


Abstract
This study evaluated the role of 18F-FDG PET as an early predictor of histopathologic response to neoadjuvant chemoradiotherapy and overall survival in patients with adenocarcinoma of the esophagus undergoing multimodal therapy. Methods: Thirty-seven patients with locally advanced adenocarcinoma of the esophagus underwent pretreatment and an intratreatment 18F-FDG PET scan in the second week of a 6-wk regimen of neoadjuvant chemoradiotherapy. Histopathologic response and overall survival were correlated with percentage change in 18F-FDG uptake (%Δmaximum standardized uptake value [%ΔSUVmax]). Results: In 16 patients (43%), treatment induced a histopathologic response (<10% viable tumor cells), which was associated with a significant (P < 0.05) survival benefit. The optimal reduction in 18F-FDG uptake, which separated histopathologic responders and nonresponders, was a −26.4% ΔSUVmax (receiver-operating-characteristic curve analysis). At this separation, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy (area under the receiver operating characteristic curve) were 62.5%, 71.4%, 62.5%, 71.4%, and 67.4%, respectively, for intratreatment 18F-FDG PET scans. Kaplan–Meier survival analysis of 18F-FDG PET responders (>26.4% reduction in SUVmax), compared with 18F-FDG PET nonresponders (<26.4% reduction in SUVmax), revealed no survival benefit for responders (P = 0.6812). Conclusion: The %ΔSUVmax during the second week of induction chemoradiation did not correlate either with histopathologic response or with survival. Our results show that, in contrast to published reports on neoadjuvant chemotherapy, combined chemoradiotherapy in patients with adenocarcinoma of the esophagus lowers the predictive accuracy of early repeated 18F-FDG PET in identifying histopathologic responders and those with chances for increased survival below clinically applicable levels.
Neoadjuvant chemotherapy alone or combined with radiation therapy is increasingly the standard of care for locally advanced esophageal cancer (1,2). A complete pathologic response after induction therapy is associated with a cure rate of approximately 60%, and a complete pathologic response or histopathologic response, defined as less than 10% residual viable tumor cells, is achieved in up to 50% of patients (1). Conversely, no response to neoadjuvant treatment may detrimentally affect survival (1–3). Consequently, there has been considerable interest in recent years in identifying patients before treatment or early during treatment who are going to benefit from induction therapy, with a particular focus on sequential metabolic imaging and a search for biomarkers or predictive gene array patterns (4). For chemoradiotherapy regimens, this focus has particular importance in view of recent trials suggesting equivalent outcomes in patients who have chemoradiation alone, compared with multimodal regimens, for esophageal squamous cell cancer (5,6).
18F-FDG PET/CT has become increasingly a standard staging modality for esophageal and junctional tumors. Studies have been extended in recent years to explore whether sequential metabolic imaging during neoadjuvant regimens may predict histopathologic response or resistance to the induction regimen. These studies may enable new trials and treatment regimens based on an understanding of metabolic imaging during neoadjuvant regimens, with potentially overall improved outcomes from individually tailored treatment regimens. In the seminal study on neoadjuvant chemotherapy, Weber et al. (7) evaluated the role of early 18F-FDG PET response in patients with esophageal adenocarcinoma and correlated change in 18F-FDG uptake with histopathologic response and survival. A metabolic threshold of a more than 35% reduction from baseline maximum standardized uptake value (SUVmax) was established, allowing the prediction of a clinical response with a sensitivity and specificity of 93% and 95%, respectively. The same group subsequently validated this threshold in other studies, concluding that metabolic changes within the first 2 wk of induction chemotherapy correlated with histopathologic response and overall survival (8–10).
In contrast to consistent studies with neoadjuvant chemotherapy alone, the predictive value of a second 18F-FDG PET scan obtained during or after induction chemoradiotherapy is inconsistent and controversial. Wieder et al. (11), also from the Munich group, studied 38 patients with squamous cell cancer receiving neoadjuvant chemoradiotherapy and, using a 30% reduction in SUVmax as a threshold, reported a high sensitivity (93%) and specificity (88%) for a second 18F-FDG PET scan after 2 wk of induction therapy. Conversely, in a previous study from this institution in a cohort that included patients with squamous cell cancer and adenocarcinoma, a second 18F-FDG PET scan after 1 wk of chemoradiotherapy had a positive predictive value of just 27% and negative predictive value of 71%, thus appearing to be of little prognostic value (12). Moreover, when a second 18F-FDG PET scan was obtained at the end of induction chemoradiotherapy, Schmidt et al. (from the University of Cologne) failed to show a significant association of changes in standardized uptake value (SUV) with clinical or histopathologic response after the completion of induction chemoradiotherapy (13–15).
