


Abstract
In peptide receptor radionuclide therapy (PRRT) using somatostatin analogs labeled with β-emitters, the radiosensitive kidney is the dose-limiting organ, because of high uptake and retention of the radionuclides after glomerular filtration. Dosimetry calculations are mostly based on the MIRD scheme, assuming homogeneous renal radioactivity distribution. The aim of this study was to reveal the radioactivity distribution in the normal human kidney after intravenous injection of [111In-diethylenetriaminepentaacetic acid (DTPA)]octreotide. Methods: Three patients received intravenous injection of [111In-DTPA]octreotide before nephrectomy because of renal cancer. Distribution of radioactivity in the human kidney was investigated using SPECT scanning before and ex vivo autoradiography of the kidney after surgery. Results: Radioactivity was localized predominantly in the cortex of the kidney. In the cortex, radioactivity was not distributed homogeneously but formed a striped pattern, with most of the radioactivity centered in the inner cortical zone. Conclusion: These findings show that average dose calculations using the MIRD scheme, assuming homogeneous renal radioactivity distribution, are inadequate to estimate the radiation dose to various parts of the kidney after PRRT. Different effects due to inhomogeneity can be expected from PRRT using radionuclides emitting particles with short particle ranges, for example, Auger electron emitters, α-emitters, and low-energy β-emitters.
On their plasma membranes, cells express receptor proteins with high affinity for regulatory peptides, such as somatostatin. Changes in the density of these receptors during disease (e.g., overexpression in many tumors) provide the basis for new imaging and radionuclide therapy methods. The peptide analogues most successfully applied for visualization of receptor-positive tumors are radiolabeled somatostatin analogues. Scintigraphy with 111In-diethylenetriaminepentaacetic acid (DTPA)-octreotide (Octreoscan; Mallinckrodt, Inc.) has proven to be sensitive and specific for localizing somatostatin receptor-positive tumors and their metastases (1). Continuing research is aimed at developing a therapeutic analog taking advantage of the specificity of the receptor binding and the localized radiation dose from the radionuclide linked to the peptide. Because indium (111In) emits 2 long-range γ-rays, it is not optimal for therapeutic use. Instead, [90Y-dodecanetetraacetic acid (DOTA),Tyr3]octreotide, with the high-energy β-emitter 90Y (mean energy, 0.93 MeV; half-life, 64 h) strongly linked in the DOTA-cage, has been developed and is now clinically being evaluated for an optimized peptide receptor radionuclide therapy (PRRT) (2–8). [90Y-DOTA-Tyr3]octreotide lacks γ-emission itself or a γ-ray-emitting diagnostic analog.
177Lu (T1/2, 6.7 d) emits, besides β-particles (mean energy, 0.13 MeV), γ-rays suitable for imaging (113 keV at 6% per decay and 208 keV at 10% per decay). Together with a slightly altered somatostatin analog, octreotate, in which the amino acid threoninol at the C-terminal side of the octapeptide has been replaced by threonine, [177Lu-DOTA-Tyr3]octreotate forms a superior therapeutic compound with considerably enhanced uptake in receptor-positive tumors (9–11).
In most radionuclide therapies, bone marrow toxicity is dose limiting. In PRRT, bone marrow is also at risk, but after PRRT using somatostatin analogs labeled with β-emitters, such as 90Y and 177Lu, the radiosensitive kidney is the dose-limiting organ because of high uptake and retention of radionuclides in the kidney after glomerular filtration.
Clinical PRRT studies aim at a maximum renal radiation dose of 23–27 Gy, because this dose is expected to produce clinically significant nephrotoxicity in 5%–50% of the subjects by 5 y of follow-up, based on experience with fractionated external-beam radiation therapies (12). Dosimetry calculations are based on the MIRD scheme, providing a generalized phantom with which the doses to all internal organs can be calculated from the organ residence times for the considered radionuclide, assuming homogeneous radioactivity distribution over the kidney. The radiation dose that can be delivered safely to the kidneys during PRRT remains to be established, however. Also, the exact mechanism of renal uptake and localization of radioactivity, whether homogeneous over the kidney or confined to certain areas, after radiolabeled somatostatin analog injection in patients is not known.
