


Abstract
Conventional myocardial perfusion PET tracers require onsite tracer production because of their short radioactive half-lives. To investigate the potential of a new 18F-labeled pyridazinone analog (18F-BMS-747158-02), we characterized this tracer in a rat model of permanent and transient coronary occlusion using small-animal PET. Methods: Myocardial 18F-BMS-747158-02 distribution in healthy rats (n = 7), rats with transient (3-min) left coronary artery occlusion (n = 11), and rats with permanent left coronary occlusion (n = 11) was analyzed with a dedicated small-animal PET scanner. Results: Normal hearts demonstrated intense and almost homogeneous tracer uptake throughout the left ventricle for more than 2 h. During permanent coronary occlusion, PET demonstrated perfusion defects, which remained unchanged (37.6% ± 8.8%, 37.4% ± 10.2%, and 36.2% ± 9.8% left ventricle at 15, 45, and 115 min, respectively, after tracer injection). After transient ischemia, the induced defect size decreased significantly after reperfusion (16.2% ± 9.3%, 6.0% ± 6.5%, and 1.4% ± 1.3% left ventricle). Tracer reinjection after transient ischemia resulted in normalization of the induced defect. Conclusion: Coronary occlusion yielded distinct myocardial 18F-BMS-747158-02 uptake defects in the area of ischemia, which demonstrated normalization of activity after reperfusion and reinjection. These promising kinetic parameters may allow for assessment of flow using exercise–rest protocols similar to those used in combination with exercise and rest perfusion SPECT.
Myocardial exercise–rest perfusion imaging using SPECT with 201Tl, 99mTc-sestamibi, or 99mTc-tetrofosmine is widely applied for clinically diagnosing and determining the prognosis of ischemic heart disease (1). However, false-positive findings caused by attenuation artifacts and underestimation of absolute perfusion abnormalities in patients with balanced 3-vessel disease are well-known limitations of the method (2). Moreover, the recent development of angiogenic therapies may require high-sensitivity, high-resolution imaging for monitoring changes in perfusion more subtle than those that occur with conventional therapies (3).
PET can overcome some limitations of SPECT by providing better temporal and spatial resolution, greater sensitivity, and established algorithms for attenuation correction (4,5). There are 3 well-established tracers for myocardial PET perfusion imaging: 82Rb, 13N-ammonia, and 15O-water. These tracers have short radioactive half-lives of 76 s, 10 min, and 2.1 min, respectively. 82Rb is produced by a radionuclide generator system, whereas production of 13N-ammonia and 15O-water require an expensive on-site cyclotron. In addition, the short radioactive half-life requires imaging protocols with tracer injections while the patient is on the scanner. These temporal limitations make it difficult to perform the exercise stress examinations commonly used in SPECT myocardial perfusion imaging.
18F-labeled perfusion PET tracers, including 18F-BMS-747158-02, for the evaluation of myocardial perfusion have recently been introduced (6–10). 18F-labeled tracers with radioactive half-lives of 110 min overcome the half-life limitations of previously used PET perfusion tracers. Such tracers may be distributed by a central cyclotron facility in a manner similar to 18F-FDG. Moreover, 18F provides better image quality and spatial resolution because it emits a lower-energy positron that travels a shorter distance in tissue before annihilation (11,12). Initial reports of 18F-BMS-747158-02 showed the compound to have promising properties as a new myocardial perfusion tracer, such as a specific, high myocardial extraction fraction and retention at different flow rates in rat and rabbit models (8–10). However, whether the kinetics of 18F-BMS-747158-02 in normally perfused and transiently ischemic myocardium reflect suitability for clinical stress perfusion studies remains unknown. In this study, we aimed to further explore the potential clinical application of the novel PET tracer 18F-BMS-747158-02 for the diagnosis of coronary artery disease using permanent and transient coronary occlusion in rats and imaging with small-animal PET.
MATERIALS AND METHODS
18F-BMS-747158-02 was characterized using a small-animal PET system and rat models. 18F-BMS-747158-02 uptake in the myocardium of healthy rats was assessed. For comparison, 13N-ammonia uptake in other healthy rats was studied. Furthermore, myocardial 18F-BMS-747158-02 uptake and time-dependent changes in tracer distribution were assessed in rats with permanent or transient coronary occlusion. One rat was studied with 13N-ammonia PET and 18F-BMS-747158-02 PET 1 wk after permanent coronary artery occlusion.
Experimental protocols were approved by the regional governmental commission of animal protection (Regierung von Oberbayern, Germany) and conformed with the guidelines of the U.S. National Institutes of Health (13).
Animal Preparation
Male Wistar rats weighing 250–300 g were used in all experiments. Healthy rats (n = 7), rats with permanent left coronary artery (LCA) occlusion (n = 11), and rats with transient LCA occlusion (n = 11) were studied (Fig. 1). Before the intervention, the rats were anesthetized with intramuscularly administered midazolam (0.1 mg/kg), fentanyl (1 μg/kg), and medetomidine (10 μg/kg). The rats were mechanically ventilated and underwent thoracotomy.

