


Abstract
Malignant lymphomas are a heterogeneous group of diseases whose treatment and prognosis depend on accurate staging and evaluation of histologic features. The conventional imaging procedure is CT; however, nuclear medicine imaging has also had a prominent role. Single-photon imaging with 67Ga-citrate has been widely used for lymphomas. PET with 18F-FDG has gained a role in the staging and follow-up of lymphomas, largely replacing gallium as the nuclear medicine study of choice. 18F-FDG PET has proved useful in the staging and follow-up of Hodgkin's disease and non-Hodgkin's lymphoma (especially more aggressive types), and the widespread use of PET/CT has also increased the sensitivity and specificity. Its usefulness for the staging of slow-growing lymphomas has not been established. After the basics of staging and classification of lymphomas have been outlined, this article will review the role of 18F-FDG PET in the management of patients with lymphoma. PET tracers other than 18F-FDG, such as positron-emitting isotopes of gallium and the cellular proliferation marker 18F-3′-deoxy-3′-fluorothymidine, will be discussed and future directions for PET in lymphoma proposed.
Malignant lymphomas are the fifth most frequently occurring type of cancer in the United States. In 2005, an estimated 7,350 new cases of Hodgkin's disease (HD) and 56,390 new cases of non-Hodgkin's lymphoma (NHL) were diagnosed (1). The NHLs are a heterogeneous group of diseases that vary in prognosis according to histologic and clinical features. We will begin by reviewing the classifications of HDs and NHLs.
HD HISTOLOGIC SUBTYPES
There are 4 histologic subtypes of HD. Currently, the Rye modification of the Lukes and Butler classification is in use throughout the world. Nodular sclerosis is the most common subtype in North America and Western Europe. Typically, a young woman presents with a mediastinal mass, with or without symptoms. Prognosis depends on the stage of the disease, the bulkiness of the tumor masses, and the presence or absence of systemic symptoms. The lymphocyte-predominance subtype is characterized by an abundance of small lymphocytes with occasional, often atypical, Reed-Sternberg cells of the “lymphocytic–histiocytic” (or “popcorn cell”) variety, with vesicular, polylobulated nuclei and small nucleoli. This subtype is associated with a favorable prognosis, although late recurrences have been reported in some series. The mixed-cellularity subtype is characterized by a pleomorphic cellular infiltrate of plasma cells, eosinophils, lymphocytes, histiocytes, and Reed-Sternberg cells. Subdiaphragmatic and extranodal presentations and the presence of B symptoms may be somewhat more frequent in patients with the mixed-cellularity subtype than in patients with the nodular-sclerosis subtype. The mixed-cellularity subtype is the second most common histologic subtype in North America and Western Europe and is more common in the poorer parts of the world and among indigent populations in the United States. It is also somewhat more common among older patients. It has been associated with a worse prognosis than has nodular sclerosis, but this difference may be due to the association of this subtype with the unfavorable clinical prognostic features. The lymphocyte-depletion subtype has a paucity of cellular elements and an increased reticular network. This subtype is associated with advanced age, systemic symptoms, retroperitoneal lymphadenopathy, and extranodal involvement and today is diagnosed infrequently because modern immunophenotyping and molecular genetic studies have demonstrated that many cases formerly thought to be lymphocyte-depletion HD are actually T-cell NHLs. The lymphocyte-depletion subtype has the worst prognosis of the 4 histologic subtypes.
NHL TUMOR CLASSIFICATION
The classification of NHL is continuing to evolve. In 1994, an international panel of pathologists published a Revised European-American Classification of Lymphoid Tumors (REAL classification) (2). Another international panel of pathologists made minor revisions to the REAL classification under the auspices of the World Health Organization in 1998 (3). This classification recognizes new entities established by improved technologies in immunophenotyping, cytogenetics, and molecular genetics. The Non-Hodgkin's Lymphoma Classification Project has defined the clinical features of the most common NHLs, which are (in order of frequency) diffuse large B-cell lymphoma (31%), follicular lymphoma (22%), small lymphocytic lymphoma (6%), mantle cell lymphoma (6%), peripheral T-cell lymphoma (6%), marginal zone B-cell lymphoma, mucosa-associated lymphoid tumor type (5%), primary mediastinal large B-cell lymphoma (2%), anaplastic large T-cell/null cell lymphoma (2%), lymphoblastic lymphoma (T-cell/B-cell) (2%), Burkitt-like lymphoma (2%), marginal zone nodal-type lymphoma (1%), lymphoplasmacytic lymphoma (1%), and Burkitt's lymphoma (<1%) (4).
The NHLs can be further divided into slow-growing types (marginal zone, small cell/chronic lymphocytic lymphoma, lymphoplasmacytic, follicular), more aggressive types (diffuse large B-cell, mantle cell, peripheral T-cell), and fast-growing types (Burkitt-type, lymphoblastic). Of the slow-growing lymphomas, the small lymphocytic lymphomas are virtually always diffuse. The small cell lymphomas of the chronic lymphocytic leukemia type are clinically and by cell marker analysis part of the same disease spectrum as chronic lymphocytic leukemia but are considered to be lymphomas when the disease is principally in lymph nodes and not peripheral blood and bone marrow. The lymphoplasmacytic variant of small cell lymphoma contains lymphoplasmacytoid and small, well-differentiated lymphocytes. The tumor cells express B-cell surface antigens, have monoclonal IgM on the surface and often within the cytoplasm, but lack CD5 expression. The bone marrow and peripheral blood are frequently involved. The follicular lymphomas usually have a reciprocal translocation between chromosomes 14 and 18 that results in deregulation and continuous expression of the bcl-2 gene on the translocated portion of chromosome 18. This gene normally blocks apoptosis. The resultant increased longevity of the malignant cells may be important in the pathogenesis of the tumors. The marginal zone lymphomas comprise small cells that resemble the small cells in the marginal zone of the spleen. Some marginal zone lymphomas occur in the lymph nodes, and others present primarily in the spleen. Some of the latter are associated with circulating lymphocytes with villous cytoplasmic membranes. The splenic marginal zone lymphomas with predominantly splenic, hepatic, and bone marrow involvement, sometimes with a leukemic phase with villous lymphocytes, have a favorable prognosis and are often diagnosed through splenectomy. The extranodal marginal zone lymphomas of the gastrointestinal tract, lung, salivary glands, conjunctiva, and thyroid gland are currently diagnosed as a separate entity termed mucosa-associated lymphoid tumors.