The aim of this study was to reveal the radioactivity distribution in the human kidney after intravenous injection with [111In-DTPA]octreotide, using ex vivo autoradiography. [111In-DTPA]octreotide is a practical model peptide for the larger group of radiolabeled somatostatin analogs currently being used for PRRT.
MATERIALS AND METHODS
Three men with single primary renal tumors received 220 MBq of [111In-DTPA]octreotide intravenously 96 h (patient 1, aged 54 y), 72 h (patient 2, aged 65 y), or 48 h (patient 3, aged 70 y) before nephrectomy. None of the patients used Sandostatin (Novartis) subcutaneously or intramuscularly. All patients gave informed consent to participate in the study. 111InCl3 and [DTPA]octreotide were from Mallinckrodt Medical BV, and labeling was performed in accordance with the package insert. Twenty-four hours after injection, planar scintigraphy and SPECT were performed. During surgery, renal tissue was obtained for ex vivo autoradiography. The pieces of radioactive kidney for autoradiography were taken from the nonneoplastic part of the organ. From patients 1 and 2, complete renal lobes (consisting of a medullary pyramid and the overlying cortex) were obtained. From patient 3, part of a renal lobe was obtained. The tissue was frozen on ethanol/dry ice and processed further for autoradiography. The tissue was embedded in TissueTek (Sakura) and processed for cryosectioning. Tissue sections (10 μm) were mounted on glass slides. Several slides were used to make autoradiographs, and the adjacent sections were hematoxylin-eosin stained. The sections were exposed to phosphor imaging screens (Packard Instruments Co.) for 1 d in radiographic cassettes. The screens were analyzed using a Cyclone phosphor imager (Packard) and a computer-assisted OptiQuant 03.00 image processing system (Packard) (1).
RESULTS
