


Article Figures & Data
Figures
- FIGURE 1.
X-ray analysis revealed the tertiary structure of anxA5, as depicted here. The protein consists of 319 amino acids. Molecule is arranged in planar cyclic structure of 4 domains, which are indicated by different colors in structure. Also shown are Ca2+ ions (green spheres).
- FIGURE 2.
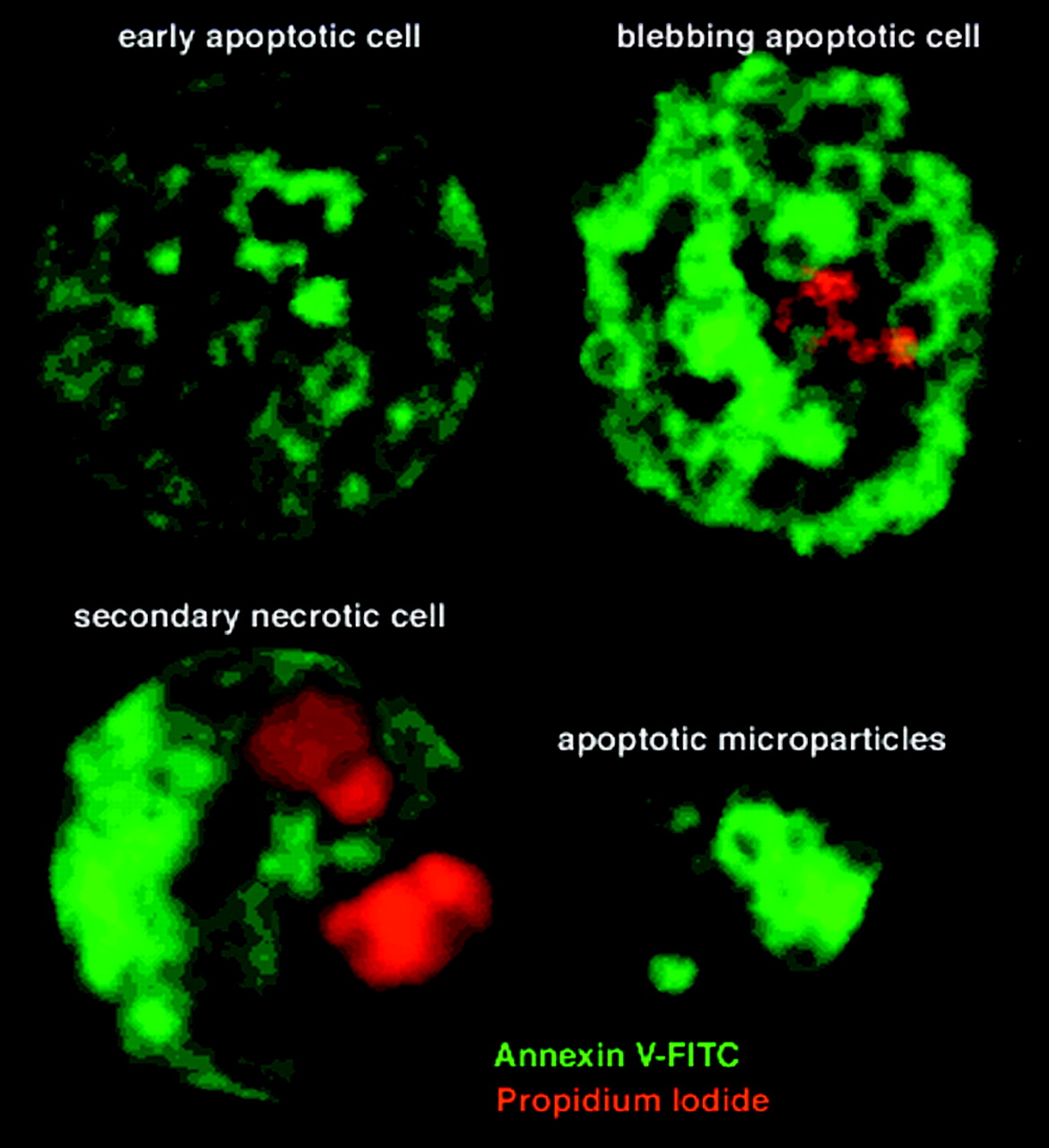
AnxA5 is able to bind to cells in all stages of cell death program. Shown are Fas (D95) ligand–stimulated Jurkat cells. (Top left) Early stage of cell death. Fluorescent anxA5 (green) binds to outer cell membrane. (Top right) Cell in later phase showing binding of PI (red), which is intercalated with DNA and anxA5. Binding of PI is indicative of disintegration of cell membrane. Also, formation of apoptotic bodies is visible. (Bottom) Final stage of PCD. Here, only anxA5 binding to cellular membrane residues can be observed. Also shown is cell undergoing secondary necrosis after PCD. AnxA5 uptake is still present, but cell structures are different from those of cells undergoing PCD only.
