


Abstract
18F-fluorobenzyl triphenyl phosphonium (FBnTP) has recently been introduced as a myocardial perfusion PET agent. We used a rat model of transient coronary occlusion to determine the stability of the perfusion defect size over time and the magnitude of redistribution. Methods: Wistar rats (n = 15) underwent thoracotomy and 2-min occlusion of the left coronary artery (LCA), followed by reperfusion. During occlusion, 18F-FBnTP (92.5 MBq) and 201Tl-thallium chloride (0.74 MBq) were injected intravenously. One minute before the animals were sacrificed at 5, 45, and 120 min after reperfusion, the LCA was occluded again and 2% Evans blue was injected intravenously to determine the ischemic territory. The hearts were excised, frozen, and sliced for serial dual-tracer autoradiography and histology. Dynamic in vivo 18F-FBnTP PET was performed on a subgroup of animals (n = 4). Results: 18F-FBnTP showed stable ischemic defects at all time points after tracer injection and reperfusion. The defects matched the blue dye defect (y = 0.97x+1.5, R2 = 0.94, y = blue-dye defect, x = 18F-FBnTP defect). Count density analysis showed no defect fill-in at 45 min but slightly increased activity at 120 min (LCA/remote uptake ratio = 0.19 ± 0.02, 0.19 ± 0.05, and 0.34 ± 0.06 at 5, 45, and 120 min, respectively, P < 0.05). For comparison, 201Tl showed complete redistribution at 120 min (LCA/remote = 0.42 ± 0.04, 0.72 ± 0.03, and 0.97 ± 0.05 at 5, 45, and 120 min, respectively, P < 0.001). Persistence of the 18F-FBnTP defect over time was confirmed by in vivo dynamic small-animal PET. Conclusion: In a transient coronary occlusion model, perfusion defect size using the new PET agent 18F-FBnTP remained stable for at least 45 min and matched the histologically defined ischemic area. This lack of significant redistribution suggests a sufficient time window for future clinical protocols with tracer injection remote from the scanner, such as in a stress testing laboratory or chest pain unit.
PET myocardial perfusion imaging is increasingly entering the clinical arena as a highly accurate technique for the workup of coronary artery disease (1,2). When compared with standard SPECT, it provides better temporal and spatial resolution, higher sensitivity for tracer detection, and robust correction of attenuation artifacts (3,4). The currently established PET myocardial perfusion tracers include 82Rb-rubidium chloride, 13N-ammonia, and 15O-water, but their short radioactive half-lives (76 s, 10 min, and 2.1 min, respectively) require expensive on-site production by a cyclotron or commitment to a dedicated generator. Additionally, a physical-exercise stress test is not practical because of the rapid decay of these tracers.
18F-fluorobenzyl triphenyl phosphonium (FBnTP) is one of several recently introduced 18F-labeled perfusion tracers. It is a cation with a mechanism of uptake similar to 99mTc-tetrofosmin and 99mTc-sestamibi and has shown promising properties such as high cardiac uptake and retention in animal models (5–8). Because of the 110-min half-life of 18F, 18F-FBnTP may help to overcome the limitations caused by the rapid decay of currently used perfusion PET tracers. Stress protocols using physical exercise may be feasible. However, stable uptake and a lack of early washout and redistribution would be necessary to allow sufficient time for the patient to be moved from the treadmill to the camera for imaging.
Accordingly, in this study we investigated the stability of 18F-FBnTP uptake and the presence of washout and redistribution. For this investigation, we tested the tracer in a rat model of transient coronary occlusion.
MATERIALS AND METHODS
Animal Model
Fifteen Wistar rats were used in this investigation. The experimental protocol was approved by the Institutional Animal Care and Use Committee and conformed to the Guide for the Care and Use of Laboratory Animals (9).