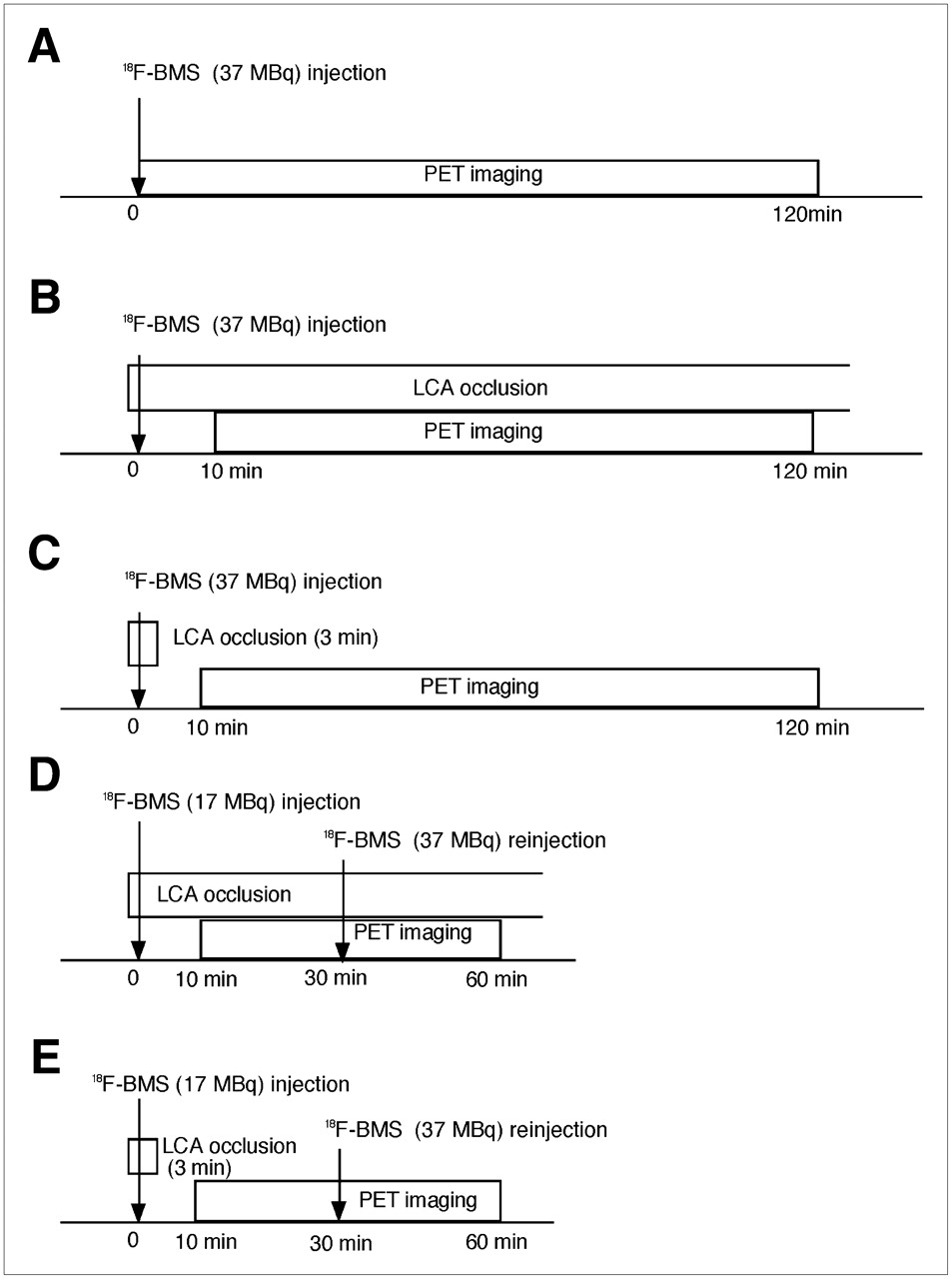
Schemas of experimental protocols of permanent and transient coronary occlusion and imaging: normal heart (A), permanent LCA occlusion (B), transient LCA occlusion (C), reinjection after permanent LCA occlusion (D), and reinjection after transient LCA occlusion (E). 18F-BMS = 18F-BMS-747158-02.
In rats with permanent LCA occlusion, a 7–0 polypropylene suture on a small, curved needle was passed through the myocardium beneath the LCA and ligated to occlude the LCA (14). Coronary occlusion was confirmed by the regional cyanosis of the myocardial surface.
In the animals with transient LCA occlusion, the suture was passed through the myocardium beneath the LCA. Subsequently, both suture ends were passed through a small vinyl tube to make a snare. The suture material was pulled tightly against the vinyl tube to occlude the LCA. After a 3-min occlusion, reperfusion was obtained by release of the snare and confirmed by a myocardial blush over the area at risk (15). After the surgery, the chest was closed, and the rats were moved to the PET scanner.
18F-BMS-747158-02 PET Protocols
Five series of experiments (protocols A–E) were performed (Fig. 1).
Protocol A was designed to address the myocardial distribution of 18F-BMS-747158-02 in normal rats over 120 min after tracer injection (n = 5). Thirty-seven megabecquerels of 18F-BMS-747158-02 were injected into the tail vein just before the start of PET data acquisition.
Protocol B evaluated the effect of coronary occlusion. The rats were injected with 18F-BMS-747158-02 (37 MBq) 1 min after permanent occlusion of the LCA and imaged from 10 to 120 min after tracer injection (n = 5).
Protocol C was designed to analyze the tracer redistribution in a reperfusion model. The LCA was occluded for a period of 3 min, and 37 MBq of 118F-BMS-747158-02 were injected 1 min after occlusion of the LCA. Image acquisition continued from 10 to 120 min after tracer injection (n = 5).
Protocols D and E were designed to investigate the effects of tracer reinjection on the cardiac tracer distribution in permanent (D) (n = 6) or transient (E) (n = 6) coronary occlusion. In both protocols, 18F-BMS-747158-02 was injected as described in protocols B and C at 10 min before the start of image acquisition (17 MBq) and 30 min after the start of image acquisition (37 MBq), which continued for 60 min.
13N-Ammonia PET of Healthy Rats and Coronary Occlusion Model
13N-ammonia PET was performed on 8 healthy rats. 13N-ammonia (55 MBq) was injected, and data were acquired from 5 to 15 min after tracer injection.
One rat was imaged 1 wk after permanent occlusion of the LCA with both 13N-ammonia and 18F-BMS-747158-02 PET. Imaging was performed for 10 min after a 5-min delay after injection of 55 MBq of 13N-ammonia. After a delay of 40 min to allow for radioactive decay, 37 MBq of 18F-BMS-747158-02 were administered, and a 10-min PET acquisition was performed.