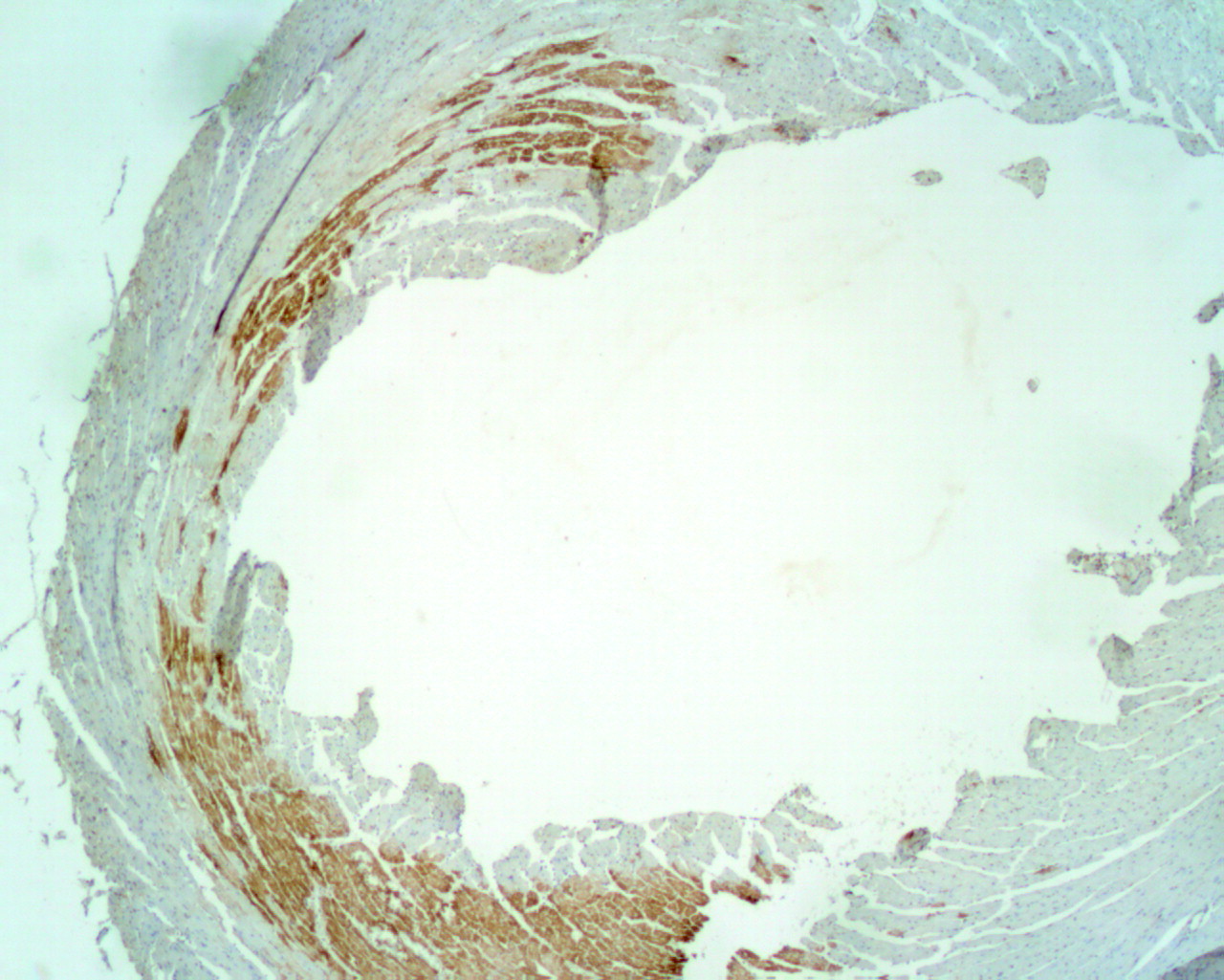
- FIGURE 3.
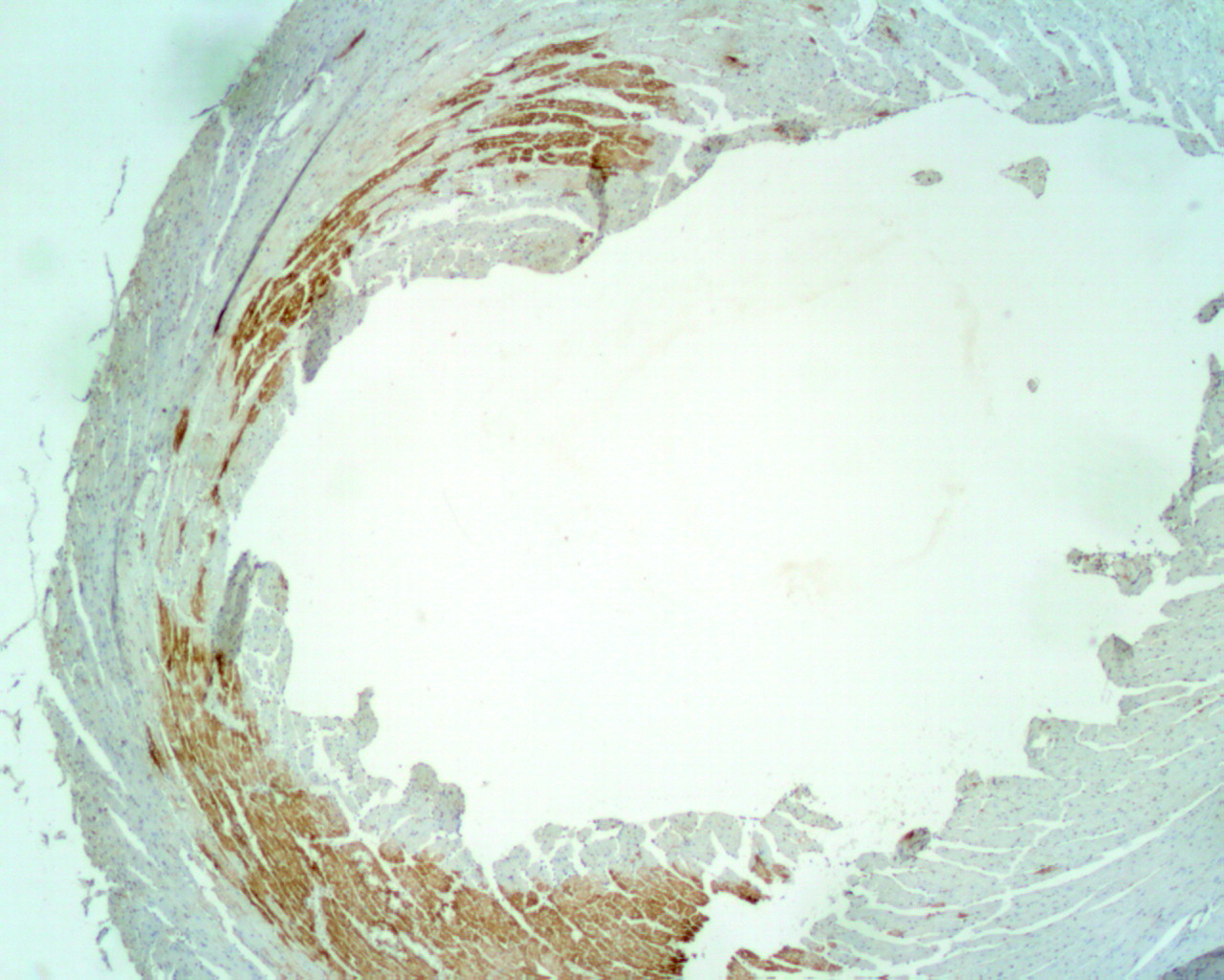
Transverse section of murine heart after 30 min of ischemia and 12 h of reperfusion. Cells were stained for presence of biotinylated anxA5.