Neoadjuvant chemoradiotherapy before surgery is the standard of care in this institution for locally advanced adenocarcinoma of the esophagus and adenocarcinoma of the esophagus type I and type II junctional tumors (1). In this study, we aimed to determine whether a second 18F-FDG PET scan obtained during the second week of a 3-wk course of radiation could predict histopathologic response and survival. Although our study initially targeted 70 patients, we closed the study on the basis of data analysis from 37 patients.
MATERIALS AND METHODS
From September 2003 to December 2007, 37 patients (31 men, 6 women) with newly diagnosed and untreated locally advanced biopsy-proven adenocarcinoma of the esophagus or junction were enrolled in this study (mean age ± SD, 58 ± 9 y [age range, 37–73 y]). Locally advanced was defined as a predicted cT3/T4 N0/1 based on CT of the neck, thorax, abdomen, and pelvis; esophagogastroscopy; endoscopic ultrasound; and whole-body 18F-FDG PET/CT. Patients who had previously received either chemotherapy or radiotherapy or demonstrated 18F-FDG PET uptake consistent with radiation-induced esophagitis were excluded (Fig. 1). The study was approved by the Institutional Review Board, and all patients gave written consent. All patients underwent 18F-FDG PET for pretreatment staging, and intratreatment 18F-FDG PET scans were obtained approximately 2 wk after the start of their neoadjuvant chemoradiotherapy, at a mean of 12 ± 2 d.

(A) Prechemoradiotherapy 18F-FDG PET scan (arrow indicates focal uptake in primary tumor). (B) Intratreatment 18F-FDG PET scan (arrow indicates diffuse or bandlike uptake in esophagus [radiation-induced esophagitis]).
Treatment Regimen
Neoadjuvant chemoradiotherapy was administered in the following manner: combination chemoradiotherapy at week 1, radiotherapy alone at weeks 2 and 3, a break in treatment at weeks 4 and 5, and chemotherapy alone at week 6, as previously described (1). 5-Fluorouracil (5-FU) was delivered at a dose of 15 mg/kg daily on days 1–5, followed by cisplatin at a dose of 75 mg/m2 on day 6. The 18F-FDG PET/CT scan and endoscopy report and results of a barium swallow at the time of CT simulation were used to outline the gross tumor volume (16). The radiotherapy planning target volume incorporated the gross tumor volume, with a 4- to 5-cm margin superiorly and inferiorly and a 2-cm margin circumferentially. A total dose of 40 Gy in 15 daily fractions (not including weekends) was delivered to the mid plane using 10- to 15-MV photons. At a minimum of 4 wk after completion of neoadjuvant chemoradiotherapy, patients were restaged by CT and esophagogastroscopy. Surgery was only undertaken when each patient's neutrophil count was above 2,000/μL on 3 successive occasions over a 2-wk period, no significant deterioration in their performance status was observed, and repeated CT did not reveal progressive disease deemed unresectable.
18F-FDG PET/CT
Whole-body scans extending from the base of the skull to the mid thigh were acquired with a PET Advance scanner (n = 12 patients) or Discovery ST PET/CT scanner (n = 25 patients) (GE Healthcare) before the start of chemoradiotherapy (pretreatment), with an intratreatment 18F-FDG PET scan 2 wk later (range, 9−14 d; mean ± SD, 12 ± 2 d). At this time, patients had received a mean of 23.4 ± 2.9 Gy of the planned 40-Gy radiotherapy dose (Table 1). Each patient was imaged with the same scanner on both occasions.
