


Abstract
Several recent reports have described the judgment of chemotherapeutic effects on malignant lymphomas by use of 18F-FDG PET as early as a few courses after the initiation of chemotherapy. However, the optimal timing of 18F-FDG PET has yet to be clarified. Earlier 18F-FDG PET, such as day 1 after chemotherapy, may be affected by inflammation or chemotoxicity in addition to chemotherapeutic effects, but the ways in which uptake is changed are as yet unclear. We therefore examined changes in 18F-FDG PET results on day 1 after the initiation of chemotherapy for malignant lymphoma. Methods: Twelve patients with non-Hodgkin’s lymphoma were enrolled in this study. 18F-FDG PET was performed before therapy to determine baseline results and then was repeated at day 1 and day 20 after the initiation of chemotherapy (just before the initiation of the second course of chemotherapy) and at the end of chemotherapy. We selected 1–9 regions of interest (ROIs) from each patient and calculated the corrected standardized uptake value (SUVcor) by subtracting the SUV of surrounding normal tissue for a semiquantitative analysis. From the ROIs in each patient, the representative SUVcor with the highest SUVcor at baseline was selected, and the mean representative SUVcors for all 12 patients at baseline, day 1, day 20, and the end of chemotherapy were evaluated. Changes in the representative SUVcor were compared by use of paired t tests (2-tailed P values of <0.05 were considered statistically significant). Results: All representative SUVcors for each patient were lower on day 1 than at baseline, and the mean ± SD representative SUVcor for all patients was significantly decreased from 10.7 ± 7.9 at baseline to 5.8 ± 5.8 at day 1 (P = 0.0002; paired t test). On day 20, the mean ± SD SUVcor was 0.7 ± 1.0, showing a further decrease from the value at day 1 (P = 0.01). Although the mean ± SD SUVcor tended to decrease again to 0.4 ± 0.7 by the end of chemotherapy compared with the value at day 20, no significant difference was identified (P = 0.37). Conclusion: 18F-FDG uptake decreased as early as day 1 after the initiation of chemotherapy, indicating that 18F-FDG PET for initial diagnosis or staging must be performed before the onset of chemotherapy, as scan results might already be severely compromised after the first day.
Use of 18F-FDG PET has proven very effective for the diagnosis and posttherapeutic follow-up of malignant lymphoma. Several recent reports have described the judgment of chemotherapeutic effects on malignant lymphomas by use of 18F-FDG PET as early as 1 or 2 courses after the initiation of chemotherapy (1–6). However, the optimal timing of 18F-FDG PET has not yet been clarified. 18F-FDG PET at an earlier time, such as 1 d after the initiation of chemotherapy, may be affected by inflammation or toxicity in addition to chemotherapeutic effects, but the ways in which uptake is changed are generally unclear. We therefore examined changes in 18F-FDG PET results 1 d after the initiation of chemotherapy for malignant lymphoma. Yamane et al. previously reported that abnormal uptake on 18F-FDG PET in 4 patients with malignant lymphoma was already decreased 1 d after the initiation of chemotherapy (7), and the present report describes further experiments with 18F-FDG PET 1 d after the initiation of chemotherapy in a larger population.
MATERIALS AND METHODS
Materials
Twelve patients (5 men and 7 women; age range, 32–81 y; mean ± SD, 63.8 ± 14.0 y) with non-Hodgkin’s lymphoma were enrolled in this study. Lymphomas were primary in 7 patients and relapsed in the remaining 5 patients.
All patients were histopathologically diagnosed after biopsy or surgery. Tumor classifications comprised B-cell follicular lymphoma (n = 7), B-cell diffuse lymphoma (n = 4), and T-cell lymphoma (n = 1). All patients provided written informed consent before every 18F-FDG PET study.
Study Design
18F-FDG PET was performed before therapy to determine baseline results and was repeated at day 1 and day 20 after the initiation of chemotherapy (just before initiation of the second course of chemotherapy) and at the end of chemotherapy.