Anesthesia was induced before the intervention and maintained during it using 1%–3% isoflurane and mechanical ventilation. Left thoracotomy was performed to expose the heart. A 7-0 polypropylene suture on a small curved needle was passed through the myocardium beneath the proximal portion of the left coronary artery (LCA). Both ends of the suture were passed through a small vinyl tube to produce a snare. Then, the LCA was occluded for 2 min by pulling both ends of the suture against the vinyl tube to tighten the snare (10–12). Tracer was injected via a tail vein during the coronary occlusion. Reperfusion was then obtained by release of the snare. The success of coronary occlusion and reperfusion was confirmed by visual identification of regional cyanosis of the myocardial surface in the risk area, followed by a blush. The short phase of ischemia was tolerated well by all animals.
Dual-Tracer Autoradiography
Dual-tracer autoradiography was performed to compare 18F-FBnTP uptake and 201Tl uptake at various times after transient ischemia. The experimental protocol is depicted in Figure 1A. Immediately after LCA occlusion, 92.5 MBq of 18F-FBnTP, which was produced as previously described (13), and 0.74 MBq of 201Tl-thallium chloride were injected via a tail vein (14). Two minutes after injection of the tracers during coronary occlusion, reperfusion was achieved. Groups of animals were studied at 5 min (n = 3), 45 min (n = 4), and 120 min (n = 4) after reperfusion. To determine the ischemic myocardial territory histologically, the LCA was occluded again using the same snare (which was left on the heart after the initial LCA occlusion), and 2 mL of Evans blue dye (2%) were injected via the tail vein just afterward. The rat was euthanized 1 min after the dye was injected. Then, the heart was removed, sliced into 20-μm short-axis sections, and placed on autoradiography plates (Multi Sensitive Phosphor Screens; Perkin Elmer). The first exposure began immediately and continued for 45 min in order to visualize 18F-radioactivity. Three days later, after decay of 18F, a second exposure was performed for 4 d to image the lower dose of 201Tl (12,14). Additionally, photographs were taken of blue-dye–stained short-axis slices.
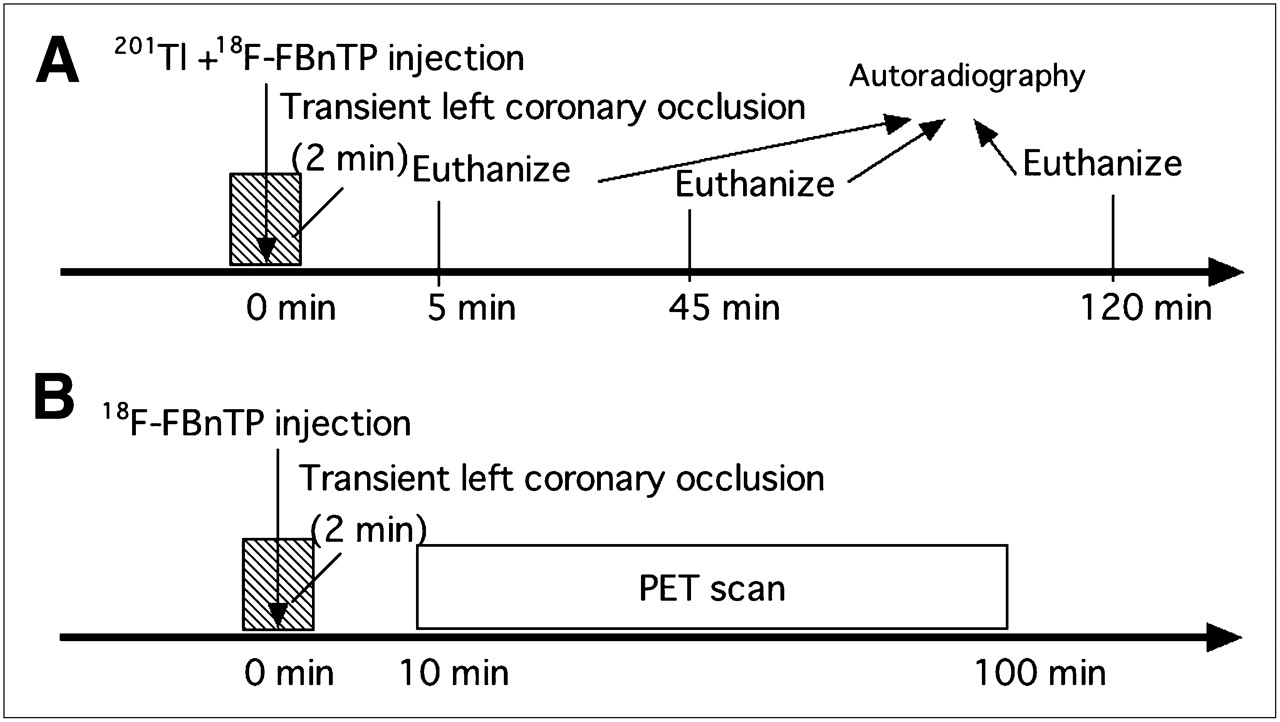
Schematic diagram of study protocols for dual-tracer autoradiography (A) and in vivo PET (B) in rat model of transient coronary occlusion.