Patients’ Pathologic Stage, Tumor Response, 18F-FDG PET Parameters, Radiation Dose, and Survival Data
18F-FDG PET images were acquired in 2-dimensional mode, starting approximately 60 min (range, 48−104 min) after the intravenous administration of 350−450 MBq of 18F-FDG, with minimal difference in uptake time between the pretreatment and intratreatment 18F-FDG PET scans (mean Δtime ± SD, 6 ± 4 min; Table 1). Patients fasted for at least 6 h before 18F-FDG administration. For all scans, patients’ blood glucose levels were less than 10 mmol/L.
Images were reconstructed using ordered-subset expectation maximum iterative reconstruction. Semiquantitative measurements of 18F-FDG uptake in pretreatment and intratreatment scans were compared to assess metabolic response to chemoradiotherapy. For optimal reproducibility and accuracy, the tumor 18F-FDG uptake was measured using a region-of-interest method (17). A cylindric region of interest with a diameter of 1.5 cm was manually placed over the tumor on the hottest transaxial slice (slice thickness, 3.27 mm), avoiding the edges of the tumor in both the pretreatment and the intratreatment 18F-FDG PET scans. The mean activity concentration within the region of interest on the hottest transaxial slice was determined and expressed as decayed corrected activity administered to the patient (SUVmax). This technique has the advantage of little interference from statistical counting-rate fluctuations (because of the use of mean values) or from nonviable tumor zones or tumor borders (which result in reduced SUVmax measurements due to partial-volume effects). All SUVmax measurements were normalized for patient body weight. The relative change in tumor SUVmax between the pretreatment and intratreatment 18F-FDG PET scans (percentage change in SUVmax [%ΔSUVmax]) was calculated and correlated with subsequent histopathologic tumor response and survival.
Histopathology
One experienced histopathologist who had no prior knowledge of the clinical or 18F-FDG PET data analyzed the resected esophagectomy section stained with hematoxylin and eosin. Each surgical specimen was examined for the extent of residual cancer (i.e., tumor histopathologic response), depth of invasion, and lymph node involvement. The criteria established by the International Union Against Cancer and the American Joint Committee on Cancer were used to grade and stage the specimens (18). Tumor response was initially graded according to the 5-point tumor-regression grade (TRG) system defined by Mandard et al. (19), with TRG 1 noted as the best response. Histopathologic responders were defined as those patients in whom less than 10% residual viable tumor cells were found in the tumor bed (TRG 1−2) and nonresponders as those in whom more than 10% residual viable tumor cells were found in the tumor bed (TRG 3−5).
Statistical Analysis
Statistical analysis was performed using commercial software (MedCalc for Windows [Microsoft], version 9.6.4.0; MedCalc Software). All quantitative data are expressed as mean ± SD. The Mann–Whitney test was used to compare tumor 18F-FDG uptake in histopathologic responder and nonresponder groups. Receiver-operating-characteristic (ROC) curve analysis was used to define the optimal cutoff or separation point in the data that could most accurately predict response in our patient group. For this cutoff or separation point, sensitivity, specificity, positive predictive value, and negative predictive value were calculated using standard formulas. Accuracy was measured as area under the ROC curve. Survival rates were calculated according to the Kaplan–Meier method. Statistical comparisons between the 2 groups of patients were performed with a log rank test. P values were considered statistically significant when less than 0.05.