18F-FDG PET Scanning
Patients were asked to fast for at least 4 h before undergoing 18F-FDG PET. Patients received an intravenous injection of 18F-FDG at 3.0–4.0 MBq/kg and then rested for about 60 min. Just before scanning was done, patients were encouraged to void to minimize bladder activity attributable to renal excretion of 18F-FDG.
18F-FDG PET was performed by use of an Advance PET scanner (GE Medical Systems). One-frame emission scans were obtained with a 2-min acquisition time at every table position, and transmission scans were obtained with a 1-min acquisition time by use of 68Ge pin sources rotating around the body. A total of 7 or 8 frames were acquired to cover from the thigh to the top of the head on each scan in 2-dimensional mode. PET images were reconstructed by use of an ordered-subset expectation maximization iterative reconstruction algorithm.
Data Analysis
Regions of interest (ROIs) were visually selected as those displaying intense uptake on baseline 18F-FDG PET. We selected 1–9 ROIs from each patient, for a total of 56 ROIs from all 12 patients. For follow-up studies at day 1, day 20, and the end of chemotherapy, we visually set the same ROI as close to that of the baseline study as possible to compare changes in uptake even if regional 18F-FDG uptake were no longer increased. Tracer uptake in ROIs was measured by use of the maximum standardized uptake value (SUVmax) for a semiquantitative analysis. The corrected SUV (SUVcor) was calculated by subtracting the SUV of surrounding normal tissue or of tissue opposite the ROIs from the SUVmax of the ROIs, as the SUVmax alone does not correctly reflect tumor activity in regions in which the SUV is low or the background uptake is high.
