


Abstract
PET with 18F-FDG is a standard staging procedure for most lymphoma subtypes. Performed during and after therapy for Hodgkin lymphoma (HL) and aggressive non-Hodgkin lymphoma (NHL), 18F-FDG PET results have a high prognostic value and correlate with survival. 18F-FDG PET has been incorporated into revised response criteria for aggressive lymphomas, and several ongoing trials are under way to investigate the value of treatment adaptation based on early 18F-FDG PET results for HL and aggressive NHL. There is little evidence to support the use of 18F-FDG PET for monitoring of the treatment of indolent lymphomas and for routine use in the surveillance setting. So that trial results can be compared and translated easily into clinical practice, uniform and evidence-based guidelines for the interpretation and reporting of response monitoring scans are warranted. Because it is still not proven that the use of interim 18F-FDG PET can improve patient outcomes, we recommend examination of the use of 18F-FDG PET for response monitoring in appropriately designed clinical trials.
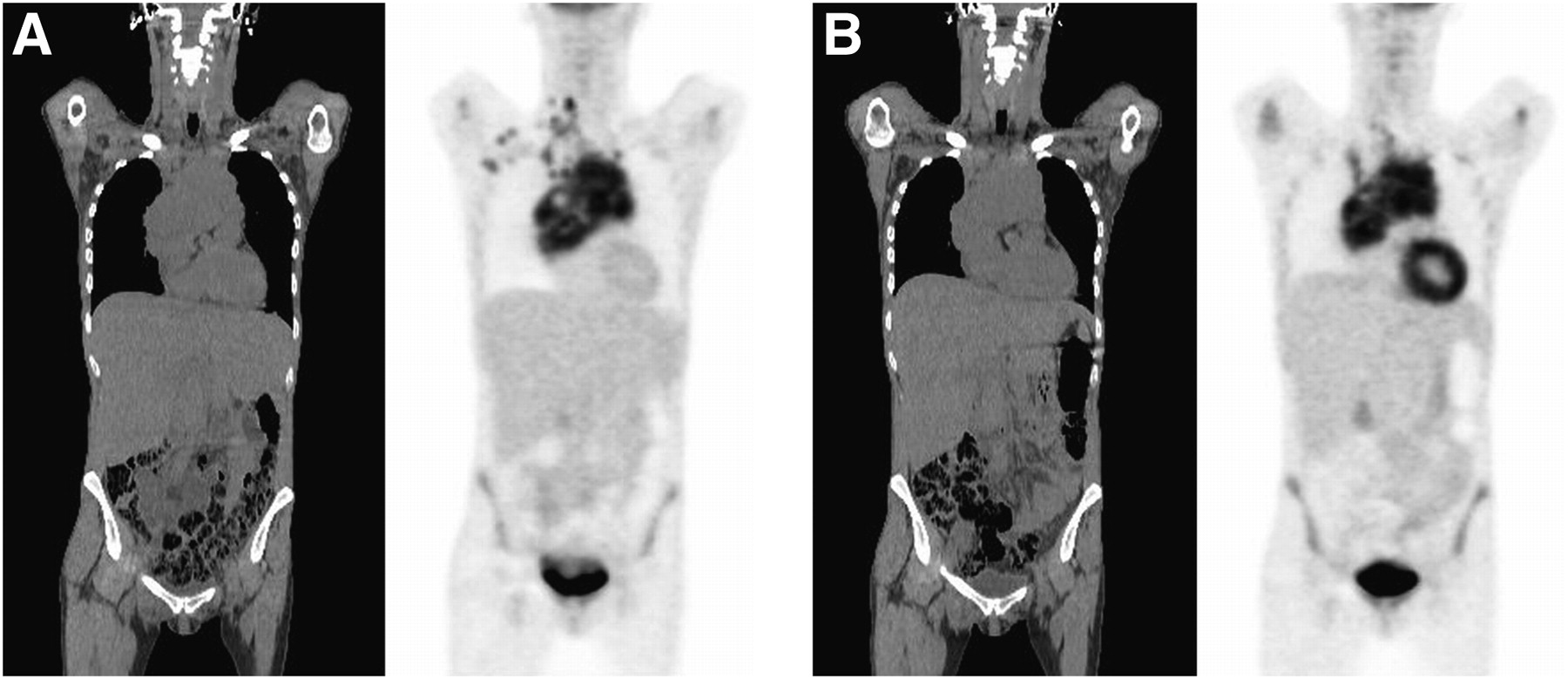
The first reports of PET with 18F-FDG for lymphoma imaging were published more than 20 y ago (1). Given that most lymphomas showed high levels of 18F-FDG uptake, several studies investigating the value of 18F-FDG PET for the diagnosis and staging of lymphomas followed. These studies almost invariably showed very high sensitivity in patients with Hodgkin lymphoma (HL) and high-grade or aggressive non-Hodgkin lymphoma (NHL) (2). 18F-FDG PET frequently detected nodal and extranodal disease sites that were missed by conventional staging methods, including CT, and improved the characterization of lesions that were equivocal on other types of imaging (Figs. 1 and 2).