Images of blue-dye–stained short-axis slices were displayed side by side with autoradiographs of 18F-FBnTP and 201Tl. Region-of-interest analysis was used to determine the ratio of remote radioactivity to defect radioactivity at all time points for both tracers. Additionally, with ImageJ software (National Institutes of Health), defect size was measured planimetrically in 4 continuous slices and expressed as a percentage of the entire myocardial circumference. The 18F-FBnTP defect was compared with the unstained area on blue-dye images as a reference.
Small-Animal PET
A dedicated small-animal PET scanner (eXplore VISTA; GE Healthcare) was used for in vivo imaging of 18F-FBnTP kinetics. The protocol is outlined in Figure 1B. Intrinsic spatial and volume resolution of this system is reported as approximately 1.4 mm and 2.9 mm3, respectively (15). In 4 animals, 37 MBq of 18F-FBnTP were injected during a 2-min LCA occlusion. The chest was closed rapidly after reperfusion had been achieved, and the animal was kept under anesthesia and placed on the scanner table immediately. A 90-min dynamic scan (10 min × 9 frames) was started approximately 10 min after tracer injection. The acquired data were reconstructed with the standard VISTA algorithm (2-dimensional ordered-subsets expectation maximization). Reconstructed pixel sizes were 0.3875 mm and 0.775 mm in the transverse and axial directions, respectively. The dimensions of the reconstructed images were 175 × 175 in each of the 61 transverse slices. Data were normalized and corrected for randoms, dead time, and decay. For quantification of the tracer signal, regions of interest were manually selected using AMIDE software (16). The defect area and contralateral remote area were identified in a midventricular short-axis image, and dynamic changes of average tracer activity in the region of interest between 10 and 90 min after tracer injection were determined.
Statistical Analysis
Data are presented as mean ± SD. The Mann–Whitney U test was used to compare differences between 2 independent groups. Comparison of continuous variables between multiple groups was performed by ANOVA using ranks (Kruskal–Wallis test), followed by the Dunn multiple-contrast hypothesis test to identify differences between pairs of groups. The relationship between 2 variables was described using simple linear regression. A value of P less than 0.05 was considered statistically significant. Statistical analysis was done with StatMate III (ATMS Co., Ltd.).
RESULTS
Figure 2 shows representative images of autoradiography and blue-dye staining. At 5 min after reperfusion, autoradiography consistently showed uptake defects in the LCA territory for both 18F-FBnTP and 201Tl. With increasing time after reperfusion, the 201Tl defect disappeared. At 120 min after reperfusion, no significant defect was identified, confirming the known redistribution phenomenon. Quantitatively, the LCA/remote uptake ratio for 201Tl images was 0.42 ± 0.04 at 5 min, 0.72 ± 0.03 at 45 min, and 0.97 ± 0.05 at 120 min (P < 0.01 vs. 5 min). For 18F-FBnTP, a clear uptake defect was found in the LCA occlusion territory until 120 min after reperfusion. The LCA/remote uptake ratio was 0.19 ± 0.02 at 5 min and remained unchanged at 0.19 ± 0.05 after 45 min, whereas there was only a mild reduction to 0.34 ± 0.06 at 120 min. LCA/remote uptake ratios were significantly higher for 18F-FBnTP than for 201Tl at all time points (P < 0.05 at 5, 45, and 120 min). There was a significant positive linear correlation between the defect size by 18F-FBnTP and the size of the unstained vascular territory on blue-dye images (P < 0.001, y = 0.97x+1.5, R2 = 0.94, y = blue-dye defect, x = 18F-FBnTP defect) (Fig. 3).