From the ROIs in each patient, the representative SUVcor with the highest SUVcor at baseline was selected, and the mean representative SUVcors for all 12 patients at baseline, day 1, day 20, and the end of chemotherapy were evaluated. Changes in the representative SUVcor between the baseline and day 1, day 1 and day 20, and day 20 and the end of chemotherapy were compared by use of paired t tests (2-tailed P values of <0.05 were considered statistically significant).
RESULTS
Table 1 shows patient data, including Ann Arbor classification, number of ROIs, and SUVcors. Figures 1–3 show 18F-FDG PET images from 3 representative patients (patients 2, 5, and 12). Figure 4 shows changes in the representative index for the ROI with the highest SUVcor at baseline 18F-FDG PET for all 12 patients at baseline, day 1, day 20, and the end of chemotherapy.
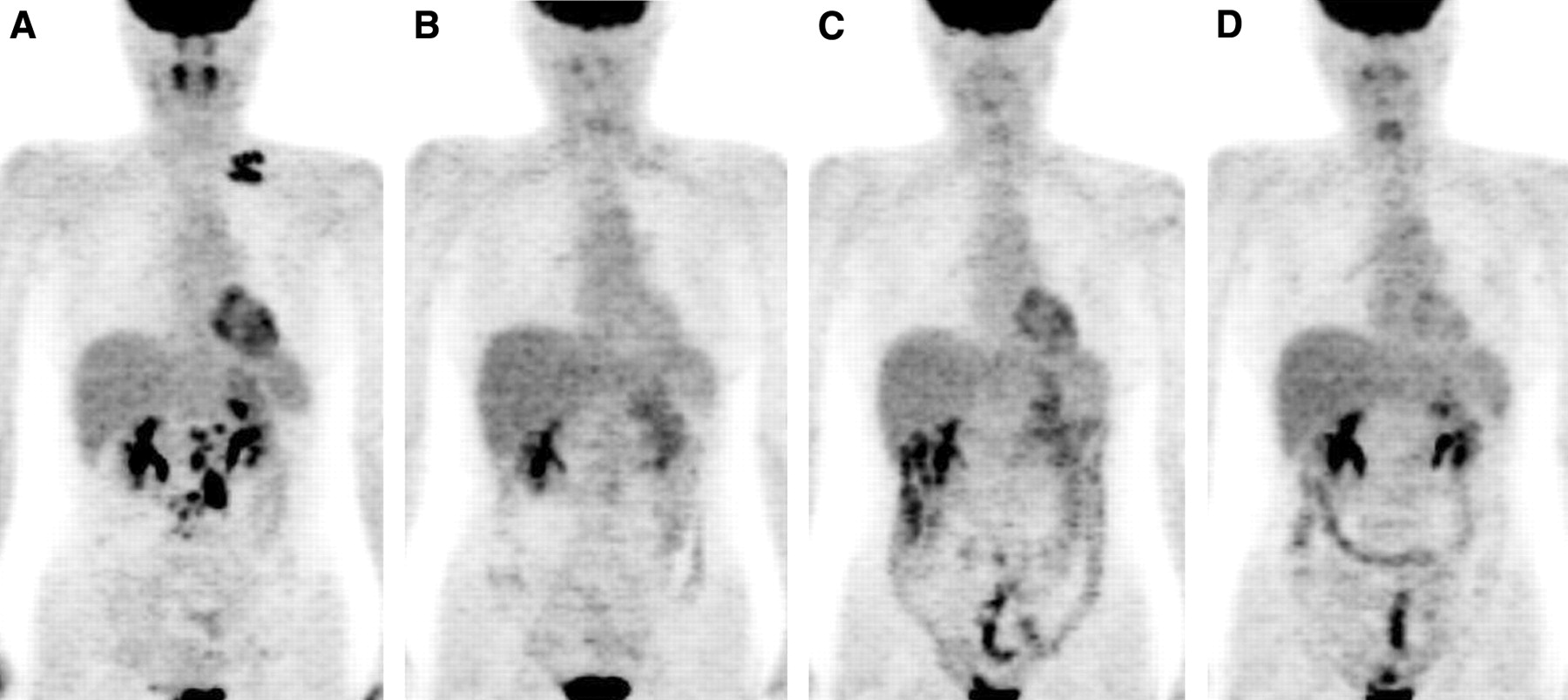
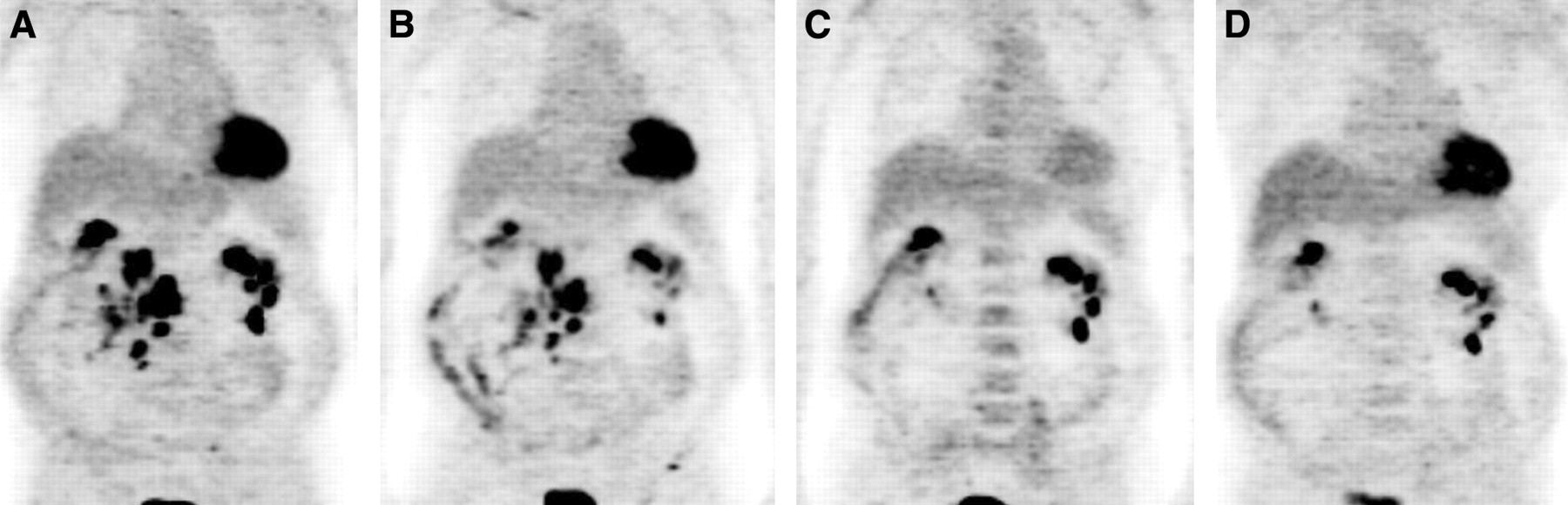
Results for patient 2, a 52-y-old woman with a B-cell diffuse large lymphoma. (A) A baseline 18F-FDG PET image revealed increased activity in left subclavicular and paraaortic abdominal nodes. (B) At day 1, almost all abnormal uptake was sharply reduced. (C) At day 20, although bowel uptake was seen, abnormal uptake in lymph nodes was negligible. (D) At the end of chemotherapy, abnormal uptake to lymph nodes was not apparent.