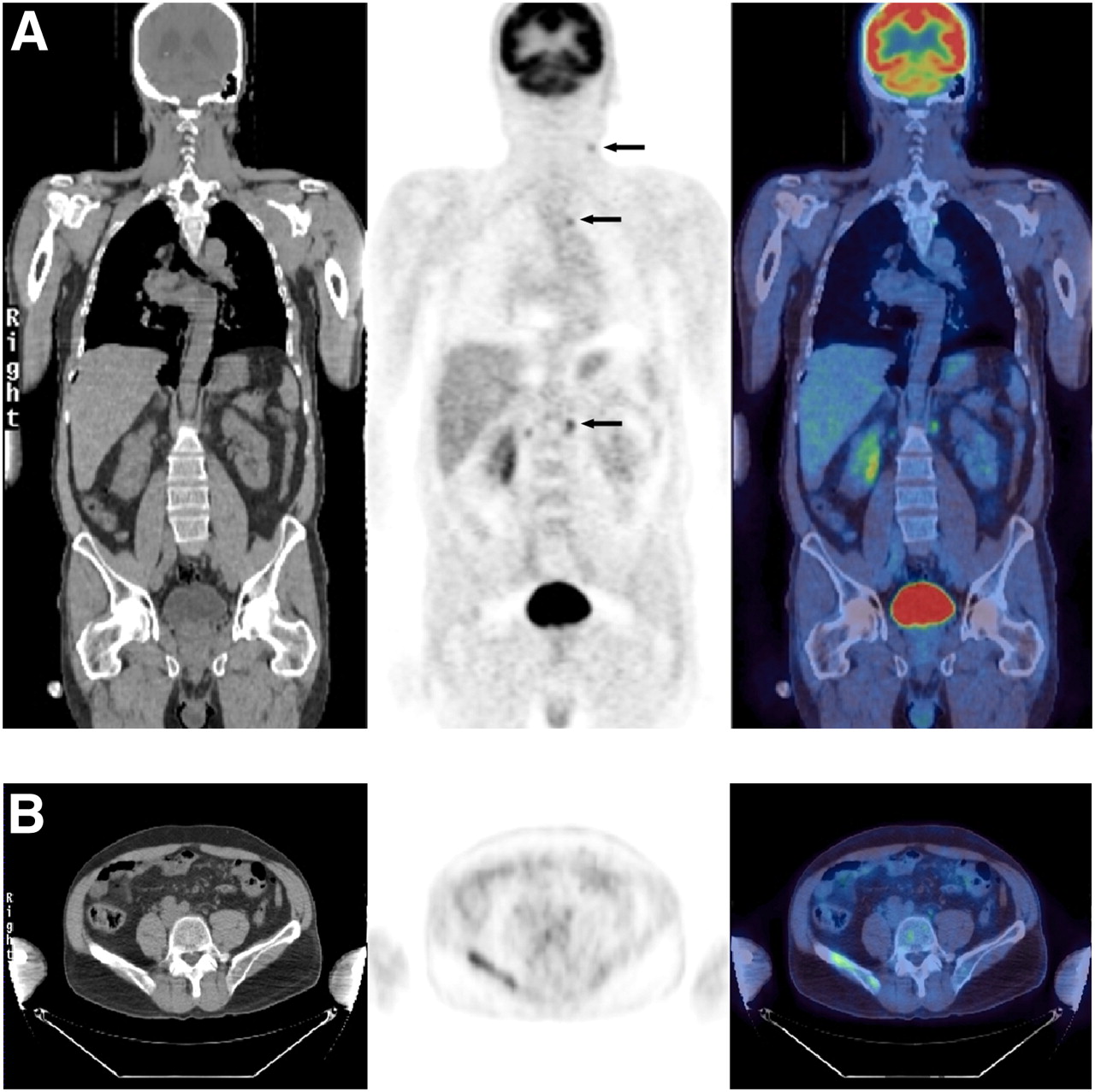
Patient diagnosed with NHL from biopsy of left cervical node. In addition to disease in left neck, 18F-FDG uptake in normally sized lymph nodes in left superior mediastinum and paraaortic nodes below diaphragm (arrows in A) and in right iliac bone (B) was indicative of stage IV rather than stage II disease.

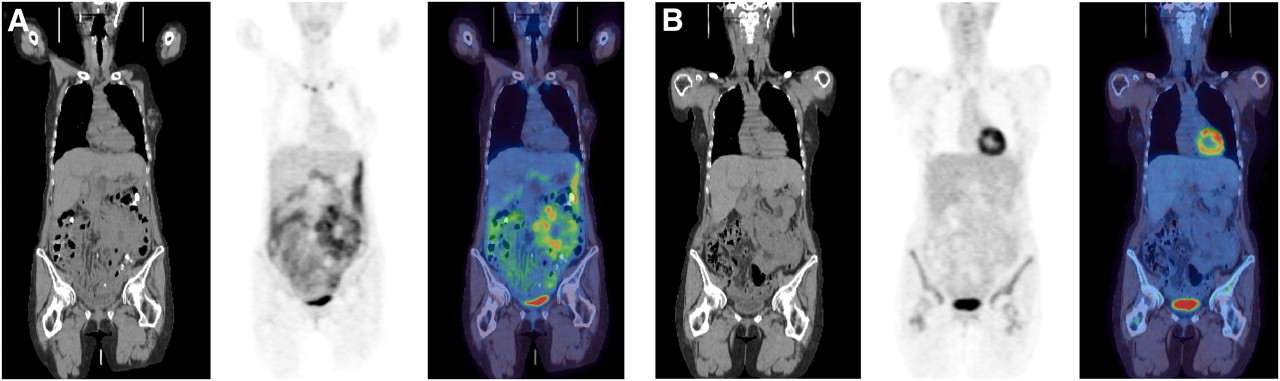
(A) At staging, patient with diffuse large B-cell lymphoma had extensive peritoneal and omental disease, which is often difficult to assess with CT. (B) Interim scanning after 2 cycles of chemotherapy showed complete metabolic response.
18F-FDG PET findings can result in the upstaging as well as the downstaging of disease (3). Because there are considerable differences in the treatments of early and advanced stages of lymphoma, 18F-FDG PET has an important potential impact on treatment strategy when used before therapy. More recent results have shown that the high sensitivity of 18F-FDG PET is accompanied by high specificity when the technique is performed as 18F-FDG PET/CT. For the heterogeneous group of low-grade or indolent lymphomas, there have been greater variations in the reported specificity and sensitivity as well as the reported impact on staging and treatment strategy, but the results are generally encouraging; 18F-FDG PET seems to be a valuable addition to existing staging tools. Although there is little or no evidence that the addition of 18F-FDG PET has had any impact on treatment outcomes, 18F-FDG PET/CT is now the cornerstone of staging procedures in the state-of-the-art management of HL and aggressive NHL. For the staging of indolent lymphomas, 18F-FDG PET/CT is still used more sporadically or in the setting of investigational protocols (4).