Figure 1A shows the SPECT image of patient 1, made 24 h after injection of [111In-DTPA]octreotide, with uptake in the tumor, spleen, and normal kidney indicated. Figure 1B shows a photograph of the renal lobe from this patient, available for autoradiography. The renal medulla and cortex can clearly be distinguished.

(A) SPECT image of patient 1, made 24 h after injection of [111In-DTPA]octreotide, showing uptake in tumor (T), spleen (S), and normal kidney (K). (B) From same patient, photograph of the renal lobe available for autoradiography 96 h after injection of [111In-DTPA]octreotide. The renal medulla (M) and cortex (C) can clearly be distinguished.
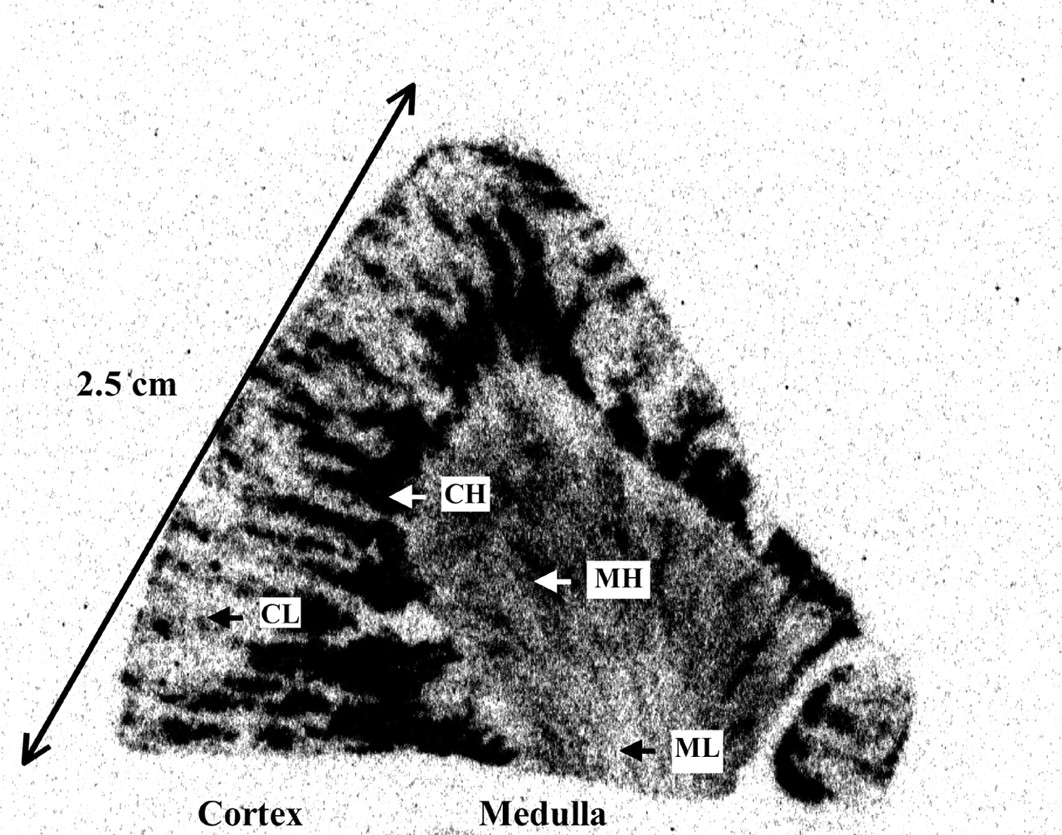
Figures 2A–2C show the ex vivo autoradiograms of renal tissue sections from the 3 patients. Radioactivity is seen to be localized predominantly, but not exclusively, in the cortex of the kidney. In the cortex, radioactivity was not distributed homogeneously but formed a consistent, striped pattern, with most radioactivity centered in the inner cortical zone. Four areas in the cortex and medulla were defined, representing cortex with high uptake (CH), cortex with low uptake (CL), medulla with high uptake (MH), and medulla with low uptake (ML) (Fig. 3). Radioactivity in 10 regions of interest (ROI) in each of these 4 areas was quantified using OptiQuant and was expressed as the percentage of the ROI with the highest radioactivity density (expressed as density light units (DLU)/mm2) for each kidney.

(A–C) Ex vivo autoradiograms of renal tissue sections from patients 1 (A), 2 (B), and 3 (C), obtained 96 h, 72 h, and 48 h, respectively, after injection of [111In-DTPA]octreotide.

Kidney ex vivo autoradiogram of patient 2, showing the 4 defined areas in the cortex and medulla.
Figure 4 shows that the relative amount of radioactivity in CH was comparable in the 3 patients (around 75% of the ROI with maximum DLU/mm2). Radioactivity in MH, however, was more variable, ranging from around 40% of the ROI with maximum DLU/mm2 for patients 1 and 2 to 80% in patient 3, who had the shortest interval (48 h) between [111In-DTPA]octreotide injection and nephrectomy. The results in the medulla of the kidney of patient 3 could not be fully evaluated because of the low amount of medullary tissue available.
