


Abstract
Early identification of chemotherapy-refractory lymphoma patients provides a basis for alternative treatment strategies. Metabolic imaging with 18F-FDG PET offers functional tissue characterization that is useful for assessing response to therapy. Our objective was to determine the predictive value of 18F-FDG PET early during chemotherapy (after 1 cycle) and at the completion of chemotherapy for subsequent progression-free survival (PFS) in patients with aggressive non-Hodgkin’s lymphoma (NHL) or Hodgkin’s disease (HD). Methods: 18F-FDG PET (dual-head coincidence camera with attenuation correction) was performed before and after 1 cycle of chemotherapy on 30 patients (17 NHL, 13 HD; mean age, 52.3 ± 16.0 y). For 23 of the 30 patients, 18F-FDG PET data were also obtained after the completion of chemotherapy. The patients had a median follow-up of 19 mo (range, 18–24 mo). Follow-up of PFS was compared between patients with positive and negative 18F-FDG PET results obtained after the first cycle of chemotherapy and at the completion of chemotherapy. Results: Positive 18F-FDG PET results obtained both after the first cycle and at the completion of therapy were associated with a shorter PFS (median, 5 and 0 mo, respectively) than were negative 18F-FDG PET results (PFS medians not reached). A statistically significant difference in PFS between positive and negative 18F-FDG PET results was obtained both after the first cycle and at the completion of chemotherapy (P ≤ 0.001). The PFS and 18F-FDG PET results obtained after the first cycle correlated better than those obtained after the completion of chemotherapy (r2 = 0.45 vs. 0.17). 18F-FDG PET had more false-negative results after the last cycle (6/17 cases, or 35%) than after the first cycle (2/13 cases, or 15%). Thus, 18F-FDG PET had greater sensitivity and positive predictive values after the first cycle (82% vs. 45.5% and 90% vs. 83%, respectively) than after the last cycle. Conclusion: 18F-FDG PET after 1 cycle of chemotherapy is predictive of 18-mo outcome in patients with aggressive NHL and HD and may earlier identify patients who would benefit from more intensive treatment programs.
Accurate evaluation of response to therapy is of vital importance in the management of patients with lymphoma (1). The main endpoint of chemotherapy is the achievement of complete remission, which is associated with a longer progression-free survival (PFS) and potential cure than is partial remission (2). The definition of complete remission, however, is usually based on anatomic imaging modalities that may be unable to differentiate viable tumor from posttherapy changes such as scarring or fibrosis. Residual abnormalities that occur after therapy are usually considered to represent persistent lymphoma; however, only a maximum of 10%–20% of residual masses was reported to be positive for lymphoma at the completion of treatment (3, 4). Thus, there was no difference in the CT-documented response rates and the size of residual masses between patients who experience disease relapse and those who remain disease free (5–7). Although MRI provides better morphologic details than does CT when contrast material is not used, the low sensitivity rate (45%) showed that MRI was not the ideal tool for predicting clinical outcome (8,9).
67Ga imaging has also been reported to be an independent predictor of outcome after 1–2 cycles of chemotherapy (6,10). Nevertheless, 67Ga imaging is less efficacious than 18F-FDG PET for intraabdominal tumors and may be less sensitive in detecting disease in some instances of aggressive lymphoma or Hodgkin’s disease (HD) (11).
Over the past few years, a large body of evidence has confirmed the potential role of 18F-FDG PET, including both dedicated and coincidence PET systems, in the staging and monitoring of lymphomas (12–16). There is a paucity of data, however, defining the role of 18F-FDG PET at the earliest possible time to predict the response to therapy. Although a change in 18F-FDG uptake at multiple early times during chemotherapy has been described, this change was only marginally predictive of outcome (17). The predictive value of 18F-FDG PET at the completion of chemotherapy has also been evaluated (18). The response after 1 cycle of chemotherapy, however, has not yet been evaluated using 18F-FDG PET in non-Hodgkin’s lymphoma (NHL) and HD. We performed this study to assess the potential of early 18F-FDG PET to predict PFS and ultimate clinical outcome. We also compared the efficacy of 18F-FDG PET performed early with that performed after the completion of chemotherapy in patients with aggressive NHL and HD.
MATERIALS AND METHODS
Between January 1998 and June 2001, 30 consecutive patients (age range, 26–77 y; mean age ± SD, 52.3 ± 16.0 y) with histologically proven aggressive (intermediate or high grade) NHL or HD were prospectively evaluated in this study. Lymphoma was classified histologically according to the International Working Formulation guidelines. NHL was diagnosed in 17 patients (15 intermediate grade [13 cases of diffuse large cell lymphoma and 2 cases of follicular large cell lymphoma] and 2 high grade [lymphoblastic lymphoma]), and HD was diagnosed in 13 patients (Table 1). Seventeen patients were evaluated at initial staging before therapy (10 NHL, 7 HD), and 13 were evaluated at relapse before salvage therapy (6 NHL, 7 HD). In the latter group, the interval between therapy and relapse ranged from 6 mo to 2 y. The patients evaluated at initial staging were categorized into high- and low-risk groups according to the international index established for NHL (19) and the known features indicating a poor prognosis for HD (B symptoms, high sedimentation rate [>30] or large mediastinal adenopathy, older age [>50 y], and 4 or more involved sites). Among 17 patients evaluated at initial staging, 9 had early-stage disease and were at low risk for recurrence (4 NHL, 5 HD) whereas 8 had at least 1 clinical factor for poor prognosis, including advanced-stage disease in 3 patients (6 NHL, 2 HD) (Table 2). All patients underwent contemporaneous CT before therapy and after the completion of chemotherapy. In addition, they underwent a clinical evaluation consisting of physical examination, laboratory screening, chest radiography, CT of the thorax and abdomen, sonography, bone-marrow biopsy (for patients with NHL), and, if indicated, MRI studies. CT scans were also obtained after the last cycle of chemotherapy.