Of the more aggressive lymphomas, diffuse large B-cell is that most commonly seen in adults. There is usually no distinction between the cleaved and noncleaved types, because they do not seem to differ clinically. Various molecular changes are seen in the diffuse large B-cell lymphomas, and the use of molecular profiling has aided in identifying subgroups with differing survivals (5). The follicular lymphomas and the small cell lymphomas of the chronic lymphocytic leukemia type can transform to a diffuse large cell histology, and this transformation is associated with further chromosomal abnormalities (in addition to t(14;18) of the follicular lymphoma type) and a poor prognosis. Also, approximately 20%−30% of cases of diffuse large B-cell lymphoma have rearranged bcl-2 at diagnosis, reflecting t(14;18), which has also been associated with a poor prognosis. Other, more aggressive types of lymphoma include peripheral T-cell lymphomas, whose prognosis is worse than that of comparable lymphomas with a B-cell phenotype. The angiocentric variety is characterized by destructive angiocentric and angioinvasive lymphomatous infiltrates and classically involves the nose, palate, and skin. The malignant cells in mantle cell lymphomas resemble lymphocytes in the mantle zone adjacent to the lymphoid follicles. The tumor cells have monoclonal surface IgM and often IgD, B-cell antigens, and CD5, but unlike small cell lymphoma of the chronic lymphocytic leukemia type, the malignant cells in mantle cell lymphomas do not express CD23. They have a characteristic reciprocal translocation, t(11;14), in which the bcl-1 locus containing the PRAD-1 or cyclin D1 gene on chromosome 11 is placed near the immune globulin heavy-chain gene on chromosome 14, resulting in deregulation and overproduction of cyclin D1 protein, a cell-cycle protein not usually expressed in lymphoid cells. This disease is usually stage IV at diagnosis, and bone marrow and leukemic presentations are common. A variant of mantle cell lymphoma can present as multiple polyps throughout the gastrointestinal tract (lymphomatous polyposis) (6).
The fast-growing lymphomas include lymphoblastic and Burkitt's lymphoma. Lymphoblastic lymphoma occurs most commonly in young adults and often includes large mediastinal masses and either initial or eventual leukemic involvement and meningeal metastasis. Cell marker studies have shown that this type is closely related to acute lymphoblastic leukemia and is of immature T-cell or, less commonly, pre–B-cell origin. The Burkitt-type lymphomas comprise small, primitive cells with noncleaved nuclei. Often, macrophages that have phagocytized necrotic debris are interspersed between the malignant cells, producing the so-called starry-sky appearance. The latter morphology is typical for cases occurring in Africa, classically in young men with jaw tumors. This is the Burkitt's lymphoma that is associated with latent Epstein–Barr virus infection and reciprocal translocation between chromosomes 8 and 14 or, less commonly, 8 and 22 or 2 and 8. There are large cell lymphomas that also have a growth fraction close to 100%, and these have been termed Burkitt-like lymphomas.
STAGING
The Ann Arbor classification can be applied to both HD and NHL and divides them into 4 stages (7): disease limited to a single lymph node or lymph node group (stage I); disease in 2 or more noncontiguous lymph node groups or spleen on the same side of the diaphragm (stage II); disease in 2 or more lymph node groups or spleen on both sides of the diaphragm (stage III); and disease in extranodal sites, usually lung, liver, bone or bone marrow, and, more rarely, other sites (stage IV).
Extranodal involvement by extension from lymph node disease to such sites as the lung, bone, pleura, or skin may occur in stages I–III and does not increase the disease to stage IV. Such disease is designated by the subscript “E” (i.e., IE, IIE, and IIIE). For each stage, the absence of systemic symptoms is designated by the subscript “A,” whereas the presence of unexplained fevers to 38°C or higher, night sweats, or weight loss of more than 10% over 6 mo is designated by the subscript “B.” In general, the prognosis worsens as the stage increases, and within each stage, the presence of the symptoms designated by the subscript “B” carries a worse prognosis than does the absence of such symptoms. Lymph node disease larger than 10 cm is defined as “bulky” and is designated by the suffix “x” added to the numeric stage (e.g., IxA, IxB, IIxA, IIxB, IIIxA, and IIIxB). Certain nodal sites of involvement are more common in NHL than in HD. Waldeyer's ring is involved in 5%−10% of patients with NHL and is extremely rare in HD. Involvement of Waldeyer's ring is associated with involvement of the gastrointestinal tract, usually the stomach or small bowel. Mesenteric nodal involvement is quite common in NHL but is seen at presentation in HD in fewer than 5% of the patients. Bone marrow involvement may be seen at presentation in from 15% to 40% of patients with NHL.
The International Non-Hodgkin's Lymphoma Prognostic Factors Project developed a predictive model for newly diagnosed patients with intermediate- or high-grade NHL treated with combination chemotherapy (8). Five clinical features at presentation were found to have prognostic importance: age (≤60 y vs. >60 y), serum low-density lipoprotein level (≤1× normal vs. >l× normal), performance status (0 or 1 vs. 2−4), stage (I or II vs. III or IV), and extranodal involvement (≤1 site vs. >1 site).
TREATMENT AND OUTCOME
The choice of treatment depends on accurate staging and accurate evaluation of prognostic factors. Radiation therapy has resulted in cures in patients with localized HD and nonaggressive NHL. Combination chemotherapy has resulted in long-term unmaintained remissions in many patients with more advanced disease, particularly HD and NHL of the diffuse large cell, lymphoblastic, and Burkitt types. Long-term progression-free survival for nonbulky HD, stages I–IIIA, at 5 y has been found to be up to 86% (9), with progression-free survival for stage IV being as high as 66% (10). Response is lower for the diffuse large B-cell type: A complete response to therapy can be seen in 63%−78% of patients (11). Combined chemotherapy and radiation therapy has been most successful for patients with stage I NHL of an intermediate- or high-grade histologic type. The role of combined chemotherapy and radiation therapy in bulky advanced-stage NHL remains to be determined.
Emerging data suggest that the addition of rituximab to combination chemotherapy may further improve the outcome over that seen with chemotherapy alone. This improvement can be demonstrated by the response rates seen in follicular lymphoma, for which the 5-y failure-free survival had been around 29% but reached a level of as high as 60% with the addition of rituximab to combination chemotherapy (12,13). Further work is needed to improve the results for these patients and for patients with other types of NHL. High-dose chemotherapy with or without radiation therapy with autologous bone marrow or peripheral stem cell rescue is an effective salvage treatment for some patients with relapsed or refractory lymphomas, particularly intermediate-grade NHL and HD. Promising results have also been achieved with radiolabeled anti-CD20 antibodies such as 90Y-ibritumomab tiuxetan and 131I-tositumomab for nonmyeloablative treatment of relapsed or refractory low-grade and follicular or transformed NHL (14), as well as in the myeloablative setting (15).