PET Acquisition and Reconstruction
All PET was performed with the animals prone. A dedicated small-animal PET scanner was used (microPET Focus 120; Siemens Medical Solutions). Data were acquired in list-mode format and reconstructed into a dynamic image with 10-min frames for 18F-BMS-747158-02 PET and a single frame for 13N-ammonia PET.
The reconstruction was done using filtered backprojection with a cutoff at the Nyquist frequency, and the resulting images had 128 × 128 × 95 voxels with a voxel size of 0.43 × 0.43 × 0.80 mm. Data were normalized and corrected for randoms, dead time, and decay.
Data Analysis
The PET images were analyzed with the ASIPro software package (Siemens Medical Solutions) and the Munich Heart software package (14,16).
Regions of interests were manually defined in a mid coronal slice at the heart (anterior wall) and in the blood pool (left ventricle), lung (right), and liver using ASIPro software. Percentages of injected dose/cm3 of tissue in the heart region of interest and the ratio of tracer activity between the heart and other organs were calculated.
Volumetric sampling was applied to delineate 3-dimensional tracer distributions throughout the left ventricular myocardium, and tracer concentrations at each sampling point were displayed in a polar map using Munich Heart software (14,16). Mean percentage uptake (expressed as a percentage of maximal uptake) was calculated for 5 segments in normal rat hearts. Tracer-uptake defects were characterized as having less than 50% activity when compared with the point of maximum activity in the myocardium. The mean percentage uptakes and regional defects were evaluated at 15, 45, and 115 min after tracer injection.
Statistical Analysis
All results were expressed as mean ± SD. Statistical analysis was done with StatMate III (ATMS Co., Ltd.). Uptake ratio was compared between 2 groups by means of the Mann–Whitney test. Differences between group comparisons were identified using ANOVA followed by the Scheffé multiple-contrast hypothesis test. A value of P less than 0.05 was considered statistically significant.
RESULTS
18F-BMS-747158-02 Distribution in Normal Rat Hearts