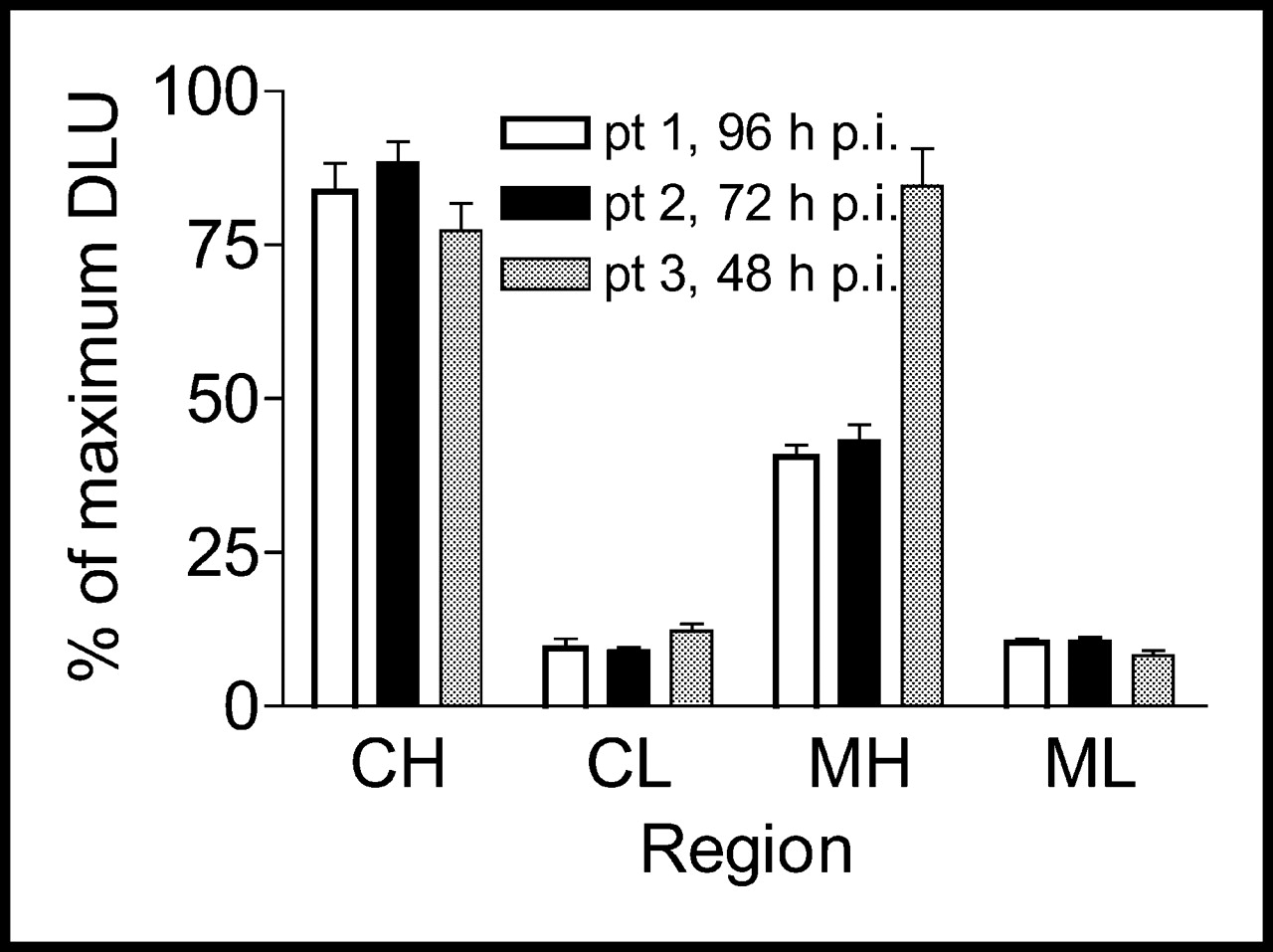
Relative amount of radioactivity in CH, CL, MH, and ML (expressed as percentage of ROI with maximum DLU/mm2). pt = patient, p.i. = after injection.
DISCUSSION
In PRRT, the goal is to deliver an effective radiation dose to the tumor without causing undesired effects on healthy tissues. Improvements in the success of radionuclide therapy depend on optimization of the radiation dose to the tumor versus the dose to normal organs in individual patients. This requires application of dosimetry models suitable for estimating the radiation dose.
When radiolabeled somatostatin analogs are used for PRRT, nephrotoxicity is an important risk. Renal toxicity can be diminished by infusing amino acids for renal protection and by applying individual dosimetry to prevent the absorbed dose from exceeding the maximum tolerated by the kidneys (23–27 Gy). Nevertheless, the radiation dose that can be administered safely to the kidneys during radionuclide therapy remains to be established and might depend on the radionuclide used for PRRT. Renal toxicity after PRRT has been described in a few patients from phase II studies using [90Y-DOTA,Tyr3]octreotide. Otte et al. (13) reported on 4 patients in whom renal toxicity developed. These 4 patients received more than 7.4 GBq/m2 but no amino acid solution for renal protection. Two of these patients showed stable renal insufficiency, and 2 required hemodialysis. Paganelli et al. (14) reported on 1 patient who, after receiving 3.3 GBq of octreotide, experienced delayed grade II kidney toxicity. Kwekkeboom et al. (11) reported on 1 patient whose kidney function was already compromised at the start of therapy and who had renal insufficiency 1 y after treatment with 29.6 GBq [177Lu-DOTA,Tyr3]octreotate.