EVALUATION OF CLINICAL STAGE
Conventional staging procedures include obtaining complete blood counts with platelet and differential counts, testing serum liver biochemistries (including alkaline phosphatase), and determining the erythrocyte sedimentation rate. Bone marrow aspiration and biopsy are also key components of initial staging. Some of these laboratory tests have prognostic value.
Nonscintigraphic Imaging Studies
Standard imaging modalities form the basis of the Cheson classification for lymphomas, a widely used measure for evaluating disease and response to treatment (16). These standard modalities include radiography of the chest and CT of the chest, abdomen, and pelvis with oral or intravenous contrast material. CT of the chest is useful in detecting disease—particularly in the retrosternal region—that may be missed on plain chest radiography. Also, some patients with bulky mediastinal and hilar nodal disease will have peripheral lung nodules that can be detected only through chest CT. For the detection of involvement in the brain, spinal cord, and bone marrow, MRI is superior to CT (17).
Scintigraphic Imaging Studies
Nuclear medicine has a well-established role in the management of malignant lymphomas. 67Ga-Citrate has been widely used for the evaluation of HD and NHL. 67Ga is transported to the area of localization mainly by 67Ga-transferrin, and the localization to tumors is due to the presence of transferrin-binding receptors on the tumor cells (18,19). In particular, 67Ga has proven useful for the evaluation of residual masses that are indeterminate for lymphoma versus necrosis (20), demonstrating 76%–100% sensitivity and 75%–96% specificity (21). Physiologic excretion of tracer in the intestines makes the procedure less sensitive and specific for disease below the diaphragm (22). The typical scanning protocol calls for the 67Ga to be injected 2−3 d before the patient is imaged and can thus create an inconvenience for the patient.
CT has been the gold standard for the staging of lymphomas but offers only structural information. CT has excellent resolution; however, disease is frequently assessed on the basis of size criteria. For example, lymph nodes less than 1 cm in diameter are not considered abnormal by most current criteria (23,24). In addition, CT may demonstrate residual masses on follow-up that represent fibrosis rather than active disease.
Although CT and MRI provide high-resolution anatomic information, PET adds information on the metabolic activity of lesions. Standardized uptake values (SUVs) are a measure of the concentration of a radiotracer in a defined region divided by the injected dose normalized for the patient's body weight at a fixed time after tracer injection. This functional information may be particularly useful in determining response to therapy, as suggested by the European Organization for Research (25). These metabolic changes may occur even if anatomic size does not change significantly.
Several positron-emitting radiopharmaceuticals have been investigated for use in the evaluation of lymphomas, but 18F-FDG has established itself as an excellent functional imaging tool for tumors. Its role in lymphoma imaging, in particular, has been well established (26). The utility of 18F-FDG for imaging tumor cells is based on Warburg's observation that the increased metabolic demands of rapidly dividing tumor cells required adenosine triphosphate generated by glycolysis (27). FDG is actively transported into cells and converted into FDG-6-phosphate by hexokinase, the first enzyme in glycolysis. The FDG-6-phosphate, because it is not a substrate for the enzyme responsible for the next step in glycolysis, is then trapped in the cell. Accurate assessment with 18F-FDG PET of the extent and metabolic activity of disease requires that patients fast for 4−6 h before undergoing scanning to keep glucose and insulin levels low. Patients should also avoid strenuous exercise for 24 h before receiving the injection to reduce uptake in skeletal muscle. After receiving the injection, patients should rest for about 60 min to allow the tracer to clear. Repetitive muscular activity during the clearance interval will also increase local uptake of 18F-FDG and may interfere with interpretation of the scan findings. Normal tissues that use glucose, such as the brain, liver, myocardium, skeletal and smooth muscle, and specific sites of brown fat above and below the diaphragm (28,29), often serve as landmarks for scan quantification. The fact that 18F-FDG accumulates at sites of infection or inflammation can be a particular problem in patients who may be immunocompromised after receiving chemotherapy (30).
In contrast to 67Ga, 18F-FDG PET is sensitive for disease below the diaphragm as well, suggesting that 18F-FDG is superior to 67Ga for both initial staging and follow-up (31–33).
PET for Initial Staging.
Many studies have demonstrated the role of 18F-FDG PET in the initial staging of lymphoma. Early studies compared 18F-FDG PET with conventional imaging studies for lymphoma, including CT and 67Ga, and showed accurate staging with PET. One such study of 60 patients, 27 with HD and 33 with NHL, undergoing an initial staging evaluation demonstrated that in 8% of patients, the disease was upstaged on the basis of PET results (34). A retrospective study by Schoder et al. (35) demonstrated that 18F-FDG PET affected the clinical management of 44% of patients; in 21%, the disease was upstaged. Moreover, PET resulted in changes in the treatment of more than 60% of patients. Another prospective study of 88 patients with HD compared the results of staging 18F-FDG PET with the results of conventional staging modalities and found that PET caused a change in the clinical stage of 20% of patients, which translated into a potential change in the management of 18% of the total number of patients (36).
Early studies have also demonstrated the usefulness of 18F-FDG PET in the evaluation of bone marrow involvement in lymphoma. Although the current practice of obtaining bone marrow biopsy samples from the iliac crests may not accurately depict the overall bone marrow involvement, and CT scans often do not demonstrate bone marrow infiltration, studies have shown that 18F-FDG PET is accurate in evaluating the presence of bone marrow disease (37). One prospective study of 78 patients compared bone marrow biopsy results with 18F-FDG PET results, using MRI or samples from additional biopsies to evaluate discordant results. This study demonstrated a sensitivity of 81% and a specificity of 100% for the detection of bone marrow disease, with only 4 cases of bone marrow involvement not being seen on PET. One caveat is that granulocyte colony-stimulating factors and even recombinant erythropoietin, which are integral parts of treatment regimens, can result in diffusely increased 18F-FDG uptake in the bone marrow and spleen, rendering it difficult to evaluate these areas on follow-up scans (Fig. 1) (38–40). This increased uptake because of growth factors generally returns to baseline levels by 1 mo (usually within 3 wk) after discontinuation of the growth factors (40,41), suggesting that clinicians should wait at least 1 mo after completion of therapy before obtaining a PET scan. Marrow hyperplasia as a consequence of recovery from a chemotherapeutic insult may also cause a generalized increase in 18F-FDG uptake in marrow.