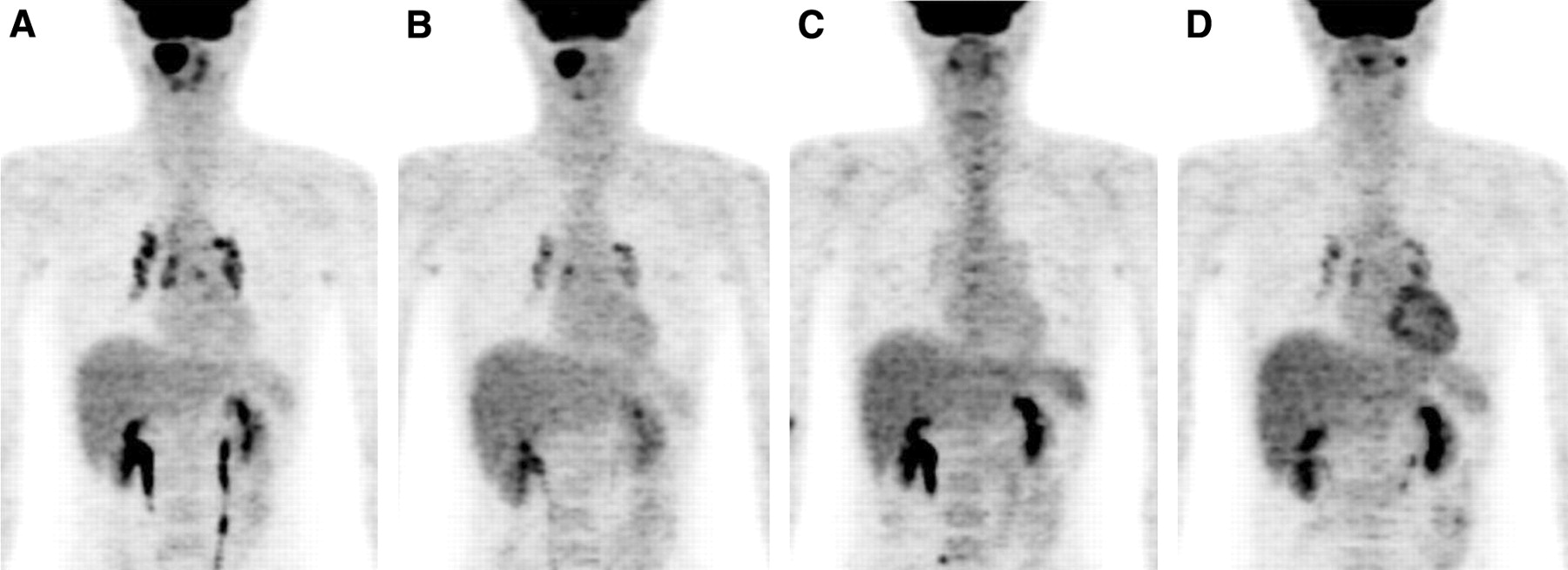
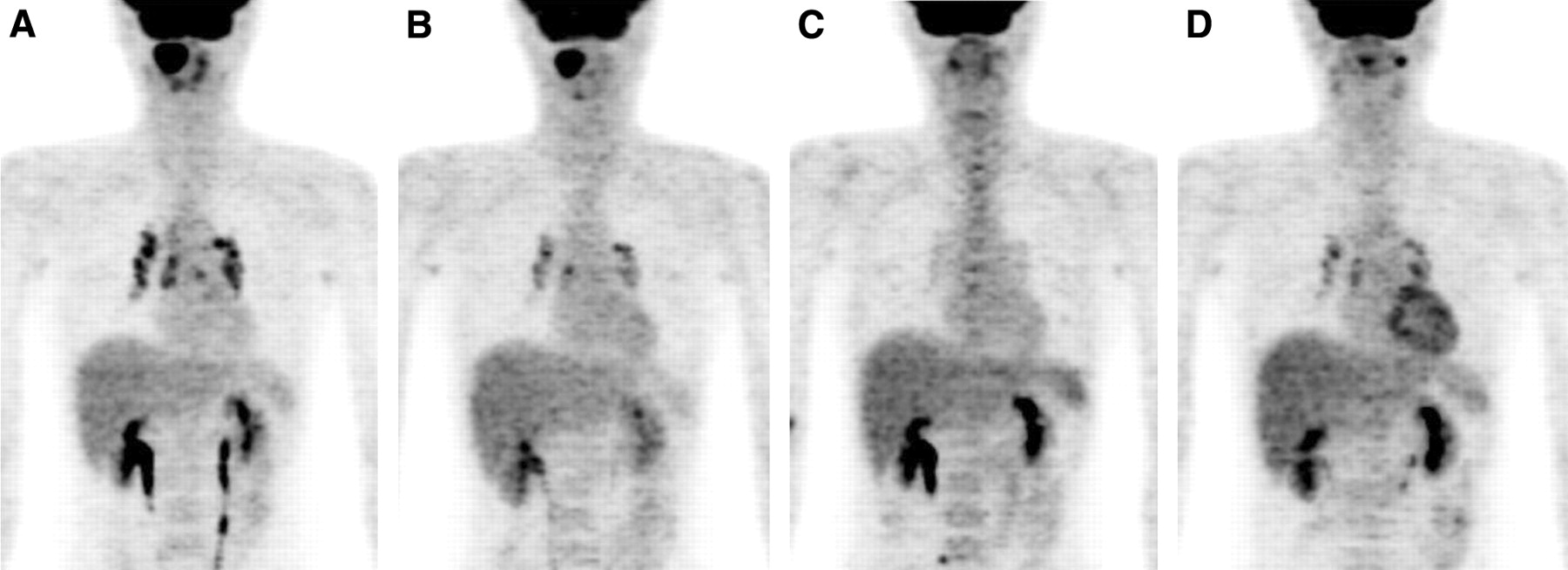
Results for patient 5, a 32-y-old man with a B-cell diffuse large lymphoma. (A) A baseline 18F-FDG PET image revealed increased activity throughout the right nasal cavity and mediastinal nodes. (B) At day 1, abnormal uptake in the nasal cavity was visually identical to that at baseline, but uptake in the mediastinum was decreased. (C) At day 20, the 18F-FDG image was basically normal, with slightly abnormal uptake in the nasal cavity or mediastinal nodes. (D) At the end of chemotherapy, uptake in the mediastinal nodes reappeared, but uptake in the nasal cavity remained normal.
