


Abstract
This prospective study was designed to assess the utility of the dual time point imaging technique by 18F-FDG PET in detecting primary breast cancer and to determine whether there is a relationship between 18F-FDG uptake and its change over time and the histopathologic subtypes. Methods: One hundred fifty-two patients with newly diagnosed breast cancer underwent 2 sequential PET scans (dual time point imaging) for preoperative staging. The maximum standardized uptake value (SUVmax) of 18F-FDG was measured from both time points. The percent change in SUVmax (Δ%SUVmax) between time points 1 (SUVmax1) and 2 (SUVmax2) was calculated. Patients were divided into 2 groups according to histopathology as invasive and noninvasive. Invasive tumors were also divided into 2 groups (>10 mm and 4−10 mm). The tumor-to-contralateral normal breast (background) ratios of SUVmax at both time points for groups were measured and the Δ%SUVmax values were calculated. Results: The mean ± SD of the SUVmax1, the SUVmax2, and the Δ%SUVmax were 3.9 ± 3.7, 4.3 ± 4.0, and 8.3% ± 11.5% for invasive; 2.0 ± 0.6, 2.1 ± 0.6, and 3.4% ± 13.0% for noninvasive; and were 1.2 ± 0.3, 1.1 ± 0.2, and –10.0% ± 10.8% for the contralateral normal breast groups, respectively. In the comparison of SUVmax1, Δ%SUVmax, and the tumor-to-background ratios among groups, all results were significant (P < 0.001). Visual assessment revealed that the sensitivity of dual time point imaging was 90.1% for invasive cancer >10 mm, 82.7% for invasive breast cancers 4−10 mm, and 76.9% for noninvasive breast cancers. Conclusion: Dual time point imaging is a simple and noninvasive method that may improve the sensitivity and accuracy of 18F-FDG PET in assessing patients with primary breast cancer. The changes that are noted in SUVs in dual time point imaging vary depending on the histopathologic type of primary breast cancer.
Recent studies have demonstrated that the uptake of 18F-FDG continues to rise in malignant tumors for several hours after the intravenous administration (1–3). In some tumors, the standardized uptake value (SUV, a quantitative measure commonly used) does not reach maximum until 130–500 min after injection of 18F-FDG (2). This is probably related to the increased glucose uptake through the glucose transporter proteins and low concentration of glucose-6-phosphatase activity in these cells. In contrast, such a prolonged period of 18F-FDG uptake is rare in inflammatory lesions or normal tissues (4). Thus, imaging at 2 time points after the administration of 18F-FDG (dual time point 18F-FDG PET) has been shown to differentiate between benign processes and malignant tumors (1,4,5).
Breast cancer is the most common malignancy and the second leading cause of cancer death among women (6). Although it is curable when detected early, about one third of women with breast cancer die of the disease (7). 18F-FDG PET has been quite effective in detecting nodal and distant metastases by acquiring a single whole-body examination in patients with breast cancer (8–10). However, the role of PET for assessing primary breast cancer is somewhat uncertain because of the variable sensitivity and specificity values that have been reported in the literature. This is partially related to the characteristically low SUV values of the primary breast cancer lesions. Therefore, the underlying biologic factors that determine the degree of glucose metabolism and subsequent 18F-FDG accumulation need to be examined to determine such discrepant results. By now, 18F-FDG PET has been shown to have some limitations in detecting breast tumors (11). The uncertainty about the role of 18F-FDG PET in assessing primary breast lesions stems primarily from the fact that the data reported so far were generated by a single time point imaging at 60 min after the administration of 18F-FDG. We, and others, have reported the added advantages of dual time point imaging in head and neck, lung, pancreatic, and cervical malignancies. These data demonstrate that imaging at 2 different time points reveals substantially higher SUVs on delayed scans compared with those measured on the initial scans (1,4,5,12–15). These studies also indicate that this approach can also improve the sensitivity of the technique for the primary and the metastatic sites (1). Therefore, single time point SUV analysis is a suboptimal method for assessing suspected breast cancer. Biologic characteristics of the tumor such as histologic subtype (invasive–noninvasive) are considered important prognostic factors in patients with breast cancer and may therefore influence glucose metabolism as detected by 18F-FDG PET. The aim of this prospective study was to assess the utility of this technique for detecting the primary breast cancer and to determine whether there is a relationship between 18F-FDG uptake and its change over time as determined by dual time point imaging and the histopathologic subtype.