Patient Characteristics
Characteristics of Patients with Relapse and with Poor Prognostic Features vs. Comparative 18F-FDG PET Results
Treatment
All patients underwent chemotherapy according to departmental protocols. All patients with aggressive NHL referred at initial staging received cyclophosphamide, doxorubicin, vincristine, and prednisone or a variant of this protocol every 3 wk for either 6 or 8 cycles. The 7 patients who were referred at relapse received infusional chemotherapy with dexamethasone, ifosfamide, cisplatin, and etoposide every 3 wk. All patients with HD received doxorubicin, bleomycin, vinblastine, and dacarbazine every 2 wk in each monthly cycle for 6 cycles.
18F-FDG PET Coincidence Imaging
All 30 patients underwent a whole-body 18F-FDG PET study before therapy and after the first cycle of chemotherapy. Twenty-three of 30 patients also had 18F-FDG PET studies at the completion of therapy. Coincidence images were obtained using a dual-head gamma camera with attenuation correction (MCD-AC; ADAC Laboratories, Milpitas, CA). The in-plane spatial resolution was 4.8 mm in full width at half maximum at the center of the field of view, with an axial field of view of 38 cm. In the transverse plane, the spatial resolution was constant radially as well as tangentially at any distance from the center to the edge of a transverse slice. In the axial direction, the spatial resolution (full width at half maximum) was approximately twice that of the transverse. All patients fasted at least 4–6 h before the start of the study. Serum glucose level was determined at the time of 18F-FDG injection using a glucometer. All patients had a serum glucose level of <130 mg/dL. Sixty minutes after the intravenous administration of 185 MBq 18F-FDG, a whole-body MCD-AC 18F-FDG PET imaging study consisting of 3 segments (pelvis, abdomen, and chest/neck) was acquired using a matrix size of 128 × 128 × 16, an acquisition time of 40 s per frame, and a scan overlap of 30% in an orbit of 180°. Ten-minute transmission scans were obtained using 153Gd sources after completion of the emission scans for attenuation correction. The images were reconstructed into transverse cross-sectional images by means of an iterative method and a Wiener filter with a cutoff frequency of 0.75 cycle per projection. The data from the whole-body acquisition were stacked in a 3-dimensional volume to allow viewing as a rotating cine display of 48 images as well as transverse or reconstructed coronal or sagittal images.
Data Analysis
Thirty patients after the first cycle of chemotherapy (within 10 d; range, 3–10 d) and 23 patients after the completion of chemotherapy (within 1 mo) were evaluated by a whole-body 18F-FDG PET study. All 18F-FDG PET scans were interpreted by 2 clinical reviewers without any knowledge of the clinical or CT data. All scans were scored either as positive or as negative. A positive result was defined as focal activity relatively higher than that of the surrounding background tissue, with no similar activity seen on the contralateral side, or increased activity in a location incompatible with normal anatomy. A negative result was defined as no pathologic 18F-FDG uptake at any site, including all sites of previously increased pathologic 18F-FDG uptake. 18F-FDG uptake that was equal to the mediastinum for lymph nodes originally located in the mediastinum was considered negative; however, the same intensity of uptake in other locations was considered positive. Before and after therapy, disease was evaluated site by site for the involved lymph nodes.
Patients who underwent both 18F-FDG PET studies (after the first and last cycles) and who either entered the study at relapse or had poor prognostic features at initial staging were categorized into a different subgroup (Table 2) to evaluate the predictive value of 18F-FDG PET when the prognostic factors were not favorable.
PFS was defined as the interval without progression of disease from the start of treatment. Treatment failure was defined as the inability to achieve a complete response, progression of disease, or recurrence of disease after a complete response. The inability to achieve a complete response or PFS was determined by a combination of clinical (residual palpable lymph nodes or other tumors), laboratory (rising lactate dehydrogenase levels or B symptoms), and imaging findings, such as CT findings (lack of resolution of lymphadenopathy or continuously enlarging lymph nodes). The primary aim of this study was to evaluate the role of 18F-FDG PET in predicting PFS after 1 cycle of chemotherapy compared with after the completion of chemotherapy
Statistical Analysis
Statistical analysis was performed using a software package (StatView 5.0; SAS Institute, Cary, NC). PFS curves were calculated by Kaplan-Meier survival analysis, and groups were compared using the log-rank test. The Kruskal-Wallis test (for multiple groups) or the Mann-Whitney test (for 2 groups) was used for pairwise comparison of the first-cycle 18F-FDG PET results with the end-therapy 18F-FDG PET data. In post hoc analysis, Bonferroni/ Dunn correction was applied when necessary, with a probability value of < 0.0167 (significance < 5%).
RESULTS
18F-FDG PET Data Obtained Early After Chemotherapy
Of the 30 scans obtained after the first cycle of chemotherapy, 15 showed residual abnormal 18F-FDG uptake and 15 showed negative findings (Table 3).
18F-FDG PET After 1 Cycle of Chemotherapy
Positive 18F-FDG PET Results.
In this group of 15 patients, 13 patients (87%) experienced disease relapse after therapy or never achieved remission (8 NHL, 5 HD). The median PFS was 0 mo (range, 0–18 mo) (Fig. 1). All relapses occurred at the site of involvement observed on pretherapy 18F-FDG PET scans. In the remaining 2 patients, 18F-FDG PET was positive for residual disease but the patients have been in complete clinical remission with a follow-up of at least 18 mo. The residual uptake in 1 patient was in the location of the thymus, and findings on a posttherapy CT scan were consistent with thymic rebound. The sites of residual uptake in the other patient were in the mediastinum and the axillary regions. Although this patient did not undergo 18F-FDG PET immediately at the completion of chemotherapy, she still maintains positive 18F-FDG PET findings in these locations after a follow-up of 18 mo but remains in clinical remission.