- FIGURE 4.
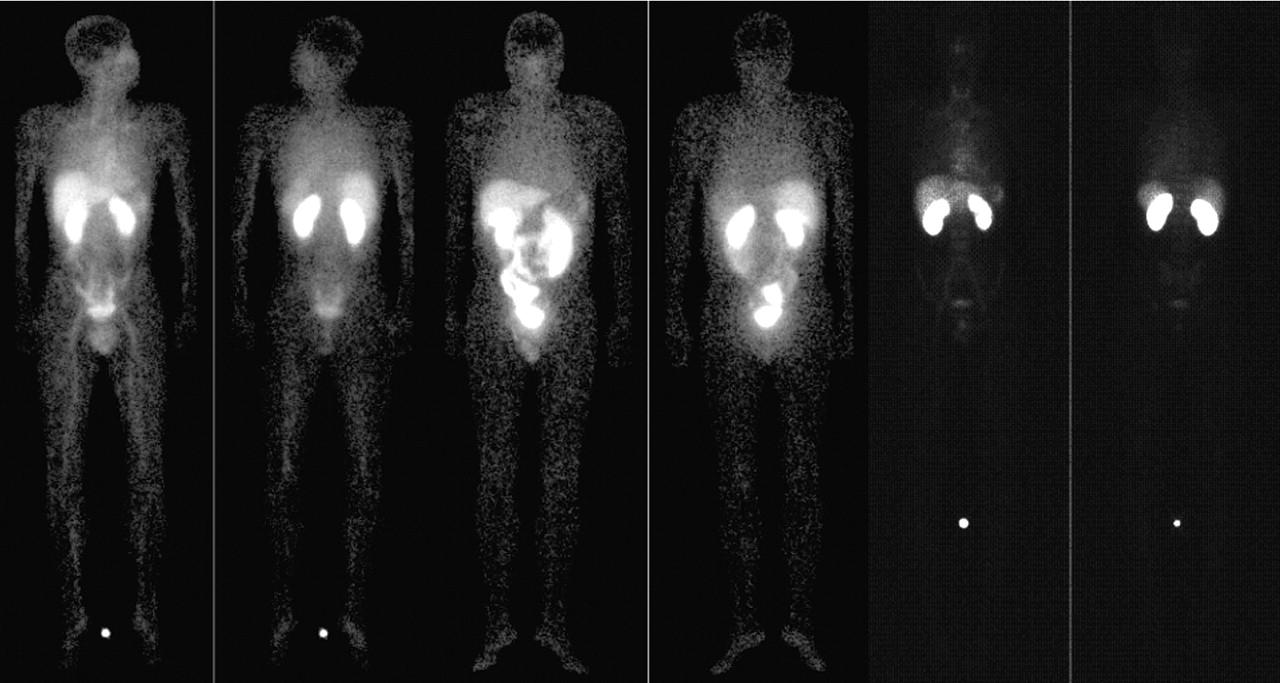
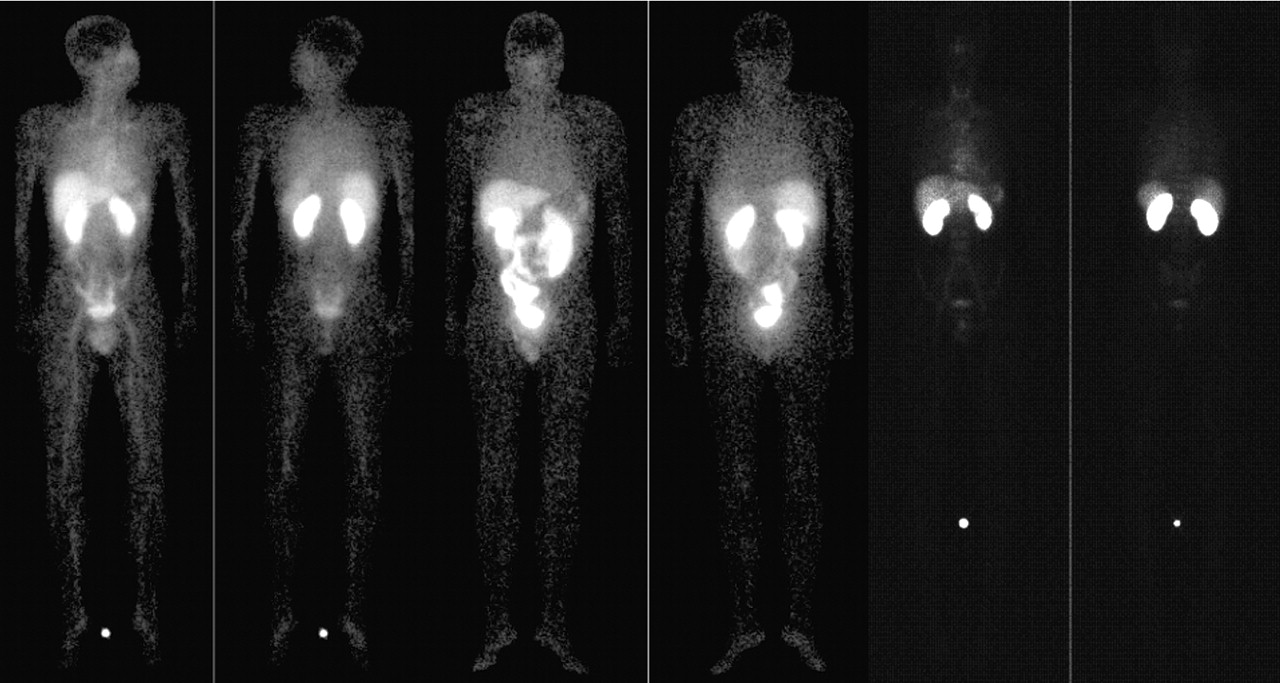
Views of whole-body scans of male volunteer (35 y) (2 left views), male patient (53 y) (2 middle views), and male volunteer (22 y) (2 right views) taken after administration of 440 MBq of imino-anxA5, 566 MBq of BTAP-anxA5, and 263 MBq of HYNIC-anxA5, respectively. In each set of views, anterior is on left and posterior is on right. These views demonstrate low uptake of HYNIC-anxA5 in abdomen, compared with that of other 2 isotope conjugation types for anxA5. HYNIC-anxA5, however, shows more uptake in kidneys than either of other conjugation types. Adapted from (43,53).