MATERIALS AND METHODS
Patient Population
One hundred fifty-two consecutive patients (age range, 24–80 y; mean age, 51.4 ± 10.7 y) with newly diagnosed breast cancer by film-screening mammography, MRI, and biopsy of the breast lesions were included in this study. For the purpose of this scientific communication, we present the data that were generated with 18F-FDG PET. This prospective National Institutes of Health–funded program project was designed to test the role of various radiologic modalities for detecting and staging primary breast cancer. This study was Health Insurance Portability and Accountability Act compliant and approved by the Institutional Review Board. Informed consent was obtained from the patients who were enrolled in this study. The average time period between the diagnostic biopsy and dual time point PET was 25 ± 12 d. The reason for the long time period until PET was due to the complications caused by diagnostic biopsy such as hematoma, seroma, or inflammatory reactions. These were excluded from analysis. None of the patients had received chemotherapy or radiation therapy before they underwent dual time point 18F-FDG PET for preoperative staging.
18F-FDG PET and Assessment
Patients fasted for at least 4 h before the PET scan and had blood glucose levels <140 mg/dL at the time of injection. 18F-FDG (5.2 MBq/kg of body weight) was administered intravenously through an indewelling catheter inserted into an antecubital vein. PET was performed on all patients using a dedicated whole-body PET scanner (Allegro; Philips Medical Systems). The first scan was performed as a whole-body image that included the entire trunk (from neck to the groin). Immediately after the whole- body scan, a second set of images of the chest were acquired. The mean time intervals between the injection of 18F-FDG and the first and second scans were 63 min (range, 46–112 min) and 104 min (range, 81–156 min), respectively. Using a 137Cs point source, transmission scans were performed to provide attenuation correction. The patients did not leave the scanning table between the 2 acquisitions, minimizing patient motion artifacts. The ordered-subsets expectation maximization method was used to reconstruct all PET images (16). After PET, patients underwent a surgical intervention that included either partial or total mastectomy. Surgical pathology results were considered to provide the definitive diagnosis against which the PET results were compared. On the basis of the surgical results, 25 patients who had no tumor (all tumor tissue was removed during excisional diagnostic biopsy) and 7 patients who had 1- to 3-mm tumor were excluded from the study. In this population some of the PET findings were false-positive because of biopsy inflammation, and the findings are not described further in this article. Therefore, 120 patients who had core biopsy were included in the study.
Visual assessment was determined by 1 experienced nuclear medicine physician and included assessing both sets of images at the same time; we believe that this is adequate for the initial analyses of these data. The interpretation consisted of only a 1-time reading of the image set. Visual (qualitative) interpretation was based on subjective impression of the degree of 18F-FDG uptake at the tumor site and the surrounding sites. If the uptake appeared distinctly focal and its contrast increased with time, the lesion was categorized as positive for cancer. In contrast, if the lesion was poorly defined and lost contrast over time, it was interpreted as negative for cancer. When the lesion could not be categorized as positive or negative, it was considered as “indeterminate” and was excluded from the final analyses. 18F-FDG PET scans were interpreted without the benefit of the other radiologic studies.
Image Analysis
After image reconstruction, a region of interest (ROI) was carefully drawn around the site of the breast lesion on the consequent 4–6 PET scan slices. Slice thickness and the slice interval were both 4 mm. This analysis was performed uniformly by an experienced nuclear medicine physician for the entire population examined. From these ROIs, the SUV was calculated according to the following formula: (mean ROI activity [MBq/g])/(injected dose [MBq]/body weight [g]), where g = grams.
The maximum SUV (SUVmax) of 18F-FDG was measured from the ROI, which was placed at the site of the lesion clearly visualized or appearing suggestive on the PET scans from first time point (SUVmax1) and second time point (SUVmax2). The percent change in SUVmax (Δ%SUVmax) between SUVmax1 and SUVmax2 was calculated. We applied the same methodology for calculating the SUVs from the contralateral normal glandular breast tissue as another reference point for comparison (group C = contralateral normal breast) as a measure of background activity and for further analysis of the data generated from the lesion sites. The SUVmax of 18F-FDG of the contralateral normal breast glandular tissue was measured from the ROI, which was placed around the normal glandular tissue at the best visualized 4–6 slices on the PET scan at both time points. The SUVmax changes were compared among groups and with contralateral breast glandular tissue values.