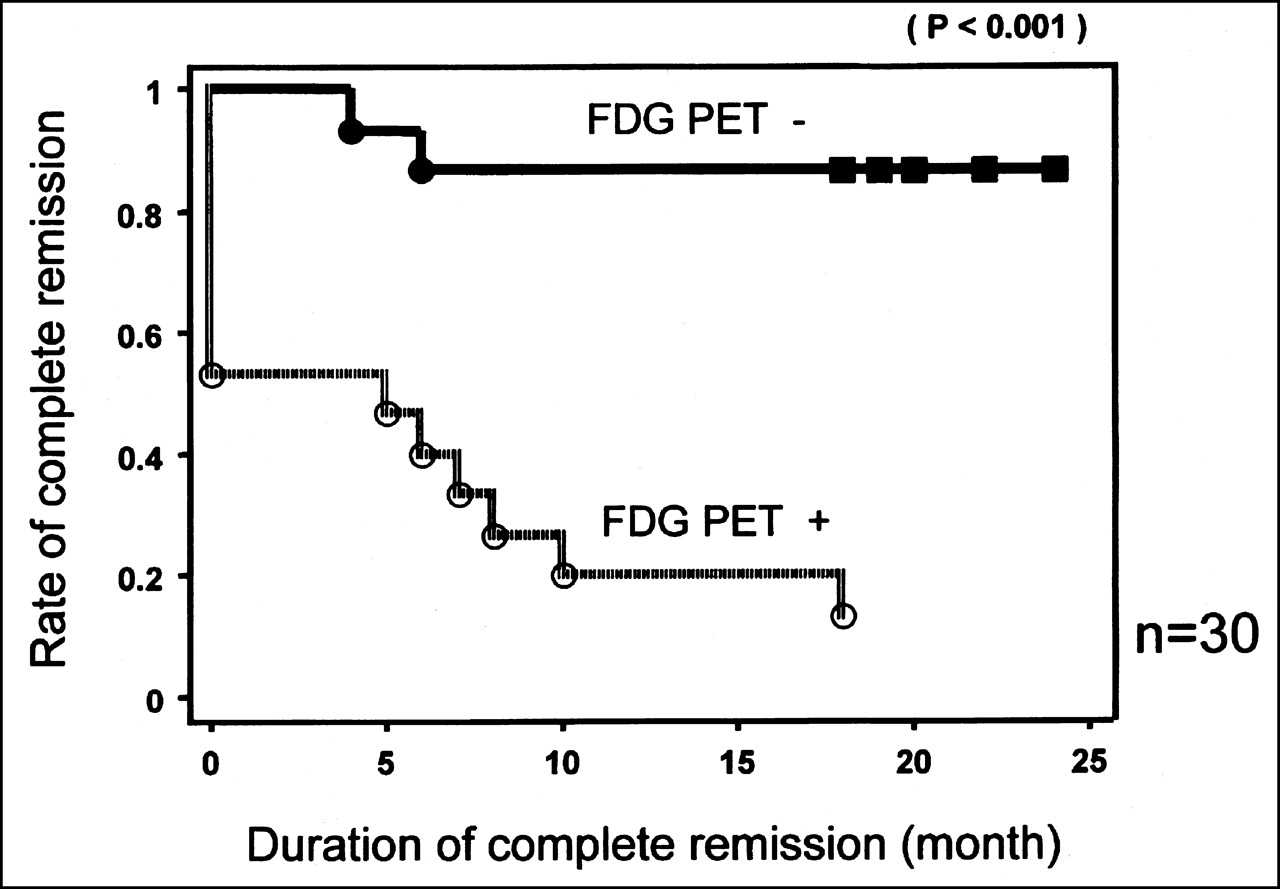
In entire group of patients who underwent 18F-FDG PET after first cycle of chemotherapy (30 patients), Kaplan-Meier estimate of PFS for 15 patients with positive 18F-FDG PET results is compared with that for 15 patients with negative 18F-FDG PET results after first cycle of chemotherapy. Statistically significant difference in PFS was found between positive and negative 18F-FDG PET results (P < 0.001).
Negative 18F-FDG PET Results.
Of the 15 patients with negative 18F-FDG PET results, 13 are still in complete remission (87%) after a median follow-up of 19 mo (range, 18–24 mo). Two 18F-FDG PET studies had false-negative findings. Although 2 patients had a brief clinical complete response (1 HD, PFS = 4 mo; 1 NHL, PFS = 6 mo), their disease eventually relapsed at the original site of involvement (mediastinum and retroperitoneal lymph nodes, respectively).
Overall Analysis.
The sensitivity, specificity, and overall accuracy of 18F-FDG PET performed after the first cycle for predicting 18-mo outcome were 87%. The positive and negative predictive values of 18F-FDG PET were also 87% (Table 3). There was a statistically significant difference in PFS between patients with negative (median PFS not reached) and those with positive (median PFS, 0 mo) 18F-FDG PET results after the first cycle of therapy (P < 0.0001) (Fig. 1).
18F-FDG PET Data Obtained Late After Chemotherapy
There were 23 patients who underwent 18F-FDG PET both after the first cycle and at the completion of therapy. Of these, 6 showed residual abnormal 18F-FDG uptake, and the studies of 17 were considered negative for residual lymphoma (Table 4).
18F-FDG PET After 1 Cycle vs. After Completion of Chemotherapy
Positive 18F-FDG PET Results.
In this group of 6 patients, 5 patients either experienced disease relapse (1 patient) or never achieved remission (4 patients). Relapse occurred at the same involved site as observed on the pretherapy 18F-FDG PET study. The median PFS in this group was 0 mo (range, 0–4 mo). In 1 of the 6 patients, 18F-FDG PET was false-positive for residual disease in the thymus, and this finding was confirmed to be thymic hyperplasia by a posttherapy CT scan. CT scans were not diagnostic for residual lymphoma and were indeterminate for viable lymphoma in all 5 patients.
Negative 18F-FDG PET Results.
Of the 17 patients with negative 18F-FDG PET results, 11 are still in complete remission (65%) after a median follow-up of 19 mo (range, 18–24 mo). The remaining 6 patients (4 NHL, 2 HD) experienced disease relapse at the original site, with a median PFS of 6.5 mo (range, 5–18 mo). The disease was in the head or neck in 2 patients and in the chest in 4 patients. Of 6 patients with false-negative results, 4 had a brief clinical complete response (1 HD, PFS = 5 mo; 3 NHL, PFS = 6, 6, and 7 mo, respectively), but their disease eventually relapsed. In 2 patients, the disease recurred at 10 and 18 mo, respectively, after the completion of therapy. Of 6 patients with false-negative 18F-FDG PET findings, CT was indeterminate for residual lymphoma in 5 and revealed partial remission based on size criteria in 1.