RESULTS
Correlation of Histopathologic Response and Patient Survival
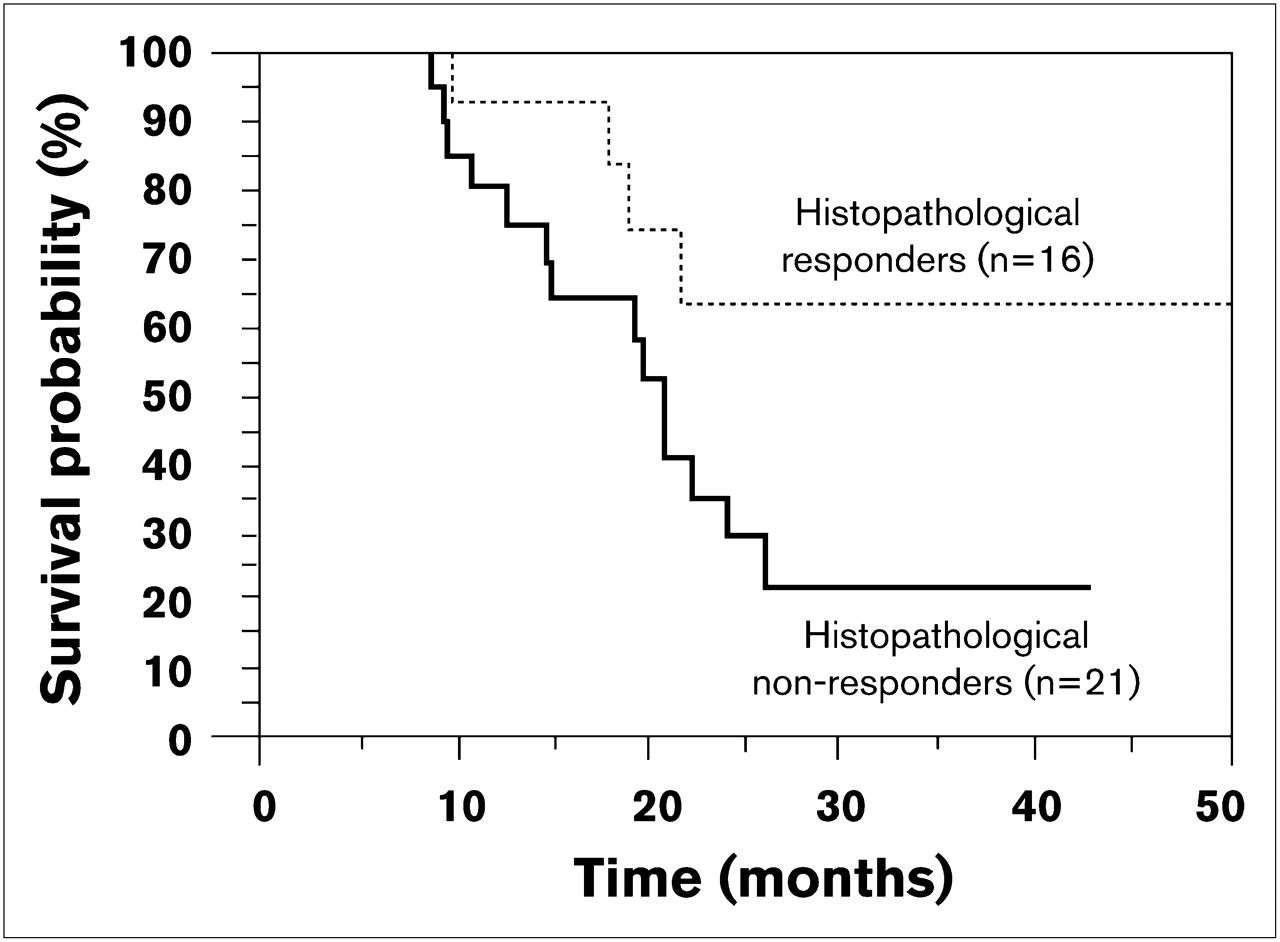
In the 37 surgical tumor specimens, there were 16 histopathologic responders (43%) and 21 nonresponders (57%). Responders, compared with histopathologic nonresponders, had a significant (P = 0.047) survival benefit (Fig. 2). After a median follow-up of 47 mo, median survival was not reached for histopathologic responders and the median survival for histopathologic nonresponders was 21 mo (P < 0.0001).

Kaplan–Meier analysis of overall survival in terms of histopathologic response. Compared with histopathologic nonresponders, histopathologic responders have improved survival (P = 0.047).