Patients were divided into 2 groups according to surgical histopathology results (group A = invasive ductal, lobular, and mixed [ductal + lobular] types); group B = ioninvasive (carcinoma in situ). Invasive cancers were also divided into 2 groups according to the size of the surgical lesion (>10 mm and 4−10 mm) for further analysis. We calculated tumor-to-background ratio (T/B ratio) of SUVmax at both time points 1 (ratio 1) and 2 (ratio 2) for each lesion (group A and group B), and the percent change in these ratios over time was calculated. For this purpose, we used the same patient's contralateral breast tissue's 2 time points' SUVmax results as background. We divided SUVmax of the tumor by the same patient's contralateral breast SUVmax value for both time points to generate these ratios.
Statistical Analysis
Conventional methods were used to generate descriptive statistics. Groups were compared by using the Student t test. P values < 0.05 were considered to represent significant difference between the 2 populations.
RESULTS
Among 152 patients, 120 patients with 123 lesions (3 patients had bilateral disease) were analyzed in this study. As mentioned above 32 patients were excluded from the analysis. Ninety patients (with 93 lesions) were found to have invasive cancers and the remaining 30 were diagnosed with noninvasive cancers and the size of invasive carcinomas ranged 4 to 60 mm. On the basis of the surgical histopathologic examination, 63 of the invasive carcinomas had a tumor size >10 mm (average, 24.9 ± 11.4 mm; range, 11–60 mm), whereas 30 had 4- to 10-mm lesions (average, 6.5 ± 2.8 mm).
Visual Assessment
Visual assessment revealed the following results: Of the 63 tumors >10 mm in size, 55 were clearly visualized on the combined dual time point scans, whereas 2 were read as indeterminate and 6 appeared without 18F-FDG uptake (false-negative). In general, images appeared more intense and clear on delayed images. However, no effort was