 2–3 wk after resection of the primary tumor. The patients in a control group (group B, n = 9) underwent an 18F-FDG PET scan at the time of diagnosis of the liver metastases and a second scan several weeks later, before initiating treatment. There was no surgical intervention between the two 18F-FDG PET scans in this group. Results: In group A, the maximum and mean standardized uptake values of the liver metastases clearly increased after resection of the primary tumor, by 38% ± 55% and 42% ± 52%, respectively, as compared with the first 18F-FDG PET scan. In group B, the maximum and mean standardized uptake values of the second 18F-FDG PET scan were not significantly higher than those of the first 18F-FDG PET scan; −11% ± 23% and 1% ± 29%, respectively. The difference in standardized uptake value increase between the 2 groups was statistically significant (P < 0.05). Conclusion: Our data cannot differentiate between the immunologic sequels caused by the surgical trauma itself and those caused by removal of the primary tumor. The observation itself, however, of increased metabolic activity after surgical resection of the primary tumor may have direct clinical applications and suggests the administration of antiangiogenic therapy after surgery of the primary tumor.
Recently, it was reported that the growth rate of liver metastases in patients in whom the primary colorectal tumor had been resected was significantly higher than the growth rate of liver metastases in patients in whom the primary tumor was still in situ (1,2). In addition, immunohistochemical analysis revealed an increased proliferation rate and increased vessel density in the metastases in the absence of the primary tumor. These data suggest that outgrowth of metastatic disease may partly be controlled by the primary tumor (3).
In animal models, primary tumor–mediated inhibition of metastatic vascularization and outgrowth is an established concept in tumor biology. Research in this area was initiated by the observation that in the Lewis lung carcinoma mouse model, resection of the primary tumor led to increased vascularization and accelerated growth of distant metastases that had previously remained microscopic. O'Reilly et al. demonstrated in a murine model that the primary tumor produced the potent antiangiogenic compound angiostatin, which prevented vascularization and thereby growth of metastases (4). More recently, it was demonstrated that irradiation of murine angiostatin-producing primary tumors was followed by subsequent rapid growth of the metastases, suggesting a similar phenomenon (5,6). Moreover, when angiostatin was replaced immediately after regression of the primary tumor, outgrowth of the metastases did not occur (5).
18F-FDG PET depicts tumors by identifying cells in the body that have increased glucose uptake and metabolism. 18F-FDG is transported into cells analogously to glucose and is converted into 18F-FDG-6-phosphate. This metabolite is trapped in the cell, because it is processed in the glycolytic pathway and hence accumulates preferentially in those cells with enhanced glucose uptake, such as tumor cells. Glucose metabolism can be measured mathematically using the standardized uptake value (SUV), a semiquantitative measure of 18F-FDG uptake. It has been demonstrated that the extent of 18F-FDG uptake in colorectal cancer metastases correlates with disease aggressiveness and prognosis (7). So, metabolic activity of the metastases as measured by 18F-FDG PET before and after resection of the primary tumor may indeed reflect the growth rate of the metastases.
In humans, the possible inhibitory effect of the primary tumor on the proliferation of distant metastases has not been studied in detail. To study the inhibitory effect of the primary tumor on the outgrowth of distant metastases in humans, we assessed the metabolic activity of liver metastases by 18F-FDG PET before and after resection of the primary colorectal tumor and compared the results with a control group who underwent 2 serial 18F-FDG PET scans without any surgical intervention.
MATERIALS AND METHODS
Patients
A total of 21 patients with colorectal liver metastases and no prior chemotherapy during the last 6 mo were potentially eligible for the study. Patients were prospectively included after they had given informed consent. The study was approved by the Institutional Review Board of the Radboud University Nijmegen Medical Centre. The presence of liver metastases was histologically confirmed in 10 patients (mainly patients from group B). In the other 11 patients, the presence of liver metastases was, apart from 18F-FDG PET, also determined by ultrasonography (n = 5) and CT (n = 7). Patients in whom most metastatic lesions showed SUVs greater than 10 at the initial 18F-FDG PET scan were excluded from the study (n = 3) because it has been recognized that liver metastases with high initial 18F-FDG uptake grow quickly and tend to develop central necrosis. The development of these necrotic areas makes serial 18F-FDG PET quantification unreliable because of reduced 18F-FDG uptake in partial necrosis and absence of 18F-FDG uptake in necrosis. (8) Another patient was excluded because a second liver metastasis developed just adjacent to the first metastasis, making measurement of separate SUVs impossible.