Correlation of Tumor 18F-FDG Uptake with Histopathologic Response
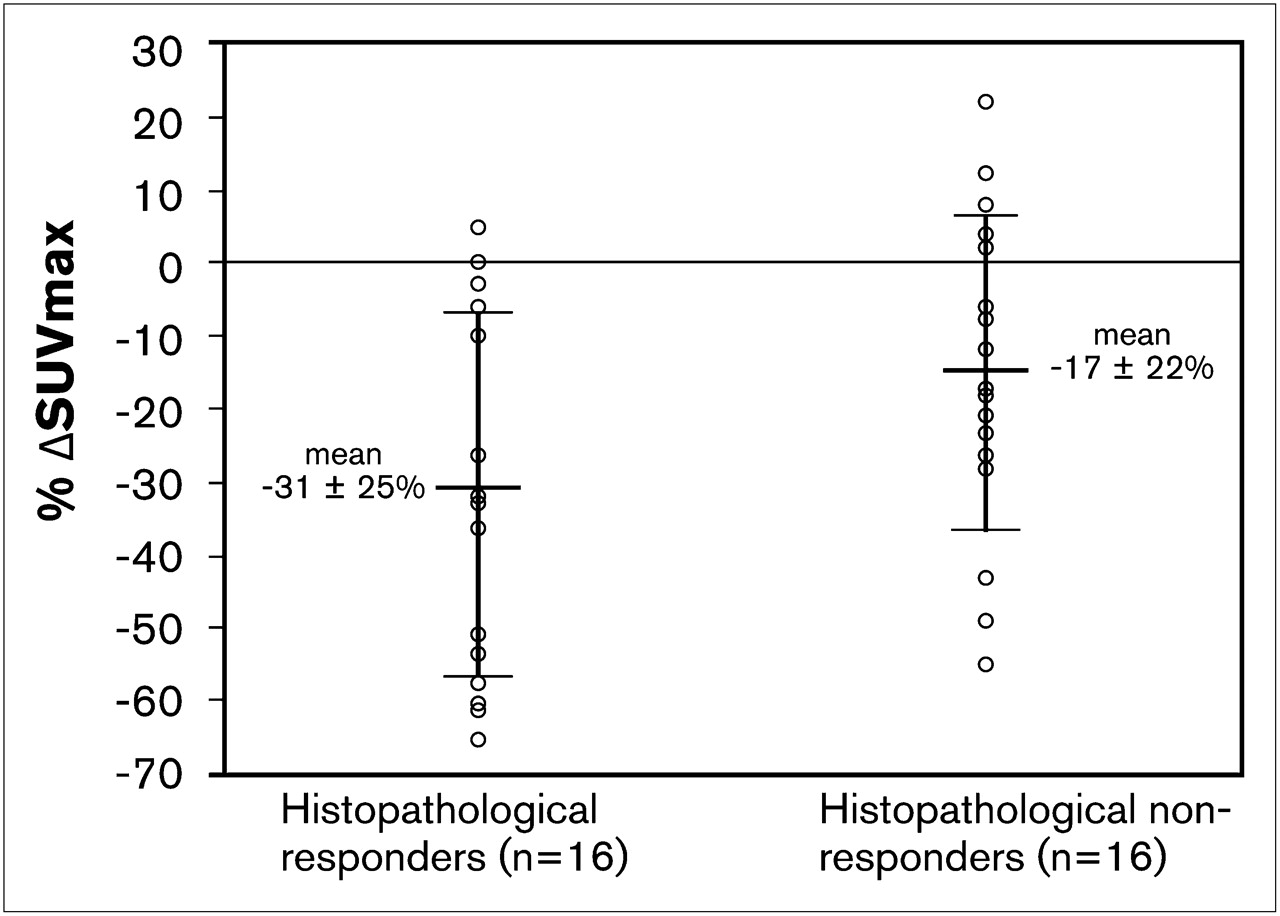
In the histopathologic responder group (n = 16), the SUVmax fell from 10.0 ± 5.5 before treatment to 6.2 ± 3.2 after 2 wk of neoadjuvant chemoradiotherapy. In the nonresponder group (n = 21), the SUVmax fell from 8.4 ± 3.7 before treatment to 6.7 ± 3.3 during chemoradiotherapy. Histopathologic responders had a greater reduction in %ΔSUVmax than histopathologic nonresponders, but there was a considerable overlap between the 2 groups (Fig. 3).