made to determine how many abnormalities were negative or questionable on the first set and clearcut on the delayed images. Therefore, the sensitivity of the dual time imaging method was 90.1% for invasive cancer >10 mm (2 indeterminate cases were not included for this analysis) Examples are presented in Figures 1 and 2. In 30 invasive tumors that were 4- to 10-mm in size, 24 were clearly detected by 18F-FDG, 5 were read as negative (false-negative), and 1 appeared indeterminate. Therefore, the sensitivity of the dual time method was 82.7% for detecting invasive cancers 4−10 mm (1 indeterminate case was excluded for this calculation). Of the 30 noninvasive tumors based on histology, 20 were seen on dual time point imaging, 4 were interpreted as indeterminate, and the remaining 6 were read as negative for cancer (false-negative). Therefore, the sensitivity of dual time 18F-FDG PET for the detection of noninvasive breast cancer was 76.9% (4 indeterminate cases were not included in this calculation). An example is presented in Figure 3. In summary, dual time point 18F-FDG PET was true-positive for 99 lesions, whereas it was indeterminate for 7 and false-negative for 17 lesions. Invasive mucinous cancer lesion was false-negative by visual assessment.

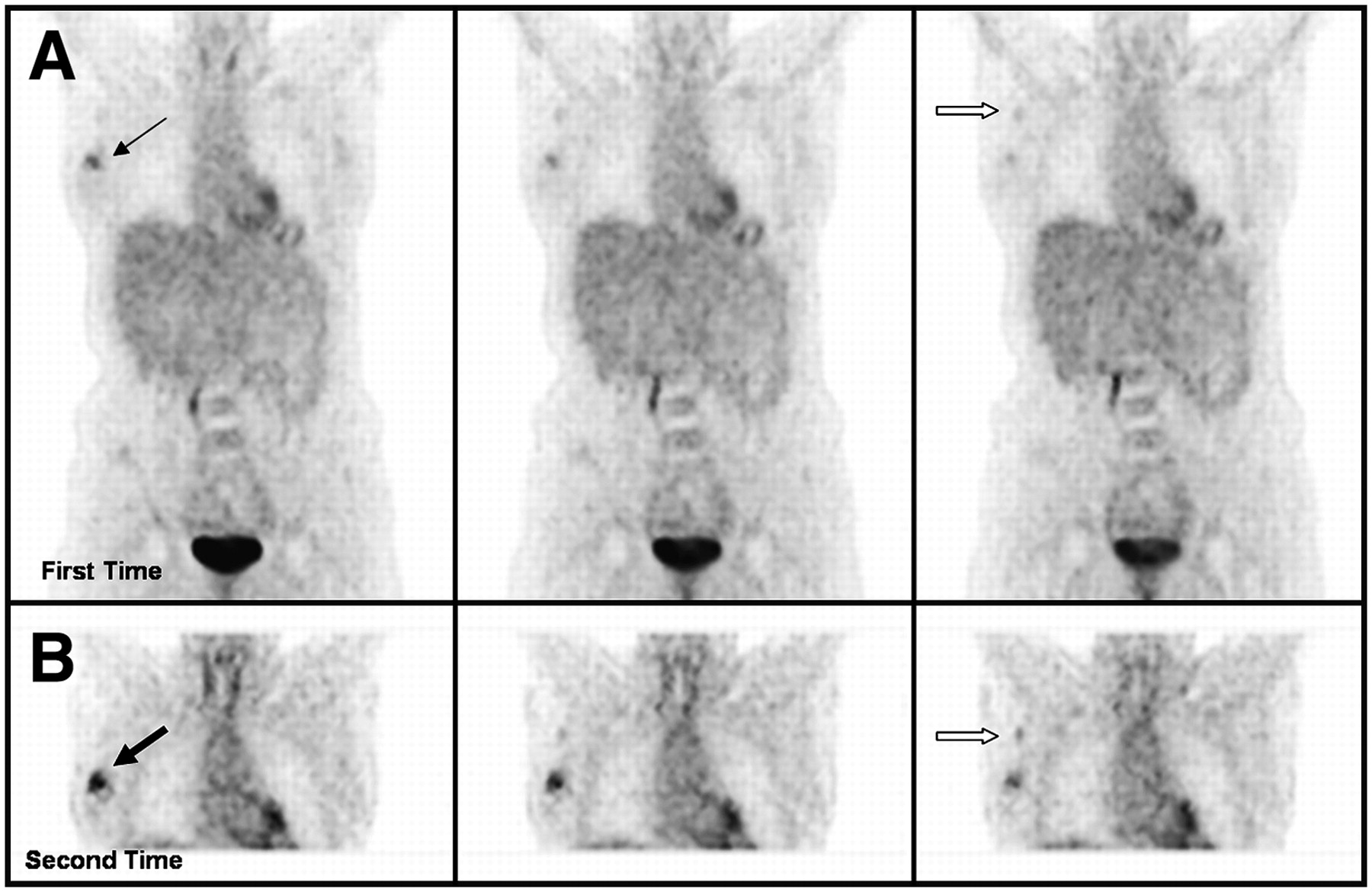
Patient with history of invasive ductal cancer of right breast had dual time point PET. (A) Coronal slices in top row were obtained at first time point. (B) Corresponding scans in bottom row were acquired at second time point. Measured SUVmax1 of lesion in first image set was 4.3 (thin arrow), whereas that of second set was 4.8 (thick arrow). Percent increase in SUV of the lesion was 11.6%. Measured SUVmax1 of normal contralateral glandular breast tissue was 1.1 in first image set, whereas that of second set was 0.9. Therefore, increase in T/B ratios between first image set and second image set was 36.4%. Surgical pathology confirmed 2-cm invasive ductal cancer.
