


Abstract
90Y radioembolization (selective internal radiation therapy [SIRT]) is a valuable therapeutic option for unresectable hepatic metastases arising from primary colorectal cancer. The present study evaluated the prognostic value of 18F-FDG PET/CT metabolic parameters for predicting survival after SIRT. Methods: Eighty patients with hepatic metastases of colorectal cancer were treated with SIRT. 18F-FDG PET/CT was performed at baseline and 3 mo after the treatment. Metabolic volume, total lesion glycolysis, and maximum and peak standardized uptake value (SUVmax and SUVpeak, respectively) according to PET Response Criteria in Solid Tumors (PERCIST 1.0) were obtained from 3 liver lesions in each patient, and the corresponding percentage changes from baseline to follow-up were calculated. Tumor response was defined as more than a 30% decrease in these parameters. Furthermore, response was evaluated in accordance with Response Evaluation Criteria in Solid Tumors (RECIST 1.1). Toxicity events and survival were recorded. Results: Overall median survival after SIRT was 60 wk. Responders who had a change in metabolic volume or total lesion glycolysis had significantly longer survival (92 vs. 49 wk [P = 0.006] and 91 vs. 48 wk [P = 0.025], respectively). However, neither RECIST 1.1 criteria nor changes in SUVpeak or SUVmax after treatment predicted outcome (P = 0.086 for RECIST; P = 0.310 for change in SUVpeak; P = 0.155 for change in SUVmax). Conclusion: Changes in metabolic volume and total lesion glycolytic rate as measured by 18F-FDG PET predicted survival in patients with hepatic metastases from colorectal cancer, whereas changes in SUVpeak or SUVmax and RECIST 1.1 criteria did not predict survival.
Colorectal cancer (CRC) is the third most common malignancy among women and the fourth most common malignancy among men worldwide, with two thirds of cases in developed countries (1). The most common site of distal metastasis arising from CRC is the liver, which is already noted in about 25% of cases at initial presentation (2). Despite major advances in systemic treatment of metastatic disease, the overall 5-y patient survival in the United States has remained lamentably low, below 10% (3). In response to this, several liver-focused treatment strategies have been developed aimed at controlling local metastatic growth. Among these treatments, radioembolization using 90Y microspheres, also known as selective internal radiation therapy (SIRT), has emerged as a palliative treatment option for hepatic metastases of CRC (4). Clinical trials with or without concomitant chemotherapy have shown that SIRT can reduce the mass of hepatic metastases sufficiently to permit their surgical resection (5). Median survival after SIRT is about 65 wk, and disease control rates in the range of 35%–88% have been reported, depending on the criteria for response assessment (4,6,7). Whereas changes in tumor mass can be assessed with morphologic MR imaging or CT, metabolic response can be measured with PET with the glucose analog of 18F-FDG. In patients with a variety of tumor types, 18F-FDG PET has proven superior to morphologic imaging for monitoring therapy response and predicting survival (8–12). Initial studies of patients with intrahepatic cholangiocellular carcinoma or hepatic metastasis of breast cancer have indicated a high prognostic value of 18F-FDG PET in the prediction of survival after SIRT (13–14).
To evaluate the prognostic value of metabolic parameters, most 18F-FDG PET studies have endeavored to correlate tracer uptake in the tumor with CT or MR imaging volumes, with duration of posttreatment survival being the standard endpoint (6,7,15–19). However, there is yet no standardized approach for response stratification by means of metabolic imaging, although the maximum 18F-FDG standardized uptake value within the tumor (SUVmax) is traditionally taken as an indicator of tumor vitality. More recently, PET Response Criteria in Solid Tumors (PERCIST 1.0) led to the adoption of a new metric, SUVpeak, defined as the mean 18F-FDG uptake within a spheric 1-cm3 region around the tumor voxel with the highest SUV, which is intended to provide a more reproducible parameter of maximum lesional uptake (20). Other authors have proposed a visual response index or changes in total lesion glycolysis as indices of metabolic response to therapy (21). However, the prognostic capabilities of these different SUV-based parameters for therapy monitoring after regional therapies such as SIRT have not hitherto been compared.