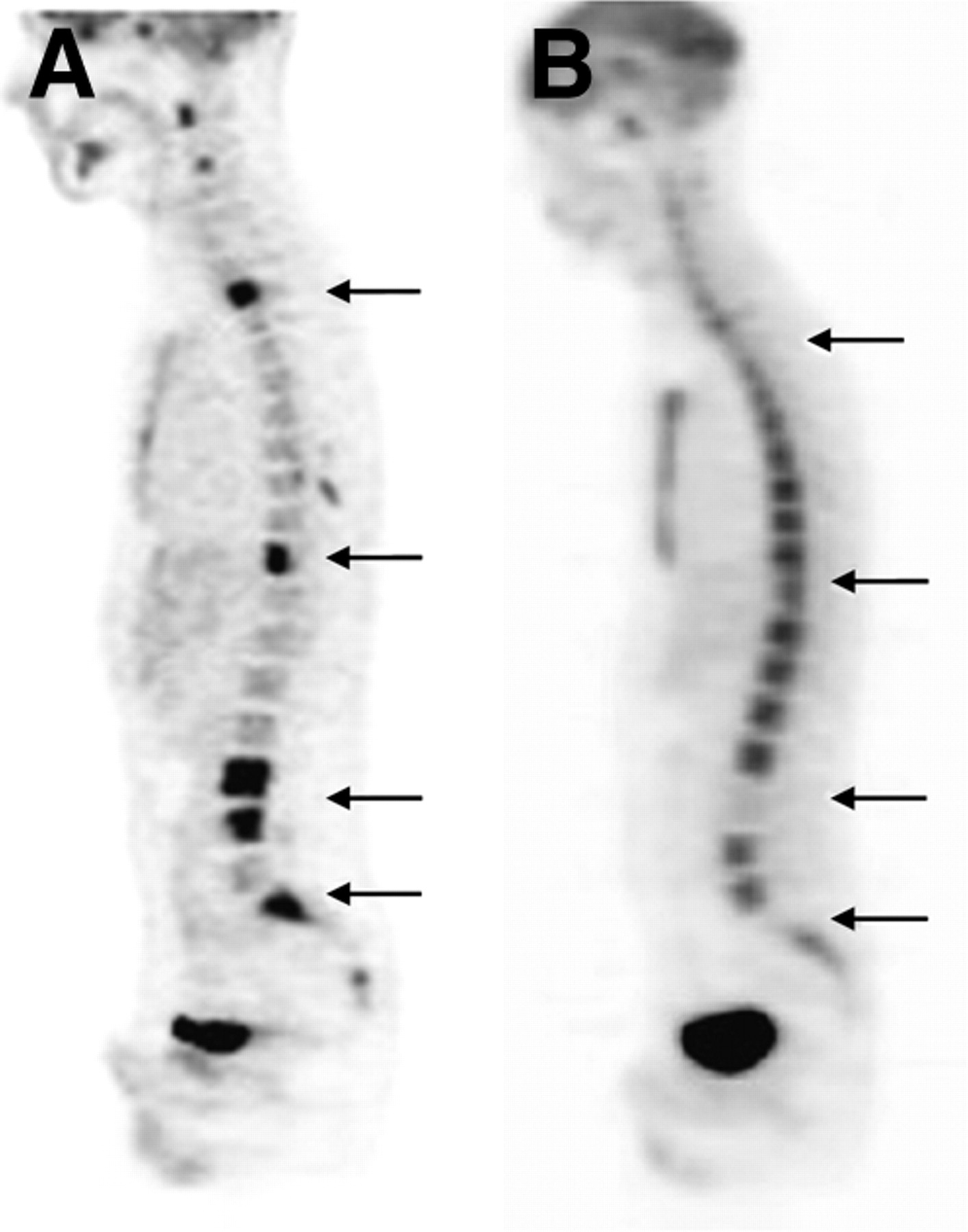
Pretherapy (A) and follow-up posttherapy (B) PET scans of patient with Burkitt's lymphoma involving multiple vertebrae (arrows). Follow-up scan demonstrates diffuse bone marrow uptake secondary to administration of growth factor, with decreased uptake seen in areas of previous bone marrow involvement.
Several studies have examined the ability of PET to differentiate between indolent and aggressive lymphomas (32,42,43). Although most studies have failed to demonstrate that PET can differentiate between tumor grades, a study of 97 patients correlated biopsy findings with the highest SUV in PET scans obtained from untreated patients or patients with relapsed or persistent disease who had not been treated within 6 mo of undergoing PET (44). All indolent lymphomas had an SUV of less than 13. Twenty-two (35%) of the 63 patients with aggressive disease, however, also had tumors with an SUV of less than 13. Although there exists an overlap between the SUVs of indolent and aggressive lymphomas, the study concluded that aggressive disease had a higher 18F-FDG uptake than did indolent lymphomas (P < 0.01) and the authors suggested that an SUV of more than 10 confers a higher likelihood for aggressive disease.
Indolent lymphomas are sometimes treated with a wait-and-watch attitude unless CT shows significant evidence of disease progression. Several groups are extending this observation to 18F-FDG PET and considering treatment if the 18F-FDG PET findings demonstrate a significantly increased uptake in lesions over time, even if lesion size does not change. Unfortunately, studies have not been able to demonstrate reliable sensitivity for PET in predicting the likelihood of response in patients with indolent lymphomas, even between different histologically indolent subtypes (45,46). In a study comparing CT and 18F-FDG PET in 42 patients, 18F-FDG PET detected 40% more follicular lymphomas and 58% fewer small lymphocytic lymphomas than did CT. This study also showed that 18F-FDG PET was less useful for detecting abdominal and pelvic nodes (26% fewer areas detected) in indolent lymphomas than in detecting peripheral and thoracic lymph nodes (47).
PET for Evaluation of Treatment Response and as a Prognostic Indicator.
