


Abstract
Increased glucose metabolism of inflammatory tissues is the main source of false-positive 18F-FDG PET findings in oncology. It has been suggested that radiolabeled nucleosides might be more tumor specific. Methods: To test this hypothesis, we compared the biodistribution of 3′-deoxy-3′-18F-fluorothymidine (FLT) and 18F-FDG in Wistar rats that bore tumors (C6 rat glioma in the right shoulder) and also had sterile inflammation in the left calf muscle (induced by injection of 0.1 mL of turpentine). Twenty-four hours after turpentine injection, the rats received an intravenous bolus (30 MBq) of either 18F-FLT (n = 5) or 18F-FDG (n = 5). Pretreatment of the animals with thymidine phosphorylase (>1,000 U/kg, intravenously) before injection of 18F-FLT proved to be necessary to reduce the serum levels of endogenous thymidine and achieve satisfactory tumor uptake of radioactivity. Results: Tumor-to-muscle ratios of 18F-FDG at 2 h after injection (13.2 ± 3.0) were higher than those of 18F-FLT (3.8 ± 1.3). 18F-FDG showed high physiologic uptake in brain and heart, whereas 18F-FLT was avidly taken up by bone marrow. 18F-FDG accumulated in the inflamed muscle, with 4.8 ± 1.2 times higher uptake in the affected thigh than in the contralateral healthy thigh, in contrast to 18F-FLT, for which this ratio was not significantly different from unity (1.3 ± 0.4). Conclusion: In 18F-FDG PET images, both tumor and inflammation were visible, but 18F-FLT PET showed only the tumor. Thus, the hypothesis that 18F-FLT has a higher tumor specificity was confirmed in our animal model.
FDG labeled with 18F is currently the most widely used radiopharmaceutical in clinical oncology. This analog of glucose is trapped in tissues after phosphorylation by hexokinase but is not a substrate for glycolysis. Although the applications of 18F-FDG PET in tumor detection, staging, and therapy evaluation are rapidly expanding, 18F-FDG uptake is not tumor specific. Various forms of inflammatory lesions also take up 18F-FDG and are a major cause of false-positive results. Histologic confirmation of 18F-FDG-positive lesions is therefore required for many types of tumors (1–6). Macrophages, which invade tumors, especially after anticancer therapy, can induce high 18F-FDG uptake as well and can complicate the interpretation of 18F-FDG PET images (1,7–9). Decreased uptake of 18F-FDG is seen in hyperglycemic patients and can cause false-negative results.
Another approach for tumor visualization is the use of radiolabeled nucleosides such as 11C-thymidine. Because 11C-thymidine is rapidly incorporated into newly synthesized DNA, this radiopharmaceutical can be used to image cellular proliferation. Animal and in vitro studies have suggested that thymidine uptake is considerable in malignant tissue but much less in inflammatory cells than is 18F-FDG uptake (10,11). Unfortunately, the imaging quality of 11C-thymidine is relatively poor, and its clinical applications are limited because of rapid in vivo degradation and the short half-life of 11C (20 min) (12–14).
However, the pyrimidine analog 3′-deoxy-3′-fluorothymidine (FLT) can be labeled with 18F (half-life, 109.8 min) and is resistant to metabolic breakdown (15). 18F-FLT is transported by the same nucleoside carrier as is thymidine and is also phosphorylated by the same enzyme, S-phase-specific thymidine kinase 1, which leads to intracellular trapping of radioactivity within the cytosol (16–21). In contrast to thymidine, 18F-FLT remains in the cytosolic fraction as 18F-FLT monophosphate and acts as a DNA chain terminator because of the 3′ substitution (17). Thus, only a very slight DNA incorporation of 18F-FLT has been observed in cell lines (18).