The aims of the present study were to evaluate the prognostic value of several 18F-FDG PET response parameters in predicting the survival of CRC patients on SIRT for hepatic metastases, and to compare the prognostic accuracy of these metabolic indicators relative to changes in CT-based tumor size. Here, overall duration of patient survival was our standard endpoint for assessing therapy response. We hypothesize that a significant decrease of 18F-FDG uptake in hepatic metastases after SIRT would be associated with longer survival, and that metabolic imaging would prove superior to morphologic imaging for predicting patient survival.
MATERIALS AND METHODS
Patients
Eighty consecutive patients with CRC treated with 90Y microspheres (SIR-Spheres; SIRTEX Medical) between October 2003 and January 2010, for whom baseline and follow-up 18F-FDG PET/CT scans were available, were included. A flow diagram for selection of the study cohort is shown in Supplemental Figure 1. As published previously (14), the inclusion criteria were age greater than 18 y; confirmed hepatic metastases from CRC; unresectable, progressive tumor refractory to chemotherapy; preserved liver function as defined by a serum bilirubin level of no more than 2.0 mg/dL; a Karnofsky index score of at least 60 (performance status of functional impairment); pre-SIRT life expectancy of at least 3 mo; and fitness to undergo angiography. Patients with limited extrahepatic metastases were not excluded if the hepatic metastases were deemed to be the predominant and presumably life-limiting aspect of the disease. Exclusion criteria were a bilirubin level greater than 2.0 mg/dL or the presence of ascites; evidence of any uncorrectable arterial blood flow to the gastrointestinal tract observed at angiography or macroaggregated albumin scintigraphy; a pulmonary shunt exceeding 20%, as estimated with macroaggregated albumin scintigraphy; or complete portal venous occlusion (22). The study protocol was approved by the local ethics committee. Written informed consent was obtained from all patients. The minimum follow-up time was 3 mo, and the observation period for overall patient survival ended on July 1, 2012. Patient characteristics are presented in Table 1.
Characteristics of Study Cohort at Baseline (n = 80)
Imaging and Pretherapeutic Examinations
Imaging with whole-body 18F-FDG PET/CT was performed in 3-dimensional mode (3 min/bed position) in a single session on the same system using a Gemini scanner (n = 97; Philips) or a Biograph 64 TruePoint scanner (n = 63; Siemens Medical Solutions). Emission scans were initiated 60 min after intravenous administration of 20 mg of furosemide, 20 mg of butylscopolamine, and 300 MBq of 18F-FDG in rapid sequence. Diagnostic CT scans of the head, thorax, abdomen, and pelvis (100–190 mAs, depending on the scanned organ region; 120 kV; collimation, 2 × 5 mm; pitch, 1.5) were acquired after intravenous injection of 120 mL of iodine-containing contrast agent (Ultravist 300, 2.5 mL/s; Schering). Initiation of CT was delayed 50 s after contrast injection in order to depict the portal venous phase of the liver. CT scans were also used for PET attenuation correction. Seven patients had their baseline and follow-up examinations in different PET instruments. Based on phantom studies conducted with the 2 instruments used, we calculated SUV conversion factors for each scanner, allowing valid pooling of the results (14).
Before angiography, patients had contrast-enhanced MR imaging of the liver, and relevant laboratory tests (liver function, coagulation profiles, metabolic panel, blood count, and tumor markers carcinoembryonic antigen and cancer antigen 19-9) were obtained. All patients underwent angiography with visceral catheterization to evaluate vascular anatomy and identify any aberrant vessels. Prophylactic embolization of the gastroduodenal, right gastric, and other extrahepatic arteries was performed before SIRT, if deemed necessary (23). Scintigraphy was performed after the application of 100 MBq of 99mTc-macroaggregated albumin (GE Healthcare) to the hepatic artery, for calculating the shunt fraction of labeled microspheres to the lung (23). In addition, baseline MR imaging and PET/CT images were evaluated for the percentage of tumor involvement of the liver, the presence of extrahepatic metastases, and portal venous occlusion.