During the last decade, 18F-FDG PET has been introduced into all of the steps of lymphoma management. In the present article, we review, from a clinical point of interest, evidence for the use of 18F-FDG PET in monitoring of the treatment of lymphomas; the topics include interim treatment monitoring, posttreatment response evaluation, and follow-up. Furthermore, the important role of 18F-FDG PET in risk-adapted or response-adapted therapy is addressed.
The review is based on an extensive search of the literature in the PubMed and EmBase online databases; personal communications and conference abstracts were not considered. The final literature search was performed on December 12, 2008. Ongoing clinical trials are mentioned only if they are registered in the ClinicalTrials.gov database (www.clinicaltrials.gov).
18F-FDG PET IN EARLY MONITORING OF LYMPHOMA TREATMENT
For both HL and NHL, well-established pretreatment prognostic factors have been shown to predict survival in large cohort studies (5–8). The clinical stage and these prognostic factors largely determine the initial treatment strategy. However, for all lymphoma subgroups, the tumor response is an important surrogate for other measures of clinical benefit from the treatment, including progression-free survival (PFS) and overall survival (OS). A precise early prediction of the response to therapy might be able to separate patients who could be cured with conventional therapy or even less intensive and less toxic regimens from patients for whom an early switch to alternative, more aggressive treatment strategies could improve the likelihood and duration of remission. This concept of risk-adapted therapy is being increasingly recognized as a way to achieve a higher cure rate with a lower or equal risk of treatment-related morbidity and mortality.
Conventional methods for treatment response monitoring are based on morphologic criteria, and a reduction in tumor size on CT is the most important determinant (9–11). However, it is not an accurate predictor of outcome. In HL, malignant cells comprise only a small fraction of the tumor volume, which is dominated by reactive infiltrating cells not directly affected by antineoplastic therapy (12). More importantly, because tumor shrinkage takes time and depends on several factors in the host, the rate of structural regression cannot form the basis for the adjustment of therapy until late during treatment. Functional imaging with 18F-FDG PET enables evaluation of the early metabolic changes rather than the morphologic changes of the lymphoma occurring later during therapy. Several studies of 18F-FDG PET after 1–3 cycles of chemotherapy for aggressive NHL (13–21) and HL (22–26) have shown that these early metabolic changes are highly predictive of the final treatment response and PFS (Table 1).
Prognostic Value of 18F-FDG PET After 1–3 Cycles of Chemotherapy for Aggressive NHL and HL
In aggressive NHL, PFS ranges from 10% to 50% at 1 y for patients with early 18F-FDG PET–positive results and from 79% to 100% at 1 y for patients with early 18F-FDG PET–negative results. The high relapse rate seen in patients with early 18F-FDG PET–positive results is consistent in both early and advanced stages. Mikhaeel et al. confirmed that the response on 18F-FDG PET after 2 or 3 cycles of treatment strongly predicted PFS and OS in a large, retrospectively studied cohort of 121 patients with high-grade NHL and a median follow-up of 28.5 mo (19). The estimated 5-y PFS rates were 89% for patients with PET-negative results, 59% for patients with minimal residual uptake on 18F-FDG PET, and 16% for patients with PET-positive results. Kaplan–Meier analyses showed strong associations between early 18F-FDG PET results and PFS and OS. Haioun et al. prospectively studied 90 patients with aggressive NHL, performing 18F-FDG PET after 2 cycles of chemotherapy (20). Similarly, they found 2-y PFS rates to be 82% and 43% and 2-y OS rates to be 90% and 60% in patients with early PET-negative and early PET-positive results, respectively. Spaepen et al. compared interim 18F-FDG PET with the International Prognostic Index (15). In a multivariate analysis, 18F-FDG PET at midtreatment was a stronger prognostic factor for PFS and OS than was the International Prognostic Index (P < 0.58 and P < 0.03, respectively).
In a retrospective analysis of 88 patients scanned after 2 or 3 cycles of ABVD-like chemotherapy (ABVD is adriamycin–bleomycin–vinblastine–dacarbazine) for HL, Hutchings et al. found 5-y PFS rates of 39% for patients with PET-positive results and 92% for patients with PET-negative results (22). These results were later confirmed in prospective studies by Hutchings et al. (23) and Gallamini et al. (25), the latter study focusing on patients with advanced HL only. Among patients who were scanned after 2 cycles of ABVD, these studies found 2-y PFS rates of 0%−6% for patients with early PET-positive results and 94% for patients with early PET-negative results (Fig. 3). The 2 cohorts of patients with advanced-stage HL were joined, and accrual was continued until a cohort of 260 patients was reached. For this cohort, the prognostic value of early 18F-FDG PET completely overshadowed the role of the International Prognostic Score (IPS), with equally dismal outcomes for patients with PET-positive results regardless of IPS stratification and correspondingly excellent survival for patients with PET-negative results independent of the IPS (26). Recent studies have raised concerns that the positive predictive value of early 18F-FDG PET may be lower in patients treated with the more dose-intensive BEACOPPesc regimen (BEACOPPesc is bleomycin–etoposide–doxorubicin–cyclophosphamide–vincristine–procarbazine–prednisone) than in patients treated with ABVD (see later discussion) (27,28).

Patient with HL had persistent active disease after 2 cycles of chemotherapy, suggesting poor prognosis. Staging (A) and interim (B) scans are shown.