Although inflammatory cells display a high metabolic activity and an avid uptake of 18F-FDG, they are recruited from elsewhere and do not divide at the site of inflammation. Because the mitotic activity of inflammatory cells is low, these cells can be expected to show a relatively low uptake of radiolabeled nucleosides. Thus, 18F-FLT may overcome a major drawback of 18F-FDG imaging.
To the best of our knowledge, no studies comparing the selectivity of 18F-FDG and 18F-FLT for tumor and inflammation have been reported in the literature. Therefore, we decided to examine the biodistribution of these radiopharmaceuticals in male Wistar rats that bore tumors and also had sterile inflammation. The inflammation was induced by injection of turpentine, which is known to result in exudation of plasma and migration of neutrophils within 24 h (22).
MATERIALS AND METHODS
Materials
18F-FLT was produced by radiofluoridation of the 2,3′-anhydro-5′-O-(4,4′-dimethoxytrityl)-thymidine precursor, with radiochemical yields of 5%–10%. 18F-FDG was produced by the Hamacher method (nucleophilic fluorination reaction followed by deprotection). The specific radioactivities of 18F-FLT and 18F-FDG were always >10 (usually 50–100) TBq/mmol. Thymidine phosphorylase (from the bacterium Escherichia coli) was obtained from Sigma. Matrigel basement membrane matrix was purchased from BD Biosciences. Turpentine came from a local paint shop.
Animal Model
The experiments were performed by licensed investigators in accordance with the Law on Animal Experiments of The Netherlands. Male Wistar rats (200- to 240-g body weight) were obtained from Harlan. After the rats had been allowed 1 wk of acclimation, C6 glioma cells (2 × 106, in a 1:1 v/v mixture of Matrigel and Dulbecco’s minimal essential medium containing 5% fetal calf serum) were subcutaneously injected into the right shoulder. Matrigel was included to avoid migration of tumor cells to sites other than the place of injection. Ten days later, 0.1 mL of turpentine was intramuscularly injected into the thigh of the left hind leg. After an additional 24 h, the radiopharmaceutical (either 18F-FDG or 18F-FLT) was intravenously administered through a tail vein.
Phosphorylase Pretreatment
To reduce the serum levels of endogenous thymidine, 5 rats were pretreated with thymidine phosphorylase (1,000–1,500 U/kg of body weight) 45 min before injection of 18F-FLT. The enzyme was administered by intravenous infusion through a tail vein. Because phosphorylase is supplied in potassium phosphate buffer, a slow rate of infusion was used (less than 50 μL/min; total volume, 0.6–1.0 mL) to avoid myocardial arrest. Plasma thymidine was measured using reversed-phase high-performance liquid chromatography (23,24).
Biodistribution Experiments
Twenty-four hours after the turpentine injection, the rats were anesthetized using (S)-ketamine (50 mg/kg intraperitoneally) and medetomidine (0.3 mg/kg intraperitoneally). The animals were kept under anesthesia for the rest of the experiment. A bolus of either 18F-FLT or 18F-FDG (0.3 mL containing 30 MBq) was administered by intravenous injection through a lateral tail vein. The rats were sacrificed 120 min after radiotracer injection by extirpation of the heart (under general ketamine/medetomidine anesthesia). Blood was collected, and normal tissues (brain, fat, bone, heart, intestines, kidney, liver, lung, skeletal muscle, pancreas, spleen, submandibular salivary gland, and urinary bladder) were excised. Urine was collected, and plasma and a red cell fraction were obtained from blood centrifugation (5 min at 1,000g). The complete tumor was excised and carefully separated from muscle and skin. Inflamed muscle was recognizable by its pale color and could generally be distinguished from the surrounding darker tissue. A relatively small sample including the inflamed region (0.71 ± 0.32 g) was excised from the affected thigh. All samples were weighed, and the radioactivity was measured using a Compugamma CS 1282 counter (LKB-Wallac), applying a decay correction. The results were expressed as dimensionless standardized uptake values (dpm measured per gram of tissue/dpm injected per gram of body weight). Tissue-to-plasma and tumor-to-muscle concentration ratios of radioactivity were also calculated.