Figure 2 demonstrates in vivo analysis of 18F-BMS-747158-02 uptake in healthy rats. The left ventricular myocardium showed excellent contrast to surrounding tissues in all rats. High tracer accumulation was preserved in the myocardium throughout the imaging period of 2 h (percentage injected dose [%ID]/cm3 > 2.0 from 15 to 115 min), with a slight decrease from 30 min (Fig. 2C). The half-life of myocardial tracer activity on PET images was calculated as 265 min using linear fitting of the time–activity curve from 25 to 115 min (y = −0.0048x + 2.53, r = 0.965; y = tracer activity [%ID/cm3], x = time after tracer injection [min]). Time-dependent changes in tracer distribution in the heart and other organs were observed. Heart-to-lung ratio and heart–to–left ventricle blood-pool ratio decreased over time (heart-to-lung ratio from 14.6 ± 3.10 at 15 min to 8.70 ± 2.4 at 115 min; heart–to–left ventricle blood pool ratio from 3.47 ± 0.76 at 15 min to 2.83 ± 0.54 at 115 min) and heart-to-liver ratio increased (from 2.07 ± 0.80 at 15 min to 2.82 ± 0.39 at 115 min) (Figs. 2A and 2B). These ratios, when compared with 13N-ammonia (heart-to-lung, 3.60 ± 0.80; heart-to-liver, 1.05 ± 0.49; heart–to–left ventricle blood pool, 2.08 ± 0.16), show significantly improved myocardium-to-tissue contrast (Figs. 2A and 2D).
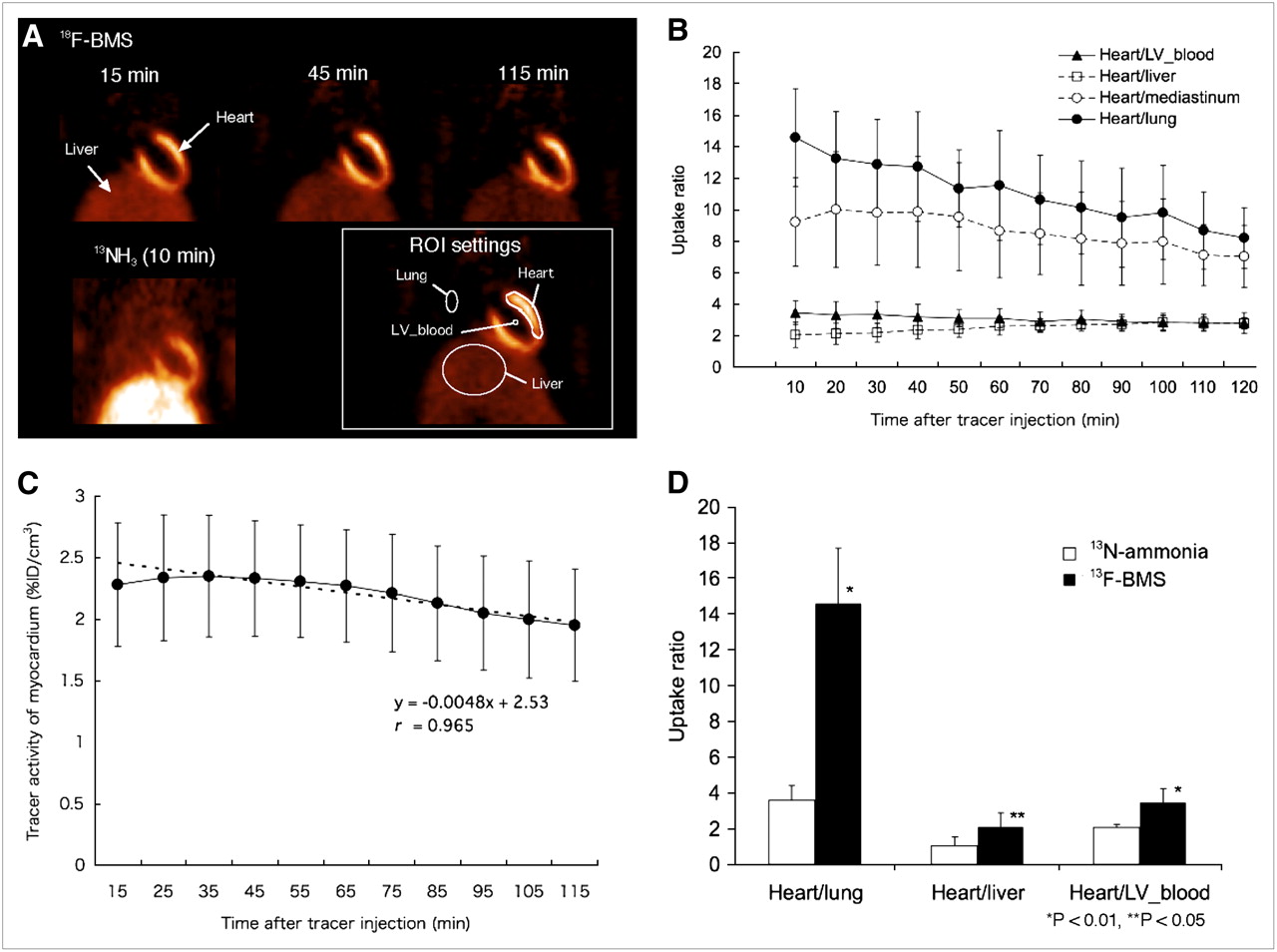
(A) Examples of 18F-BMS-747158-02 (18F-BMS) PET images of chest of healthy rat at 15, 45, and 115 min after tracer injection and 13N-ammonia PET image at 10 min in coronal view. Example of regions of interest for measurement of tracer activity is displayed in white box. (B and C) Ratio of 18F-BMS uptake between myocardium and surrounding organs (B) and absolute 18F-BMS activity of myocardium (%ID/cm3) (C). (D) Comparison of 18F-BMS uptake ratios at 15 min after injection and 13N-ammonia at 10 min.
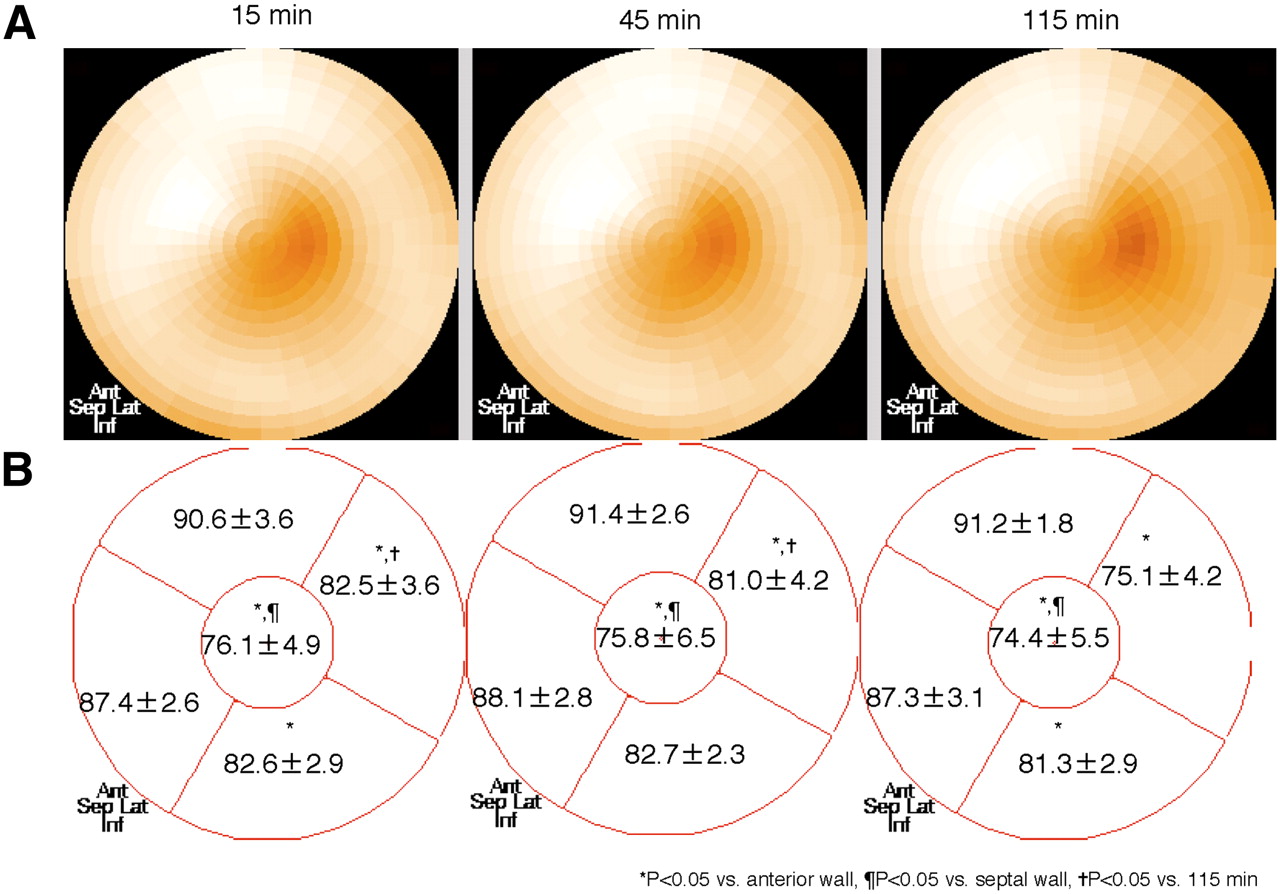
18F-BMS-747158-02 uptake in the myocardium was almost homogeneous throughout the left ventricle. However, small differences were observed, with the lowest uptake in apical segments, when compared with anterior, septal, inferior, and lateral areas at 15, 45, and 115 min after tracer injection. Small (approximately 5%) but significant differences in tracer distribution were found in the lateral wall at 115 min, as compared with 15 and 45 min (Fig. 3).