Overall Analysis.
The sensitivity, specificity, and overall accuracy of 18F-FDG PET performed after the completion of chemotherapy for predicting 18-mo outcome were 45.5%, 92%, and 70%, respectively. The positive and negative predictive values of 18F-FDG PET were 83% and 65%, respectively (Table 5). There was a statistically significant difference in PFS between the patients with negative (median PFS not reached) and those with positive (median PFS, 0 mo) 18F-FDG PET results after the completion of therapy (P < 0.001) (Fig. 2)

In group of patients who underwent both early and late 18F-FDG PET (23 patients), Kaplan-Meier estimate of PFS for 6 patients with positive 18F-FDG PET results is compared with that for 17 patients with negative 18F-FDG PET results at completion of chemotherapy. Statistically significant difference in PFS was found between positive and negative 18F-FDG PET results (P = 0.001).
Overall Comparative Analysis
Comparative Data Between Early and Late Evaluations
The results of 18F-FDG PET obtained after the first cycle and at the completion of chemotherapy were concordant in 17 of 23 patients (positive concordance in 5 patients, negative concordance in 12 patients) (9 NHL, 8 HD) and discordant in 6 patients (positive after the first cycle but negative at completion in 5 patients, negative after the first cycle but positive at completion in 1 patient) (4 NHL, 2 HD).
Discordant Results.
In 5 of 6 patients with discordant results, 18F-FDG PET results after the first cycle of therapy accurately predicted relapse whereas all 5 18F-FDG PET studies at the completion of chemotherapy were false-negative for residual disease in all patients (Fig. 3). The disease relapsed in these 5 patients, with a median PFS of 7 mo (range, 5–18 mo). There was 1 HD patient in whom 18F-FDG PET after 1 cycle of chemotherapy was false-negative in the mediastinum whereas 18F-FDG PET after the completion of chemotherapy was true-positive in predicting disease recurrence. This patient had disease relapse in the mediastinum after a PFS of 4 mo.

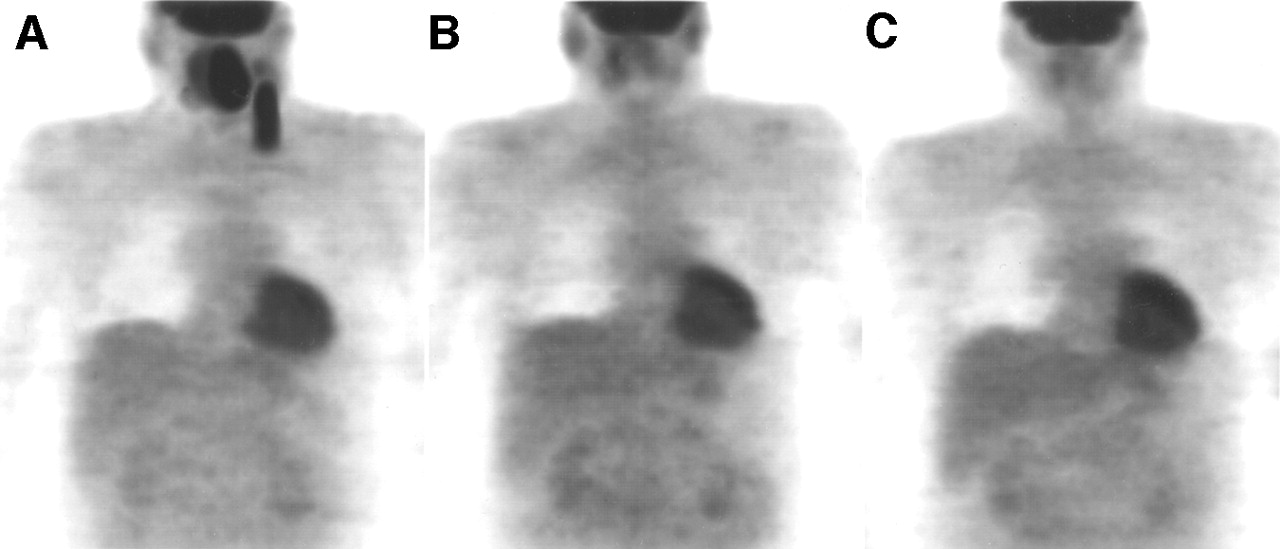
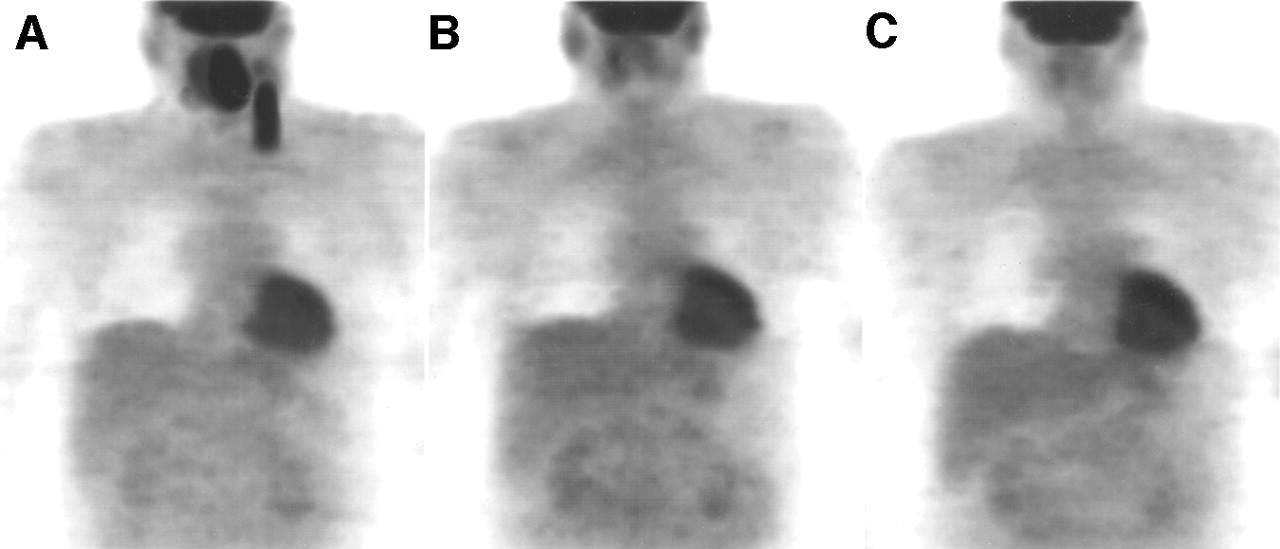
A 35-y-old man with bulky HD underwent 18F-FDG PET before (A), after first cycle of (B), and at completion of (C) chemotherapy. Pretherapy 18F-FDG PET images reveal radiotracer uptake in anterior mediastinum involving both hilar regions and extending into left supraclavicular region. Patient underwent chemotherapy with doxorubicin, bleomycin, vinblastine, and dacarbazine. 18F-FDG PET after first cycle of chemotherapy reveals residual disease in right anterior mediastinum, whereas 18F-FDG PET at completion of chemotherapy shows no evidence of residual lymphoma in corresponding regions. Disease relapsed in mediastinum after PFS of 6 mo. Images obtained after first cycle show physiologic uptake in salivary glands, oral mucosa, right shoulder (trapezius muscle), and heart.