Two groups of patients were analyzed (Table 1). Group A consisted of patients who presented with primary colorectal cancer and synchronous liver metastases, scheduled for resection of the primary tumor (n = 8). 18F-FDG PET was performed shortly before (mean, 14 d; range, 3–36 d) and 2–3 wk after resection of the colorectal primary tumor. Group B consisted of patients with colorectal liver metastases in whom the primary tumor had been resected at least 6 mo earlier (n = 7) or with the primary tumor in situ without being scheduled for primary resection (n = 2). In this group, the multidisciplinary team decided to adopt a wait-and-see policy for some time before a definite decision was made to further treat the colorectal liver metastases. In this group, serial 18F-FDG PET was performed without any surgical or medical intervention in between. Eventually, patients in group B were scheduled for either hepatic resection (n = 6) or further systemic chemotherapy (n = 3) after both 18F-FDG PET scans.
Results of Group Analysis
18F-FDG PET
A dedicated PET/CT scanner (ECAT-EXACT or Biograph PET/CT; Siemens/CTI) was used for data acquisition. Before 18F-FDG injection, patients fasted for at least 6 h. Intake of sugar-free liquids was permitted. One hour after intravenous injection of 200–220 MBq of 18F-FDG (Mallinckrodt Medical), emission and transmission images of the area between the upper part of the femora and the base of the skull were acquired. The images were corrected for attenuation and reconstructed using ordered-subsets expectation maximization.
To determine the metabolic activity of the liver metastases, an experienced nuclear physician who was unaware of the time point of 18F-FDG PET drew volumes of interest around all metastases. For this procedure, an automatic 50% isocontour (ECAT software tool) was used, enclosing pixels with 50% or more of the maximum radioactivity within the volume of interest. Mean SUV (50% isocontour) and maximum SUV (SUVmax) were calculated using the concentration of 18F-FDG in the volume of interest as measured by PET, divided by the injected dose and multiplied by body weight as a normalization factor. For each patient, the mean SUV and SUVmax were determined by calculating the average value of all liver lesions.
Statistical Analysis
SUV measurements were analyzed by independent t tests. Differences were considered statistically significant when P was 0.05 or less. Data are presented as mean values ± SDs.
RESULTS
Patient data and tumor characteristics are summarized in Table 1. Age, sex, N stage of the primary tumor, and size of the metastases were similar for both groups. The number of metastases was significantly higher in group B, but initial SUVs, which may reflect possible biologic behavior of the metastases (7), were not statistically different between the 2 groups. On the first 18F-FDG PET at study entry, the mean SUVmax was 7.1 ± 3.2 for group A, and 6.0 ± 2.8 for group B.
The interval between the two 18F-FDG PET scans in patients of group A, who underwent a scan before and after surgery of the primary tumor, was 35 d (range, 21–57 d). The interval between the two 18F-FDG PET scans in patients of group B, who underwent 2 scans without any intervention, was 69 d (range, 19–126 d).