There are very few data on the value of interim 18F-FDG PET for indolent lymphomas. Bishu et al. reported results for a retrospective series of 31 patients with advanced-stage follicular lymphoma (FL), of whom 11 had 18F-FDG PET scans midway through 4 cycles of chemotherapy (29). Although the numbers were far too small for any statistically significant differences, 4 patients with some persistent 18F-FDG uptake had a mean PFS of 17 mo, whereas 7 patients with interim PET-negative results had a mean PFS of 30 mo. Even if a clear correlation between interim 18F-FDG PET results and treatment outcomes or PFS is shown in the future, the clinical implications are uncertain, because advanced-stage indolent lymphoma is very different from HL and aggressive NHL. First, current therapies for advanced-stage FL are very rarely curative, but it is far from clear that early treatment intensification with autologous stem cell transplantation (ASCT) or allogeneic bone marrow transplantation is of any benefit for nonresponding patients. Second, the long natural history of FL and the relative success of subsequent treatments in inducing lasting remissions mean that a longer time to first progression does not necessarily translate into longer survival. There are no reports on the value of interim 18F-FDG PET for localized FL or the more uncommon subtypes of indolent NHL, such as marginal-zone lymphoma and small lymphocytic lymphoma.
EARLY PET RESPONSE–ADAPTED LYMPHOMA THERAPY
Aggressive NHL includes several lymphoma subtypes for which first-line treatment of both localized and advanced disease stages is given with a curative intent. Patients who have aggressive NHL and who respond poorly to first-line treatment or relapse soon afterward generally have a very poor prognosis, even with high-dose salvage regimens. Such patients could benefit from the recognition of treatment failure early during first-line therapy so that a more intensive regimen can be initiated as soon as possible. Several trials are currently investigating whether patients with early or midtreatment PET-positive results for diffuse large B-cell lymphoma will benefit from early escalation to a more intensive regimen or even high-dose therapy with ASCT (Table 2) (30–34).
Ongoing Trials with Early PET Response–Adapted Therapies
As for patients with NHL, there is yet no evidence that patients with HL will benefit from having treatment adapted according to the results of early 18F-FDG PET. The vast majority of patients with early-stage HL (>90%) are cured with standard therapy, including a brief course of polychemotherapy followed by irradiation of the initially involved disease sites. Once cured, however, the patients still have a dramatically reduced life expectancy because of treatment-related illness, including second cancers and cardiopulmonary disease. In fact, more patients with early-stage HL die from late effects of therapy than from the disease itself. Given that a large fraction of patients with early-stage HL are subjected to some amount of overtreatment, there is potential benefit in identifying patients who have early-stage disease and who are eligible for less intensive treatment. Several trials have investigated such PET response–adapted therapy for early-stage HL (Table 2). The U.K. National Cancer Research Institute (NCRI) Lymphoma Group RAPID trial for patients with early-stage disease as well as the German Hodgkin Study Group (GHSG) HD16 protocol investigated the effects of reducing treatment intensity by omitting radiotherapy for patients with early-stage disease and interim PET-negative results (35). The experimental arms of the European Organization for Research and Treatment of Cancer–Groupe d'Etudes des Lymphomes de l'Adulte–Intergruppo Italiano dei Linfomi H10 protocol also omitted radiotherapy for patients with PET-negative results while escalating treatment to BEACOPPesc followed by radiotherapy for patients with PET-positive results (36). Therefore, this trial tested the effects of a less toxic treatment for patients with a low risk of failure while, at the same time, attempting treatment intensification for patients regarded as having a high risk of failure on the basis of positive interim 18F-FDG PET results. The prognostic value of interim 18F-FDG PET was largely attributed to the high predictive value for patients with advanced-stage disease. In a study by Hutchings et al., only 1 of 5 patients with early-stage disease and interim 18F-FDG PET–positive results relapsed, and this patient was successfully treated with salvage therapy (23). Therefore, intensification with BEACOPPesc might cause unnecessary toxicity in patients who would have been cured with standard therapy.
In advanced-stage HL, patients who fail to reach remission or relapse early after first-line therapy have a much poorer prognosis and need to be identified as early as possible to lower the risk of treatment failure, avoid unnecessary toxicity, and increase the chance of long-term survival (37). About 70% of patients are cured with a prolonged course of ABVD, with or without consolidation radiotherapy, which is the first-line therapy at most centers. The more intensive BEACOPPesc cures 85%−90% of patients if given as first-line therapy but also raises serious concerns regarding acute toxicity and second malignancies (38).
Several trials investigating PET response–adapted therapy were launched recently (Table 2). Most trials involve early treatment intensification with BEACOPPesc (the Gruppo Italiano Terapie Innovative nei Linfomi trial and a European trial of response-adapted therapy in HL) (39,40) or even ASCT (the Intergruppo Italiano dei Linfomi trial) (41) in patients who still have PET-positive results after 2 cycles of ABVD. In contrast, in the BEACOPPesc-based GHSG HD18 trial, patients with advanced-stage HL in the experimental arm will be randomized to an abbreviated treatment course if they have PET-negative results after 2 cycles of BEACOPPesc (42).