Concordant Results.
Of 12 concordant negative 18F-FDG PET studies, 11 were of cases that are still in remission after a median follow-up of 19 mo (range, 18–24 mo) (Fig. 4). There was only 1 patient with false-negative results, whose disease relapsed with a PFS of 6 mo. Of 5 concordant positive 18F-FDG PET studies, 4 were of patients who were never free of disease. There was 1 patient in whom both 18F-FDG PET studies revealed false-positive findings for residual disease. This patient had CT-confirmed thymic hyperplasia.
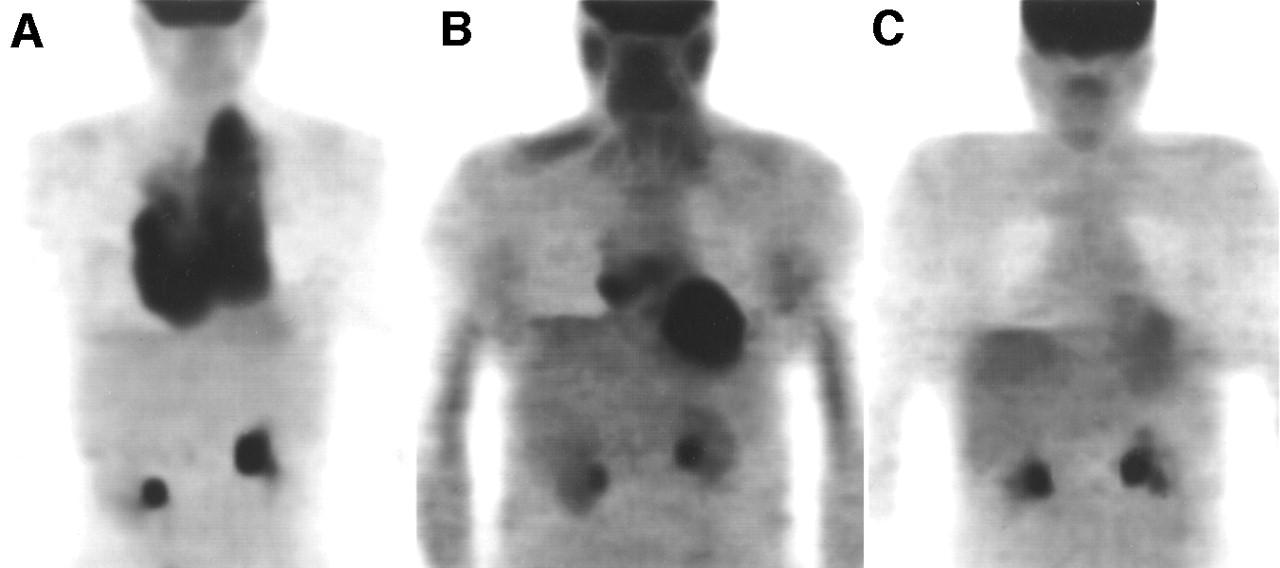
A 45-y-old man with NHL underwent 18F-FDG PET before (A), after first cycle of (B), and at completion of (C) chemotherapy. Pretherapy 18F-FDG PET images reveal radiotracer uptake in nasopharynx and left cervical lymph nodes. Patient underwent chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone. Both after first cycle and at completion of chemotherapy, 18F-FDG PET reveals no evidence of residual disease. Disease was still in remission after PFS of 18 mo. All images show physiologic uptake in heart.
The detection of residual tumor by 18F-FDG PET after the first cycle of chemotherapy had a higher sensitivity, negative predictive value, positive predictive value, and accuracy for relapse than that by 18F-FDG PET at the completion of chemotherapy (82% vs. 45.5%, 85% vs. 65%, 90% vs. 83%, and 87% vs. 70%, respectively). The specificity for 18F-FDG PET after the first cycle and last cycle of chemotherapy was the same (92%) (Table 5).
18F-FDG PET results obtained after the first cycle and after the completion of chemotherapy using the logistic regression for 23 patients indicated a statistically significant difference in PFS between patients with negative and those with positive 18F-FDG PET results (P ≤ 0.001) (Figs. 2 and 5); however, PFS and 18F-FDG PET correlated better after the first cycle of therapy than after the completion of therapy (r2 = 0.45 vs. 0.17; χ2 = 14.2 vs. 4.36). The 18-mo actuarial PFS rates after 1 cycle and after the completion of chemotherapy for patients with negative 18F-FDG PET results were 85% and 65%, respectively, compared with 10% and 17%, respectively, for patients with positive 18F-FDG PET results.

In group of patients who underwent both early and late 18F-FDG PET (23 patients), Kaplan-Meier estimate of PFS for 10 patients with positive 18F-FDG PET results is compared with that for 13 patients with negative 18F-FDG PET results after first cycle of chemotherapy. Statistically significant difference in PFS was found between positive and negative 18F-FDG PET results (P < 0.001).