Histologic Examination of Inflamed Muscle and C6 Tumors
Excised tumors and the inflamed parts of the thigh muscle were fixed in formalin and embedded in paraffin. Sections 5 μm thick were stained with hematoxylin and eosin.
PET Imaging
Rats anesthetized with ketamine and medetomidine were placed into a positron camera (ECAT 962/HR+, 4.5 mm in full width at half maximum; Siemens) and received a bolus injection of either 18F-FLT or 18F-FDG (30 MBq) through a tail vein. Data were acquired from 90 to 150 min. A zoom factor of 1.5 was applied during reconstruction (by filtered backprojection), and the matrix size was 128 × 128.
Statistical Analysis
Statistical analysis was performed using the software package Statistix (NH Analytic Software). Differences between the various groups (18F-FLT, 18F-FLT with phosphorylase pretreatment, and 18F-FDG) were tested for statistical significance using the 2-sided student t test for independent samples. P values < 0.05 were considered significant.
RESULTS
Development of Tumor and Inflammation
The growth rate of C6 tumors in Wistar rats proved to be variable. Tumor mass at radiotracer injection was 1.61 ± 0.89 g (mean ± SD; range, 0.41–2.97 g). Turpentine injection resulted in visible swelling of the inflamed thigh after 24 h, although the behavior of the rats during this period was normal. The body weight of the animals during the biodistribution experiments was 325 ± 27 g.
18F-FLT Uptake in Untreated Rats
In initial experiments on 3 rats, the radiopharmaceutical 18F-FLT was administered directly to the animals without any pretreatment. To our surprise, the nucleoside did not accumulate above plasma levels in any organ except bone marrow, small intestine, kidney, and urinary bladder (Table 1). Radioactivity did not accumulate even in the C6 tumors (Table 2). High serum levels of endogenous thymidine may have saturated tissue nucleoside transporters or thymidine kinase 1 and have blocked uptake or trapping of 18F-FLT. Anthony F. Shields (Karmanos Cancer Institute), Peter S. Conti, and James R. Bading (University of Southern California) suggested that we infuse thymidine phosphorylase before injection of 18F-FLT to circumvent this problem. The next 5 rats were pretreated in this way; the radiolabeled nucleoside was administered 45 min after the start of enzyme infusion. Data on untreated animals were compared with data on the thymidine phosphorylase-pretreated group.
Standardized Uptake Values at 120 Minutes After Injection
Tissue-to-Plasma and Tissue-to-Muscle Ratios Besides Selectivity Index (Tumor vs. Inflammation)
18F-FLT Uptake After Pretreatment
Pretreatment of animals with thymidine phosphorylase (intravenously, 45 min before administration of the radiotracer) did not affect tissue-to-plasma ratios of 18F-FLT in brain, adipose tissue, urinary bladder, heart, kidney, liver, lung, normal and inflamed skeletal muscle, pancreas, or red blood cells. However, infusion of the enzyme increased the accumulation of 18F-FLT in bone, bone marrow, and the C6 tumor (Tables 1 and 2). Plasma levels of radioactivity tended to decrease after phosphorylase infusion. Thus, tissue-to-plasma ratios of radioactivity were significantly increased in bone, bone marrow, intestines, tumor, spleen, and submandibular salivary gland (data not shown). Tumor-to-muscle ratios of radioactivity also significantly increased after phosphorylase treatment (Table 2). Plasma levels of thymidine were measured in a parallel experiment on a single rat and were found to decrease from 0.15 μg/mL to undetectable levels after phosphorylase infusion.