PET FOR END-OF-TREATMENT RESPONSE EVALUATION IN LYMPHOMA
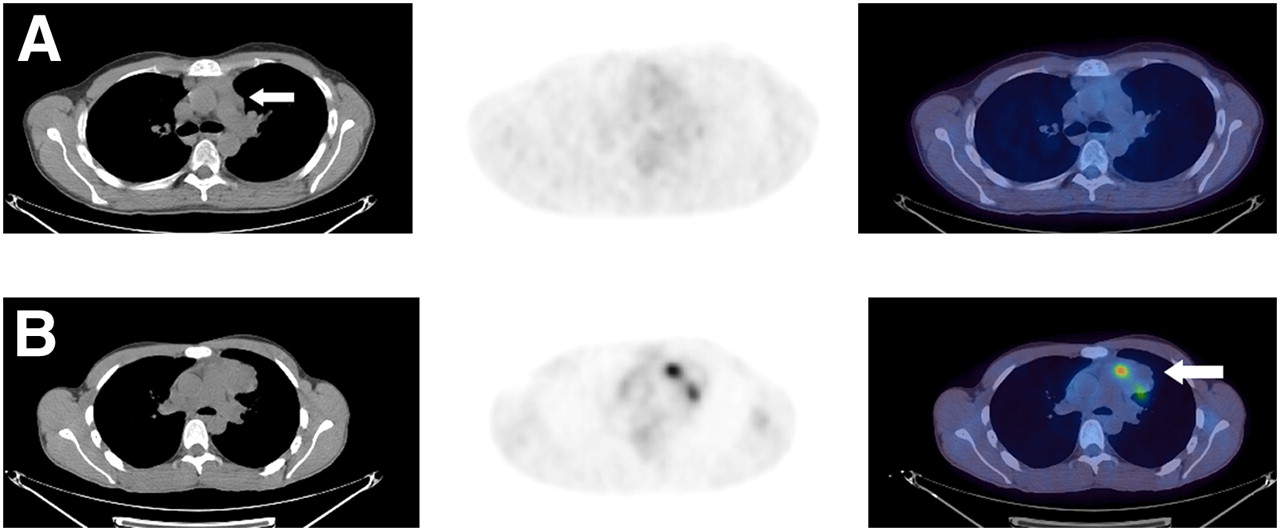
Response serves as an important surrogate for other measures of clinical benefit, such as PFS and OS. Response also serves as an important guide in decisions regarding continuation of or change in therapy. Until recently, response evaluation in lymphoma was done according to the International Workshop Criteria and the Cotswold Criteria for NHL and HL (8,43). These criteria were based mainly on morphologic changes, with a reduction in tumor size on CT being the most important factor. After the completion of therapy, CT scans often reveal residual masses. By conventional methods, it is very difficult to assess whether these masses represent viable lymphoma cells or fibrotic scar tissue. Performing a biopsy on all such lesions would be impractical and inaccurate because residual masses may contain a mixture of fibrosis and viable lymphoma cells; hence, false-negative results attributable to sampling error would be expected. Many studies have shown that 18F-FDG PET performed after treatment is highly predictive of PFS and OS in HL and aggressive NHL with or without residual masses on CT (44–72). It seems that 18F-FDG PET has the ability, at least to some extent, to distinguish between viable lymphoma cells and necrosis or fibrosis in residual masses after treatment (Fig. 4). The situation is less clear for indolent NHL, but recent articles reported a clear correlation between posttherapy 18F-FDG PET results and short-term clinical outcomes (29,73).
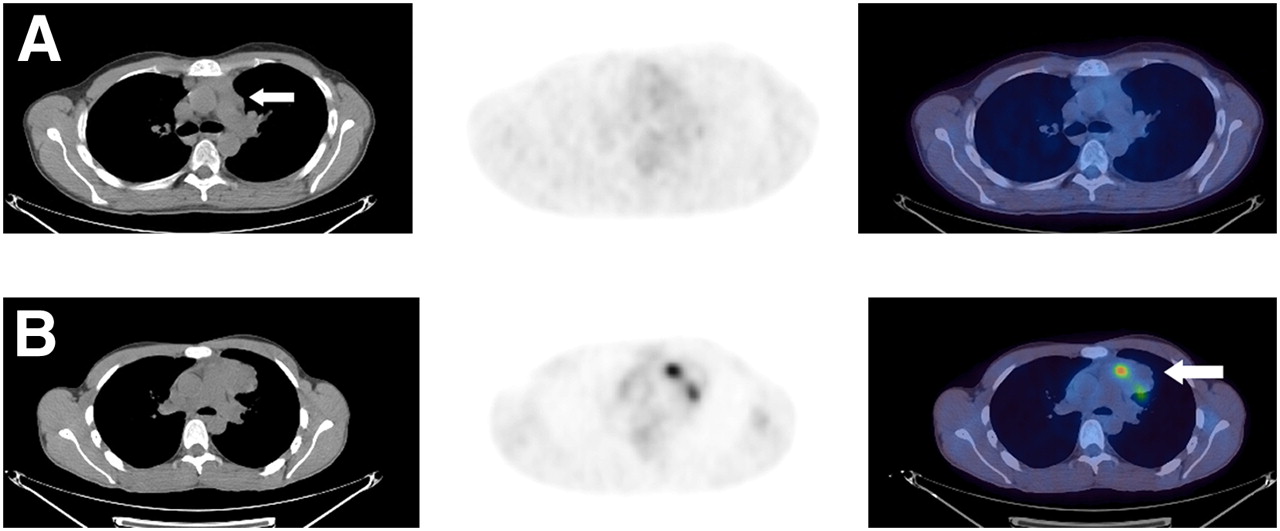
Differences between 2 patients with residual mediastinal masses after treatment. (A) No significant uptake in left anterior mediastinal mass in one patient. (B) Focal uptake in mediastinal mass, suggesting residual tumor, in another patient. Viable lymphoma cells may be contained in large areas of fibrosis, leading to sampling errors at biopsy.
On the basis of these findings, the International Harmonization Project has developed new recommendations for response criteria for aggressive malignant lymphomas, incorporating 18F-FDG PET into the definitions of end-of-treatment responses for 18F-FDG–avid lymphomas (74,75). However, it is clear that a negative 18F-FDG PET scan after therapy does not exclude the presence of microscopic disease (60). It is hoped that the number of false-negative results obtained with the new response criteria will be much smaller than the number of false-positive results obtained with the old ones, thus sparing a significant number of patients from unnecessary treatment. Recent retrospective analyses confirmed the superiority of the new response criteria for HL and aggressive NHL (76,77). However, it must be remembered that experience with response evaluation with 18F-FDG PET was obtained in patients receiving conventional treatment. Reducing treatment, for example, by abbreviating chemotherapy or omitting radiotherapy, on the basis of 18F-FDG PET results obtained before completion of the planned treatment must be regarded as an experimental approach (78). Recent data raise some concerns. In an Italian study, 160 patients with bulky HL had a PET-negative residual mass after chemotherapy (79). They were randomized to receive radiotherapy of the original bulky site or no further treatment; 14% of patients in the no-further-treatment arm relapsed within 18 mo, but only 2.5% in the radiotherapy arm did so. On the other hand, interim results in the GHSG HD15 study revealed a 94% negative predictive value of postchemotherapy 18F-FDG PET for patients who had advanced-stage HL and who received no radiotherapy, despite having at least one residual mass of more than 2.5 cm, indicating that radiotherapy can be safely omitted in patients with advanced-stage HL and PET-negative results after the end of chemotherapy (80). The new recommendations for response criteria are not yet supported by substantial amounts of clinical data, and long-term follow-up of patients with lymphoma evaluated on the basis of these criteria is awaited with great interest.