- FIGURE 5.
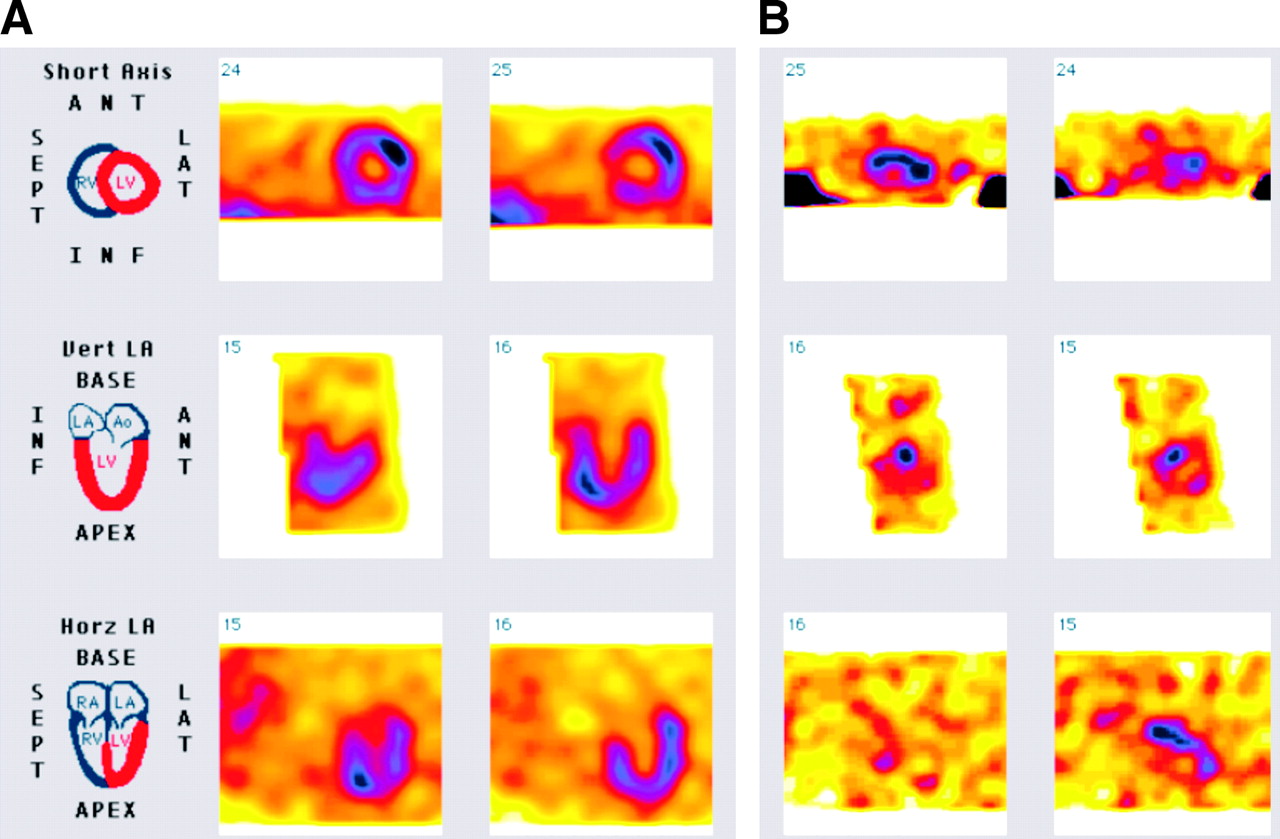
(A) Methoxyisobutylisonitrile (MIBI) scintigraphy depicting area of perfusion, indicating area at risk. (B) Binding of 99mTc-anxA5 to reperfused myocardium, indicative of presence of PCD. ANT = anterior; LAT = lateral; INF = inferior; Vert LA = vertical long axis; Horz LA = horizontal long axis; RV = right ventricle; LV = left ventricle; LA = left atrium; Ao = aorta; RA = right atrium.
- FIGURE 6.
Example of 99mTc-anxA5 uptake in patient with heart failure. Dual-isotope scan shows multifocal anxA5 uptake in patient with idiopathic dilated cardiomyopathy. (Top rows) 201Tl images for orientation purposes. (Bottom rows) Corresponding anxA5 images showing multifocal uptake (arrows). SEPT = septal; LAT = lateral; INF = inferior; ANT = anterior. Adapted from (74).
- FIGURE 7.