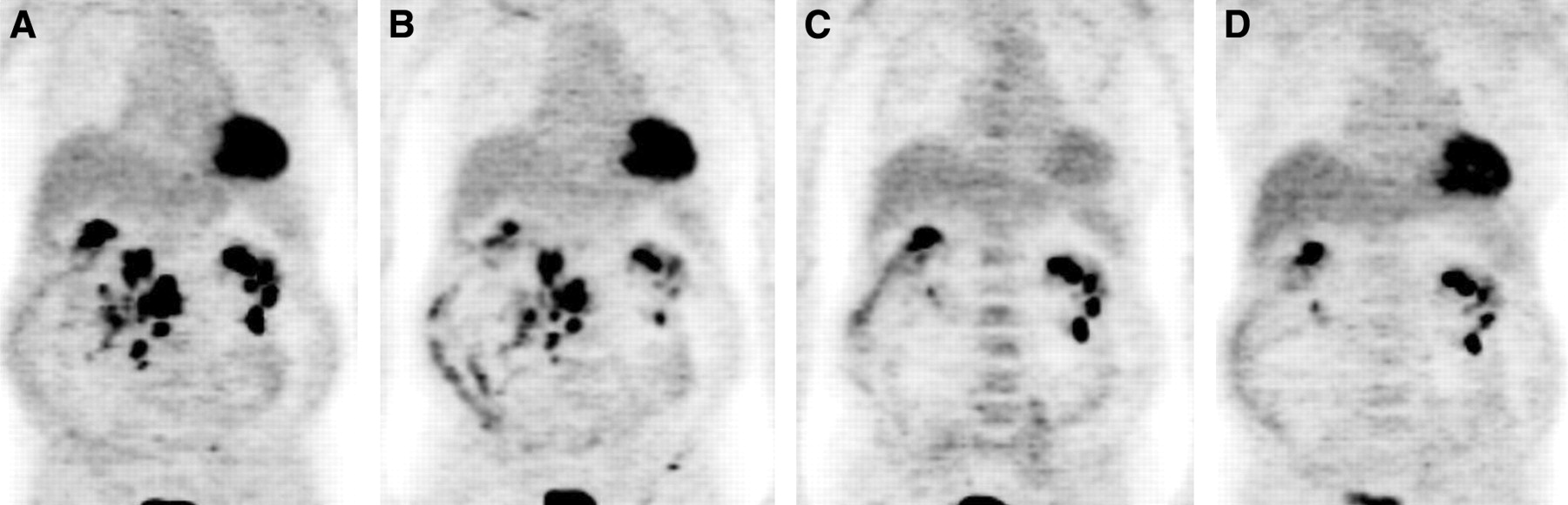
Results for patient 12, a 76-y-old man with a B-cell diffuse mixed lymphoma. (A) A baseline 18F-FDG PET image revealed multiple foci of increased activity in mesenteric lymph nodes. (B) At day 1, uptake in mesenteric lymph nodes was visually identical to that at baseline. (C) At day 20, abnormal uptake disappeared. Renal uptake was unclear because of the presence of multiple renal cysts. (D) At the end of chemotherapy, the 18F-FDG image showed no abnormal uptake.

Changes in the representative index for the ROI with the highest SUVcor at baseline 18F-FDG PET for all 12 patients at baseline, day 1, day 20, and the end of chemotherapy. Compared with that at baseline, the SUV at day 1 was significantly decreased (P = 0.0002, paired t test). The SUV at day 20 was further significantly decreased compared with that at day 1 (P = 0.01), but no significant difference was observed between day 20 and the end of chemotherapy (P = 0.37). N/S = nonsignificant.
Patient Data, ROIs, and SUVcors
On day 1, all representative SUVcors for each patient were lower than those at baseline, and the mean ± SD representative SUVcor for all patients was significantly decreased from 10.7 ± 7.9 at baseline to 5.8 ± 5.8 at day 1 (P = 0.0002, as determined by paired t test). The representative SUVcor was further decreased in 11 patients at day 20 and was stable in the remaining patient. The mean ± SD representative SUVcor for all patients was 0.7 ± 1.0 at day 20, a value significantly lower than that at day 1 (P = 0.01, as determined by paired t test). At the end of chemotherapy, the representative SUVcor was decreased in 4 patients, increased in 2 patients, and stable in the remaining 6 patients. The mean ± SD representative SUVcor for all 12 patients was 0.4 ± 0.7 at the end of chemotherapy, and no significant difference was observed compared with that at day 20 (P = 0.37).