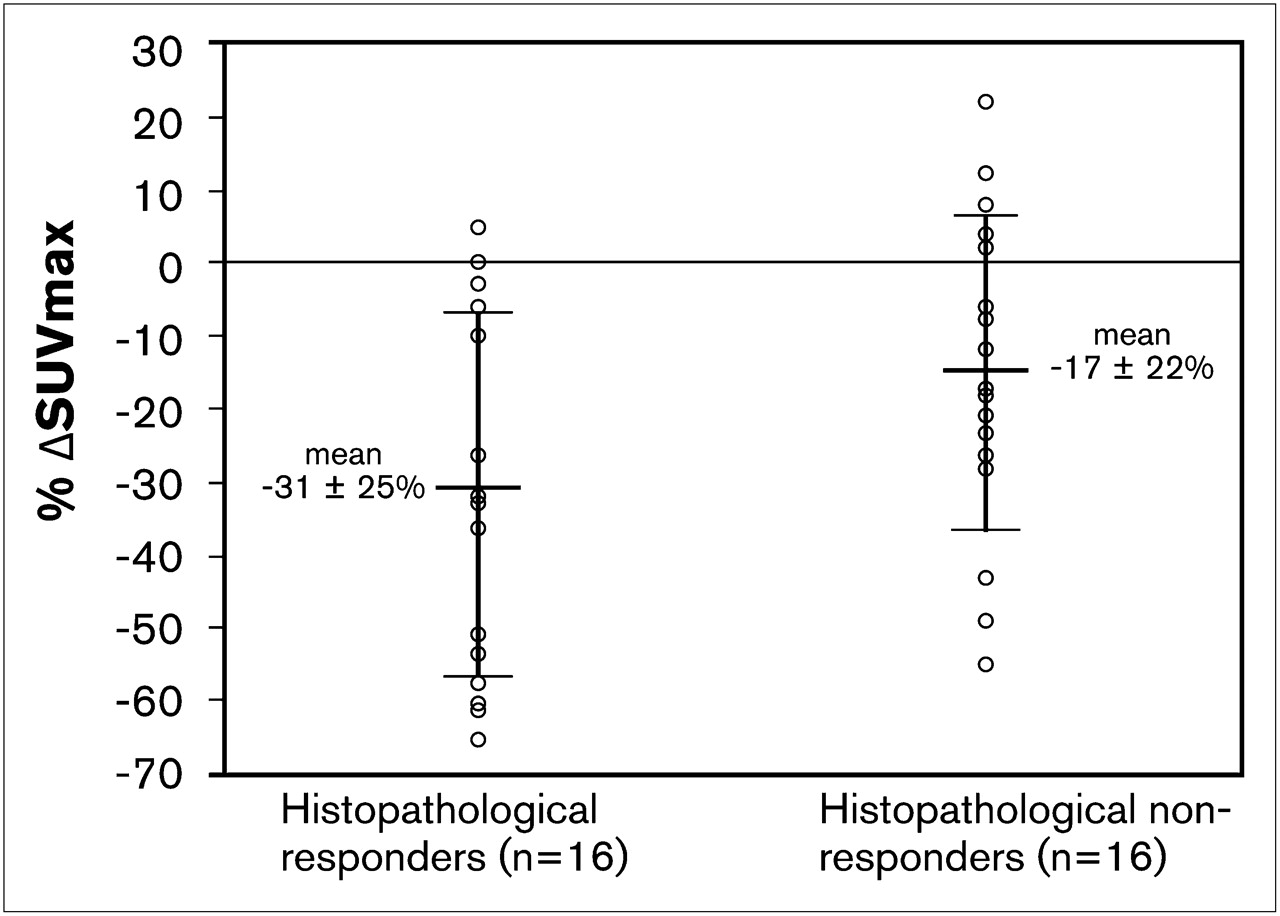
Relative changes in 18F-FDG uptake (%ΔSUVmax) between pretreatment and intratreatment PET scans for histopathologic responders and nonresponders. Error bars denote SD.
ROC analysis identified that the optimal separation of the 2 groups was a reduction in SUVmax of −26.4% (Fig. 4). At this separation, the sensitivity of the test was 62.5% (95% confidence interval [CI], 35.5%–84.7%), specificity 71.4% (95% CI, 47.8%–88.6%), positive predictive value 62.5% (95% CI, 34.6%–85.3%), and negative predictive value 71.4% (95% CI, 47.2%–89.0%). The overall accuracy of the test was 67.4% (95% CI, 50.1%–81.9%), as measured by the area under the ROC curve.