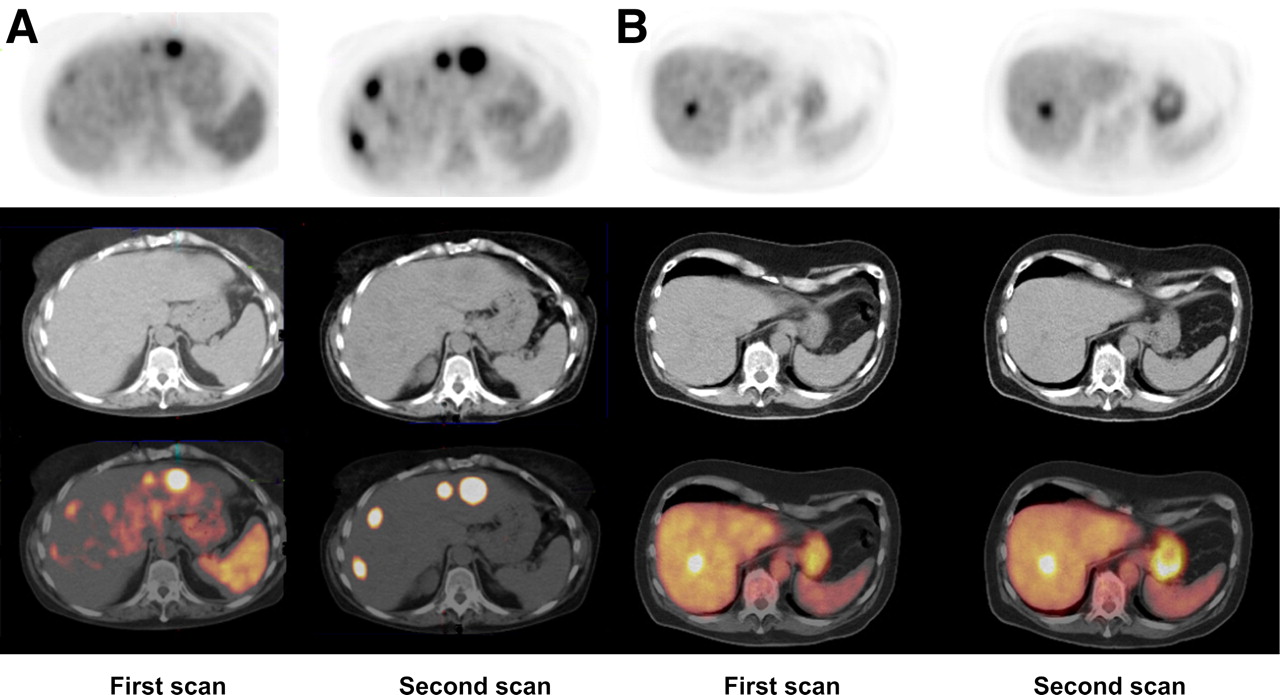
The SUV was measured for only those metastatic lesions that could clearly be identified as separate. The average SUVmax at baseline and the average SUVmax at follow-up is shown in Table 2 for all patients. As mentioned earlier, patients in whom most of the lesions showed an initial SUVmax of more than 10 were excluded from further analysis. The increase in SUVmax was measured for each lesion, and the average of the changes in SUVmax is shown for each patient. In group A, the SUVmax and mean SUV clearly increased after resection of the primary tumor in 6 of 8 patients (Fig. 1). The mean increase in SUVmax and mean SUV was 38% ± 55% and 42% ± 52%, respectively. In contrast, in group B none of the patients showed a significant difference between the two 18F-FDG PET scans. In this group, the difference in SUVmax and mean SUV was −11% ± 23% and 1% ± 29%, respectively. The difference in SUV increase between the 2 groups was statistically significant for both SUVmax (P = 0.027) and mean SUV (P = 0.048). A typical example of increased 18F-FDG uptake in liver metastases after resection of the primary tumor, as compared with 18F-FDG uptake in 2 subsequent 18F-FDG PET scans in a patient of group B, is shown in Figure 2. No correlation was found when comparing the change in SUVmax with the change in diameter of the lesions. The mean increase in diameter in group A was 9.3%, with an increase in SUVmax of 38%. In contrast, in group B the mean diameter of the metastases showed an increase of 58%, with a decrease in the SUVmax of 11%.

(A) Graph showing major increase in group A SUVmax between 18F-FDG PET before (T1) and after (T2) resection of primary colorectal tumor. (B) Graph showing no significant increase in group B SUVmax during T1-to-T2 interval comparable to that for group A.