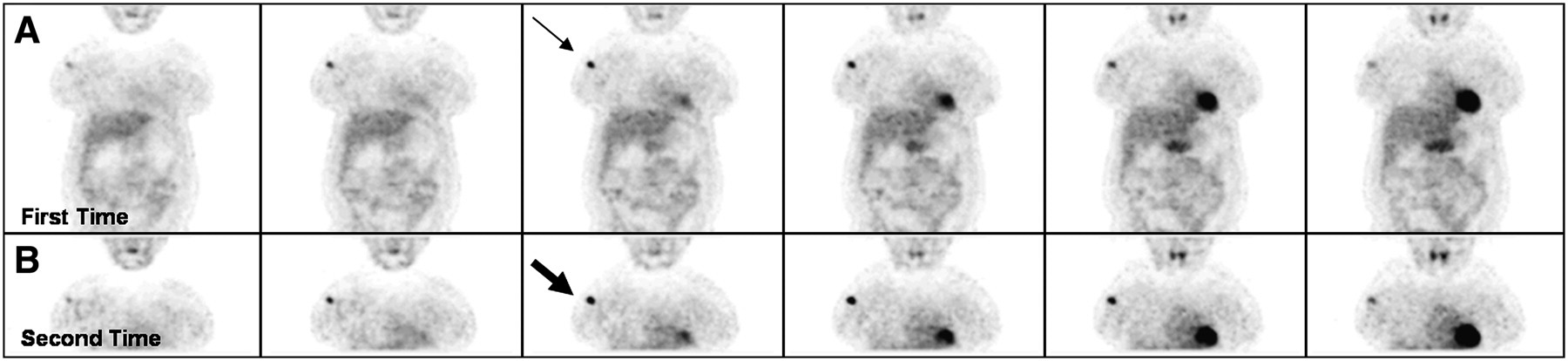
Patient with invasive ductal carcinoma of right breast was examined with dual time point PET. (A) Coronal slices in top row were obtained at first time point. (B) Corresponding images in bottom row were acquired at second time point. Images in both sets clearly show primary lesion. However, intensity of uptake was substantially higher on delayed images. In addition, axillary lymph node metastasis was faintly visualized on first set but was clearly demonstrated on second set. Measured SUVmax1 of lesion in first image set was 2.2 (thin black arrow), whereas that of second set was 2.6 (thick black arrow). Percent increase in SUV of the lesion was 18.2%. SUVmax1 of metastatic right axillary lymph node was 1.0 in first set (open arrow in A) and increased to 1.1 in second set (open arrow in B). Surgical pathology confirmed 2.5-cm invasive ductal carcinoma with axillary metastasis.

Patient with history of noninvasive carcinoma of right breast underwent dual time point 18F-FDG PET for preoperative staging. (A) Coronal slices in top row were obtained at first time point. (B) Corresponding scans in bottom row were acquired at second time point. Lesion is questionable in first set, whereas it is clearly visualized in second set. Measured SUVmax1 of lesion in first image set (thin arrow) was 1.4, whereas that of second set was 1.9 (thick arrow). Percent change from first to second time point of this measurement was 35.7%. Surgical pathology confirmed noninvasive breast tumor.
SUV Measurements
The SUVmax could not be measured for the lesions that were not visualized on PET scan. These lesions were not 18F-FDG avid and, therefore, they were false-negative. Therefore, SUVmax could be calculated for 106 lesions and for the contralateral breasts. The means ± SD of the SUVmax1, the SUVmax2, and Δ%SUVmax were 3.9 ± 3.7, 4.3 ± 4.0, and 8.3% ± 11.5% for group A; 2.0 ± 0.6, 2.1 ± 0.6, and 3.4% ± 13.0% for group B; and 1.2 ± 0.3, 1.1 ± 0.2, and −10.0% ± 10.8% for group C, respectively. When SUVmax1 and the Δ%SUVmax among these 3 groups were compared separately, results were statistically significant for each comparison (P < 0.001). The percent change (decrease in 18F-FDG uptake) between SUVmax1 and SUVmax2 over time in the contralateral normal breast tissue was also significant (P = 0.02). The percent change between ratio 1 and ratio 2 over time was 22.0% ± 26.8% for group A and 15.7% ± 18.6% for group B. Because of some outlier values that resulted in high SD, we calculated the confidence interval (CI) for these data. For group A and B, the 95% CI values for the Δ%SUVmax were 6.0%−10.6% and −1.3% to 8.0%, respectively. For group A and B, the 95% CI values for the percent change over time between the T/B ratios at dual time imaging were 15.9%−28.1% and 8.0%−23.5%, respectively. When we compared the ratio 1 of group A and ratio 2 of group A with those of group B values, results were statistically significant (P < 0.001) (Table 1).