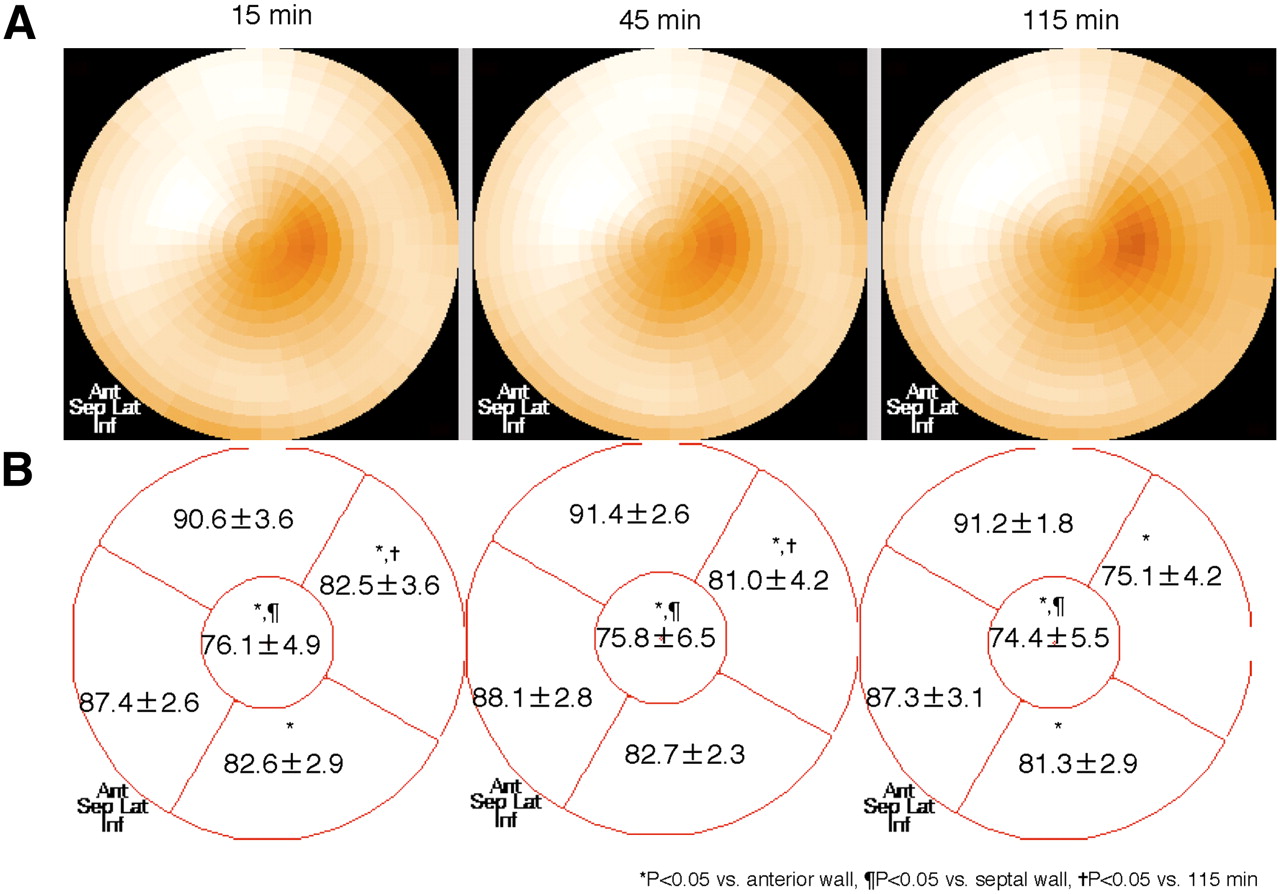
Normal pattern of left ventricular 18F-BMS-747158-02 (18F-BMS) distribution at 15, 45, and 115 min after tracer injection as shown in mean polar maps (A) and as mean uptake values (% left ventricle maximum) with SD (B). Uptake was nearly homogeneous throughout left ventricle, with slightly lower uptake in apical segment.
18F-BMS-747158-02 Uptake in LCA Occlusion
18F-BMS-747158-02 PET images demonstrated a defect in the myocardium of all rats with LCA occlusion at 15 min after tracer injection. As shown in Figure 4, the induced 18F-BMS-747158-02 uptake defect visualized at 15 min corresponded precisely to the defect in 13N-ammonia images. Images obtained using 18F-BMS-747158-02 demonstrated improved contrast and higher resolution resulting in better delineation of induced lesions, despite a higher injected dose of 13N-ammonia (57 MBq) versus 18F-BMS-747158-02 (37 MBq).

Short-axis images of rat heart 1 wk after coronary occlusion using 18F-BMS-747158-02 (18F-BMS) PET and 13N-ammonia PET. Arrows indicate localization of myocardial infarction.
18F-BMS-747158-02 Redistribution After Reperfusion
The defect size induced by permanent LCA occlusion did not change over 2 h (37.6% ± 8.8% left ventricle at 15 min, 37.4% ± 10.2% left ventricle at 45 min, and 36.2% ± 9.8% left ventricle at 115 min). The tracer activity (%ID/cm3) in normal myocardium and the induced defect were also constant throughout the imaging period. In contrast, tracer redistributed in the induced defect after reperfusion after 3 min of coronary occlusion (Fig. 5). A significant reduction (P < 0.01) in perfusion defect size occurred after reperfusion (16.2% ± 9.3% left ventricle at 15 min, 6.0% ± 6.5% left ventricle at 45 min, and 1.4% ± 1.3% left ventricle at 115 min). Tracer activity in the defect increased over time after reperfusion, whereas the activity of normally perfused myocardium remained constant. In rats with transient LCA occlusion (3 min) and reperfusion, the activity within the defect approached normal myocardial activity at 115 min after tracer injection (Fig. 6).