90Y Device and Radioembolization
SIR-Spheres are nonbiodegradable resin microspheres containing 90Y, a β-emitting radionuclide with a 64.2-h half-life. In one patient, the right and left liver lobes were treated sequentially because of challenging vessel anatomy. All other patients received SIRT treatment of both lobes within a single session. SIR-Spheres were applied directly into the right or left hepatic artery. The applied activity of SIR-Spheres was calculated from the percentage involvement of the liver (tumor volume/liver volume × 100) and the body surface area as
Assessment of Response
Serum levels of liver transaminases (alanine transaminase [ALT] and aspartate transaminase) and bilirubin were obtained before and 3 mo after SIRT treatment. The National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0, were used to assess liver toxicity based on the presence of ascites and serum levels of bilirubin and ALT before and after treatment (24). The follow-up protocol additionally included physical examination and 18F-FDG PET/CT 3 mo after SIRT.
For calculation of CT-based local response, the target lesions in the liver were defined as 2 lesions with the largest diameter. The appearance of new lesions after treatment was noted. Tumor response was assessed on the CT scans using Response Evaluation Criteria in Solid Tumors (RECIST 1.1), that is, partial response, stable disease, any response (partial response or stable disease), or progressive disease (25).
For PET-based response assessment, hepatic target lesions were the 3 tumor lesions with the highest 18F-FDG uptake at baseline, in accordance with PERCIST 1.0 (20). Metabolic volume was determined using a semiautomatic algorithm implemented in a 3-dimensional volume-rendering tool (Hybrid Viewer 3D for research; Hermes Medical Solutions). Here, the image display intensity was normalized for blood-pool activity in the aortic arch, and the volume of interest was automatically segmented by the contour of an SUV cutoff accurately delimiting pathologic lesion uptake from normal uptake of surrounding liver tissue. Volume delineations were performed by 2 observers with extensive PET/CT experience. Within each volume of interest, the 18F-FDG parameters SUVmax, mean SUV, and SUVpeak were recorded according to PERCIST 1.0 (in our study with adjustment for body weight) (20). Total lesion glycolysis was calculated as
For response assessment, we summed the metabolic volume, total lesion glycolysis, SUVpeak, and SUVmax of the target liver lesions and calculated the percentage change in the follow-up scan relative to baseline measurements. Any decrease exceeding 30% of the summed baseline parameter was taken to indicate a therapy response (responder), whereas any lesser decrease or an increase was considered as nonresponse (nonresponder).
Survival Analysis
All statistical analyses of survival data were calculated using the SPSS software package (version 15.0, SPSS Inc.). Data were analyzed retrospectively. Kaplan–Meier analysis of survival was based on the interval between the date of SIRT and the last date of contact as censored observation or disease-related death as the event of interest. A log-rank test was used for statistical comparison of survival rates between independent subgroups. Univariate survival analysis was conducted by Cox proportional hazards regression, and corresponding hazard ratio estimates are reported. A statistically significant difference was defined as a P value of less than 0.05. Quantitative survival data are given as median and 95% confidence interval, in weeks.
RESULTS
Patients
Twenty-two women and 58 men (median age, 60.9 ± 15.9 y) were included in the study (Table 1). The median interval between initial diagnosis and SIRT was 118 ± 87 wk. Hepatic tumor burden was more than 25% in 23 of 80 patients. Twenty-nine patients presented with extrahepatic metastases, mostly located in lymph nodes or the lungs. Most patients had undergone multiple chemotherapies before SIRT. Twenty-seven of 80 patients had liver surgery (hemihepatectomy or partial liver resection), and 18 patients had prior local treatment, including external radiotherapy (n = 7), radiofrequency ablation (n = 6), transcatheter arterial chemoembolization (n = 3), laser-induced thermotherapy (n = 3), high-frequency thermotherapy (n = 1), and SIRT (n = 1). Three patients had received more than one local treatment before admission.
Toxicity
Patients were treated with a median activity of 1.8 ± 0.5 GBq of 90Y microspheres. Three months after SIRT, increased liver toxicity was found for 33 patients according to serum bilirubin level and 28 patients according to serum ALT activity. Fourteen patients had both increased bilirubin and ALT toxicities. In 19 patients, toxicity grades increased by 2 or 3 on the basis of bilirubin level, ALT level, or ascites 3 mo after SIRT (Table 2). Eight patients had a serum bilirubin level above 3.0 mg/dL 3 mo after SIRT. In 1 patient, bilirubin level increased to 22.2 mg/dL, and the size of hepatic metastases rapidly progressed during follow-up. This patient died 23 wk after SIRT. In 1 patient, the bilirubin stabilized at 2.8 mg/dL, though the size of hepatic metastasis showed progression to follow-up. This patient died at 48 wk after SIRT. No further bilirubin levels were obtained from the other 6 patients in our clinic. Their survivals after SIRT were 19, 20, 21, 26, 33, and 39 wk. No change in liver toxicity was seen in 39 patients according to bilirubin and 47 according to serum ALT level, and improved toxicity was seen in 8 patients according to bilirubin and 5 according to ALT.