(A) Dual-tracer autoradiographic short-axis images and photographs of blue-dye staining at 3 different time points after tracer injection and reperfusion. 201Tl (green) demonstrates complete redistribution at 120 min, but 18F-FBnTP (red) shows stable defect over time, delineating territory of LCA as confirmed by absence of blue dye. (B) Graph of uptake ratios for LCA occlusion area relative to remote area for both tracers at all 3 time points (*P < 0.01 vs. 5 min).

Regression plot for comparison between percentage defect area in 18F-FBnTP images and percentage blue-dye stain defect area.
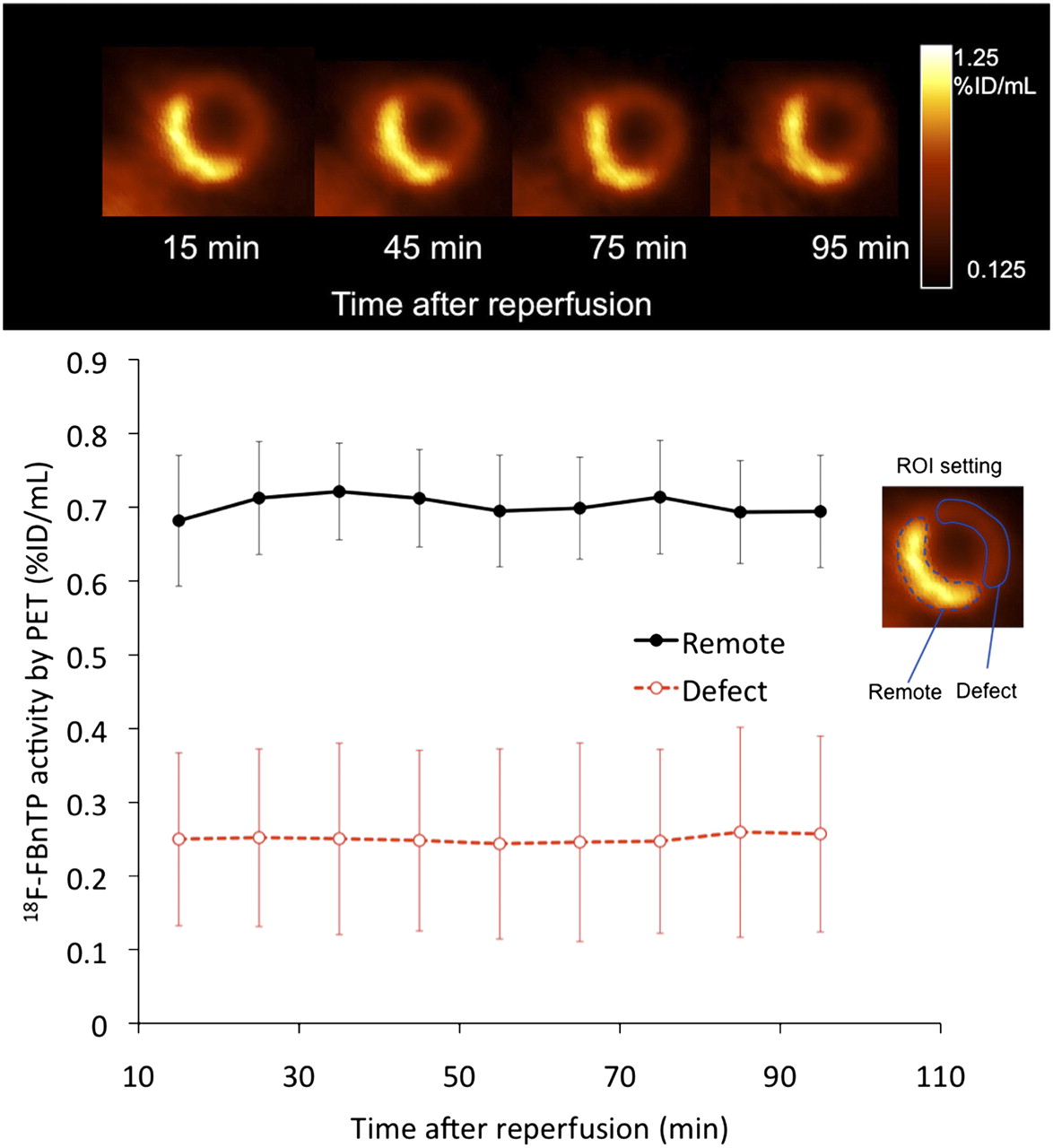
In vivo PET confirmed the findings of autoradiography. Figure 4 shows serial short-axis dynamic PET images after 18F-FBnTP injection during short-term LCA occlusion, followed by reperfusion. The defect remained stable throughout the study period of 10–95 min after injection. Quantification of tracer uptake in the defect and remote area, as also shown in Figure 4, confirmed 18F-FBnTP stability and lack of washout or redistribution. LCA/remote uptake ratios were 0.36 ± 0.13, 0.34 ± 0.14, and 0.36 ± 0.16 at 15, 45, and 95 min after tracer injection, respectively.

Representative short-axis small-animal PET images of 18F-FBnTP at different time points after tracer administration during short-term occlusion, followed by reperfusion. Graph shows mean uptake in defect and remote area. %ID = percentage injected dose; ROI = region of interest.
DISCUSSION
We used a rat model of short-term coronary occlusion followed by reperfusion to study the kinetic properties of the 18F labeled myocardial perfusion agent 18F-FBnTP. Autoradiography and in vivo PET confirmed that this tracer, unlike 201Tl-thallium chloride, shows a stable perfusion defect in the ischemic territory, without relevant washout or redistribution during the first 2 h after injection.