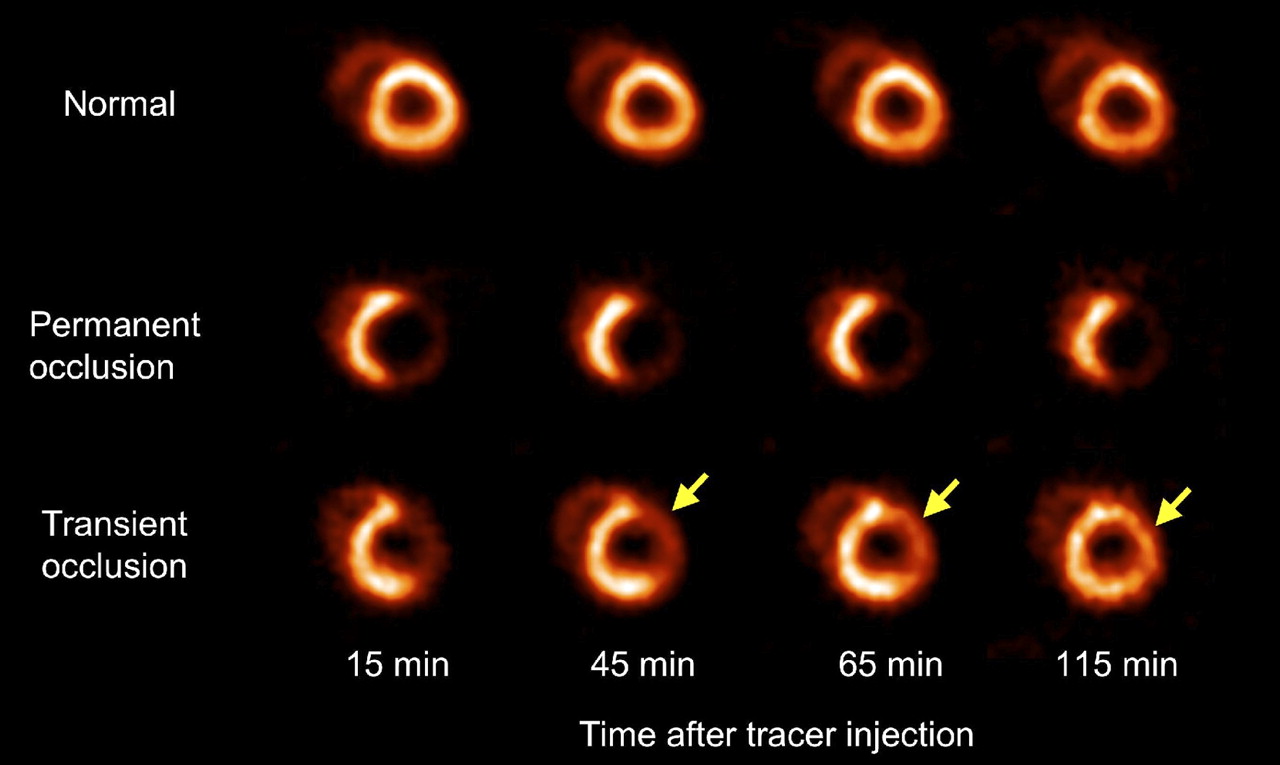
Representative short-axis images of rat hearts without coronary occlusion, permanent coronary occlusion, and transient coronary occlusion at different time points after tracer administration. Tracer redistribution is seen in induced defect after reperfusion (arrows).
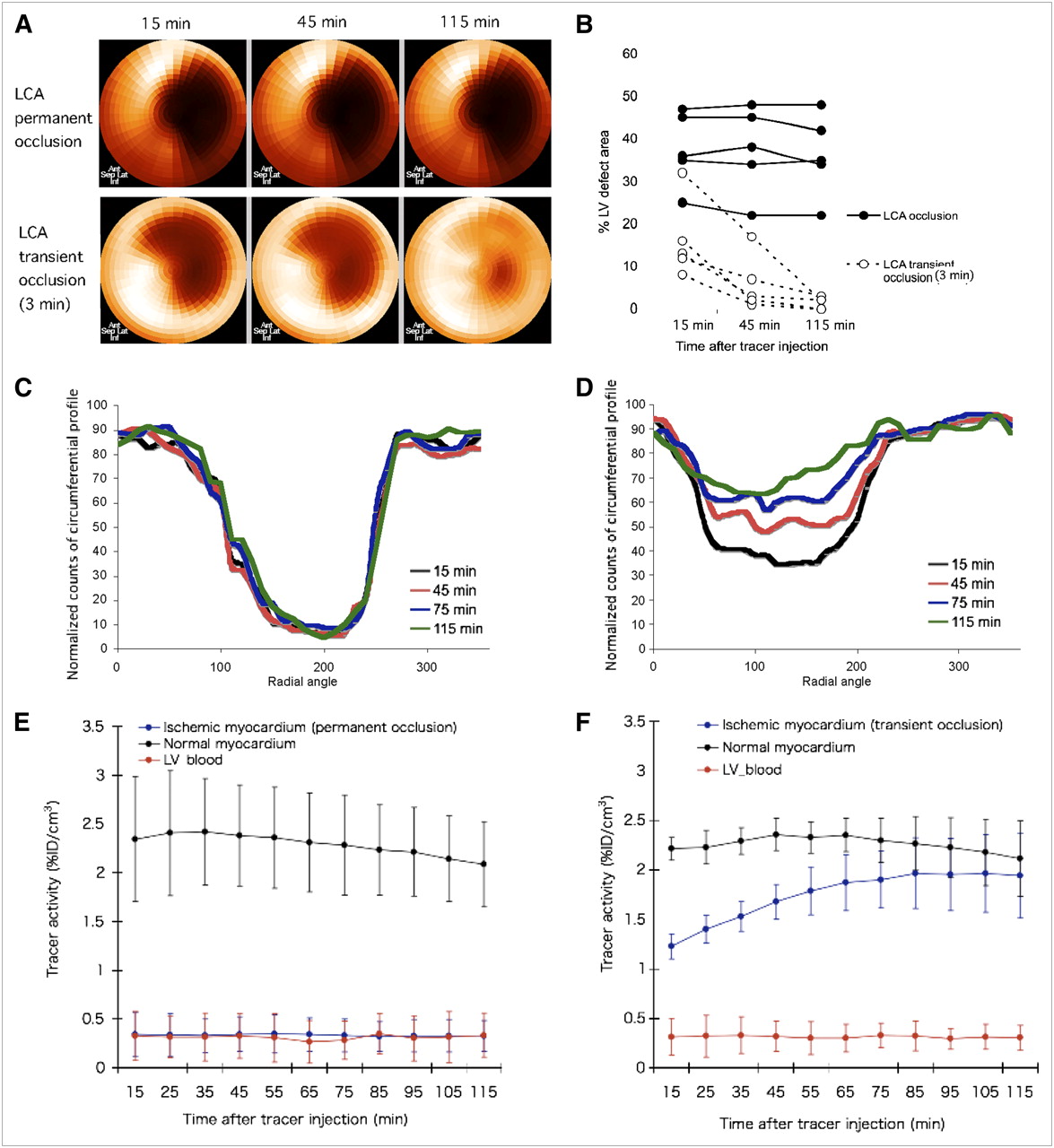
Changes in myocardial 18F-BMS-747158-02 (18F-BMS) distribution after both permanent and transient coronary occlusion are shown in representative polar maps (A) and as defect area expressed as percentage of total left ventricular myocardium (B). Normalized counts of circumferential profiles after permanent occlusion (C) or transient occlusion (D) are also shown. Mean values are shown for tracer activity in induced defect and normally perfused myocardium after permanent (E) and transient occlusion (F). Tracer activity in defect increased over time after reperfusion in transient coronary occlusion.
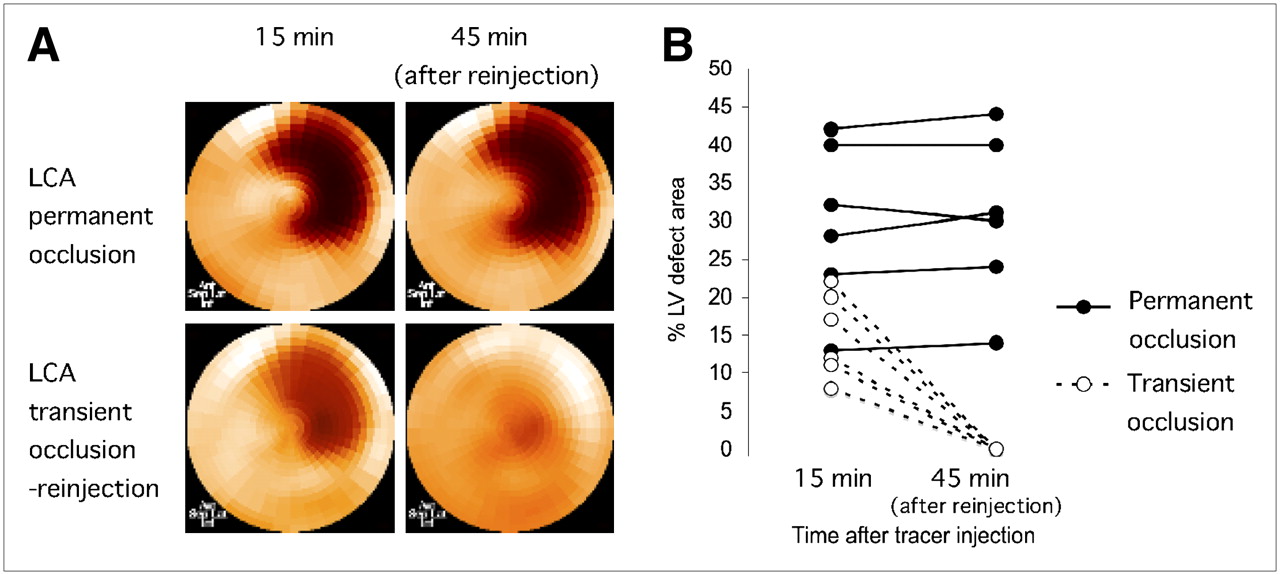
Tracer reinjection did not change the defect size (29.7% ± 10.8% at 15 min, 30.5% ± 10.8% after reinjection) in animals with permanent LCA occlusion. In contrast, rats with transient LCA occlusion demonstrated resolution of the induced defect, with increased tracer activity after reinjection (defect size: 15.0% ± 5.5% at 15 min, 0% ± 0% after reinjection) (Fig. 7). The defect took 2 h to disappear without reinjection (protocol C), but tracer reinjection enhanced the normalization process, which became apparent rapidly after reinjection in the transient LCA occlusion model (protocol E).

