


Abstract
This study investigated whether the reference background above which a residual mass is considered positive in the International Harmonization Project criteria should be modified for early 18F-FDG PET evaluation. Methods: In 92 patients with newly diagnosed diffuse large B-cell lymphoma, the maximal standardized uptake value (SUVmax) was measured on post–cycle 2 PET in the most intense residual mass (or, in the case of negative PET findings, in the area of most intense tumor uptake before therapy), in the mediastinal blood pool (MBP) and the liver, as potential reference background tissues. Results: With MBP as a reference (SUVmax, 2.0 ± 0.6), PET was unable to distinguish early responders from nonresponders. In contrast, with liver as a reference (SUVmax, 2.5 ± 0.7), 2-y progression-free survival was significantly different between patients with PET-negative findings (81.8% [95% confidence interval, 71%–93%]) and patients with PET-positive findings (51.8% [95% confidence interval, 35%–69%], P = 0.003). Conclusion: When assessing early response, particularly in risk-adapted therapeutic trials, it seems preferable to refer to a background tissue (liver) with a higher level of uptake than that of current international criteria (MBP) which were designed for end-of-treatment evaluation.
PET with 18F-FDG has become a powerful tool for identifying—as early as after 2 cycles of first-line chemotherapy—which patients with diffuse large B-cell lymphoma (1,2) and classic Hodgkin lymphoma (3,4) are responders. Consequently, many ongoing clinical trials focus on tailoring therapeutic strategies based on early PET as an indicator of chemosensitivity (5). Some use the International Harmonization Project interpretation criteria (6), which were current at the time of the trial design but are adapted to end-of-treatment evaluation. In diffuse large B-cell lymphoma, the GELA LNH2007-3B study (7) is evaluating a chemotherapy escalation scheme based on interim PET findings of metabolically active residual masses. However, the central-review readers have observed an unexpectedly high rate of positive findings and substantial interobserver variability using these criteria (8).
The purpose of the present study was to investigate whether the reference background above which a residual mass is considered positive in the International Harmonization Project criteria should be modified for interim PET evaluation in hopes of improving the positive predictive value and overall accuracy of interim scans in diffuse large B-cell lymphoma.
MATERIALS AND METHODS
Patients
The population consisted of 92 patients with newly diagnosed diffuse large B-cell lymphoma (9) and previously enrolled in a prospective multicenter trial designed to assess the prognostic value of early PET after 2 cycles of induction chemotherapy (2). Patient characteristics and treatment regimens have been previously described (9). Importantly, the treatment strategy was planned at inclusion according to age, International Prognostic Index, and anthracycline-based protocols currently active at that time and was not influenced by PET results. The study was approved by our institutional review board, and all patients gave informed written consent.
PET
All patients underwent 18F-FDG PET before the onset of chemotherapy (PET0) and after 2 cycles (PET2). Images were acquired on a dedicated C-PET camera (ADAC) for the first 81 patients (at Tenon Hospital) and on a Gemini PET/CT system (Philips) for the last 11 patients (at H. Mondor Hospital). The image acquisition and reconstruction parameters have been previously described (9). All patients also underwent concurrent diagnostic CT of the chest, abdomen, and pelvis within a week of each PET scan and then every 6 mo for follow-up based on the International Workshop Criteria (10). Outcome analysis was masked to the PET results.
Standardized Uptake Value (SUV) Analysis of 18F-FDG Uptake
Experience has shown that visual interpretation of images through comparison with a certain tissue background, such as the mediastinal blood pool (MBP), is prone to considerable interobserver variability but is substantially improved by using a simple semiquantitative approach in which the residual lesion is considered positive when its maximal SUV (SUVmax) exceeds that of reference background by 25% (11).
For each attenuation-corrected PET dataset, the tumor with the most intense uptake was carefully identified, relying on a graded color-scale, with red indicating the maximal count value. A volume of interest (VOI) encompassing the entire tumor was drawn to ensure correct identification of this maximum. On PET2 images, in cases of residual tumor, the VOI was drawn on the most intense focus even though its location differed from the most intense tumor on PET0. When no lesions were identifiable, the VOI was drawn on PET2 in the area of most intense tumor uptake before therapy, with careful slice-to-slice comparison with PET0. In addition, a VOI was drawn on 5 contiguous slices in the MBP (at the level of the aortic arch) and in the liver parenchyma (at mid height), making sure that VOI outlines were restricted to areas of physiologic uptake and avoiding neighboring sites of residual disease (Fig. 1). Mean SUV (SUVmean) and SUVmax were calculated in each VOI after proper calibration and normalization to body weight (9).