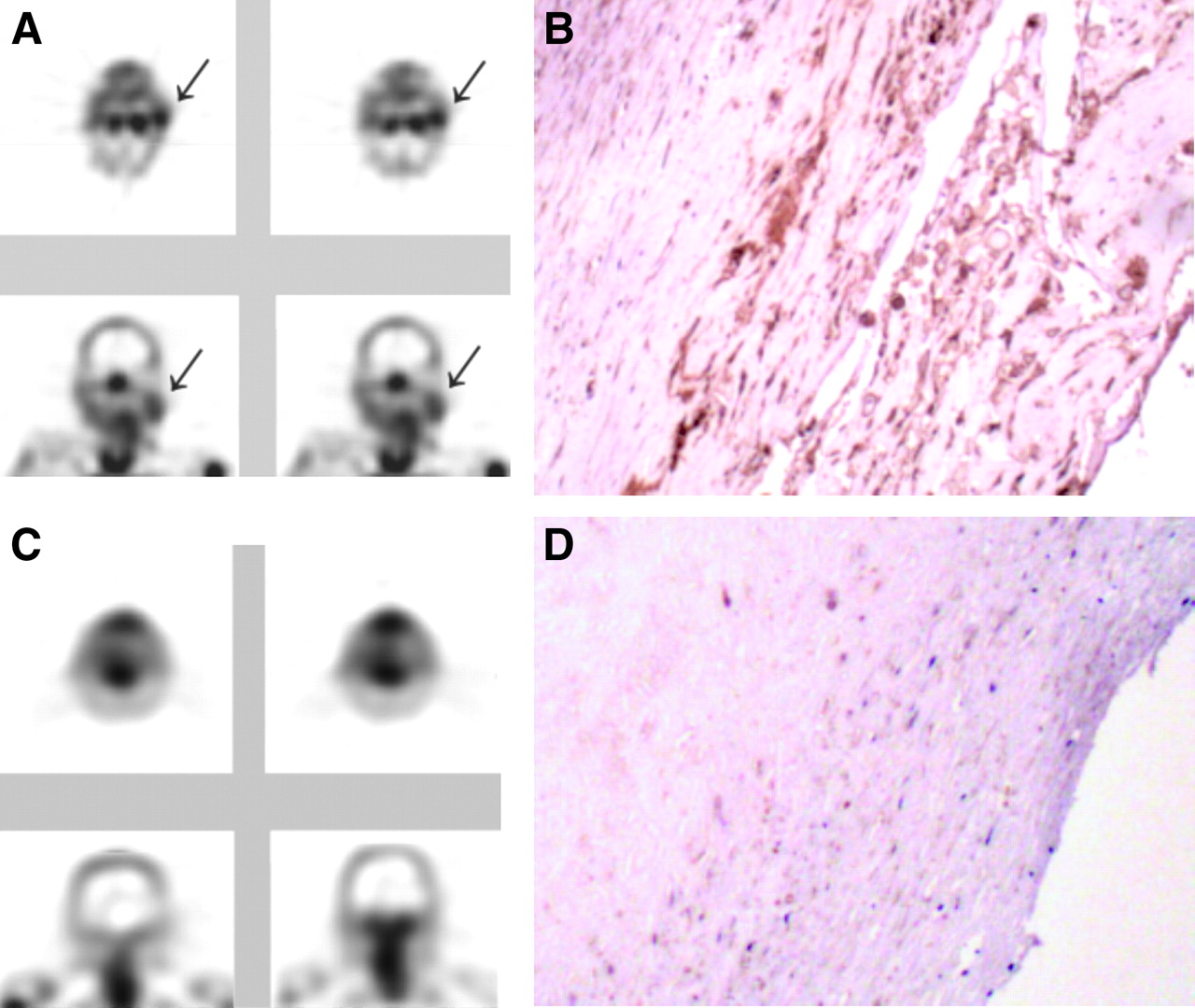
99mTc-AnxA5 imaging in patients with atherosclerosis. (A) Transverse and coronal SPECT views from patient who had had transient ischemic attack 3 d before imaging. Although stenosis was clinically significant in both carotid arteries, uptake of anxA5 was evident only in culprit lesion (arrows). (B) Histopathologic examination of tissues from this patient shows extensive binding of anxA5 detected by rabbit antiannexin antibodies. (C) For another patient, who had had transient ischemic attack 3 mo before imaging, images do not show any uptake of anxA5. (D) Similarly, histopathologic analysis does not show significant binding of anxA5, although lesion within the carotid artery is evident. Adapted from (40).
- FIGURE 8.
(A) Thallium perfusion scintigraphy of malignant tumor showing perfused myocardium of left ventricle in short-axis orientation. (B) Increased uptake of BTAP-anxA5 within contour of left ventricle on short-axis SPECT with orientation similar to that of perfusion scintigram. ANT = anterior; SEPT = septal; LAT = lateral; INF = inferior; Vert LA = vertical long axis; Horz LA = horizontal long axis; RV = right ventricle; LV = left ventricle; LA = left atrium; Ao = aorta; RA = right atrium. Adapted from (41).