Comparative Data Between Early and Late Evaluations for Patients with Poor Prognostic Features
Among 23 patients on whom comparative 18F-FDG PET data (after the first and last cycles of therapy) were available, 18 poor-prognosis patients, consisting of 10 who were in relapse before salvage therapy and 8 who had features of high risk for recurrence at initial staging, were evaluated (Table 2). Eleven of 18 patients had disease relapse, with a median PFS of 5 mo (range, 0–18 mo), and 7 were in sustained remission during a median follow-up of 19 mo (range, 18–24 mo). 18F-FDG PET after the first cycle and last cycle of chemotherapy predicted PFS in 15 patients (83%) and 11 patients (61%), respectively. After the first cycle, the 18F-FDG PET results were false-negative in 2, false-positive in 1 (thymic rebound), true-positive in 9, and true-negative in 6; after the last cycle, the 18F-FDG PET results were false-negative in 6, false-positive in 1 (thymic rebound), true-positive in 5, and true-negative in 6.
The results of 18F-FDG PET after the first cycle and at the completion of chemotherapy were concordant in 12 of 18 patients (positive concordance in 5 patients, negative concordance in 7 patients) and discordant in 6 patients. Among 6 patients with discordant results, the relapse that occurred in 5 had been predicted by 18F-FDG PET after the first cycle of therapy, whereas 18F-FDG PET after the last cycle had been false-negative in all 6 (Fig. 3). In these 5 patients, median PFS was 7 mo (range, 5–18 mo). In 1 discordant case, 18F-FDG PET after 1 cycle was false-negative in the mediastinum and converted to true-positive at the completion of therapy. The disease of this patient relapsed after a PFS of 4 mo. Of 5 patients with concordant positive 18F-FDG PET studies, 4 never achieved remission (PFS, 0 mo). In 1 patient with thymic hyperplasia, both 18F-FDG PET studies were false-positive. Among 7 concordant negative studies, 6 were of patients whose disease was in complete remission during a median follow-up of 19.5 mo (range, 18–24 mo). There was 1 false-negative study for a patient whose disease relapsed at 6 mo.
Overall Comparative Analysis
The comparative statistical values between data obtained for 18F-FDG PET after the first cycle and at the completion of chemotherapy were similar to those obtained for the entire patient group (Table 5). Sensitivity, specificity, negative predictive value, positive predictive value, and accuracy for 18F-FDG PET after the first cycle versus at the completion of chemotherapy were 82% versus 45.5%, 86% versus 86%, 75% versus 50%, 90% versus 83%, and 83% versus 61%, respectively.
A comparison of the 18F-FDG PET results obtained after the first cycle and at the completion of chemotherapy using logistic regression for 18 patients indicated a statistically significant difference in PFS between positive and negative 18F-FDG PET results at the completion of therapy (P ≤ 0.001). The 18-mo actuarial PFS rates for patients with negative 18F-FDG PET studies were 75% and 50%, compared with 10% and 17% for patients with positive 18F-FDG PET results, after 1 cycle and at the completion of chemotherapy, respectively.
DISCUSSION
Efforts are now being made to improve the outcome of patients who do not achieve a sustained complete remission with aggressive therapy (7,20,21). In this regard, our findings clearly showed that 18F-FDG PET has a high prognostic value for evaluation of therapy as early as after 1 cycle in aggressive NHL and HD. Ninety percent of patients with positive 18F-FDG PET results after 1 cycle experienced disease relapse with a median PFS of 5 mo, whereas for 85% of patients who had negative 18F-FDG PET findings, the disease remained in complete remission with a minimum follow-up of 18 mo. Disease relapsed in all patients with persistent 18F-FDG uptake both after the first cycle and at the completion of therapy, except 1 patient who had thymic rebound, a condition known to cause false-positive findings (22, 23). The PFS was significantly different (P < 0.001) between patients with negative 18F-FDG PET results and patients with positive 18F-FDG PET results after 1 cycle of treatment. After the completion of chemotherapy, although there was a statistically significant difference between patients with 18F-FDG PET negative findings and patients with 18F-FDG PET positive findings, 18F-FDG PET results were not as good a predictor of long-term outcome (Table 5; Fig. 2). 18F-FDG PET findings after the completion of chemotherapy yielded a significantly lower sensitivity and negative predictive value than did findings after the first cycle.
The disease activity may completely resolve after therapy, but residual masses may persist on CT because resolution of therapy-induced anatomic changes usually lags behind tumor cell mortality. 67Ga imaging is a standard procedure for the posttreatment evaluation of tumor viability. In previous studies, 67Ga imaging after 1 cycle of therapy has been found to be predictive of outcome in aggressive NHL and HD but, because of the physiologic excretion of 67Ga in the bowel, is less effective for the interpretation of abdominal involvement (6,10, 24). Furthermore, 67Ga imaging lacks sensitivity for deeply located small lesions. Various reports have shown the effectiveness of 18F-FDG PET in the posttreatment evaluation of lymphomas. The results of a previous study indicated that 18F-FDG PET was superior to 67Ga scintigraphy in accurately detecting disease sites in aggressive NHL and HD, with a sensitivity of 100% and 80.3%, respectively (11). Furthermore, 18F-FDG PET scans have a higher diagnostic and prognostic value than CT scans in the posttreatment evaluation of lymphomas (15). Thus, 18F-FDG PET has become the most helpful noninvasive modality in differentiating tumor recurrence from fibrosis when CT scans show a residual mass (12,15,22, 23,25,26).