18F-FBnTP is a phosphonium cation that targets mitochondria via a membrane potential–dependent mechanism, similar to the commercially available 99mTc-labeled perfusion SPECT tracers 99mTc-sestamibi and 99mTc-tetrofosmin (5,6). In comparisons with 99mTc-tetrofosmin, a 2.7 times higher perfusion defect contrast and a superior, albeit still nonlinear, relationship between myocardial uptake and microsphere-determined flow were found in a dog model of coronary stenosis, indicating superior characteristics for myocardial perfusion imaging (7). Uptake remained stable in this study until 60 min after injection. Before this work, another study had already reported stable and homogeneous uptake in the heart of healthy dogs, with little in vivo metabolism of the agent (5). Additional in vitro 18F-FBnTP kinetic studies using isolated dog myocytes showed stable tracer binding for 120 min after resuspension in tracer-free solution (5).
The present study not only confirmed stable 18F-FBnTP distribution without redistribution, comparable to 99mTc-sestamibi and 99mTc-tetrofosmin (17), but also added new information to prior work. First, it showed that 18F-FBnTP detects perfusion defects accurately in rats, using small-animal imaging, whereas prior results were obtained in dogs. Second, it validated the size of the 18F-FBnTP perfusion defect against ex vivo blue-dye staining of the ischemic area. And third, it compared 18F-FBnTP with 201Tl and showed superior separation between ischemic and remote areas, as well as absence of redistribution for 18F-FBnTP. The difference of separation even at the early time points (5 min) might be caused by a lack of 18F-FBnTP redistribution and a rapid 201Tl redistribution into the ischemic area. A small decline in the defect-to-remote ratio for 18F-FBnTP at 120 min after injection was most likely overrated by a decay of 18F radioactivity and redistribution into the ischemic area of spillover from coinjected 201Tl for dual-tracer autoradiography. Such spillover effects are unlikely at earlier time points because of the 125-fold difference in radioactivity between the 2 tracers at the time of injection. This conjecture is supported by the additional in vivo PET study that did not show any significant redistribution over the study period of 110 min. Because other cationic tracers such as 99mTc-sestamibi are known to redistribute over time to some degree (18), further confirmatory studies in different experimental models might be necessary to conclude the absence of redistribution.