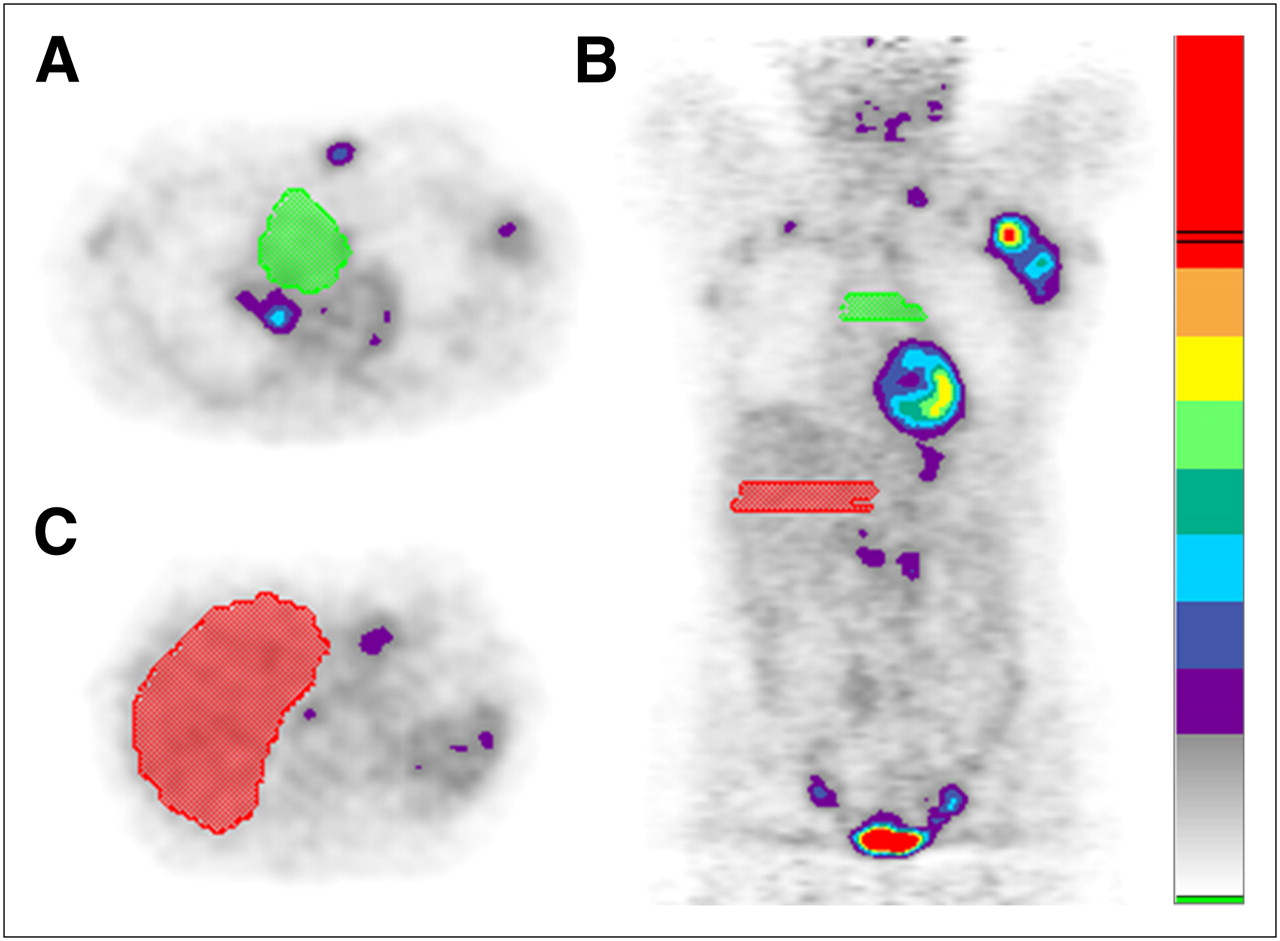
Example of VOI drawings in the 2 reference backgrounds: MBP, green outlines on axial slice (A), liver, red outlines on axial slice (C), and both on coronal slice (B).