Myocardial 18F-BMS-747158-02 (18F-BMS) distribution patterns before and after tracer reinjection in rats after permanent and transient coronary occlusion. Representative polar maps (A) and plots of defect area (B) are shown. Tracer uptake defects resolved after tracer reinjection in rats after transient coronary occlusion but not in permanent coronary occlusion.
DISCUSSION
The results of this study indicate promising properties for 18F-BMS-747158-02 as a novel 18F-labeled PET tracer for the diagnosis and evaluation of coronary artery disease. In the normal rat heart, tracer uptake in the left ventricular wall shows high contrast to surrounding tissue and high myocardial retention throughout the imaging period of 2 h. This finding confirms the previously reported high first-pass extraction and high myocardial retention in isolated perfused rat hearts (10). The high contrast ratio between myocardial and hepatic tissue represents a favorable feature for the evaluation of the inferior wall of the left ventricle, as compared with 13N-ammonia. In animals with coronary occlusion, the induced defect was clearly delineated and remained unchanged over the entire imaging protocol. In contrast, reperfusion after short, transient ischemia (3 min) yielded tracer redistribution to the induced defect. Tracer reinjection further enhanced the normalization process. The clinical application of this tracer for the diagnosis of coronary artery disease and for the assessment of tissue viability may involve tracer injection under physical stress conditions with early and late imaging studies.