Changes in CTCAE Grades 3 Months After SIRT (n = 80)
There was 1 death within 12 wk after SIRT; this patient died shortly after follow-up examination, most likely because of rapid progression of the disease. The patient had undergone multiple chemotherapies, hemicolectomy, and splenectomy before SIRT and presented with lymph node metastasis and a 25%–50% metastatic tumor burden in the liver. Pretherapeutic cancer antigen 19-9 (58,876 U/mL) and carcinoembryonic antigen (3,662 ng/mL) were both markedly elevated.
Response and Survival
Survival data were available for 78 of 80 patients. Two patients were lost to follow-up, and their last documented contact was taken as censored survival. Four patients were still alive at the end of the observation period. Response assessment with CT and 18F-FDG PET was available for all 80 patients. Overall median survival after SIRT was 60 wk (Table 3; Fig. 1A). Median survival after the initial diagnosis of CRC was 195 wk. According to RECIST 1.1 criteria, 40 patients (50%) had any response (partial response or stable disease), whereas 40 (50%) showed progression (5 with increased lesion diameter, 22 with new lesions, and 13 with both). Response as assessed by RECIST 1.1 showed no significant correlation with overall survival according to the log-rank test (P = 0.086, Fig. 1B).
Kaplan–Meier Survival and Univariate Cox Regression Analysis

Kaplan–Meier curves for overall survival, RECIST, and change in metabolic volume and total lesion glycolysis. (A) Kaplan–Meier survival curve and median survival of CRC study cohort after SIRT. Four patients were alive at end of observation period. Last date of contact was taken as censored survival for 2 patients. (B) Kaplan–Meier survival curves of patients with any response (stable disease or partial response; green line) and progressive disease (blue line) as determined by RECIST 1.1 criteria. Difference was not significant according to log rank test (P = 0.086). (C and D) Kaplan–Meier survival curves as function of change in metabolic volume and total lesion glycolysis. Responders (green line) showed significantly longer survival than nonresponders (blue line; change in metabolic volume: P = 0.006; change in total lesion glycolysis: P = 0.025). *P < 0.05. AR = any response; MetVol = metabolic volume; n.s. = not significant; PD = progressive disease; PR = partial response; SD = stable disease.