PET2 images were considered positive when SUVmax in the residual tumor or area of initial tumor before therapy was 125% of the particular reference backgrounds investigated: SUVmax or SUVmean of the MBP or the liver. A 125% threshold was thought to best represent the mere visual impression of “higher uptake” than the background level by observer consensus because this threshold resulted in similar accuracy while minimizing the inherent interobserver variability of visual interpretation (11).
Statistical Analysis
To evaluate the early prognostic value of PET2, progression-free survival (PFS) and overall survival (OS) were chosen as endpoints. PFS was defined as the interval from the date of enrollment to the first evidence of progression or relapse. OS was defined as the interval from the date of enrollment to death from any cause. Continuous variables were compared using the Student t test, and significance was obtained when the 2-sided P value was less than 0.05. Survival curves according to visual and SUV analyses were obtained using Kaplan–Meier plots and compared using the Log rank test. In addition, receiver-operating-characteristic analysis was performed to identify the optimal threshold for predicting PFS for each category of reference background.
RESULTS
Patient Outcome
During a median follow-up period of 42 mo after inclusion, 63 patients were free from progression (PFS, 68.5%) whereas the remaining 29 progressed or relapsed, with a median delay of 6.7 mo; in addition, 71 patients survived (OS, 77.2%) whereas the remaining 21 died, with a median delay of 9.1 mo. Thirteen deaths were due to lymphoma progression, 3 to cardiac events, 3 to infectious complications, 1 to treatment toxicity, and 1 to a car accident.
Predictive Values of MBP-Based Interpretations
There was no statistically significant difference between SUVs computed from the C-PET system and those obtained from the Gemini PET/CT system for tumor, MBP, or liver on PET0 (P = 0.2–0.6) or PET2 (P = 0.1–0.4, respectively). SUVs are displayed in Table 1. SUVmax averaged 13.2 ± 4.8 on PET0 and decreased to 3.4 ± 2.7 on PET2 (4.8 ± 4.2 in patients who progressed and 2.7 ± 1.2 in those who did not, P = 0.0004).
Mean and Maximal SUVs in Most Intense Tumor, MBP, and Liver at PET0 and PET2
When MBP was taken as the reference background for positivity, with the >125% SUVmax criterion (which may be considered close to a “quantitative International Harmonization Project criterion”), PET2 was unable to distinguish early responders from nonresponders. The 2-y estimate for PFS was 76.0% (95% confidence interval [CI], 62%–90%) in the PET-negative patients, compared with 65.1% (95% CI, 51%–79%) in the PET-positive patients (P = 0.24, Fig. 2A). The accuracies of this approach for predicting PFS and OS were 52.2% and 56.5%, respectively (Table 2). Accuracies increased to 70.7% and 72.8%, respectively, when the optimal criterion, determined by receiver-operating-characteristic analysis, was >168% SUVmax. The 2-y estimate for PFS was 80.2% (95% CI, 70%–91%) in the PET-negative patients, compared with 48.1% (95% CI, 29%–67%) in the PET-positive patients (P = 0.001, Fig. 2C).

Kaplan–Meier estimates of PFS according to PET2 status: based on uptake > 125% of SUVmax in MBP (hazard ratio, 0.641; 95% CI, 0.311–1.340) (A), based on uptake > 125% of SUVmax in liver (hazard ratio, 0.348; 95% CI, 0.143–0.676) (B), based on uptake > 168% of SUVmax in MBP (hazard ratio, 0.322; 95% CI, 0.109–0.580) (C), and based on uptake > 140% of SUVmax in liver (hazard ratio, 0.264; 95% CI, 0.088–0.458) (D).
Outcome Prediction Using Different Reference Backgrounds for PET Interpretation at 2 Cycles of Chemotherapy
With SUVmean, positive predictive values (PPVs) and accuracies were always lower than those obtained with the corresponding SUVmax thresholds (>125% or receiver-operating-characteristic–optimized criterion), for PFS and for OS prediction.
Predictive Values of Liver-Based Interpretations
When liver activity was used as a reference with the >125% SUVmax criterion, PET2 was a strong predictor of survival. The 2-y estimate for PFS was 81.8% (95% CI, 71%–93%) in PET-negative patients, compared with 51.8% (95% CI, 35%–69%) in PET-positive patients (P = 0.003, Fig. 2B). The accuracies of this approach for predicting PFS and OS were 67.4% and 69.6%, respectively (Table 2). Accuracies increased to 72.8% and 75.0%, respectively, when the optimal criterion was >140% SUVmax. The 2-y estimate for PFS was 83.2% (95% CI, 73%–93%) in PET-negative patients, compared with 44.6% (95% CI, 26%–63%) in PET-positive patients (P = 0.0001, Fig. 2D).