(A) 18F-FDG PET scan of patient in group A. Rapid outgrowth of indolent liver metastases occurred after removal of primary colorectal carcinoma. SUVmax of largest lesion was 7.0 on first scan and 12.1 on second scan. (B) 18F-FDG PET scan of patient in group B. 18F-FDG uptake increased slightly between the 2 subsequent PET/CT scans. SUVmax was 7.6 on first scan and 8.3 on second scan.
Data on SUVmax
DISCUSSION
Although only a limited number of patients could be included, our results demonstrated a significant increase in 18F-FDG uptake of colorectal liver metastases after resection of the primary tumor had been observed. In contrast, 18F-FDG uptake in liver metastases remained stable on 2 subsequent 18F-FDG PET scans of patients without any surgical or other therapeutic intervention between the scans.
These results may indicate that in humans, as in animal models, the primary tumor can inhibit growth of its metastases. This inhibitory effect on secondary tumor growth is reversed when the primary tumor is resected. For example, in mice, Li et al. demonstrated increased microvessel density, a higher cell proliferation index of tumor cells, and a decreased apoptotic index after resection of a primary tumor, compared with a sham operation (9).
On the other hand, the increased metabolic activity observed after resection of the primary colorectal tumor may also be caused by the surgical trauma of the resection itself. Surgery alone might stimulate proinflammatory cytokines (IL-6 and IL-1β), resulting in enhanced expression of vascular endothelial growth factor and angiogenesis (10). Our data, as presented in this study, cannot differentiate between the 2 hypotheses. Another explanation for the outgrowth of the metastases could be that the increase in 18F-FDG uptake is caused by mere time-dependent progression and that synchronous liver metastases (group A) would grow faster than metachronous liver metastases (most patients in group B). This explanation, however, is unlikely because initial SUVs in both groups were identical and the interval between the 2 serial 18F-FDG PET scans was even longer in group B than in group A. Furthermore, increased retention of 18F-FDG may be due to an increased size of the lesion; however, our results did not show a correlation between the alteration in tumor size and the change in SUV.
Increased growth of metastases after the removal of a primary tumor has been observed in various animal models and was related to loss of antiangiogenic factors produced by the primary tumor (4,11). The balance between pro- and antiangiogenic factors within the vascular bed of the metastases determines whether the metastases will remain dormant or will proliferate. The dormant state of metastases has been explained by the production of antiangiogenic factors by the primary tumor, such as angiostatin, resulting in inhibition of growth of distant metastases (4). Resection of the primary tumor would interfere with this inhibitory control mechanism, resulting in activation of the angiogenic switch in the metastatic lesions. In patients, this mechanism is supported by earlier findings that vascularization of colorectal liver metastases was significantly increased in the absence of the primary tumor (1). However, data on angiostatin production in patients with colorectal cancer are scarce and indicate at the least that not all primary colorectal tumors may produce angiostatin (12). This indication could also explain why 2 patients in our series did not show an increase in metabolic activity after resection of the primary tumor.
In tumor-bearing animals, vascularization and subsequent growth of distant metastases can be slowed by systemic administration of angiogenesis inhibitors (13–15).
Although the precise mechanism of increased metabolic activity after resection of the primary colorectal tumor as observed in our study still has to be elucidated, slowing of this accelerated growth by angiogenesis inhibitors seems promising. The present approach of serial 18F-FDG PET scans before and after resection of the primary tumor would possibly allow a direct measurement of the therapeutic effect of such antiangiogenic therapy. Such studies might provide insight into the use of adjuvant antiangiogenic agents to prevent accelerated outgrowth of distant metastases after resection of the primary colorectal tumor.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 5, 2007.
- Accepted for publication February 26, 2008.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CapeOX perioperative chemotherapy versus postoperative chemotherapy for locally advanced resectable colon cancer: protocol for a two-period randomised controlled phase III trial
- Reply: Increased Metabolic Activity of Indolent Liver Metastases After Resection of a Primary Colorectal Tumor
- Increased Metabolic Activity of Indolent Liver Metastases After Resection of a Primary Colorectal Tumor