PET FOR FOLLOW-UP OF LYMPHOMA
Very few studies have investigated the value of 18F-FDG PET and 18F-FDG PET/CT in the follow-up setting. In a series of 21 HL cases studied by Dittmann et al., 18F-FDG PET was found to have no advantage over CT (52). To monitor 36 patients with HL, Jerusalem et al. used PET every 4–6 mo for 2–3 y after the completion of therapy (81). A repeat scan was performed 4–6 wk later in all patients with abnormal 18F-FDG uptake. Eleven patients had a positive 18F-FDG PET scan at some point after the completion of primary therapy. One patient had residual tumor cells, and 4 patients relapsed during 5–24 mo of follow-up. All 5 relapses were correctly identified by PET before clinical symptoms or signs, laboratory results, or CT suggested relapse. Confirmation of the relapses was obtained by biopsy in 4 patients and by CT findings and clear clinical symptoms in the remaining patient. False-positive 18F-FDG PET studies incorrectly suggested possible relapses in 6 patients, but confirmatory 18F-FDG PET studies were always negative.
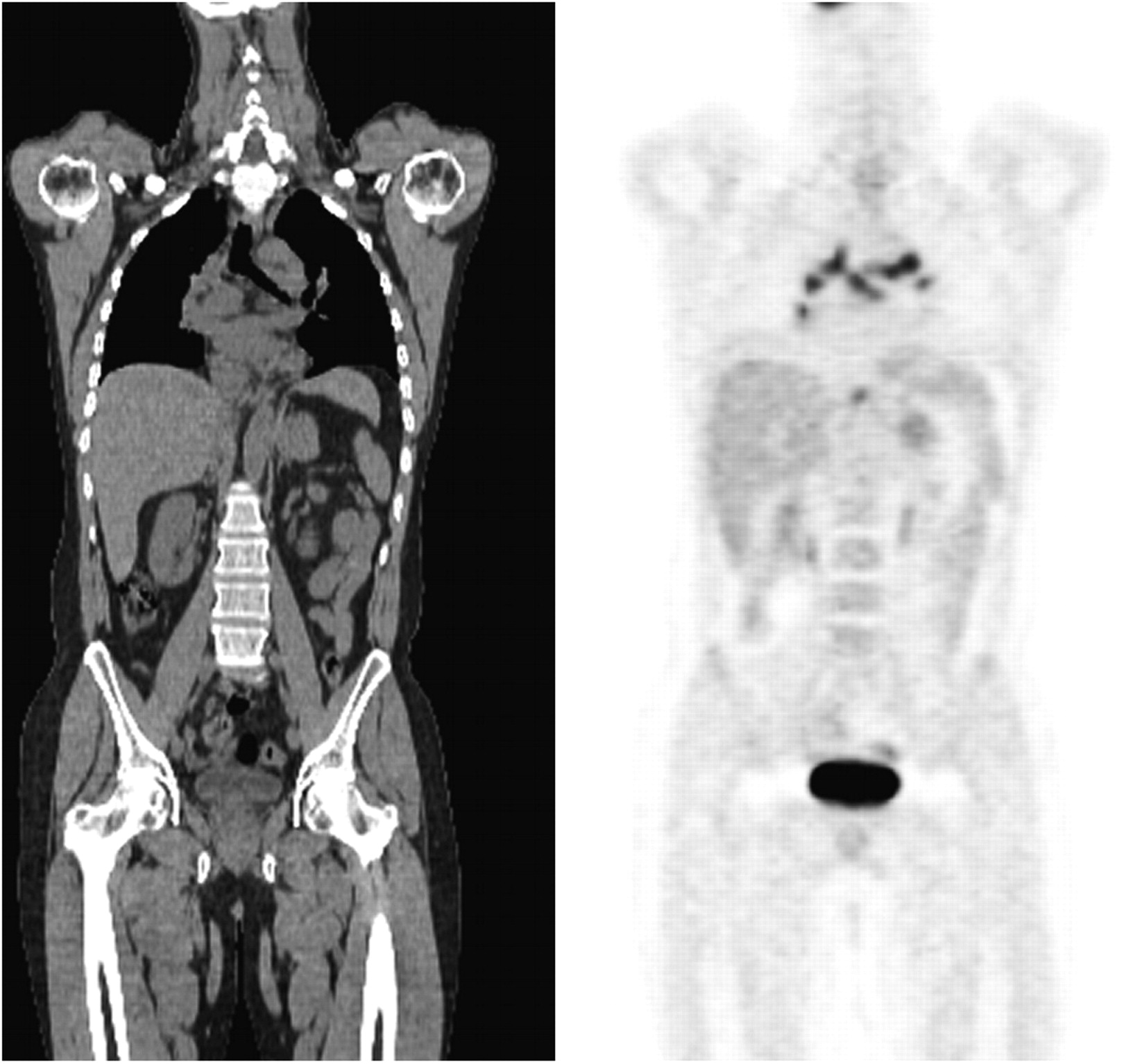
In a more recent study, Zinzani et al. retrospectively studied 151 patients with mediastinal lymphoma (HL and aggressive NHL) (82). The follow-up program for each patient included 18F-FDG PET every 6 mo for the first 2 y and then every 12 mo for a further 3 y, along with standard follow-up procedures. Positive 18F-FDG PET results suggested lymphoma relapse in 30 of 151 patients at a median of 22 mo after the completion of therapy. Histology confirmed relapse in 17 of the 30 patients, whereas either a benign condition (fibrosis [n = 9] or sarcoidlike granulomatosis [n = 3]) or an unrelated neoplasm (a thymoma) was demonstrated in the remaining 13 patients (Fig. 5). Only 3 of the 17 patients with relapse had symptoms or signs suggesting relapse at the time of the positive 18F-FDG PET scan.