Here again, with SUVmean, PPVs and accuracies were always lower than those obtained with the corresponding SUVmax threshold (>125% or receiver-operating-characteristic–optimized criterion), for PFS and for OS prediction.
Response Assessment with Conventional Diagnostic Methods
At the end of induction chemotherapy, 19 patients had a complete response according to CT, 50 had a complete response unconfirmed, 13 had a partial response, 2 had stable disease, 7 had progressive disease, and 1 did not undergo CT because the patient died during induction chemotherapy (Table 3).
Prediction of Chemotherapy Response (End of Induction) Using Liver-Based Early PET Interpretation
DISCUSSION
The most predictive criterion proposed so far for early PET interpretation in diffuse large B-cell lymphoma was to consider as positive (i.e., predictive of relapse) a SUVmax reduction of less than 66% between PET0 and PET2 in the most intense tumor (9). This approach dramatically reduced false-positive interpretations and, as such, is currently used in the PETAL study from the Essen group, Germany, to identify candidates for chemotherapy intensification (12). In the first 266 patients, with a median follow-up of less than 6 mo, lymphoma relapses across all International Prognostic Index risk groups have already occurred 3 times more frequently in PET2-positive than in PET2-negative patients, 23% (9/40) versus 8% (19/226), P = 0.021 (13). Importantly, this study will provide an external validation of the 66% SUVmax reduction criterion.
However, to be applicable, this criterion requires a baseline scan, which is not mandatory according to the International Harmonization Project criteria for response assessment of lymphoma and is, in fact, not routinely performed in most risk-adapted trials (6). An alternative approach investigated in the current study is to compare residual tumor uptake with an internal reference background, such as MBP or liver. SUV semiquantification was used to minimize subjectivity of PET2 interpretation as previously documented (11). Background intensities were stable between PET0 and PET2, indicating a relatively low influence of treatment regimens on MBP and liver uptake of 18F-FDG (Table 1). This finding is interesting, considering the observation that chemotherapy-induced steatosis and sinusoid obstruction affect liver imaging by CT, ultrasound, and MRI but apparently not, at least not to any significant extent, by 18F-FDG PET (14). In addition, there was little variability in the SUVs of both the liver and MBP between patients. This has been previously shown for the liver (15) and is now also shown for the MBP.
Our data clearly demonstrate that the liver is a reference background superior to MBP for early PET interpretation in diffuse large B-cell lymphoma, even when using the conservative >125% SUVmax criterion, which should perform similarly to visual interpretation of liver activity but with lower interobserver variability. Indeed, it seems justified to use a higher level of reference background because, at 2 cycles, residual “tumor” uptake likely represents a significant component of posttherapy inflammatory changes at this relatively early time after treatment, with or without a minimal amount of viable tumor cells likely to be eradicated with further treatment (16,17). Corticosteroids have been shown to help reduce the contribution of inflammatory cells to the 18F-FDG uptake and were included in our chemotherapy regimens (18). With liver uptake as the reference background (>125% SUVmax), PPV reached 48.6% for PFS prediction, corresponding to a reduction of 15 false-positives, compared with MBP in the same setting. The difference between MBP and liver uptake was only 0.5 units in terms of SUVmax (2.0 ± 0.6 vs. 2.5 ± 0.7, respectively) but was sufficient to reduce false-positives. Interestingly, the >125% SUVmax liver criterion resulted in performance similar to our previously published custom visual analysis allowing minimal residual uptake (9).
Receiver-operating-characteristic analysis has identified optimal thresholds (e.g., >168% of MBP SUVmax, >140% of liver SUVmax) leading to higher predictive values and accuracies. Obviously, these figures cannot be transposed to a visual scale of interpretation, but they strengthen the message that liver appears a better reference organ than MBP for early PET interpretation. Although the positive predictive value of the >140% liver SUVmax criterion remains lower than those obtained by measuring the SUV reduction or by waiting 2 additional cycles, this criterion results in a better sensitivity and slightly higher negative predictive value (9,19). With the caveats of the somewhat different outcome measure (PFS vs. event-free survival) evaluated using the >140% liver SUVmax criterion, SUV reduction after 2 cycles and SUV reduction after 4 cycles, the difference in overall accuracy between these 3 approaches was relatively small (72.8%, 76.1%, and 77.5%, respectively). For OS prediction, the accuracies were 75.0%, 84.8%, and 80.0%, respectively, but here again the higher accuracy with the SUV reduction (due to higher PPV) was at the expense of substantially lower sensitivity (66.7% for the >140% liver SUVmax criterion vs. 52.4% and 52.9% for SUV reduction at 2 and 4 cycles, respectively).