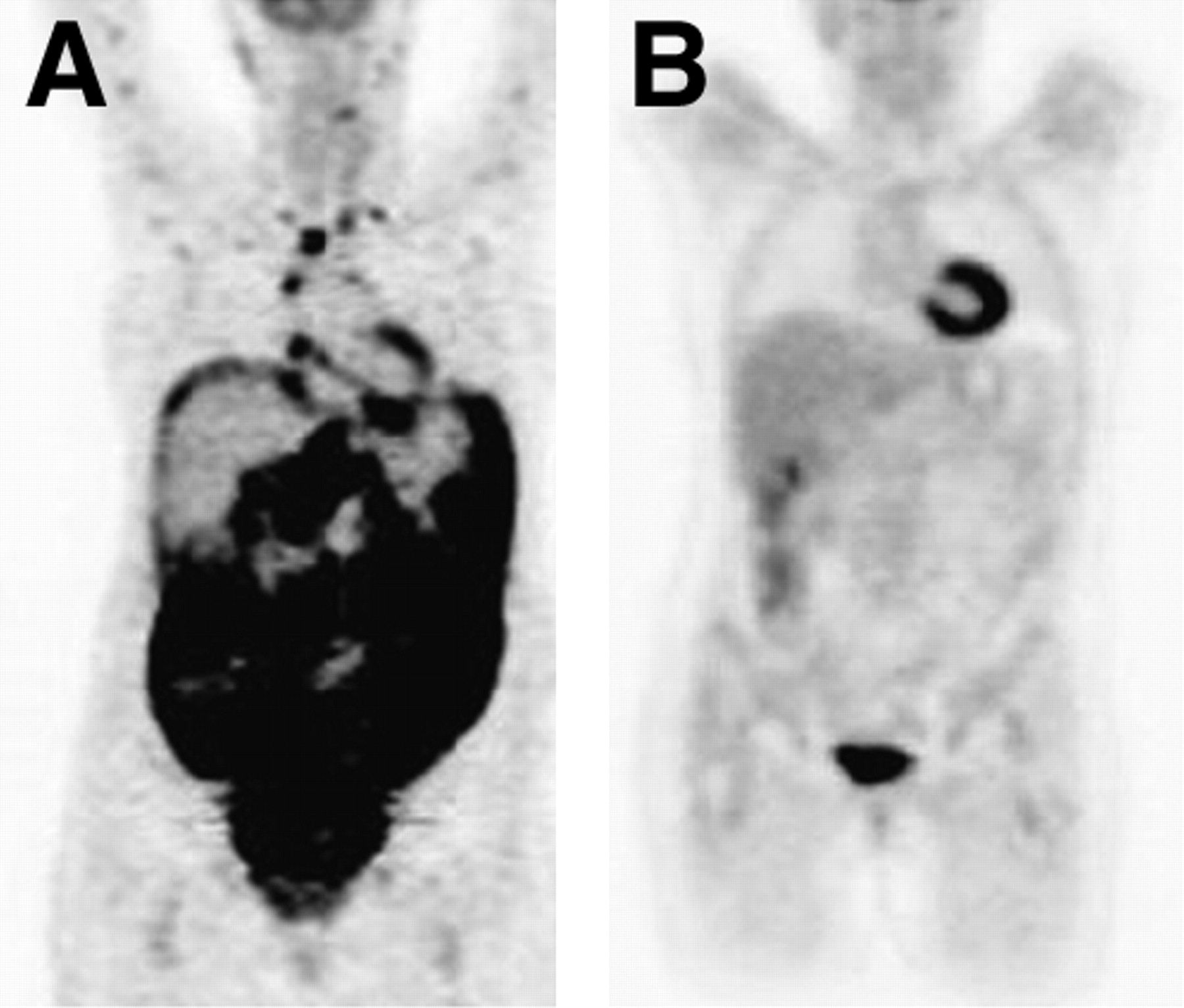
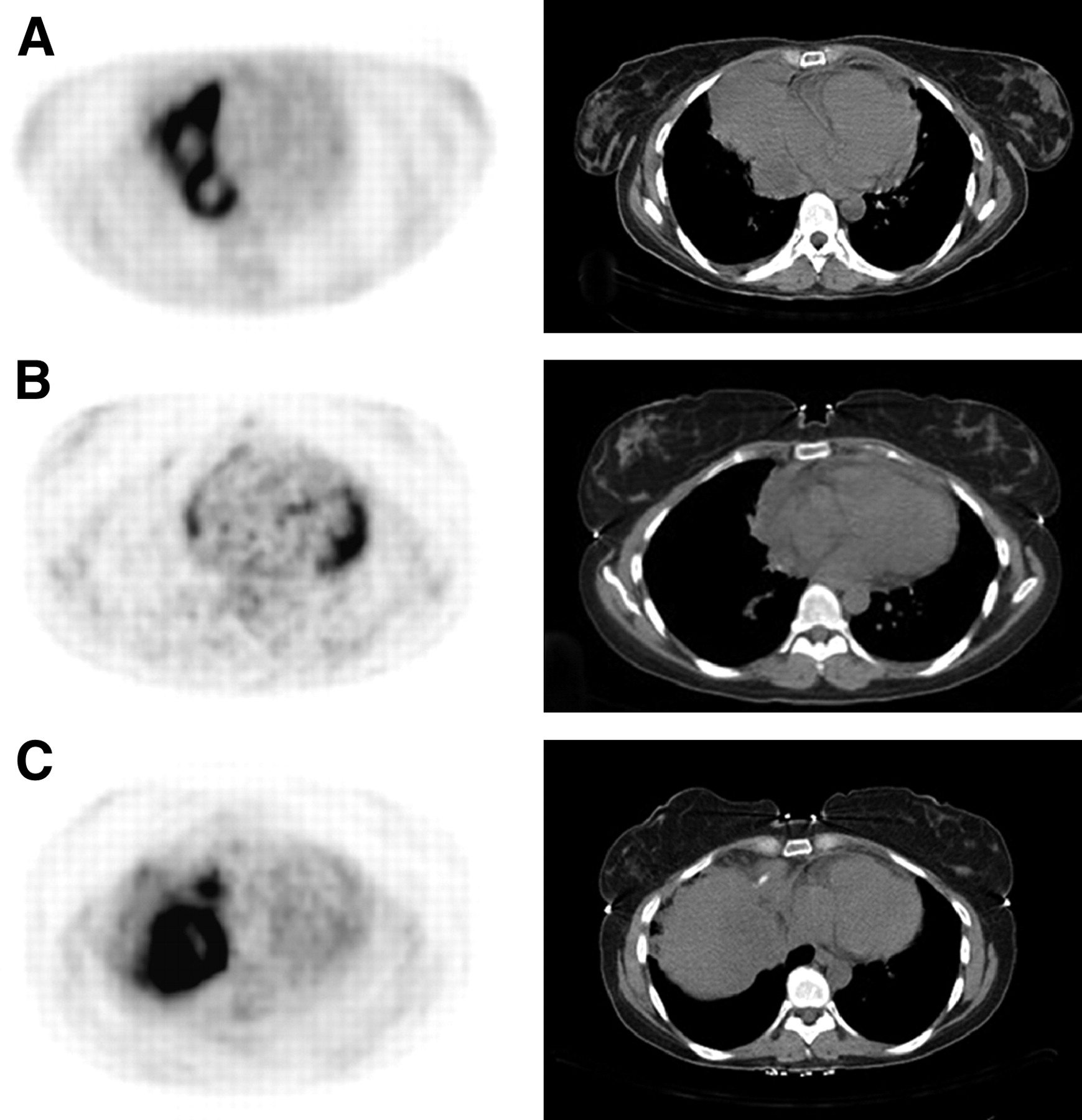
CT scans obtained after treatment may demonstrate a residual tumor mass that is not metabolically active. 18F-FDG PET has been shown to be able to distinguish between posttreatment fibrosis and viable tumor (Figs. 2 and 3). A retrospective review of 27 patients found that all 15 patients with residual biopsy-proven disease and 11 of 12 patients who were disease free were correctly identified with 18F-FDG PET (48). 18F-FDG PET had a higher specificity (92% vs. 17%, P < 0.01), accuracy (96% vs. 63%, P < 0.05), and positive predictive value (94% vs. 60%, P < 0.05) than did CT.