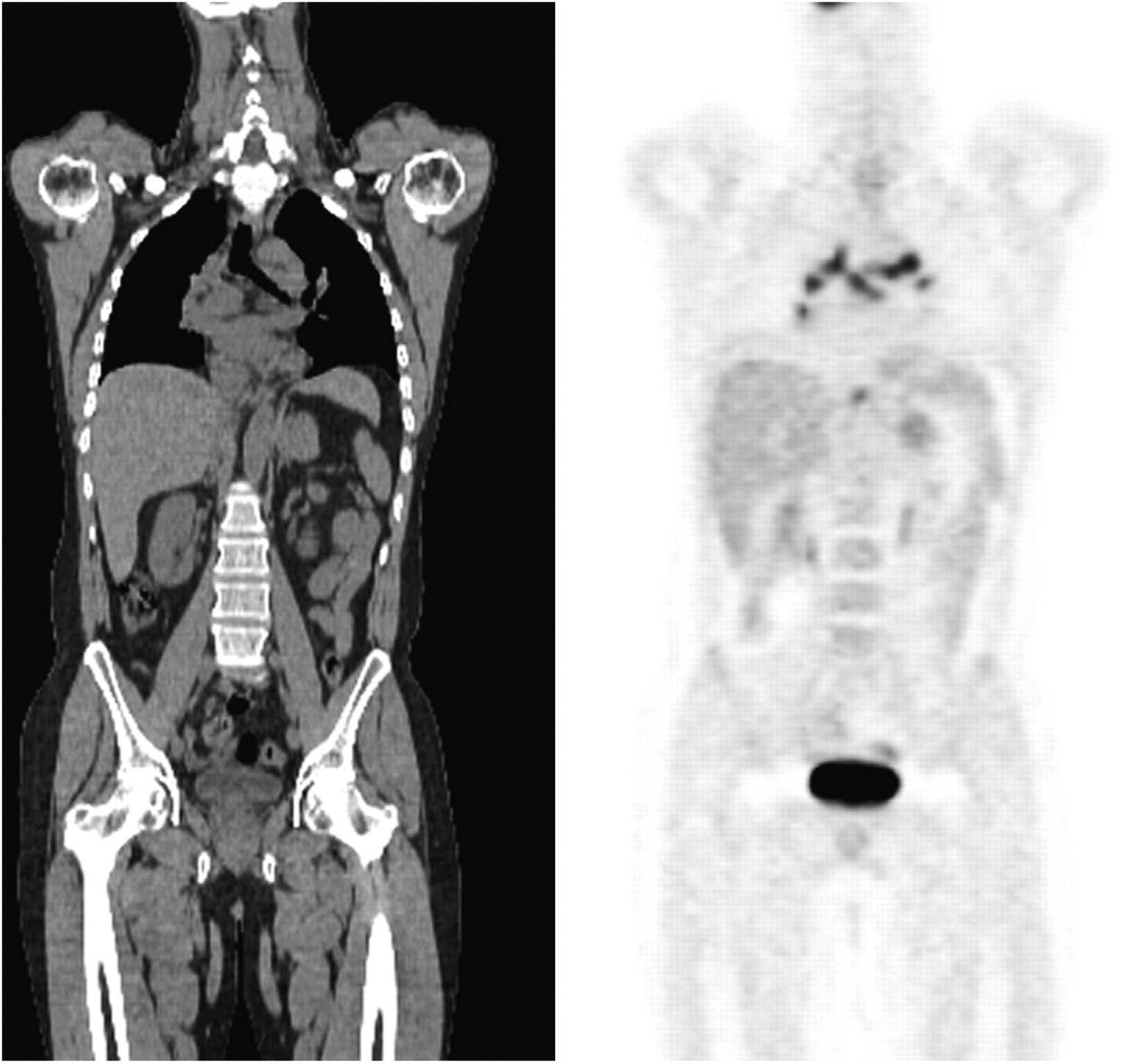
Uptake in mediastinum after treatment was attributed to sarcomatoid reaction on biopsy. Patient remains clinically well 2 y from this scan.
These studies may or may not suggest a role for 18F-FDG PET in the detection of preclinical relapse, allowing for patients to enter salvage therapy with minimal disease rather than overt relapse. For clinical situations in which a potentially curable salvage therapy is available, further studies are warranted to investigate the cost-effectiveness and the benefit for patients of 18F-FDG PET in the follow-up setting.
PET FOR RESPONSE PREDICTION BEFORE HIGH-DOSE SALVAGE THERAPY
The duration of remission before relapse and the response to induction therapy are important prognostic factors that predict good outcomes after high-dose chemotherapy with ASCT (83,84). Several studies have shown that 18F-FDG PET performed after induction therapy and just before ASCT can predict which patients will achieve long-term remission after the salvage regimen. These studies all reported short PFS in patients with persistent disease on 18F-FDG PET. However, these studies also reported a rate of false-positive results that was higher than that obtained when 18F-FDG PET was performed early during first-line therapy (85–88). The role of 18F-FDG PET in this setting is unclear, and there is no evidence to support a less-than-curative strategy despite a suboptimal metabolic response to induction therapy.