Because current SPECT scanners have a spatial resolution of more than 1 cm (Fig. 1), accurate measurement of regional differences in radioactivity within the cortex and separation of radioactivity in the medulla from radioactivity in the cortex is not possible. However, using ex vivo autoradiography after injection of [111In-DTPA]octreotide, we could show that distribution of radioactivity in the human renal cortex and medulla was not uniform. Different parts of the kidney will thus receive radiation doses that differ tremendously from each other and from the calculated average dose to the whole kidney. The glomeruli, which form radiation-sensitive functional units for late radiation damage, are not evenly distributed over the cortex in human kidneys; most (about 85%) of the glomeruli are in the outer cortical regions. Based on our findings, with the greatest part of the radioactivity in the inner cortical zone, different effects due to this inhomogeneity can be expected from PRRT using radionuclides emitting particles with short ranges, such as Auger electron emitters, α-emitters, and low-energy β-emitters. These radionuclides will minimize the dose to the sensitive glomeruli in the outer renal cortex. Accordantly, renal toxicity after PRRT was found most often in studies using the long-ranged 90Y-labeled peptide (13,14), whereas studies using octreotide labeled with short-ranged 111In found no renal toxicity, even though estimated radiation doses to the kidneys could be as high as 40 Gy (15). These clinical sparing effects in the kidney remain, however, to be further investigated.
We will soon perform ex vivo autoradiography studies using renal tissue from more patients and, if available, from larger parts of the kidney, to build a model of the 3-dimensional location of radioactivity and to calculate the dosimetric consequences thereof. Furthermore, we will perform immunohistochemistry tests on adjacent sections to determine the exact histologic localization of the radioactivity in the human kidney.
CONCLUSION
After injection of [111In-DTPA]octreotide, radioactivity is retained predominantly, but not exclusively, in the renal cortex, leading to different radiation doses to different parts of the kidney.
Footnotes
Received Oct. 31, 2003; revision accepted Jan. 21, 2004.
For correspondence or reprints contact: Marion de Jong, PhD, Department of Nuclear Medicine, Erasmus MC, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: m.hendriks-dejong{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Beyond Average: {alpha}-Particle Distribution and Dose Heterogeneity in Bone Metastatic Prostate Cancer
- Toward a Patient-Specific Traceable Quantification of SPECT/CT-Based Radiopharmaceutical Distributions
- What You See Is Not What You Get: On the Accuracy of Voxel-Based Dosimetry in Molecular Radiotherapy
- 4-Step Renal Dosimetry Dependent on Cortex Geometry Applied to 90Y Peptide Receptor Radiotherapy: Evaluation Using a Fillable Kidney Phantom Imaged by 90Y PET
- Nephrotoxicity in Mice After Repeated Imaging Using 111In-Labeled Peptides
- MIRD Pamphlet No. 20: The Effect of Model Assumptions on Kidney Dosimetry and Response--Implications for Radionuclide Therapy
- Reconstruction Parameters for 111In-Pentetreotide SPECT: Variability with Respect to Body Weight and Body Region
- Radiation Dose Distribution in Human Kidneys by Octreotides in Peptide Receptor Radionuclide Therapy
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- 18F-Labeled Bombesin Analogs for Targeting GRP Receptor-Expressing Prostate Cancer
- Oral Versus Intravenous Administration of Lysine: Equal Effectiveness in Reduction of Renal Uptake of [111In-DTPA]Octreotide
- Megalin Is Essential for Renal Proximal Tubule Reabsorption of 111In-DTPA-Octreotide
- Patient-Specific Dosimetry in Predicting Renal Toxicity with 90Y-DOTATOC: Relevance of Kidney Volume and Dose Rate in Finding a Dose-Effect Relationship
- Practical Dosimetry of Peptide Receptor Radionuclide Therapy with 90Y-Labeled Somatostatin Analogs
- Improving Insight into Radiobiology and Radionuclide Therapy