ROC curve analysis for prediction of response. ROC curve analysis identified optimal point of separation as change in SUVmax of −26.4%. At this separation, sensitivity is 62.5%, specificity is 71.4%, positive predictive value is 62.5%, negative predictive value is 71.4%, and accuracy (area under ROC curve) is 67.4%.
Correlation of Tumor 18F-FDG Uptake with Survival
Kaplan–Meier survival analysis at the separation of −26.4% ΔSUVmax is shown in Figure 5A; 18F-FDG PET responders (n = 16) had a median survival of 21 mo and 18F-FDG PET nonresponders (n = 21) a median survival of 24.1 mo (P = 0.6812). Survival data were also analyzed using a previously published separation value of −35% ΔSUVmax (7–9) (Fig. 5B). At this separation value, 18F-FDG PET responders had a median survival of 19.1 mo, and the 18F-FDG PET nonresponders had a median survival of 24.1 mo (P = 0.3715).

(A) Kaplan–Meier analysis of overall survival in terms of PET response. 18F-FDG PET responders (n = 16), compared with 18F-FDG PET nonresponders (n = 21), did not demonstrate increased survival (P = 0.6812) with cutoff %ΔSUVmax of −26.4% to define PET response. (B) 18F-FDG PET responders (n = 12), compared with 18F-FDG PET nonresponders (n = 25), did not demonstrate increased survival time (P = 0.3715) with a cutoff %ΔSUVmax of −35% to define PET response.
DISCUSSION
The prognosis for patients with esophageal carcinoma is poor; accordingly, there has been enormous interest in the use of neoadjuvant and adjuvant therapies in an attempt to improve the dismal outcomes associated with surgery alone. Neoadjuvant therapy may improve treatment outcomes for some patients (1,2), and there is emerging interest in sequential metabolic response measurement using 18F-FDG PET as a surrogate marker of histopathologic response and survival for cancer (20–24). For esophageal cancer, the value of sequential metabolic imaging in patients who receive neoadjuvant chemotherapy has been demonstrated in several studies from the Munich group, and this principle was adapted in the MUNICON trial (9). In contrast, studies of neoadjuvant combination radiation and chemotherapy have been conflicting (11,12,14). In this study, in which 43% of patients on the treatment regimen achieved a histopathologic response, the intratreatment %ΔSUVmax had a poor predictive value for histopathologic response and survival, suggesting that adding radiotherapy to the treatment regime results in unreliable predictive results from intratreatment change in 18F-FDG uptake.
Several factors may result in discordance between studies and needed to be considered in this study before we could confidently draw conclusions based on our analysis. First, SUV measurement is not a standardized technique, and methods can vary widely. SUVs are influenced by many factors, including 18F-FDG uptake time, blood glucose levels, reconstruction algorithm, and the number of pixels sampled. This study compared SUVmax in 2 scans (pretreatment and intratreatment) in which the scanning parameters were as similar as possible to facilitate direct comparison. The technique provides a high degree of reproducibility, which is of particular importance when comparing small changes in SUVmax between 2 scans. The data were also analyzed using several alternative semiquantitative measurements for 18F-FDG accumulation (i.e., metabolic tumor volume, SUVmax in a single pixel, mean SUV in the whole tumor volume, total tumor glycolysis), none of which improved the correlation with either histopathologic response or survival. Accordingly, the method used to measure SUV is unlikely to be a factor in the failure of early repeated 18F-FDG PET scans to predict histopathologic response and survival.
The timing of the second scan may also be relevant. If the scan is obtained too early, the effects of neoadjuvant therapy on carbohydrate metabolism may not have peaked, whereas if obtained too late, a radiation-induced inflammatory flare may mask the findings (25). The mean duration of 12 d of neoadjuvant treatment (range, 9−14 d) in this study before the second scan is comparable with other studies, but to narrow the interval spread, we reanalyzed our data, excluding patients for whom the second scan was obtained less than 10 d from the start of chemoradiotherapy. The results (data not shown) show no significant improvement in sensitivity and specificity (69% and 58%, respectively), and this is consequently unlikely to be a significant factor.