Pretherapy (A) and follow-up posttherapy (B) PET scans of patient with diffuse large B-cell lymphoma with extensive 18F-FDG–avid disease in the neck, mediastinum, and peritoneal infiltration. Follow-up scan demonstrates resolution of disease.

Pretherapy (A) and posttherapy (B and C) PET scans (left) and CT scans (right) of patient with diffuse large B-cell lymphoma and large anterior mediastinal/right pericardial mass. Pretherapy scan shows intense 18F-FDG uptake. One follow-up scan (B) demonstrates shrinkage of mass but persistent uptake. Biopsy was negative for malignant cells. A later follow-up scan (C) demonstrates growth of residual 18F-FDG–avid mass.
There has been much interest in the potential value of PET as a prognostic indicator. Mikhaeel et al. (49) compared the accuracy of PET with that of CT in the assessment of remission in 49 patients with aggressive NHL. Pre- and posttherapy PET scans were obtained for 45 patients, and 33 patients had pre- and posttherapy CT scans. Relapse rates were 100% for patients with positive PET findings and only 17% for those with negative PET findings. In a recently published retrospective analysis of 75 patients with HD or aggressive NHL treated with standard chemotherapy regimens with or without radiation therapy whose disease was restaged with PET and CT, a correlation was found between positive findings on restaging PET and clinical relapse (50). 18F-FDG PET was performed at least 1 mo after the completion of chemotherapy and at least 3 mo after the completion of radiotherapy to minimize false-positive results. Dedicated CT was also performed. After the end of therapy, 59 patients (79%) had negative PET findings, whereas only 16 patients had positive PET findings. Follow-up of these patients revealed that 14 of the 16 PET-positive patients had disease relapse or progression (at a median of 9 mo after completing therapy), whereas none of the 59 PET-negative patients had local disease relapse (P = 0.00001). When the PET and CT results were combined, it was found that of the 5 patients with positive PET findings and negative CT findings after therapy, 4 experienced local relapse or progression of disease 3−12 mo after restaging; none of the 30 patients with negative 18F-FDG PET findings and positive CT findings had experienced disease relapse 6−15 mo later.
Studies of response to treatment with radiolabeled antibodies have also used PET response to document clinical response. A recently published study of 8 patients who had received prior myeloablative therapy and were subsequently being treated with full-dose 90Y-ibritumomab tiuxetan therapy used both CT and 18F-FDG PET to monitor response (51). By 18F-FDG PET, that study demonstrated a complete response in 1 of 7 patients with measurable disease—a finding that correlated with a 10-mo disease-free survival. One patient with residual disease on imaging studies after treatment demonstrated disease progression after 12 wk.
PET for Early Assessment of Treatment Response.
Several investigators have studied the predictive role of PET early in a chemotherapeutic regimen. One study evaluated 18F-FDG uptake using a hybrid PET instrument before and after 1 cycle of chemotherapy in 30 patients with NHL or HD (52). Scans were scored as positive if they showed focal activity that was relatively higher than surrounding background activity. In that study, 15 patients had residual 18F-FDG–avid disease after 1 cycle of therapy. Of these 15 patients, 13 (87%) either experienced relapse or never achieved remission. The remaining 2 patients were in clinical remission for at least 18 mo after therapy. One of these patients had 18F-FDG–avid disease in the thymus, attributed to thymic rebound rather than residual disease. Negative PET findings in that study were highly predictive of remission, with 87% of the patients in complete remission after a median of 19 mo of follow-up. Another study—of 121 patients with NHL, 75 of whom had diffuse large B-cell lymphoma—assessed the utility of 18F-FDG PET after 2–3 cycles of chemotherapy (53). The median follow-up interval for all patients was 24.4 mo. Response was correlated to progression-free survival and overall survival using Kaplan–Meier survival analysis. The 5-y progression-free survival was estimated at 88% for the patients with negative PET findings and only 16.2% for those with positive findings. The authors analyzed subgroups of only the patients with diffuse large B-cell lymphoma and found that 18F-FDG PET still had a predictive value for progression-free survival and overall survival and that the survival curves were similar to those for the whole study.
One study of 20 patients with HD and NHL used visual and quantitative analysis of 18F-FDG PET performed before and after 1 or 2 cycles of chemotherapy (54). Whether complete response had been achieved was determined at the end of therapy on the basis of clinical findings and conventional imaging findings. Follow-up was performed for 24 mo. The study found that of 16 patients with residual uptake after 1 or 2 cycles, only 10 showed no response after completion of therapy (nonresponders). Quantitative analysis demonstrated that those who achieved remission but whose interim PET scan showed persistent uptake had a greater reduction in 18F-FDG uptake than did the nonresponders. The authors were able to separate the responders from the nonresponders using a cutoff of a 60% reduction in SUV.
Several studies have examined 18F-FDG PET for posttreatment and interim evaluation of HD only (55–57), but most studies of NHL have included a range of different histologic types. A recently published prospective study followed 90 patients, 94% of whom had diffuse large B-cell lymphoma (58). All patients received doxorubicin-containing regimens, with or without rituximab, although some received the regimen on a conventional schedule of 8 cycles every 3 wk and some received a dose-intensified regimen with more frequent dosing. 18F-FDG PET and CT were performed before and after 2 cycles of chemotherapy (early PET). Foci of 18F-FDG uptake on baseline scans were scored using a 3-point scale, with posttherapy scans graded as either negative or positive for uptake. Of the 54 patients whose early PET findings were negative, 2-y event-free survival was 82% and overall survival was 90%, compared with a 43% 2-y event-free survival for patients whose early PET findings were positive. This statistically significant prognostic impact (P < 0.001) of early PET was independent of treatment schedule.
PET for Standardized Assessment of Quantitative Parameters.
In 1999, the European Organization for Research summarized recommendations for the measurement of tumor response using 18F-FDG PET (25). Using SUV as the measure of response, the group classified progressive metabolic disease as an increase in SUV of greater than 25% from baseline. A partial metabolic response was classified as a decrease in SUV of 15%−25% after 1 cycle of chemotherapy and a decrease of greater than 25% after more than 1 treatment cycle. Complete metabolic response was defined as complete resolution of 18F-FDG uptake in the tumor. These guidelines may be useful in developing further prognostic factors when using early or interim PET to predict relapse or disease-free survival.