The results of our study (i.e., the stability of the perfusion defect and the absence of redistribution) suggest—for future clinical protocols—that 18F-FBnTP will allow sufficient time for the patient to be moved from a treadmill to the PET camera for poststress imaging. The ability to perform physical-exercise stress perfusion PET with this longer-lived PET agent may be a future clinical advantage.
Our study also enabled a comparison of 18F-FBnTP with another 18F-labeled perfusion tracer, 18F-BMS-747158-02. 18F-BMS-747158-02, an analog of the insecticide pyridaben, has promising characteristics as a myocardial perfusion tracer (19–22). Unlike 18F-FBnTP, 18F-BMS-747158-02 is already undergoing clinical trials. It has recently been evaluated in a similar model of transient ischemia and reperfusion in rats, where, in contrast to 18F-FBnTP in the present study, continuous slow tracer redistribution was found over 120 min (10). This difference may be a result of different uptake mechanisms. 18F-BMS-747158-02 targets mitochondrial complex I (21,22), whereas 18F-FBnTP targets mitochondrial membrane potential (8). Whether this observation can be translated across species and has implications for clinical application of both agents remains to be determined.
Some limitations of the present study should be considered. First, although our results suggest that physical exercise may be an option in clinical studies because of stable uptake and lack of redistribution, our study was an experimental study in a rodent model. Early clinical applications will be necessary to show that 18F-FBnTP is useful for imaging myocardial perfusion in humans and to confirm the lack of redistribution. And second, we used a model of tracer injection during temporary coronary artery occlusion followed by immediate reperfusion. This model was well suited to determine perfusion defect size but is not identical to the clinical situation, in which hemodynamically relevant stenosis is unmasked by a stress-induced increase of myocardial blood flow. The present model, however, has been well established in prior work (10). Additionally, the success of restoration of perfusion in the LCA area without irreversible tissue damage was confirmed not only by the restoration of color and wall motion of the heart during the procedure but also by the redistribution of coinjected 201Tl.
CONCLUSION
18F-FBnTP is a new PET tracer for assessment of myocardial perfusion abnormalities that shows stability of tracer uptake after injection, a lack of redistribution, and accurate delineation of the flow defect area. These characteristics suggest that exercise stress perfusion PET protocols may be possible in future clinical applications, similar to protocols currently used for SPECT with technetium-labeled agents.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Jennifer Merrill Roselle Abraham, James Fox, and Gilbert Green for their excellent research assistance, and Gola Javadi for her careful editorial assistance. This project was supported in part by a 2008 Nuclear Cardiology Foundation Research Award and an American Heart Association Mid-Atlantic Affiliate Postdoctoral Fellowship Award. The work was also supported in part by National Institutes of Health grant 1RO1HL092985.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication December 8, 2010.
- Accepted for publication February 18, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Targeted Imaging for Cell Death in Cardiovascular Disorders
- 11C-Methionine PET of Myocardial Inflammation in a Rat Model of Experimental Autoimmune Myocarditis
- Comparison of 18F-Labeled Fluoroalkylphosphonium Cations with 13N-NH3 for PET Myocardial Perfusion Imaging
- Imaging Cell Death
- Evaluation of a Mitochondrial Voltage Sensor, (18F-Fluoropentyl)Triphenylphosphonium Cation, in a Rat Myocardial Infarction Model