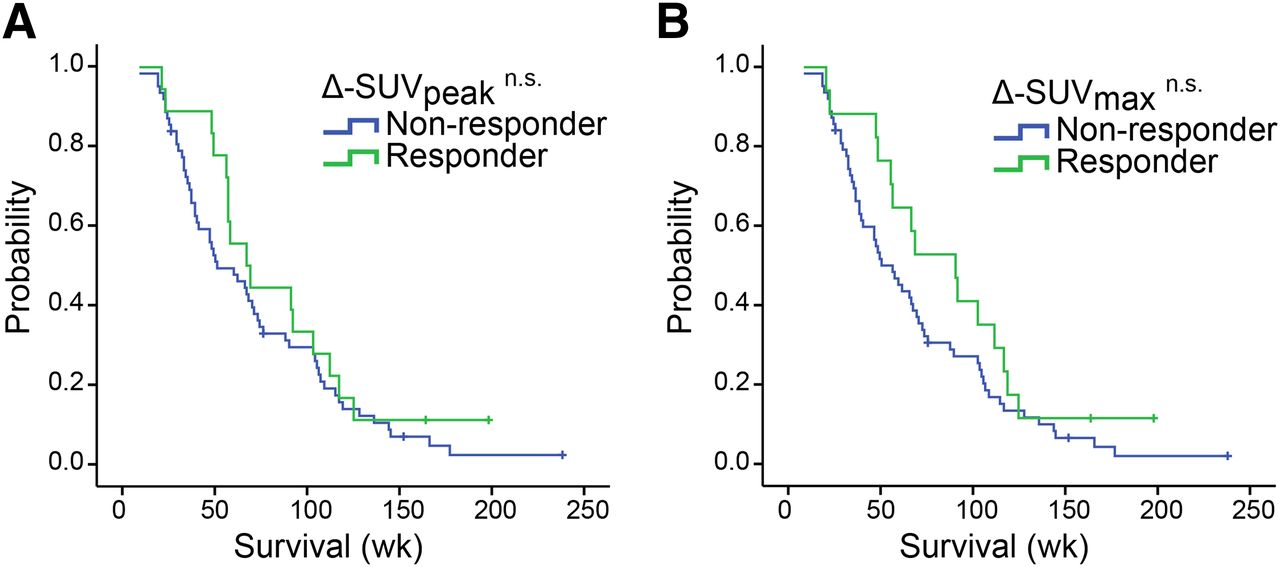
According to PET findings, there were 27 responders (34%) by change in metabolic volume, 30 (38%) by change in total lesion glycolysis, 18 (23%) by change in SUVpeak, and 17 (21%) by change in SUVmax. A change in metabolic volume correlated significantly with overall survival after SIRT, for which median survival of responders was 92 wk versus 49 wk for nonresponders (P = 0.006), as did a change in total lesion glycolysis, for which median survival of responders was 91 wk versus 48 wk for nonresponders (P = 0.025) (Table 3; Figs. 1C and 1D). Neither change in SUVpeak (P = 0.310) nor change in SUVmax (P = 0.155) responses showed any significant association with overall patient survival (Table 3; Figs. 2A and 2B). Furthermore, we found no significant difference in survival by testing a 20% or 10% reduction in SUVpeak or SUVmax as alternate cut-offs for response (20% change in SUVpeak: P = 0.452; 10% change in SUVpeak: P = 0.808; 20% change in SUVmax: P = 0.331; 10% change in SUVmax: P = 0.881).

Kaplan–Meier survival curves for change in SUVpeak and SUVmax. (A and B) Kaplan–Meier survival curves as functions of change in SUVpeak and SUVmax. Difference was not significant according to log rank test (change in SUVpeak: P = 0.310; change in SUVmax: P = 0.155). n.s. = not significant.
In 15 patients, changes in metabolic volume or total lesion glycolysis indicated therapy response (1 case of metabolic volume only, 1 case of total lesion glycolysis only, 13 cases of both) whereas SUVpeak and SUVmax did not. Median survival of these patients was 104 wk (95% confidence interval, 54–154 wk). Median survival of patients with any PET response was 73 wk (49–97 wk) (n = 35), and that of patients with no response by PET criteria was 41 wk (28–54 wk) (n = 45), giving an overall median survival of 60 wk (45–75 wk) for the entire group. In 27 patients, changes in metabolic volume and total lesion glycolysis indicated therapy response. Seven of these patients had progression, and 20 had any response according to RECIST. Median survival of patients with response according to metabolic volume and total lesion glycolysis plus progressive disease according to RECIST was 69 wk (46–92 wk) versus 73 wk (20–126 wk) for patients plus any response according to RECIST. Survival did not significantly differ between these 2 groups, according to the log-rank test (P = 0.978).