In our data, the relapse rate when 18F-FDG PET at the completion of therapy had negative results was higher than that when 18F-FDG PET after the first cycle had negative results (35% vs. 15%). After the completion of therapy, there were 6 false-negative 18F-FDG PET studies, with relapses occurring at a median of 7 mo. Interestingly, in 5 of these 6 studies, 18F-FDG PET after the first cycle predicted relapse by showing residual 18F-FDG uptake in the tumor. In these studies, CT had no additional value in predicting recurrence. Other studies have also shown CT to offer no further benefit in predicting the outcome of lymphoma (7,18). The superior capability of 18F-FDG PET to predict outcome in patients with aggressive lymphoma and HD early during therapy is most likely the consequence of the sensitivity and rapid response characteristics of these lymphomas to chemotherapy. Our findings suggest that positive 18F-FDG PET results after 1 cycle reflect the metabolic activity of potentially resistant clones, which, although responding to chemotherapy, do so more slowly than do those homogeneously sensitive tumor cells. In a recent study, disease later relapsed in 20% of all lymphoma patients for whom 18F-FDG PET performed at the completion of therapy had negative findings (18). In contrast to the high false-negative rate observed with late 18F-FDG PET studies, only 2 early 18F-FDG PET studies had false-negative findings, which recurred after brief clinical remissions. This recurrence may possibly result from a small cluster of resistant clones that remained after the first cycle of therapy and escaped detection because of the resolution limits of the PET scanner.
The results for both the poor-prognosis group and the entire group after the first cycle of chemotherapy were similar, except that negative predictive value was lower for the poor-prognosis group (85% vs. 75%). This finding, however, may stem from the small size of the study group. Although the rate of relapse in patients with a poor prognosis is expected to be high, 18F-FDG PET was accurate in predicting remission. Indeed, 6 of 7 patients with concordant negative 18F-FDG PET findings both after the first cycle and at completion remain in complete remission with a median follow-up of 19.5 mo. Although the predictive value for remission was equal for both early and late studies, there is an advantage to assessing this poor-prognosis group early during chemotherapy, because early evidence of persistent disease may mandate an innovative intervention such as bone marrow transplantation. In this group, 18F-FDG PET may prove to be the imaging modality of choice for follow-up.
In our group of patients, for negative 18F-FDG PET findings after the first and last cycles, relapse rates were 15% (2/11 patients) and 35% (6/17 patients), respectively. The relapse rates after the last cycle of chemotherapy in our data appear to be higher than those reported for a prior study (18). The prior study included only patients evaluated at initial staging who underwent first-line therapy and included patients with low-grade lymphoma. Our series included both patients at initial staging and patients at relapse before salvage therapy, who were at a higher risk of disease recurrence. In our data, we investigated only aggressive NHL and HD because both types of lymphoma are sensitive to chemotherapy and potentially curable and may benefit from earlier more intensive treatment programs if tumor resistance is detected. In the previous study, the minimal follow-up period in some patients was 12 mo, whereas the minimal follow-up period in our study was 18 mo. Hence, by virtue of our study design, higher relapse rates than those observed in the prior study were anticipated.
Romer et al. (17) reported that 18F-FDG PET studies performed 7–42 d after therapeutic intervention had some predictive value in a small number of patients with high-grade NHL. In this study, chemotherapy caused a rapid decrease in tumor 18F-FDG uptake as early as 7 d after treatment, and 18F-FDG uptake continued to decline during therapy. During a follow-up of 16 ± 4 mo, 50% of patients continued to show remission. Our findings were similar to those obtained in this previous study except that remission rates in our series were higher. In our series, 85% of patients with complete disappearance of 18F-FDG uptake after 1 cycle of chemotherapy were in remission during a median follow-up of 19 mo. The differences in remission rates between our study and the previous study can be attributed to differences in study design. The previous study evaluated only 11 patients, and the main objectives were to determine the extent and time course of changes in 18F-FDG use in response to therapy and whether these changes in early uptake predicted the outcome of therapy. In our study, we evaluated 30 patients and our main objective was to determine whether 18F-FDG PET could determine the outcome of therapy after the first cycle of therapy versus after the completion of therapy.
If abnormal 18F-FDG uptake is seen after the first cycle of chemotherapy, the chances for relapse are significantly high; thus, close follow-up is mandatory in this group of patients. Negative 18F-FDG PET results after the first cycle were highly suggestive of long-term remission, whereas negative results after the completion of chemotherapy were less accurate. Although tumor progression or disease relapse may still develop in a few patients with negative 18F-FDG PET results early during treatment, 18F-FDG PET after the first cycle of chemotherapy remains far more predictive of outcome than is late 18F-FDG PET.
Patients with relapsed or refractory aggressive NHL or HD (appropriate candidates) generally receive second-line chemotherapy, and if the disease is sensitive to second-line chemotherapy, randomized trials have shown a survival benefit from high-dose chemotherapy and stem cell transplantation (27). If sufficient data were available that persistent positive 18F-FDG PET results after 1 cycle of chemotherapy portend a poor prognosis, one could argue either that one should switch the treatment to second-line chemotherapy and stem cell transplantation without completing a full course of initial chemotherapy or that one should, contrary to the usual procedure, repeat the 18F-FDG PET after 2–3 cycles and, if the findings are still positive, repeat the tumor biopsy or push for an earlier switch to an alternative dose-intense treatment. Our study provides a strong argument for consideration of a follow-up trial in which 18F-FDG PET is performed after 1 cycle to evaluate a potential subsequent change in treatment based on the results. Patients with negative 18F-FDG PET findings after 1 cycle and thus a good prognosis would continue with a full course of their first-line treatment, whereas patients with positive 18F-FDG PET findings after 1 cycle and thus a less favorable prognosis could be randomized to receive a full course of first-line treatment.
Of note, this study used a dual-head coincidence camera with attenuation correction instead of a dedicated full-ring PET system. Coincidence cameras have one third the sensitivity of dedicated PET systems. With the added benefit of attenuation correction, however, the detection rate of coincidence PET has been reported to increase from 60% to 80% for lesions ≤ 2 cm (28). Given the superior sensitivity of dedicated PET systems, it is even more impressive that the prognostic value of 18F-FDG imaging early during therapy was so readily shown in this study.
CONCLUSION
We believe that this study indicates that 18F-FDG PET, by itself, has a high prognostic value after the first cycle of therapy and is a valid alternative for posttreatment evaluation of aggressive NHL and HD. If these data are substantiated by other studies, 18F-FDG PET evaluation after the first cycle may need to be incorporated into standard follow-up procedures.
Footnotes
Received Sep. 19, 2001; revision accepted Jan. 3, 2002.