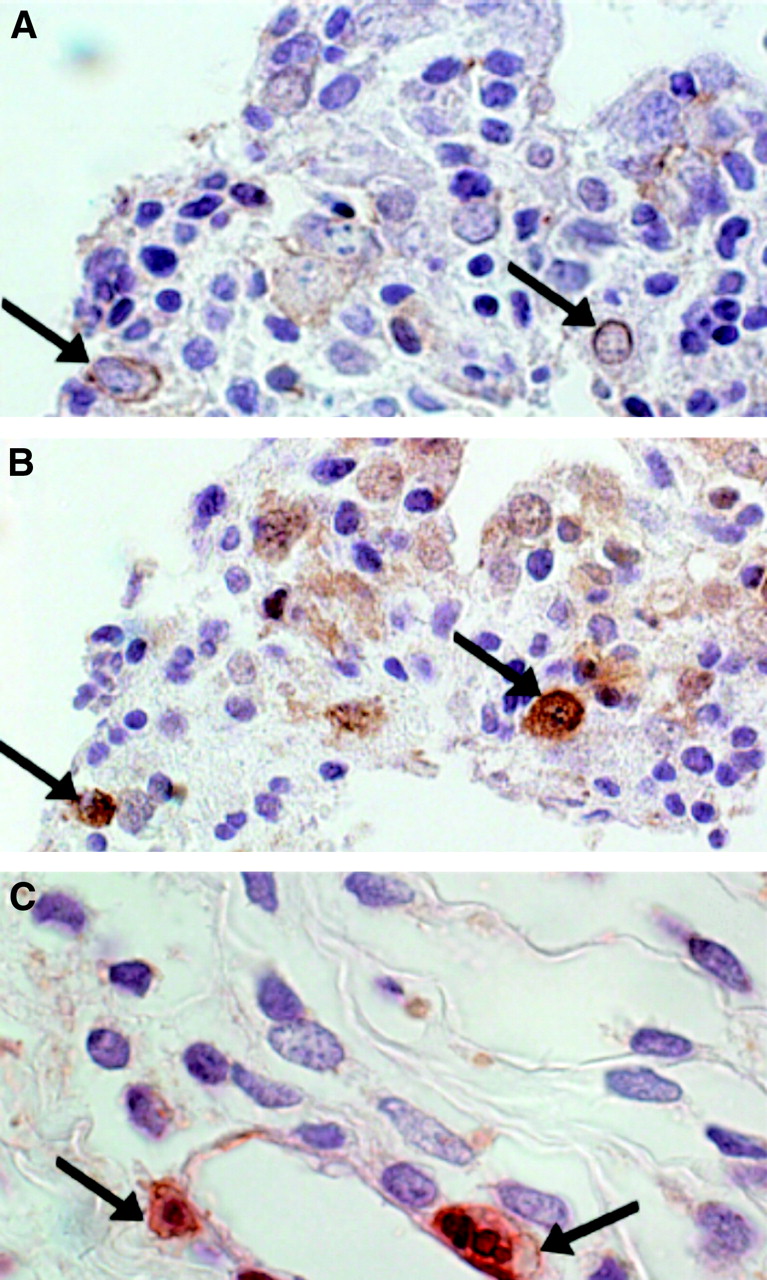
- FIGURE 9.
Malignant intracardiac sarcoma (immunohistologic analysis). (A) AnxA5 antibody staining (brown staining, arrows). (B) CM-1 antibody staining, indicating caspase 3 activation (brown staining, arrows). (C) Double staining with both CM-1 antibody (red staining) and anxA5 antibody (brown staining, arrows). Adapted from (41).
- FIGURE 10.
(A) Thallium perfusion scintigraphy of benign tumor shows perfused left ventricle of myocardium in short-axis orientation. (B) No increased uptake of BTAP-anxA5 can be seen within contour of left ventricle on short-axis SPECT with orientation similar to that of perfusion scintigram. (C) Upon histologic examination, tissue was found to have features of myxoma, with clustering of nuclei and large cellular matrices. No significant anxA5 antibody uptake and no caspase 3 activation could be demonstrated. ANT = anterior; SEPT = septal; LAT = lateral; INF = inferior; Vert LA = vertical long axis; Horz LA = horizontal long axis; RV = right ventricle; LV = left ventricle; LA = left atrium; Ao = aorta; RA = right atrium.
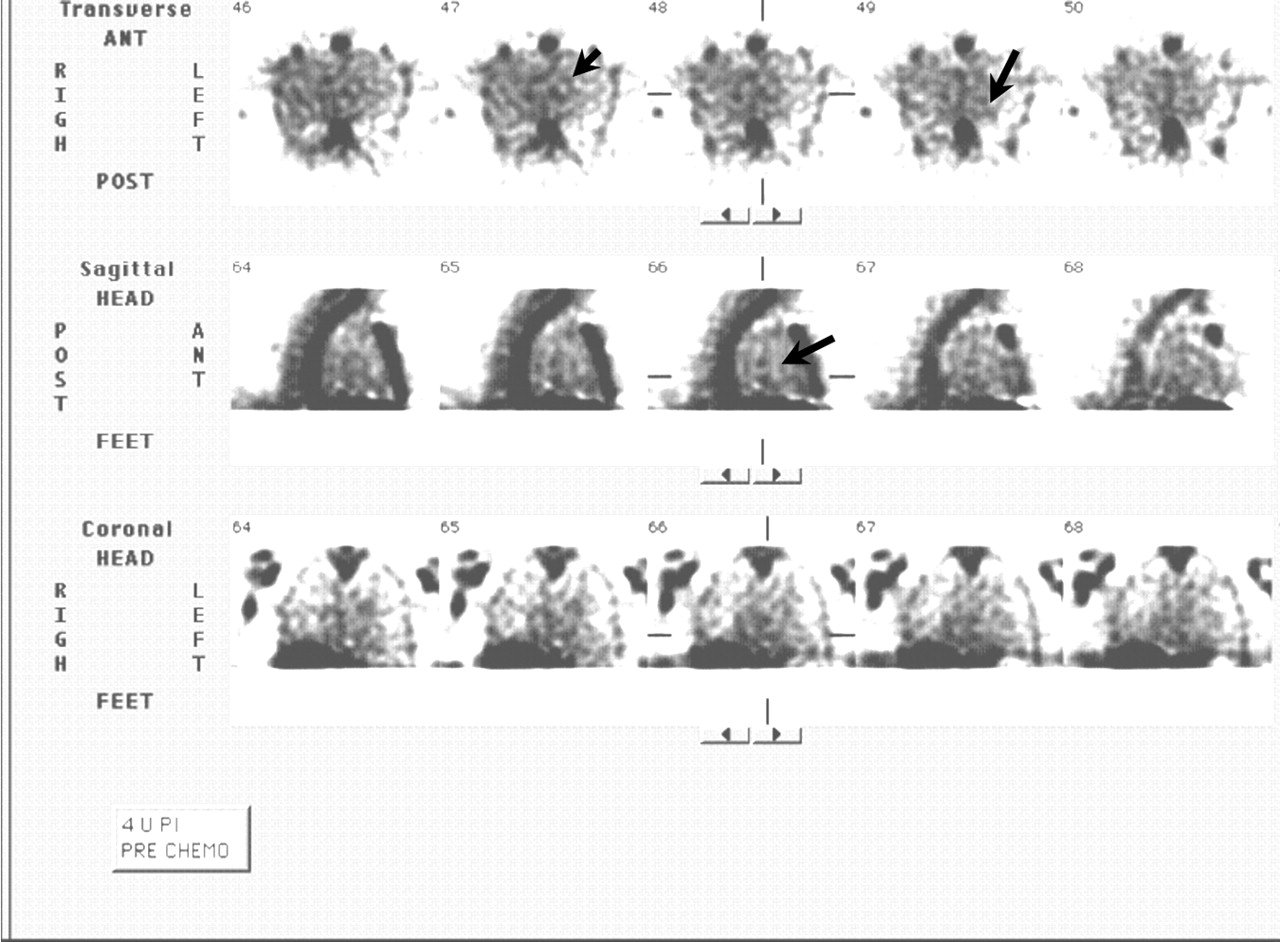
- FIGURE 11.