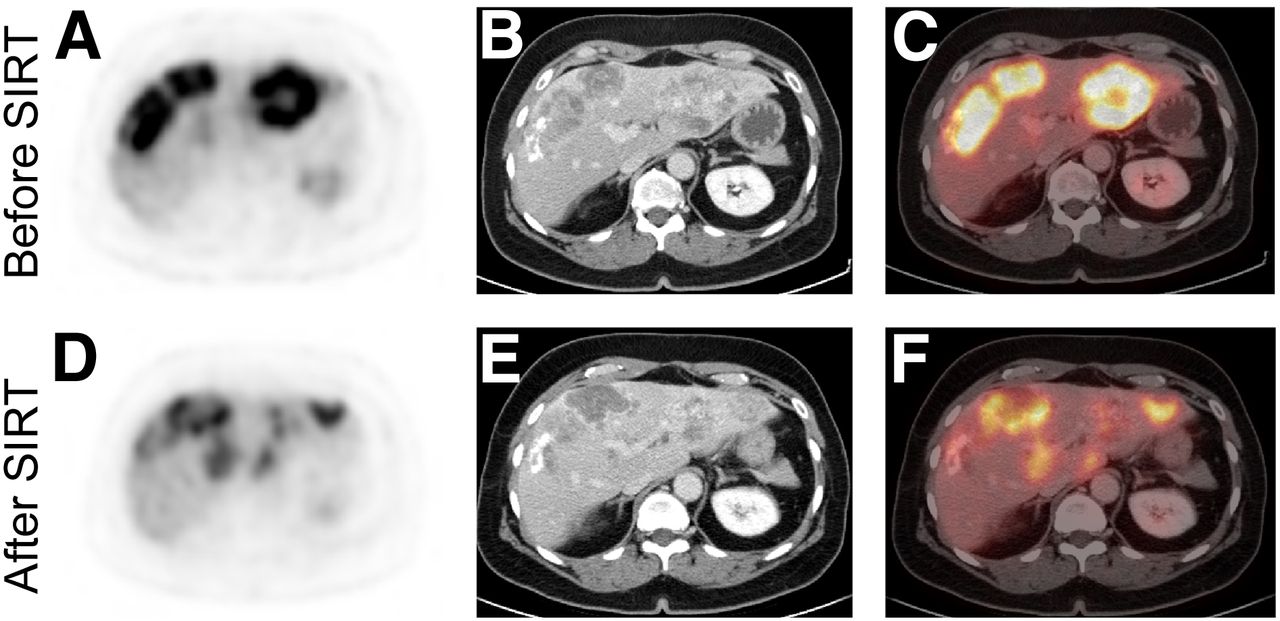
Representative images of PET/CT findings before and after SIRT are shown in Figure 3. Corresponding hazard ratio estimates and univariate Cox regression analysis of responder versus nonresponder for RECIST criteria and PET parameters are presented in Table 3.
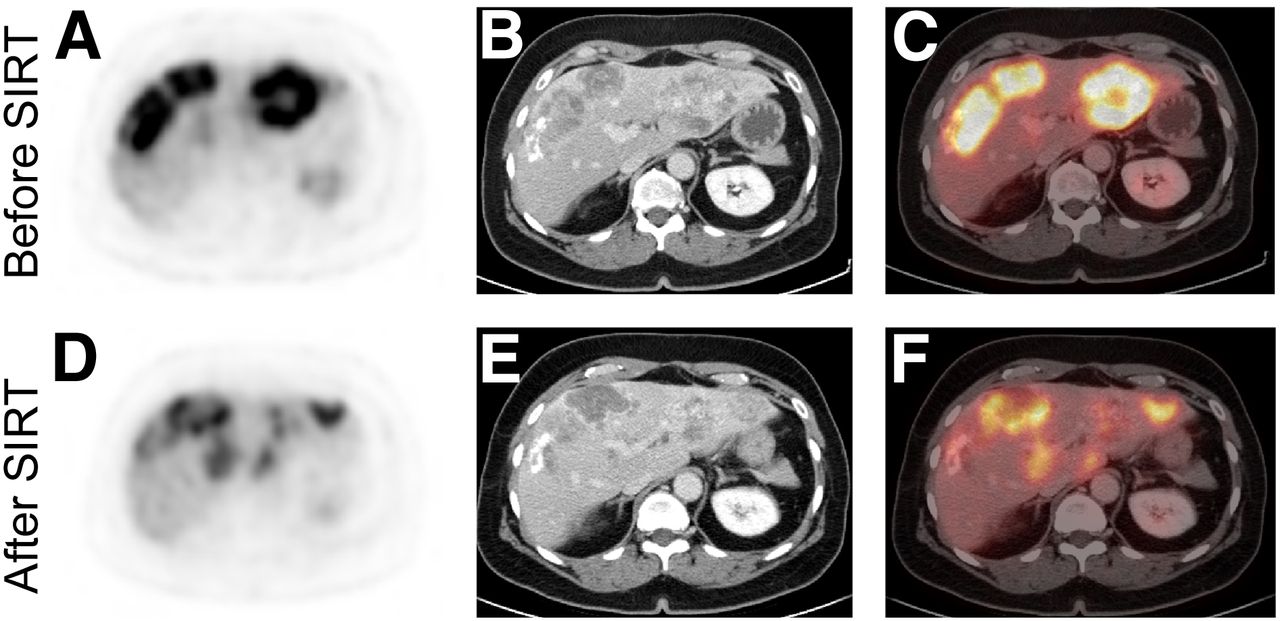
PET/CT before and after SIRT of hepatic metastasis in 63-y-old woman. Representative images of tumor lesions with highest 18F-FDG uptake at baseline are shown. (A and D) 18F-FDG PET images. After SIRT, metabolic volume and total lesion glycolysis decreased by more than 30% (Responder). Small lesion foci with high 18F-FDG uptake remain after treatment, and limited changes of SUVpeak and SUVmax (each < 30%, nonresponder) were noted after SIRT. This patient survived 104 wk after SIRT, at median 60-wk survival of study cohort. (B and E) Corresponding CT images. (C and F) Corresponding PET/CT images. Patient had stable disease according to RECIST 1.1.