PET has been proven to be a reliable and efficient technique to assess myocardial perfusion in patients with known or suspected coronary artery disease (17,18). Recently, Bateman et al. compared the diagnostic accuracy of rest/pharmacologic stress perfusion with 99mTc-sestamibi SPECT and 82Rb PET in matched patient populations (5). The results demonstrated higher overall accuracy for PET (89%) than for SPECT (79%), based on an angiographic criterion of more than 70% coronary stenosis. In patients with multivessel coronary disease, PET identified more defects than did SPECT (71% vs. 48%).
Conventional PET perfusion tracers such as 3N-ammonia, 15O-water, or 82Rb have short physical half-lives, which allow repeated studies after decay. A pharmacologic stress protocol is commonly used for conventional PET perfusion studies because of technical limitations in performing exercise stress testing with short-lived isotopes. On the other hand, exercise stress testing is often preferred for SPECT perfusion imaging because it offers important clinical and hemodynamic information in addition to myocardial perfusion. Recently, Chow et al. compared treadmill exercise and dipyridamole stress using 13N-ammonia perfusion PET (19). They found larger and more severe perfusion defects with physical exercise than with dipyridamole, indicating that exercise may offer diagnostic advantages for 13N-ammonia perfusion imaging. Because of the longer half-life of 18F, 18F-labeled perfusion tracers can potentially be used in exercise stress testing by injection of tracer during peak exercise and postinjection imaging. However, the longer half-life also limits the use of tracer in protocols involving repeated measurements on a single day. Therefore, protocols involving stress and rest studies on separate days, or validation of a tracer reinjection protocol, are required. In addition, an increased radiation dose should be considered when determining the injection dose of the tracer.
The chemical structure of BMS-747158-02, a modification of the pyridazinone insecticide pyidaben, was described in previous publications (8–10). These compounds are known to bind tightly to mitochondrial complex I, with high affinity in myocardial tissue (8,9,20). Observed highly selective myocardial tracer uptake may be explained partly by the high content of mitochondria in the left ventricular myocardium. Given the high extraction fraction, which appeared to be flow-independent as measured in isolated rat hearts (10), 18F-BMS-747158-02 uptake is most likely to reflect blood flow. The feasibility of quantification requires confirmation in large-animal models using microsphere reference measurements. In addition, the influence of hypoxia on tracer retention, which may cause changes in mitochondrial structure and function, have not been addressed. Similar observations have been reported for 99mTc-sestamibi but have not affected its clinical application (21,22).
Redistribution is an advantage of 201Tl SPECT tracer kinetics that is not shared by 99mTc perfusion SPECT tracers for the assessment of myocardial viability using stress/rest redistribution protocols. Experimental studies after coronary occlusion and reperfusion in dogs showed in the induced defect an increase in relative 201Tl activity (23) caused by the differential washout rates in normal and postischemic myocardium. Faster 201Tl washout in normal myocardium results in a decrease in defect size based on the evaluation of relative myocardial tracer distributions.
We observed tracer redistribution with 18F-BMS-747158-02 after reperfusion. In contrast to 201Tl kinetics, we found time-dependent increases in tracer activity in the induced defect whereas the activity remained constant in normally perfused myocardium. High extraction fraction and minimal washout of the tracer from myocardium were demonstrated in isolated perfused rat heart (10). Therefore, after initial tracer uptake, tracer washout from extracardiac organs, as well as some recirculation within the myocardium, may be possible sources of the increased activity. Although the mechanism of redistribution may differ from that of 201Tl redistribution, the observed kinetics may allow for a clinical protocol in the diagnosis of coronary artery disease similar to conventional stress/rest 201Tl perfusion imaging. However, the kinetics observed in rat heart may not directly apply to other species, including humans. Future studies on other species are required to confirm the redistribution and to define the optimal time window between tracer injection and imaging to maintain a high sensitivity for detection of perfusion abnormalities.
CONCLUSION
We found that cardiac accumulation of 18F-BMS-747158-02 in normal rat hearts was rapid, relatively homogeneous, high, and persisted over 2 h. Additionally, transient coronary occlusion demonstrated well-delineated defects in tracer uptake followed by tracer redistribution after reperfusion. These results indicate that this 18F-labeled compound may be an excellent candidate in the assessment of myocardial perfusion using PET and conventional physical exercise stress protocols, which are currently used in tandem with SPECT.
Acknowledgments
We are grateful to Antti Sarastie and Som Javadi for their careful editorial assistance. This study was supported by a research grant from Bristol-Myers Squibb Medical Imaging. Ming Yu, David S. Casebier, and Simon P. Robinson are employees of Bristol-Myers Squibb Medical Imaging.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 29, 2008.
- Accepted for publication June 24, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Assessment of the 18F-Labeled PET Tracer LMI1195 for Imaging Norepinephrine Handling in Rat Hearts
- Myocardial Uptake of 7'-(Z)-[123I]Iodorotenone During Vasodilator Stress in Dogs With Critical Coronary Stenoses
- Stable Delineation of the Ischemic Area by the PET Perfusion Tracer 18F-Fluorobenzyl Triphenyl Phosphonium After Transient Coronary Occlusion
- Radionuclide Imaging of Angiotensin II Type 1 Receptor Upregulation After Myocardial Ischemia-Reperfusion Injury
- Evaluation of the Novel Myocardial Perfusion Positron-Emission Tomography Tracer 18F-BMS-747158-02: Comparison to 13N-Ammonia and Validation With Microspheres in a Pig Model
- Evaluation of a Novel 18F-Labeled Positron-Emission Tomography Perfusion Tracer for the Assessment of Myocardial Infarct Size in Rats