Relying on measurements of metabolic activity also requires that the measurements be reproducible. Various factors can influence the measurement of 18F-FDG uptake, including the time between tracer injection and scanning, because tracer uptake increases over time until approximately 90 min; patient blood glucose levels; lesion size; tumor heterogeneity; and even reconstruction parameters (59). Nevertheless, studies have found measurement of SUV to be consistent: One study that repeated imaging within 10 d showed the 95% normal range for differences in SUV to be only ±0.9, implying that a change in SUV will be considered significant if the difference is more than 0.9 (60).
PET/CT.
The widespread use of combined PET/CT systems offers the potential for more accurate staging with 18F-FDG PET. In particular, PET/CT allows accurate spatial localization of abnormal radioactivity uptake. Although software for merging PET and CT images obtained on different scanners exists, such merging does not always result in accurately fused images (61). Moreover, combined PET/CT offers the advantage of maintaining the same patient positioning on the same bed for both scans. One study compared the reading of side-by-side PET and CT images with the reading of combined PET/CT images and followed the patients for more than 12 mo (62). That study of only 27 patients demonstrated a sensitivity of 78% for CT alone, 86% for 18F-FDG PET alone, 93% for side-by-side CT and 18F-FDG PET, and 93% for combined PET/CT. This result demonstrates the inherent problem facing comparisons of PET/CT with PET alone, in that a careful review of functional 18F-FDG images is complete only when comparable structural (CT or MR) images are reviewed at the same time. A larger study, of 73 patients, followed up the patients clinically and through additional imaging and histology examinations. Discordant results between PET only and PET/CT were seen in 7 patients, with combined PET/CT correctly upstaging disease in 2 patients and downstaging it in 5 patients. PET/CT has been particularly useful in decreasing false-positive PET findings, especially uptake in brown adipose tissue (28,29). Although uptake in brown adipose tissue is often symmetric, particularly in the neck and shoulders, proper localization is especially important for areas such as the upper abdomen, where asymmetric uptake may be mistaken for malignancy (30).
The CT component is, in most cases, not optimized for structural imaging but for attenuation correction of the PET images. The use of CT for attenuation correction (rather than a 68Ge or 137Cs transmission source) reduces scanning time by 40% and also results in virtually noiseless attenuation correction factors (63,64). Current practice consists of performing low-dose, unenhanced CT for PET attenuation and coregistration and, when indicated, separate contrast-enhanced CT. Because this approach increases the patient's exposure to radiation, much attention has been placed on the effect of iodinated contrast material on CT-based attenuation correction. Some studies have shown that PET/CT can be performed with intravenous contrast material without introducing artifacts (65,66), whereas other studies are investigating whether additional contrast-enhanced CT is even needed at all in patients with lymphoma (67).
Other PET Tracers and Future Directions.
Positron-emitting isotopes of gallium would be a natural choice for PET, and several are being investigated for use. 68Ga is convenient because it can be eluted from a germanium–gallium generator, but its short half-life of only 68 min makes it less useful for producing good PET images. 66Ga has a longer half-life (9.5 h) but is difficult to produce in most cyclotrons. Its longer half-life, however, means that commercial manufacturing and distribution would be feasible.
Other 18F-labeled tracers are also under investigation. 18F-3′-deoxy-3′-fluorothymidine (FLT) is a marker of cellular proliferation that is currently being investigated as an alternative to 18F-FDG PET. Although the bone marrow uptake of 18F-FLT may reduce its sensitivity, initial studies have demonstrated promise in imaging NHL (68,69). These studies, of only a few patients, have shown comparable results between 18F-FLT and 18F-FDG PET. One perceived advantage of 18F-FLT PET is that it does not accumulate in areas of inflammation (which can be common in this particular patient population after radiation or infection) and may thus reduce the false-positive rate.
CONCLUSION
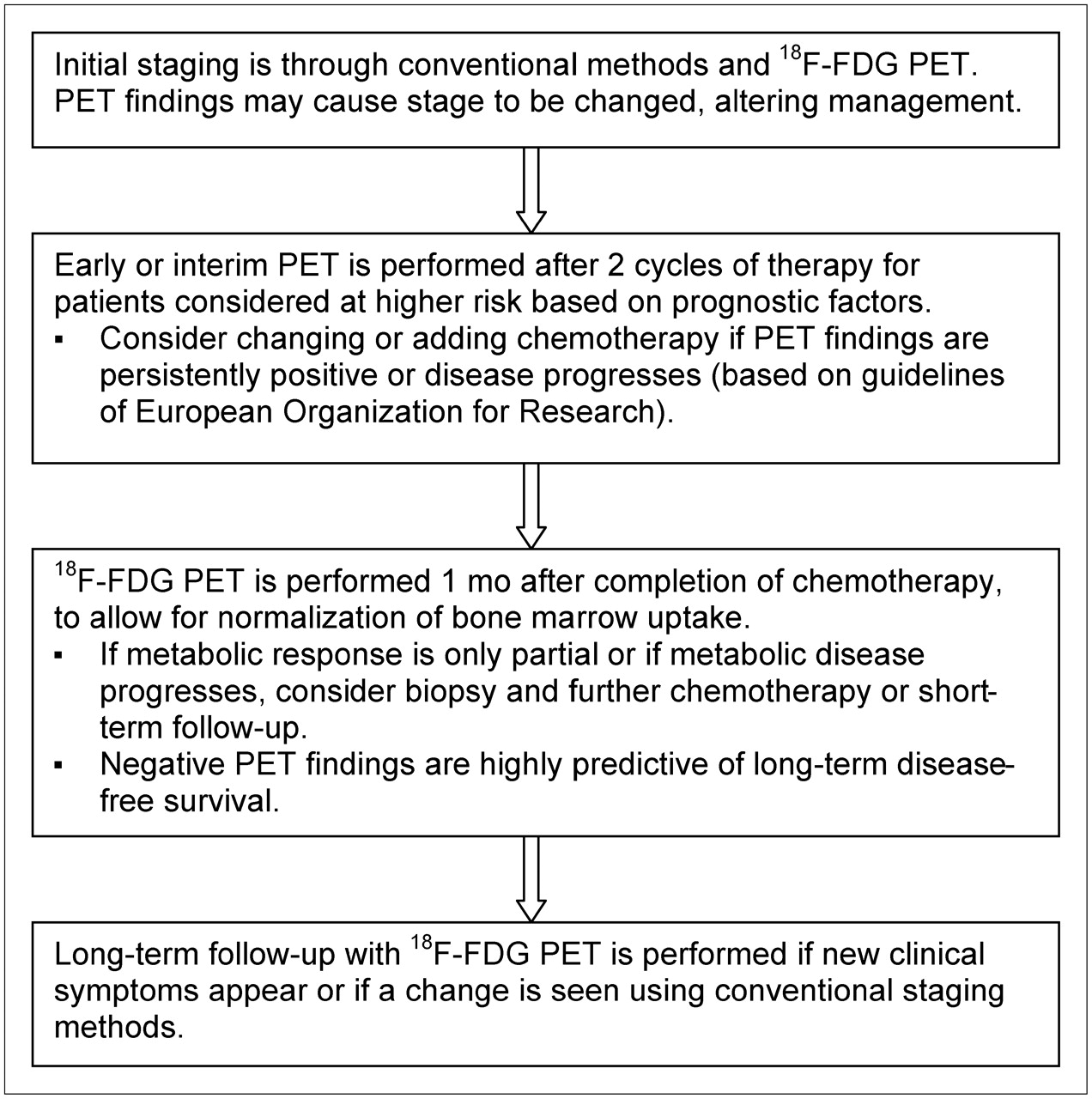
Although CT remains the gold standard for the staging and follow-up of malignant lymphomas, 18F-FDG PET has a potential role in accurately staging disease and in predicting response to therapy. This role has the potential to affect both the initial choice of chemotherapy and the decision to alter management based on the initial response to therapy (Fig. 4). PET performed early in a chemotherapeutic regimen has demonstrated a role in identifying patients who will experience relapse and may require further treatment, but attention to the timing of the scan in relation to chemotherapy and growth factors is crucial. Many studies have used subjective grading systems to assess response and have evaluated progression-free survival on the basis of negative or positive findings on follow-up scans. Further studies should focus on measuring response on the basis of SUV: Determining a cutoff value when assessing the percentage of change in SUV may improve the prognostic value of interim PET. Because most studies have shown variable SUVs among both aggressive and indolent lymphomas, the usefulness of a follow-up scan hinges on the existence of a pretherapy scan demonstrating 18F-FDG–avid disease. The role of 18F-FDG PET for indolent lymphomas remains unclear, and further studies have to be designed to investigate the role of PET for specific histologic types.