Third, the selection of cutoff SUVmax may be important, because a range of cutoff values defining therapy response during chemotherapy or chemoradiation has been used by other authors, broadly varying from a −20% to a −35% reduction in 18F-FDG uptake (7–15,23,24). We reanalyzed our data using both our optimal cutoff value of −26.4% and a selected cutoff value of −35% ΔSUVmax, which is cited in previous early-response 18F-FDG PET studies and defines the standard in the MUNICON trial (7–9). Neither cutoff value resulted in any separation approaching significance (P = 0.6812 and 0.3715, respectively).
The interval to surgery after neoadjuvant therapy may also be relevant. Schiepers et al. (26) have shown that radiotherapy reduces neoplastic cell numbers in tumors but does not eliminate proliferation in the remaining viable cell fraction, and a longer delay may affect the histopathologic response. To comply with the clinical requirements set out in this study, some of our patients had the time from the end of chemoradiotherapy to surgery prolonged. The range, between 25 and 91 d, was longer than the 28−42 d described by Wieder et al. (11). Excluding patients whose surgery was performed beyond 52 d left 9 histopathologic responders and 11 nonresponders. The sensitivity, specificity, and accuracy in this more comparable group was minimally changed at 78%, 64%, and 73%, respectively, compared with 62.5%, 71.4%, and 67.4% in the total group.
Finally, the neoadjuvant regimen itself may be a factor. Chemotherapy and radiotherapy are both known to affect carbohydrate metabolism in tumor cells, and 18F-FDG is being used as a biomarker of carbohydrate metabolism. In vitro studies have shown an early transient rise in 18F-FDG uptake after exposure of tumor cell lines to chemotherapy; however, a similar reactive chemotherapy flare in vivo with resultant increase in SUV measurements is not described (27). In contrast, in addition to directly affecting tumor cell metabolic activity, radiotherapy can induce an inflammatory cell reaction, with focal accumulation of inflammatory cells in the radiotherapy-treated zone and associated increased uptake of 18F-FDG in these nontumor cells (26,28). 18F-FDG PET is unable to distinguish whether tracer uptake is associated with inflammatory cells or residual viable tumor cells. Therefore, during radiotherapy treatment if an inflammatory response occurs, 18F-FDG will be taken up by the inflammatory cells and may mask the reduced 18F-FDG uptake in the responding tumor cells. This inflammatory response may result in reduced specificity, sensitivity, and predictive value and may be a factor in this study; nonetheless, this response does not explain the discordance between the findings in this study and the Wieder study. Chemotherapy has been reported to suppress local inflammatory response, and the recovery of the response after cessation of therapy is substantial after 5 d (29). In the study by Wieder et al. (11), chemotherapy was administered daily for 28 d (5-FU, 300 mg/m2), concurrently with radiotherapy; consequently, the intratreatment 18F-FDG PET scan was acquired while the patient was receiving chemotherapy. In this study, chemotherapy was administered for 6 d—5-FU (15 mg/kg) for the first 5 d and cisplatin on the sixth day—and the intratreatment 18F-FDG PET scan was obtained 3–8 d after the cessation of chemotherapy. A possible explanation for the difference may be that the continued chemoradiotherapy in Wieder's study suppressed the inflammatory response to radiation therapy, in contrast to this study, in which chemotherapy was discontinued before the intratreatment 18F-FDG PET scan.
CONCLUSION
Neoadjuvant chemoradiation in locally advanced esophageal adenocarcinoma resulted in a histopathologic response in 43% of patients and an associated survival benefit. An early sequential intratreatment 18F-FDG PET scan (%ΔSUVmax) did not predict histopathologic response or survival with sufficient clinical accuracy (ROC accuracy, 67%). A radiotherapy-induced inflammatory response is most likely affecting the results. The chemotherapy regime we used in our study may be the determining factor that contributed to the negative findings. These data raise awareness that the chemotherapy regime used in neoadjuvant chemoradiotherapy may reduce the effectiveness of the early 18F-FDG PET test in predicting response and outcome.
Acknowledgments
The study was funded by internal funds of the Department of Clinical Surgery, St. James's Hospital.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 31, 2010.
- Accepted for publication August 30, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}