DISCUSSION
18F-FDG PET is a very useful method for evaluating the response to chemotherapy for malignant lymphoma, and an early analysis of chemotherapeutic effects should prove useful for planning subsequent therapy. Hoekstra et al. (1) performed 18F-FDG scintigraphy by using a conventional γ-camera within days after the initiation of chemotherapy in 5 patients with malignant lymphomas and reported that effective treatment sharply reduced metabolic tumor activity before a volume response. Spaepen et al. (2) described a significant association between the disappearance of uptake at midtreatment 18F-FDG PET (3 or 4 courses after the initiation of chemotherapy) and both progression-free survival and overall survival in patients with aggressive non-Hodgkin’s lymphoma. Jerusalem et al. (3) reported that 18F-FDG PET after 2–5 courses of chemotherapy could predict complete remission, progression-free survival, and overall survival. Furthermore, Mikhaeel et al. (4) reported that 18F-FDG PET after 2 or 3 courses of chemotherapy for malignant lymphoma could predict long-term outcomes. Kostakoglu et al. (5) described 18F-FDG PET after 1 course (3–10 d) of chemotherapy as being predictive of the 18-mo outcome in patients with aggressive non-Hodgkin’s lymphoma and Hodgkin’s disease. However, Römer et al. (6) reported that for 18F-FDG PET at 7 and 42 d after the initiation of chemotherapy, the results at 42 d correlated better with the nonillness period than did those at 7 d.
Some trials investigating the early judgment of chemotherapeutic effects for malignant tumors other than malignant lymphomas have been reported. In a breast cancer study (8), prompt decreases were observed in the rate of 18F-FDG influx, compared with basal levels, after 8 d of treatment and in the estimated rate of 18F-FDG phosphorylation to 18F-FDG-6-phosphate, antedating any decrement in tumor size. In a study examining treatment responses to chemotherapy in patients with relapsed germ cell tumors (9), 18F-FDG PET after 2 or 3 courses of chemotherapy was more predictive of outcomes than was CT or serum tumor marker levels. Cremerius et al. (10) also studied patients with relapsed germ cell tumors but concluded that 18F-FDG PET must be performed at least 2 wk after the completion of chemotherapy because of a loss of sensitivity and diagnostic accuracy.
Although the optimal timing for the early judgment of chemotherapeutic effects has been discussed for several kinds of malignant tumors other than lymphomas, no clear solutions have been determined. Moreover, as no well-regulated clinical studies regarding metabolic changes 1 d after the initiation of chemotherapy have been reported, changes in 18F-FDG uptake just after the start of chemotherapy represent an intriguing subject.
The present 12 patients, in addition to the 4 patients previously reported by Yamane et al. (7), displayed significantly decreased 18F-FDG uptake 1 d after the initiation of chemotherapy. However, in an examination of causes for changes in 18F-FDG uptake, the effects of inflammation or increased energy consumption in compensation for toxic stress or apoptosis must be considered in addition to the effects of chemotherapy on decreased tumor cell proliferation.