The concept of minimal residual uptake has been used in many studies, but its definition varies. For Mikhaeel et al., minimal residual uptake was defined as a focus of low-grade uptake in an area of previously noted disease, likely to represent inflammation but for which small-volume malignancy could not be excluded (20). Therefore, minimal residual uptake was a “gray zone” with intermediate prognosis, such as the “complete remission unconfirmed” category of conventional assessment (10). The definition of minimal residual uptake was more stringent in Hodgkin lymphoma: for Gallamini et al., the definition was uptake equal to or slightly higher than the MBP, with an SUV between 2.0 and 3.5 (3). In this case, minimal residual uptake was considered a negative finding. Finally, an international consensus for early PET evaluation has recently been reached favoring the use of the London criteria, which emphasize comparison of residual uptake with liver uptake (21). The London criteria are currently being validated and have already shown moderate to fair interobserver agreement (22,23).
CONCLUSION
For assessment of early response, particularly in risk-adapted therapeutic trials, it seems preferable to refer to a background with a higher level of uptake (the liver) than that of the current international criteria (the MBP), which were designed for end-of-treatment evaluation. This approach warrants further validation in larger clinical trials.
Acknowledgments
We thank the entire team of the AP-HP PET center at Tenon Hospital, Paris, especially Prof. Jean-Noël Talbot, for their help with C-PET imaging. This study was supported by the Délégation à la Recherche Clinique de l'Assistance Publique-Hôpitaux de Paris (PHRC-AOM00152), the Société Française de Radiologie (SFR), and the Association pour la Recherche sur le Cancer (ARC).
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication July 2, 2010.
- Accepted for publication September 8, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Validation of the {Delta}SUVmax for Interim PET Interpretation in Diffuse Large B-Cell Lymphoma on the Basis of the GAINED Clinical Trial
- Application of the Lugano Classification for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The PRoLoG Consensus Initiative (Part 2--Technical)
- Application of the Lugano Classification for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The PRoLoG Consensus Initiative (Part 1--Clinical)
- Follicular Lymphoma Treated with First-Line Immunochemotherapy: A Review of PET/CT in Patients Who Did Not Achieve a Complete Metabolic Response in the GALLIUM Study
- Interim PET in Diffuse Large B-Cell Lymphoma
- Interim PET Evaluation in Diffuse Large B-Cell Lymphoma Using Published Recommendations: Comparison of the Deauville 5-Point Scale and the {Delta}SUVmax Method
- Quantitative Assessment of Interim PET/CT Could Have More Prognostic Relevance than Visual Assessment for Predicting Clinical Outcome of Extranodal Diffuse Large B Cell Lymphoma
- FDG-PET-driven consolidation strategy in diffuse large B-cell lymphoma: final results of a randomized phase 2 study
- Interim PET-driven strategy in de novo diffuse large B-cell lymphoma: do we trust the driver?
- Evaluation of Diffusion-Weighted Magnetic Resonance Imaging for Follow-up and Treatment Response Assessment of Lymphoma: Results of an 18F-FDG-PET/CT-Controlled Prospective Study in 64 Patients
- Reply to B. Bennani-Baiti et al, H.J.A. Adams et al, E. Laffon et al, and E.A. Hawkes et al
- The importance of harmonizing interim positron emission tomography in non-Hodgkin lymphoma: focus on the Deauville criteria
- The predictive role of interim positron emission tomography for Hodgkin lymphoma treatment outcome is confirmed using the interpretation criteria of the Deauville five-point scale
- Interim 18F-FDG PET SUVmax Reduction Is Superior to Visual Analysis in Predicting Outcome Early in Hodgkin Lymphoma Patients
- Early Determination of Prognosis by Interim 3'-Deoxy-3'-18F-Fluorothymidine PET in Patients with Non-Hodgkin Lymphoma
- Interim PET-CT in the management of diffuse large B-cell lymphoma
- SUVmax reduction improves early prognosis value of interim positron emission tomography scans in diffuse large B-cell lymphoma