GENERAL CONSIDERATIONS AND RECOMMENDATIONS
To ensure that the results of clinical trials of 18F-FDG PET for therapy monitoring are comparable and translatable into clinical practice, it is advisable to perform scans strictly according to protocols with well-documented quality control procedures and to interpret images according to transparent, simple, and preferably uniform criteria. There have been efforts to set guidelines for the interpretation of posttherapy 18F-FDG PET for HL and aggressive NHL (75). Although those guidelines may not be based on substantial amounts of evidence and await further validation, they do represent a step in the right direction. Similar guidelines for the interpretation of interim 18F-FDG PET images are warranted, as it should be recognized that different criteria are probably needed at different time points during treatment and that reporting criteria may vary according to whether the outcome of the scan is deescalation or intensification of treatment. Indolent and aggressive lymphomas probably have very different metabolic uptake patterns and dynamics during therapy (89), and although patients with aggressive lymphomas are likely to benefit from having relevant treatment adaptations performed as early as possible, such may not be the case for indolent lymphomas. Hence, optimal timing of a treatment monitoring 18F-FDG PET scan as well as optimal reading algorithms probably vary among different lymphoma subtypes.
There are many different algorithms for the reading and reporting of interim 18F-FDG PET results. It is not clear whether semiquantitative analysis with standardized uptake values (absolute values or reduction) adds to the value of visual analysis (23). Clinicians should be well aware that 18F-FDG uptake represents a continuum and that there is a risk of losing important information if scans are reported as either “black” or “white.” We recommend an algorithm in which 18F-FDG avidity is scored relative to background uptake in the mediastinum and liver and in which reporting allows for one or more intermediate scoring groups (minimal residual uptake). This strategy allows for more clearly defined groups of truly PET-positive and PET-negative patients eligible for PET-based treatment adaptation.
To reduce the risk of false-negative and false-positive readings, it is strongly recommended that a baseline scan be available for comparison and that interim scans be performed as PET/CT with either low-dose or diagnostic CT quality. As with other oncologic indications and to reduce the risk of false-negative results attributable to metabolic stunning of tumor cells, the time from chemotherapy to scanning should be no less than 10 d (90). Because many lymphoma regimens are given at biweekly intervals, this timing represents a logistic challenge for PET response–adapted protocols. Nevertheless, we recommend that scans be interpreted by a central review panel of nuclear medicine physicians in such clinical trials.
CONCLUSION
18F-FDG PET/CT has become a standard procedure for posttreatment response evaluation for most lymphoma subtypes. It is hoped that more precise pretreatment predictive markers will be available in the future. For the time being, however, early response monitoring with 18F-FDG PET is the best tool for risk-adapted lymphoma therapy. This method may improve the outcome for patients who respond poorly to therapy and who may benefit from an early treatment adaptation. It may also allow therapy to be tailored to patients who have a low risk of treatment failure and who would otherwise receive unnecessarily toxic treatment.
Many important questions are left unanswered. The role of 18F-FDG PET in monitoring radioimmunotherapy and therapy with biologic agents is still unclear, as is the role of 18F-FDG PET in the selection of patients for maintenance therapy. With the abundance of early PET response–adapted clinical trials, there is an urgent need for uniform, evidence-based interpretation criteria and reporting guidelines for early interim 18F-FDG PET/CT. Although the prognostic value of therapy monitoring with 18F-FDG PET is well established for lymphoma, there is still no evidence that this practice improves patient outcomes. For this reason, we recommend that the use of 18F-FDG PET for response monitoring as well as follow-up takes place in the setting of clinical trials.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.
- 8.↵
- 9.↵
- 10.
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.↵
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.↵
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- Received for publication December 15, 2008.
- Accepted for publication February 16, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- 18F-FDG PET IN EARLY MONITORING OF LYMPHOMA TREATMENT
- EARLY PET RESPONSE–ADAPTED LYMPHOMA THERAPY
- PET FOR END-OF-TREATMENT RESPONSE EVALUATION IN LYMPHOMA
- PET FOR FOLLOW-UP OF LYMPHOMA
- PET FOR RESPONSE PREDICTION BEFORE HIGH-DOSE SALVAGE THERAPY
- GENERAL CONSIDERATIONS AND RECOMMENDATIONS
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Syntheses and Discovery of a Novel Class of Cinnamic Hydroxamates as Histone Deacetylase Inhibitors by Multimodality Molecular Imaging in Living Subjects
- Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group
- In Vivo Treatment Sensitivity Testing With Positron Emission Tomography/Computed Tomography After One Cycle of Chemotherapy for Hodgkin Lymphoma
- Interim 18F-FDG PET SUVmax Reduction Is Superior to Visual Analysis in Predicting Outcome Early in Hodgkin Lymphoma Patients
- Measuring tumour response: RECIST 1.1 and beyond
- How does PET/CT help in selecting therapy for patients with Hodgkin lymphoma?
- Interim PET-CT in the management of diffuse large B-cell lymphoma
- Not-So-Random Errors: Randomized Controlled Trials Are Not the Only Evidence of the Value of PET
- Oncologic PET/MRI, Part 2: Bone Tumors, Soft-Tissue Tumors, Melanoma, and Lymphoma
- Repeatability of 18F-FDG Uptake Measurements in Tumors: A Metaanalysis
- Early-Stage Hodgkin's Lymphoma: In Pursuit of Perfection
- Interim 18-FDG-PET/CT failed to predict the outcome in diffuse large B-cell lymphoma patients treated at the diagnosis with rituximab-CHOP
- Plasma thymus and activation-regulated chemokine as an early response marker in classical Hodgkin's lymphoma
- Early Repeated 18F-FDG PET Scans During Neoadjuvant Chemoradiation Fail to Predict Histopathologic Response or Survival Benefit in Adenocarcinoma of the Esophagus
- Improvement of Early 18F-FDG PET Interpretation in Diffuse Large B-Cell Lymphoma: Importance of the Reference Background
- Assessing Tumor Response to Therapy