For correspondence or reprints contact: Lale Kostakoglu, MD, New York Presbyterian Hospital, Weill Cornell Medical Center, 525 E. 68th St., Starr: 221, New York, NY 10021.
E-mail: lak2005{at}mail.med.cornell.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- In Vivo Treatment Sensitivity Testing With Positron Emission Tomography/Computed Tomography After One Cycle of Chemotherapy for Hodgkin Lymphoma
- Validation of Several SUV-Based Parameters Derived from 18F-FDG PET for Prediction of Survival After SIRT of Hepatic Metastases from Colorectal Cancer
- Interim FDG-PET in Hodgkin lymphoma: a compass for a safe navigation in clinical trials?
- 18F-FDG PET/CT Predicts Survival After Radioembolization of Hepatic Metastases from Breast Cancer
- Interim [18F]Fluorodeoxyglucose Positron Emission Tomography Scan in Diffuse Large B-Cell Lymphoma Treated With Anthracycline-Based Chemotherapy Plus Rituximab
- Specific biomarkers of receptors, pathways of inhibition and targeted therapies: clinical applications
- PET/CT with 18F-FLT: Does It Improve the Therapeutic Management of Metastatic Germ Cell Tumors?
- Mixed Response in Interim Positron Emission Tomography/Computed Tomography Leads to Detection of a Gastrointestinal Stromal Tumor in a Patient With Mediastinal Diffuse Large B-Cell Lymphoma
- Early and Late Therapy Response Assessment With [18F]Fluorodeoxyglucose Positron Emission Tomography in Pediatric Hodgkin's Lymphoma: Analysis of a Prospective Multicenter Trial
- Tumor Metabolic Phenotypes on 18F FDG PET
- PET/CT for Therapy Response Assessment in Lymphoma
- Role of [18F]Fluorodeoxyglucose Positron Emission Tomography Scan in the Follow-Up of Lymphoma
- Fluorine-18-Fluorodeoxyglucose Positron Emission Tomography for Interim Response Assessment of Advanced-Stage Hodgkin's Lymphoma and Diffuse Large B-Cell Lymphoma: A Systematic Review
- Prognostic Value of Interim 18F-FDG PET in Patients with Diffuse Large B-Cell Lymphoma: SUV-Based Assessment at 4 Cycles of Chemotherapy
- Reproducibility of Standardized Uptake Value Measurements Determined by 18F-FDG PET in Malignant Tumors
- Evaluation of response to fractionated radioimmunotherapy with 90Y-epratuzumab in non-Hodgkin's lymphoma by 18F-fluorodeoxyglucose positron emission tomography
- Early 18F-FDG PET for Prediction of Prognosis in Patients with Diffuse Large B-Cell Lymphoma: SUV-Based Assessment Versus Visual Analysis
- Early Interim 2-[18F]Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography Is Prognostically Superior to International Prognostic Score in Advanced-Stage Hodgkin's Lymphoma: A Report From a Joint Italian-Danish Study
- A Pilot Study of [18F]Fluorodeoxyglucose Positron Emission Tomography Scans During and After Radiation-Based Therapy in Patients With Non Small-Cell Lung Cancer
- Respective prognostic values of germinal center phenotype and early 18fluorodeoxyglucose-positron emission tomography scanning in previously untreated patients with diffuse large B-cell lymphoma
- Histological verification of positive positron emission tomography findings in the follow-up of patients with mediastinal lymphoma
- Time Course of Early Response to Chemotherapy in Non-Small Cell Lung Cancer Patients with 18F-FDG PET/CT
- Effect of Corticosteroids on 18F-FDG Uptake in Tumor Lesions After Chemotherapy
- Use of Positron Emission Tomography for Response Assessment of Lymphoma: Consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma
- Revised Response Criteria for Malignant Lymphoma
- Risk-adapted BEACOPP regimen can reduce the cumulative dose of chemotherapy for standard and high-risk Hodgkin lymphoma with no impairment of outcome
- Integrating PET and PET/CT into the Risk-Adapted Therapy of Lymphoma
- Cost-Effectiveness Analysis of Computerized Tomography in the Routine Follow-Up of Patients After Primary Treatment for Hodgkin's Disease
- The Role of PET in Lymphoma
- Positron Emission Tomography As an Imaging Biomarker
- Utility of Positron Emission Tomography (PET) Scanning in Managing Patients with Hodgkin Lymphoma
- Optimal Use of Prognostic Factors in Non-Hodgkin Lymphoma
- FDG-PET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma
- PET for response assessment in oncology: radiotherapy and chemotherapy
- [18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in aggressive lymphoma: an early prognostic tool for predicting patient outcome
- Role of Positron Emission Tomography in Lymphoma
- Use of PET for Monitoring Cancer Therapy and for Predicting Outcome
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- Imaging DNA Synthesis In Vivo with 18F-FMAU and PET
- Diffuse Large B-Cell Lymphoma: Risk Stratification and Management of Relapsed Disease
- Decreased 18F-FDG Uptake 1 Day After Initiation of Chemotherapy for Malignant Lymphomas
- Early Identification of Therapeutic Failure in Nonseminomatous Germ Cell Tumors by Assessing Serum Tumor Marker Decline During Chemotherapy: Still Not Ready for Routine Clinical Use
- Chemotherapy With or Without Radiotherapy in Limited-Stage Diffuse Aggressive Non-Hodgkin's Lymphoma: Eastern Cooperative Oncology Group Study 1484
- PET/CT in Oncology: Integration into Clinical Management of Lymphoma, Melanoma, and Gastrointestinal Malignancies
- Hodgkin's Lymphoma: Evolving Concepts with Implications for Practice
- PET Scans in the Staging of Lymphoma: Current Status
- Prognostic Value of PET Using 18F-FDG in Hodgkin's Disease for Posttreatment Evaluation
- Early Response to Chemotherapy in Hypopharyngeal Cancer: Assessment with 11C-Methionine PET, Correlation with Morphologic Response, and Clinical Outcome
- 18F-FDG PET Evaluation of the Response to Therapy for Lymphoma and for Breast, Lung, and Colorectal Carcinoma
- Assessment of Lymphoma Therapy Using 18F-FDG PET