DISCUSSION
The aim of this study was to evaluate the prognostic values of several metabolic parameters based on 18F-FDG PET and RECIST 1.1 criteria as predictors of duration of patient survival after SIRT of hepatic metastasis from CRC. The median survival of our entire patient population (60 wk) falls within the survival range of 6.7 to 17.0 mo reported in a review of previously published studies (26). Several 18F-FDG PET studies have reported a prognostic value of metabolic imaging in small patient cohorts, albeit without reporting overall patient survival as an indicator for treatment response (6,7,15). Zerizer et al. published an initial report on the correlation between 2-y progression-free survival and 18F-FDG PET metabolic response as determined by European Organization for Research and Treatment of Cancer (EORTC) criteria in 25 CRC patients (27). In their study, a posttherapeutic change in SUVmax of 2.0 or less in the lesion with the highest 18F-FDG uptake was a strong predictor of progression-free survival, whereas RECIST 1.1 criteria and tumor density criteria, based on those of Choi et al. (28), did not emerge as useful prognostic markers. Overall, the prognostic value of RECIST criteria after SIRT of hepatic metastasis remains a matter of some controversy in the literature. Several trials have shown only small changes in largest tumor diameter after SIRT (18), whereas other studies with concurrent SIRT and chemotherapy have reported disease control rates as high as 90% based on CT findings (29,30). In our study, a response according to RECIST criteria, either partial response or stable disease, was seen in 40 of 80 patients, indicating a disease control rate of 50%. This rate falls somewhat below the range of previously published disease control rates of 56%–60% in 2 prospective and 1 retrospective SIRT trial in a total of 74 patients (31–33). Since, in our hands, SIRT was performed in a salvage situation, the slightly lower response may arise from a more advanced course of disease. The overall median survival of 76 wk among our responders by RECIST criteria exceeded the 47-wk survival of patients with progressive disease. However, this difference was not statistically significant according to the log rank test (Table 3). Our finding underscores the well-known controversy regarding the prognostic value of morphologic response parameters in the case of hepatic CRC metastasis.
Based on EORTC criteria, the standardized 18F-FDG uptake value of the hottest voxel in the lesion (SUVmax) has traditionally been chosen as a hallmark of tumor vitality for determining metabolic response to treatment (34). Considering the existing EORTC criteria, International Workshop criteria, World Health Organization criteria, and RECIST, a consensus group has proposed a new criterion, known as PERCIST 1.0, as a basic framework for clinical trials (20). Here, the SUVpeak, that is, the mean SUV of a 1-cm3 volume of interest located around the hottest voxel, imparting to this volume of interest the highest possible mean uptake, was adopted as a new standard metric, giving optimal tumor-to-background ratio and reproducibility (35). The consensus group defined a reduction in SUVpeak of 30% or more in relative terms, and 0.8 SUV units in absolute terms, as indicating a metabolic response. In a previous study on soft-tissue sarcomas, changes in SUVpeak by these criteria significantly correlated with patient survival (36). In our study the mean SUVpeak of the 3 liver lesions with the highest 18F-FDG uptake at baseline decreased after SIRT from 10.2 to 9.2 and the mean SUVmax decreased from 12.6 to 11.6. However, duration of survival was not significantly different for responder and nonresponder groups, as determined by the log-rank test. This was not due to the criterion’s rather high cutoff value of a 30% decrease, since we likewise found no significant differences in survival by group with 20% or 10% reductions in SUVpeak or SUVmax.