SUVmax Measurements and Changes over Time in Normal Breast, Invasive Cancer, Noninvasive Cancer, and T/B Ratios
The calculated SUVmax1 values of invasive ductal, lobular, and mixed types were 4.3 ± 3.9, 2.7 ± 1.8, and 2.0 ± 0.9, respectively. In the comparison of the SUVmax1 of invasive ductal carcinoma with those of the invasive lobular and mixed type, the results were significant (P = 0.04 and P < 0.001, respectively) (Table 2). Only 1 patient each with medullary cancer and mucinous cancer was enrolled in the study and they were included in Table 2 without statistical analysis. We then divided invasive cancers into 2 groups according to tumor size (>10 mm and 4−10 mm). The calculated means ± SD of the SUVmax1, SUVmax2, Δ%SUVmax between 2 time points over time, and the percent change over time in T/B ratios at dual time imaging for the >10-mm tumors were 4.8 ± 4.1, 5.3 ± 4.4, 8.6% ± 12.2%, and 23.1% ± 28.5%, respectively. The same calculated values for 4- to 10-mm tumors were 1.9 ± 0.8, 2.0 ± 0.7, 6.5% ± 9.9%, and 18.8% ± 23.5%, respectively (Table 3). Because of some outlier values that resulted in high SD, we calculated the CI for these data. Among invasive tumors, for the group of tumors >10 mm and for the other group that has 4- to 10-mm tumors, the 95% CI values for Δ%SUVmax were 5.5%−11.8% and 2.8%−10.3%, respectively. For the same groups, the 95% CI values for the percent change over time between ratio 1 and ratio 2 at dual time imaging were 15.1%−31.0% and 8.2%−29.3%, respectively. By visual assessment, most lesions became more intense on delayed scans. We investigated the possible reasons for the false-negative results and noted that the histopathology of the 6 false-negative invasive cancers >1 cm were mixed (ductal + lobular) in 3, lobular in 1, mucinous in 1, and invasive ductal in 1. In addition, estrogen receptors were positive in all, progesterone receptors were positive in 5, and all were negative for HER2/Neu (c-erbB-2) receptors.
SUVmax Measurements and Changes over Time in Invasive Cancers According to Subtypes
SUVmax Measurements and Changes over Time According to Tumor Size in Invasive Cancers with Increase in T/B Ratios
DISCUSSION
Because the uptake of 18F-FDG in malignancies is expected to increase over several hours, an initial inclination would be to perform a single scan at a later time point than at the usual 45–60 min after injection of the compound. In theory, this should lead to improved contrast between the lesion and the background and improved diagnostic accuracy, making dual time point scanning unnecessary. However, this will lead to improved sensitivity but the specificity may remain low because of the overall low uptake of these lesions. Therefore, we believe that changes in the dual time point SUVs would be a more valuable diagnostic tool than a delayed single time point alone.
As with most other cancers, studies have shown that most breast malignancies also have a gradual increase in SUV with time after 18F-FDG injection (17,18) and also there is an overexpression of Glut-1 glucose transporters in human breast cancer as in other malignancies (19,20). 18F-FDG PET is very sensitive in detecting advanced disease with nodal or distant metastasis (8–10). However, this technique is known to have some limitations in detecting (a) small-sized tumors, (b) more well-differentiated histologic subtypes of tumors (tubular carcinoma and in situ carcinoma), and (c) lobular carcinomas (11). The overall sensitivities and specificities in these studies for detecting primary breast cancer ranged from 80% to 100% and 75% to 100%, respectively, with an accuracy of 70%–97%, a positive predictive value of 81%–100%, and a negative predictive value of 52%–89% (7,8,21–26). Reports with high sensitivity for PET are partially related to including patients with large-size tumors and the criteria used for interpreting the scans. The results from our study demonstrated that malignancies in the breast follow the same general trend of most other types of cancers and revealed increased 18F-FDG uptake over time. In the comparison of the results of noninvasive cancers with invasive cancers, our study demonstrated that invasive cancer lesions had a higher dual time point increase in 18F-FDG uptake. In addition, invasive ductal cancer showed a significantly higher SUVmax1 value than those of invasive lobular and mixed types, which are relatively well-differentiated invasive cancers in this study. These results are in line with those reported in the literature (11). Demura et al. showed that there is a positive correlation in dual time point change with the degree of cellular differentiation in lung cancers (12). Despite the lower SUVmax1 values of invasive lobular and mixed types in this study, we calculated the increased uptake and high T/B ratio on the delayed image as the invasive ductal type, which resulted in higher detectability for these types. Our results showed a strong correlation between dual time point changes and histologic subtypes in breast cancer.
Another important result of our study was that, although the malignant tissues had positive dual time changes in SUV, the normal breast tissue showed either no change or negative dual time point changes. This would suggest that dual time point imaging will improve the sensitivity of the test, as it is expected that normal tissue would not accumulate 18F-FDG over an extended period of time.