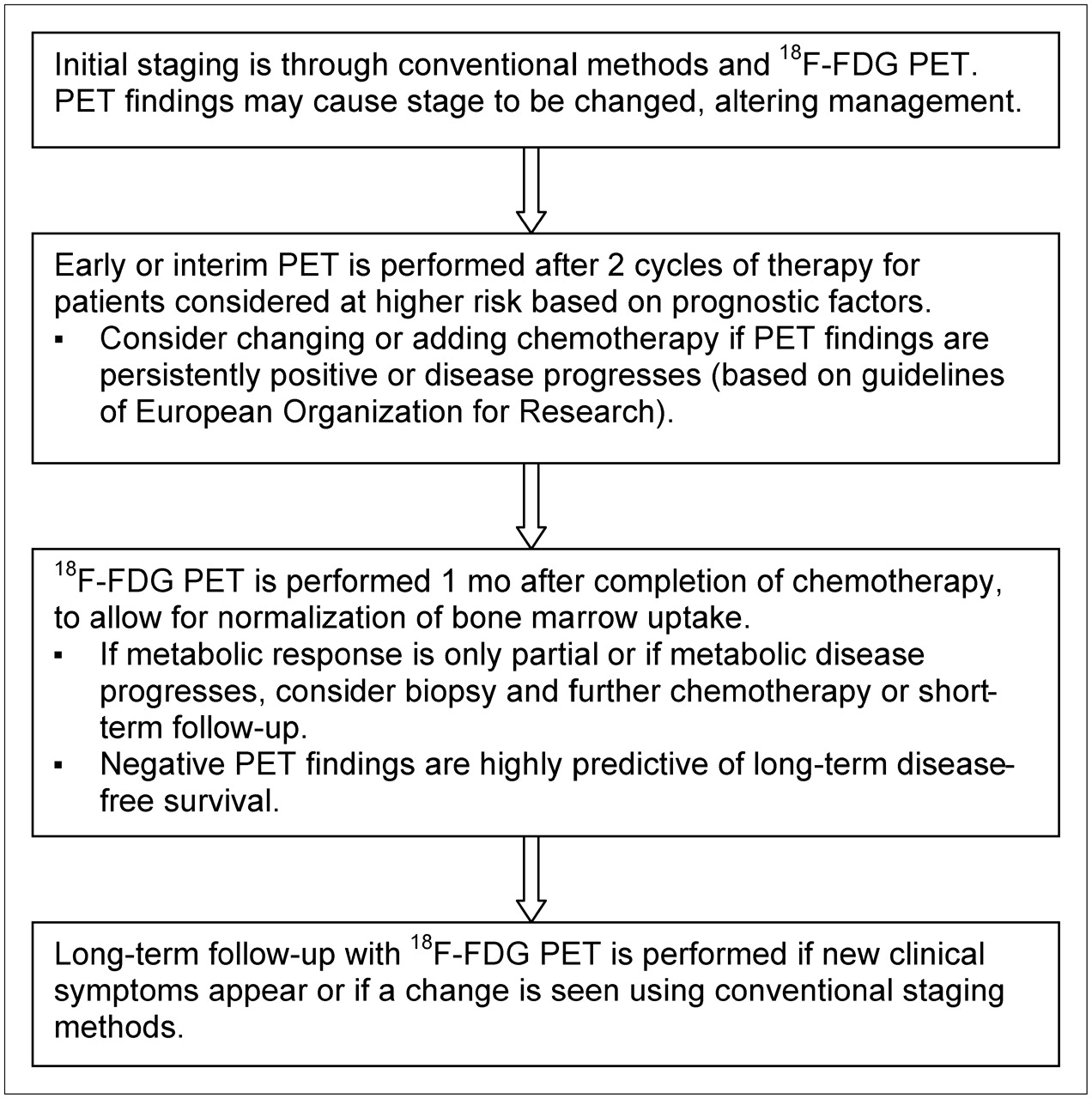
Summary of management of HD and aggressive NHL using 18F-FDG PET.
Acknowledgments
The authors thank Drs. H. William Strauss and Chaitanya R. Divgi for invaluable suggestions and advice.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH AUGUST 2007.
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- Received for publication February 3, 2006.
- Accepted for publication May 11, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Validation of Convolutional Neural Networks for Fast Determination of Whole-Body Metabolic Tumor Burden in Pediatric Lymphoma
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- Clinical utility of 18F FDG-PET/CT in the detection of bone marrow disease in Hodgkin's lymphoma
- The Role of PET and PET/CT in Managing the Care of Lymphoma Patients
- Introduction
- Role of PET/CT Scanning in Initial and Post-Treatment Assessment of Hodgkin Disease
- Imaging in staging of malignant lymphoma: a systematic review