Choosing functional lesion parameters such as metabolic volume or total lesion glycolysis might be expected to overcome the evident limitations of SUVpeak and SUVmax as prognostic indicators. Indeed, Gulec et al. showed in a phase II clinical trial of SIRT in patients with multiple hepatic metastases from CRC that absolute metabolic volume and total lesion glycolysis before and after treatment were predictive of overall patient survival, without, however, including percentage change of these parameters into survival analysis and without comparing these parameters to SUVpeak or SUVmax (37). In our study comparing RECIST 1.1 criteria and posttherapy changes of 4 SUV-based PET parameters for the prediction of overall survival of 80 CRC patients after SIRT, changes in total lesion glycolysis and metabolic volume after SIRT treatment were predictive of patient survival. Patients referred for radioembolization are usually at late stage, show extensive liver involvement (29% of our group had >25% involvement), and have already undergone a range of local and systemic regimes. These pretreatments may have resulted in necrosis and inhomogeneity of intrahepatic metastases preceding SIRT, at the time of baseline 18F-FDG PET. In addition, the radiation dose from SIRT is inhomogeneously distributed to hepatic lesions (38). In contrast to parameters defined by a single voxel (SUVmax), attributes of the whole lesion, such as lesion volume or mean uptake, seem less susceptible to variable treatment effects that might leave residual vital tumor foci within a generally well-treated hepatic metastasis (Fig. 3). Our findings are in accordance with those of Gulec et al., who similarly provided evidence for a correlation between metabolic volume or total lesion glycolysis and survival duration in 20 CRC patients with multiple hepatic metastases (37). In contrast, Zerizer et al. found an absolute decrease in SUVmax to have a predictive value, without reporting corresponding changes in total lesion glycolysis or metabolic volume (27). This difference may reflect their smaller cohort size (25 vs. 80 patients), their briefer follow-up protocol (early follow-up at 6–8 wk vs. 12 wk), or differing criteria for defining response (absolute decline in SUVmax vs. PERCIST criteria) and for the study endpoint (progression-free survival vs. overall survival).
The present study had several limitations. A rather small patient cohort was analyzed because SIRT was performed in a palliative setting and patients were preselected by a set of inclusion criteria. Data analysis was performed retrospectively. Patients received no further cancer-directed therapy until follow-up at 3 mo. However, we did not analyze the effect of treatments after this period that might potentially have influenced survival in the late-line setting. Finally, 2 patients were lost to follow-up. and their last date of contact was taken as censored survival. The random loss of the 2 subjects should not have created a significant follow-up bias.
CONCLUSION
Monitoring metabolic changes in a larger proportion of the intrahepatic metastatic burden with functional imaging emerges as a valuable tool to predict duration of survival after SIRT in patients with advanced CRC.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Alexander Haug, Philipp Paprottka, Tobias Jakobs, and Peter Bartenstein have received fees or travel-related expenses for oral presentations at events organized by SIRTEX Medical (Sydney, Australia). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Andreas Elsner for customizing the Hybrid Viewer 3D and for continuous technical support.
Footnotes
Published online May 31, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 26, 2012.
- Accepted for publication February 24, 2013.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transarterial Radioembolization in the TACOME Trial: Dosimetric Analysis and Clinical Features in Predicting Response and Overall Survival
- Additional Local Therapy for Liver Metastases in Patients with Metastatic Castration-Resistant Prostate Cancer Receiving Systemic PSMA-Targeted Therapy
- 18F-FDG PET/CT in Local Ablative Therapies: A Systematic Review
- SIRFLOX: Progression-Free Survival in the Liver As a Surrogate End Point for Survival?
- Safety, Efficacy, and Prognostic Factors After Radioembolization of Hepatic Metastases from Breast Cancer: A Large Single-Center Experience in 81 Patients
- Use of PERCIST for Prediction of Progression-Free and Overall Survival After Radioembolization for Liver Metastases from Pancreatic Cancer
- Prognostic Value of Metabolic Tumor Volume and Total Lesion Glycolysis on Preoperative 18F-FDG PET/CT in Patients with Pancreatic Cancer