The percent change over time in T/B ratios between ratio 1 and ratio 2 was high, as shown before for invasive and noninvasive cancers, which resulted in improvement in the detection of malignant lesions. Therefore, by using this method, despite the low initial SUV of small tumors, the intensity of the uptake was higher on delayed images, which resulted in higher detectability. In our study the visual assessment revealed the following results: The sensitivities of the dual time imaging method in detecting invasive cancer >10 mm, invasive cancers 4−10 mm, and noninvasive breast cancer were 90.1%, 82.7%, and 76.9%, respectively. In the largest study in the literature, Avril et al. (24), using single time point PET, found the sensitivities of PET were 91%, 57%, and 25% in detecting tumors >10 mm, <10 mm, and noninvasive cancer, respectively. When we compare our results with those of Avril et al., we conclude that dual time imaging substantially increases the contrast between the lesion and the surrounding background and, therefore, improves the sensitivity of this technique for detecting primary breast cancer.
There are limitations that probably influenced the sensitivity in this study. First, all of these patients had prior diagnostic biopsies that likely removed a portion of the cancer tissue. Consequently, the overall 18F-FDG uptake was decreased, lowering the contrast on the PET study because of the smaller size of the remaining tumor tissue at the site. However, it is possible that in some patients inflammatory reaction to surgical intervention could have contributed to the uptake of the lesion site. Considering the design of the study, this type of effect was unavoidable but likely did not substantially alter the results described in this study. In addition, we excluded patients who could have been inappropriate for this analyses because of the factors described earlier. Second, the time interval between the first and the second scans was an average of 39 min. Given the initial low SUV levels, breast cancer lesions may require a longer interval of time to allow adequate 18F-FDG accumulation. As mentioned earlier, most cancers require several hours to reach the maximum level in 18F-FDG uptake. We believe that if this study were performed before biopsy and the time interval between the 2 scans could have been longer, such as 60 min, our results would have been more striking. Also, because of the nature of the study, the specificity of the technique in excluding cancer could not be determined and is the subject of further investigation. Also, we consider the small sample of patients in the category of noninvasive tumors as a deficiency of this report. However, as we increase the number of patients in each of these categories, updated data will be generated for future communications. We also believe that dual time point imaging has a potential role in detecting recurrent disease where either single time point 18F-FDG PET images or other diagnostic studies may appear indeterminate.
CONCLUSION
Our data indicate that 18F-FDG uptake increases with time in breast malignancies that are demonstrable by dual time point PET. On the other hand, the uptake of 18F-FDG in normal breast tissue decreases with time. We also were able to show that the histopathologic type contributes to the changes that are noted in the measured SUVs in dual time point 18F-FDG PET in patients with breast cancer. The difference in such measures may reflect the biologic behavior, including the degree of aggressiveness of the underlying malignancy. Dual time point imaging was especially useful in detecting (a) noninvasive (carcinoma in situ) breast cancer, (b) invasive small lesions (<10 mm), and (c) invasive lobular and mixed types of carcinomas. We conclude that dual time point imaging is a simple and noninvasive method that will improve the sensitivity and accuracy of 18F-FDG PET in assessing patients with primary breast cancer.
Acknowledgments
This work was supported by U.S. Public Health Services Research grant M01-RR00040 from the National Institutes of Health. This study was presented at the Radiological Society of North America 2005 meeting and was selected for a Research Trainee Prize by the Scientific Program Committee. The authors thank Janet Saffer, PhD, physicist at the Hospital of the University of Pennsylvania, for her valuable assistance in analyzing data from this study.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 25, 2006.
- Accepted for publication June 12, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Assessing PET Parameters in Oncologic 18F-FDG Studies
- Multicenter Clinical Trials Using 18F-FDG PET to Measure Early Response to Oncologic Therapy: Effects of Injection-to-Acquisition Time Variability on Required Sample Size
- Voxel-Based Analysis of Dual-Time-Point 18F-FDG PET Images for Brain Tumor Identification and Delineation
- PET Tumor Metabolism in Locally Advanced Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: Value of Static versus Kinetic Measures of Fluorodeoxyglucose Uptake
- 18F-FDG PET of Locally Invasive Breast Cancer and Association of Estrogen Receptor Status with Standardized Uptake Value: Microarray and Immunohistochemical Analysis
- The Effect of Age, Menopausal State, and Breast Density on 18F-FDG Uptake in Normal Glandular Breast Tissue
- 18F-FDG Uptake in Lung, Breast, and Colon Cancers: Molecular Biology Correlates and Disease Characterization
- Reproducibility of Standardized Uptake Value Measurements Determined by 18F-FDG PET in Malignant Tumors
- Time and Again, Children Resemble Their Parents
- Breast Cancer Staging in a Single Session: Whole-Body PET/CT Mammography