SPECT image of non–small cell lung carcinoma. Increased uptake of HYNIC-anxA5 can be seen within thorax (arrows). ANT = anterior; POST = posterior; 4 h PI = 4 h after injection of HYNIC-anxA5; PRE CHEMO = before chemotherapy.
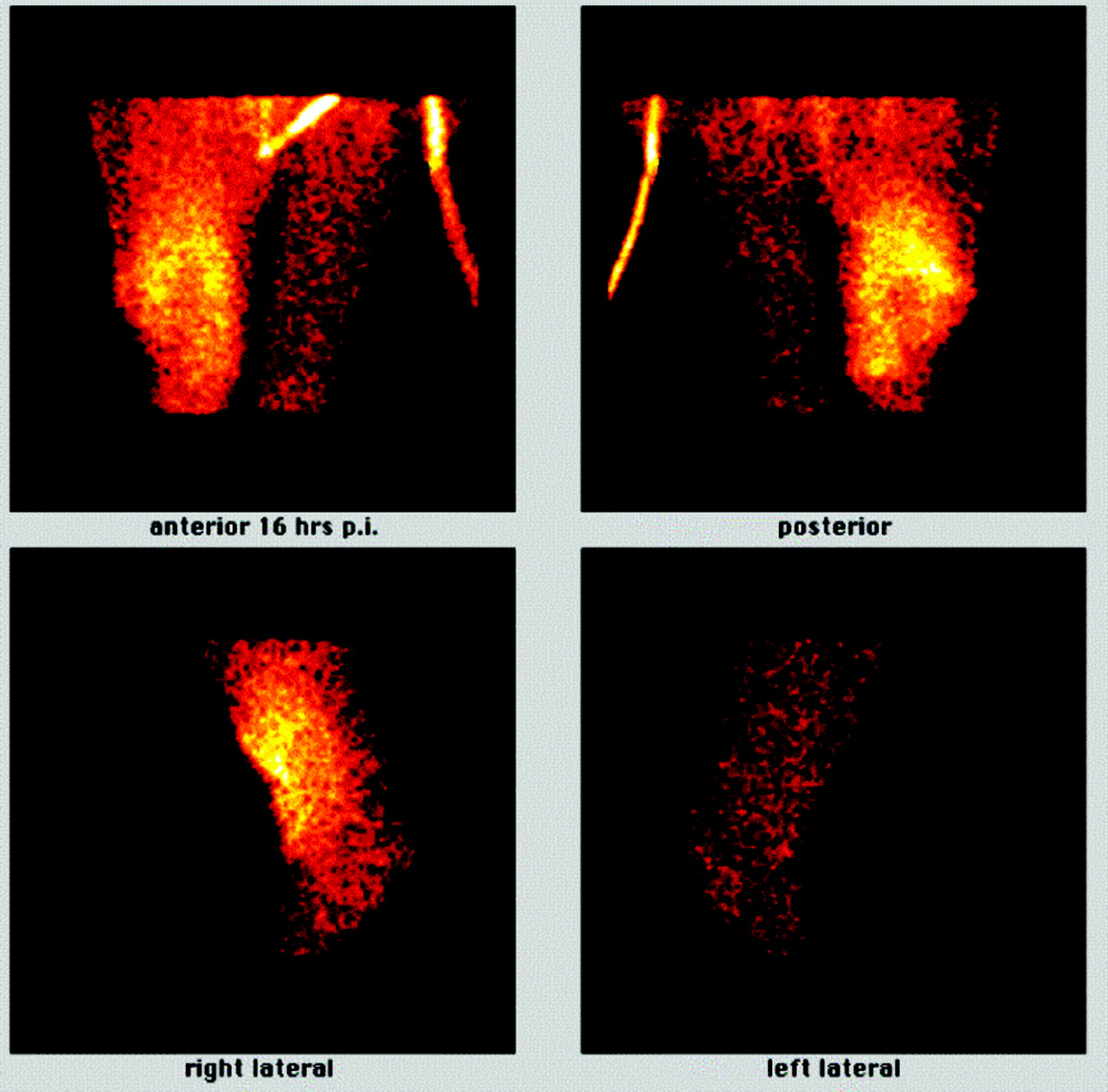
- FIGURE 12.
Planar images of patient with sarcoma of right leg at 16 h after injection (p.i.) of BTAP-anxA5. There was increased uptake of BTAP-anxA5 in major part of upper right leg, with central zone of decreased activity. Almost no uptake was seen in left leg. Adapted from (43).