Spaepen et al. (11) reported that 18F-FDG uptake in animal models 1 d after the start of chemotherapy correlated well with decreased tumor activity because of the absence of inflammatory cells, whereas 18F-FDG uptake 8 d after the start of chemotherapy did not correlate as closely with tumor activity because of the appearance of inflammatory reactions. Haberkorn et al. (12) treated rats in a Morris hepatoma model with gemcitabine and reported increases in 18F-FDG uptake immediately after treatment and decreases to normal values by 24 h. This increase in glucose uptake soon after therapy was interpreted as resulting from stress reactions by tumor cells, protecting cells from apoptosis during the early period after the exposure to cytotoxic elements. Conversely, Dittmann et al. (13) studied cells derived from human esophageal squamous cell carcinomas and incubated with cisplatin or 5-fluorouracil. The uptake of 18F-fluorothymidine after 24 h decreased in cells treated with cisplatin and increased in cells treated with 5-fluorouracil. However, the uptake of 18F-FDG did not differ significantly from control values, suggesting that 18F-FDG uptake after chemotherapy does not correlate with cell proliferation and that metabolic dynamics differ for various pharmacotherapies. As several kinds of drugs are used to treat malignant lymphomas, 18F-FDG dynamics soon after the administration of chemotherapy may be greatly complicated by the behaviors of specific drugs. 18F-FDG PET for initial diagnosis or staging therefore probably should be performed before the initiation of chemotherapy, as scan results after the first day might already be severely compromised.
The 18F-FDG activity used in the present investigation (3.0–4.0 MBq/kg) is lower than that usually used in studies of this kind, and we know that this protocol with a short scan time has drawbacks when SUV comparisons are made by statistical means. However, we can usually obtain satisfactory images for diagnosis in routine 18F-FDG PET studies with this protocol, and the possibility of a decreased SUV on day 1 in all 12 patients representing a statistical error is extremely unlikely. To address these issues, we are planning further studies to clarify the suitability of this protocol.
Clarification of the relationship between the change in uptake on day 1 and progression-free survival, overall survival, or histopathologic type was not possible given the small patient population and the limited follow-up period (3–15 mo). With 18F-FDG PET, increasing SUVcors were seen in 2 patients (patients 7 and 10) at the end of planned chemotherapy, but uptake in these patients gradually decreased to normal values by day 20. These 2 patients are currently being monitored without treatment, as no signs of relapse have yet been detected with CT, tumor markers, or 18F-FDG PET. One patient with a T-cell lymphoma (patient 8) relapsed 3 mo after the end of chemotherapy, but no relationship between SUV dynamics and relapse could be determined with this patient alone. One report has described a relationship between prognosis and the results of 18F-FDG PET after 1 course of chemotherapy for malignant lymphoma (5); the present study may support such findings, as the SUVcor at day 20 was decreased to the same value as that seen at the end of chemotherapy, with no significant difference being found between the values. Further studies are necessary to determine the utility of early 18F-FDG PET for predicting late relapse and assisting in chemotherapeutic planning.
CONCLUSION
We performed 18F-FDG PET in patients with malignant lymphomas before treatment as a baseline and at day 1, day 20, and the end of chemotherapy. 18F-FDG uptake decreased as early as day 1 after the initiation of chemotherapy, indicating that 18F-FDG PET for initial diagnosis or staging must be performed before the onset of chemotherapy, as scan results might already be severely compromised after the first day. Although no relationship between prognosis and rate of decrease in 18F-FDG uptake could be identified at day 1, given the limited population and follow-up period, further studies are needed to confirm the early effects of chemotherapy on malignant lymphomas.
Footnotes
Received Feb. 26, 2004; revision accepted May 21, 2004.
For correspondence or reprints contact: Tomohiko Yamane, MD, Daiyukai General Hospital, 1-9-9, Sakura, Ichinomiya, Aichi 491-8551, Japan.
E-mail: yamane{at}mail.ne.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Systematic Comparison of 18F-C-SNAT to Established Radiotracer Imaging Agents for the Detection of Tumor Response to Treatment
- Early 18F-FDG PET for Prediction of Prognosis in Patients with Diffuse Large B-Cell Lymphoma: SUV-Based Assessment Versus Visual Analysis
- Vascular Inflammation Evaluated by [18F]-Fluorodeoxyglucose Positron Emission Tomography Is Associated With the Metabolic Syndrome
- Monitoring Cancer Treatment with PET/CT: Does It Make a Difference?
- PET for response assessment in oncology: radiotherapy and chemotherapy
- Use of PET for Monitoring Cancer Therapy and for Predicting Outcome