Tables
Radiopharmaceutical Emissions and energy Physical half-life Advantages (Pro) or Disadvantages (Con) 99mTc-AnxA5 (general) γ, 140.5 keV 6.02 h Pro: 99mTc can be obtained easily at low cost by use of 99Mo/99mTc generators; excellent imaging properties Con: difficult radiochemistry for technetium; biodistribution influenced by conjugation method 99mTc-Imino-anxA5 γ, 140.5 keV 6.02 h Pro: labeling can be performed easily Con: RCP ≈ 80%; high uptake of radiopharmaceutical in liver, kidneys, and spleen; long biologic half-life 99mTc-BTAP-anxA5 γ, 140.5 keV 6.02 h Pro: RCP > 93%; short biologic half-life Con: labeling method very laborious; high radioactivity uptake in liver, kidneys, spleen, and abdomen; low radiochemical yield 99mTc-HYNIC-anxA5 γ, 140.5 keV 6.02 h Pro: labeling method well established; prefabricated kit, so labeling can be performed easily Con: high uptake of radiopharmaceutical in kidneys and liver; long biologic half-life 99mTc-EC-anxA5 γ, 140.5 keV 6.02 h Pro: prefabricated kit, so labeling can be performed easily Con: to establish this method, more research is required 94mTc-AnxA5 (general) β+, 2.5 MeV 53 min Pro: easiest way to transform SPECT into PET; when HYNIC-anxA5 is used, labeling can be performed easily Con: difficult radiochemistry for technetium; biodistribution influenced by conjugation method; expensive and difficult to obtain 123I-AnxA5 γ, 160 keV 13 h Pro: no uptake in liver and kidneys after 12 h; good imaging expected in abdominal region, compared to that with known 99mTc compounds; good radiochemical purity Con: laborious labeling method; more expensive than 99mTc labeling 124I-AnxA5 β+, E = 1.53, 2.14 MeV, γ (complex decay under emission of several high-energy γ-photons) 4.2 d Pro: long-lived PET tracer; suitable for animal studies and studies in humans with terminal disease; labeled compound with long shelf-life (4 d without detectable deiodination); RCP > 95% Con: high radiation burden and therefore less suitable for patient imaging; laborious labeling method 125I-AnxA5 EC, 35 keV 60 d Pro: long-lived isotope; very useful for research purposes to test iodine labeling techniques in animals; low radiation burden for research workers Con: no imaging possibility 111In-AnxA5 γ, 173 keV, 247 keV (ratio of both energies is 1:1), electron capture gives x-ray energy of 23 keV 2.8 d Pro: longer-lived isotope; may be suitable for imaging of tumor response in patients Con: difficult radiochemistry for indium; biodistribution influenced by conjugation method; biodistribution of pegylated In-conjugated anxA5 appears to be poor; rather high radiation burden in patients 18F-AnxA5 β+, 633 keV 110 min Pro: PET tracer with optimal half-life for imaging; promising agent for patient imaging Con: more research is required to establish its use in patients; labeling method is not yet standardized Cell death imaging targets in studies supporting clinical evidence Reference(s) Cardiovascular disease Myocardial infarction 2,64 Cardiac allograft rejection 39 Heart failure 74 Carotid atherosclerosis 40 Oncology Intracardiac tumors (malignant: 99mTc-anxA5 uptake; benign: so far no 99mTc-anxA5 uptake) 40,79 Head and neck tumors 42 Non-Hodgkin’s lymphoma 43,85 Recurrent follicular lymphoma 86 Leukemia 87 Non–small cell lung cancer 85 Sarcoma 43 Breast cancer 43,85 Cancer therapy: positive correlation between 99mTc-anxA5 uptake and therapy efficacy 85,87
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lung basement membranes are compositionally and structurally altered following resolution of acute inflammation
- Mag-Net: Rapid enrichment of membrane-bound particles enables high coverage quantitative analysis of the plasma proteome
- Mag-Net: Rapid enrichment of membrane-bound particles enables high coverage quantitative analysis of the plasma proteome
- Noninvasive Whole-Body Imaging of Phosphatidylethanolamine as a Cell Death Marker Using 99mTc-Duramycin During TNF-Induced SIRS
- Cardioprotective Effects of HSP72 Administration on Ischemia-Reperfusion Injury
- Severe, Early Axonal Degeneration Following Experimental Anterior Ischemic Optic Neuropathy
- A Peptide-Based Positron Emission Tomography Probe for In Vivo Detection of Caspase Activity in Apoptotic Cells
- Recent Advances in the Molecular Imaging of Programmed Cell Death: Part I--Pathophysiology and Radiotracers
- Imaging DNA Damage In Vivo Using {gamma}H2AX-Targeted Immunoconjugates
- A Universally Applicable 68Ga-Labeling Technique for Proteins
- Engineered Annexin A5 Variants Have Impaired Cell Entry for Molecular Imaging of Apoptosis Using Pretargeting Strategies
- Annexin A5 Therapy Attenuates Vascular Inflammation and Remodeling and Improves Endothelial Function in Mice
- Apoptosis Imaging: Beyond Annexin V
- Imaging of Atherosclerosis in Apoliprotein E Knockout Mice: Targeting of a Folate-Conjugated Radiopharmaceutical to Activated Macrophages
- Imaging of Apoptosis
- Molecular Imaging of Neurovascular Cell Death in Experimental Cerebral Stroke by PET
- Identifying vulnerable carotid plaques by noninvasive imaging
- In Vivo Detection of Apoptosis
- Real-Time In Vivo Imaging of Retinal Cell Apoptosis after Laser Exposure
- Effect of Postconditioning on Myocardial 99mTc-Annexin-V Uptake: Comparison with Ischemic Preconditioning and Caspase Inhibitor Treatment
- Nuclear Imaging Probes: from Bench to Bedside
- Sequential 99mTc-Hydrazinonicotinamide-Annexin V Imaging for Predicting Response to Chemotherapy