Biodistribution of 18F-FDG and 18F-FLT
The next 5 animals received 18F-FDG rather than 18F-FLT, to compare the biodistribution of the 2 radiopharmaceuticals. The glucose analog 18F-FDG showed physiologic uptake in heart and brain. 18F-FDG uptake was higher than 18F-FLT uptake in C6 tumors, inflamed muscle, brain, adipose tissue, kidney, large intestine, lung, and submandibular salivary gland (Table 1). In contrast, 18F-FLT accumulated more in bone, bone marrow, and healthy muscle than did 18F-FDG (Table 1).
Selectivity of 18F-FDG and 18F-FLT
18F-FLT did not accumulate in inflammatory tissue (tissue-to-plasma and tissue-to-muscle ratios were not significantly different from unity). However, 18F-FDG accumulation was 4.8-fold higher (P = 0.0002) in inflamed thigh muscle than in the noninflamed contralateral thigh (Table 2). The selectivity index (tumor-to-inflammatory tissue ratio corrected for uptake in healthy muscle) was >10.6 for 18F-FLT and 3.5 for 18F-FDG (Table 2).
Tumor-to-plasma ratios of 18F-FLT and 18F-FDG were not significantly different, but tumor-to-muscle ratios of 18F-FDG were significantly higher (P = 0.001) than those of 18F-FLT (Table 2).
Histology of Inflamed Muscle and C6 Tumors
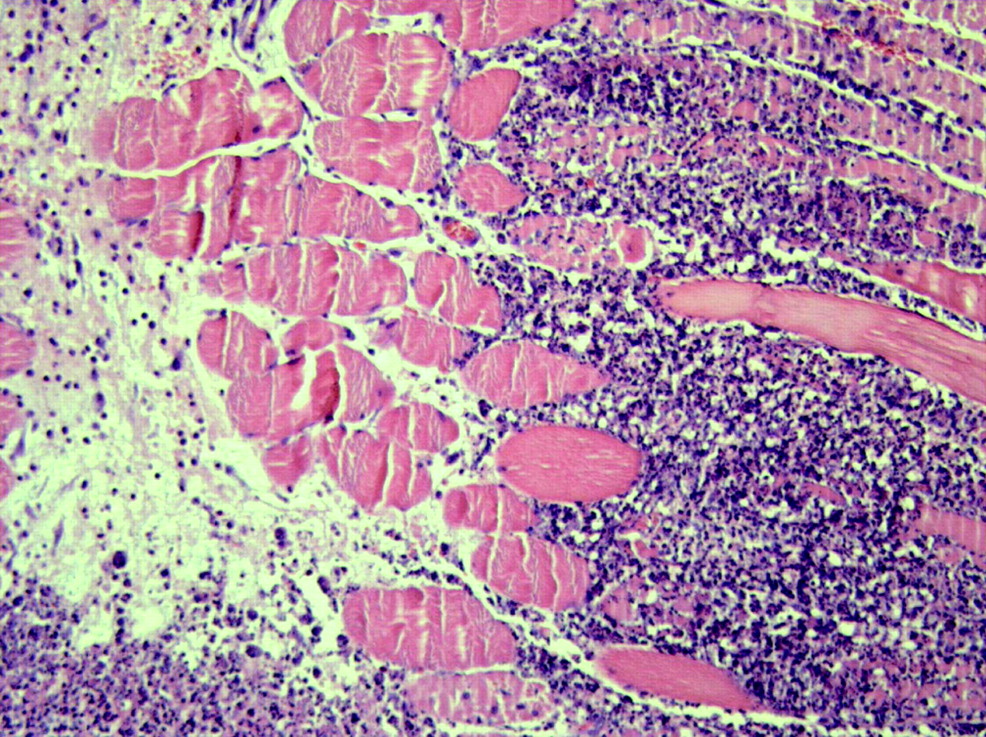
Histologic examination of the muscle specimens excised 24 h after turpentine injection showed an acute inflammatory reaction. Massive infiltration of neutrophils was seen in and between partially necrotic muscle fibers—the picture of acute myositis (Fig. 1). In the border of the inflammatory infiltrate, macrophages and few fibroblasts could be discerned.
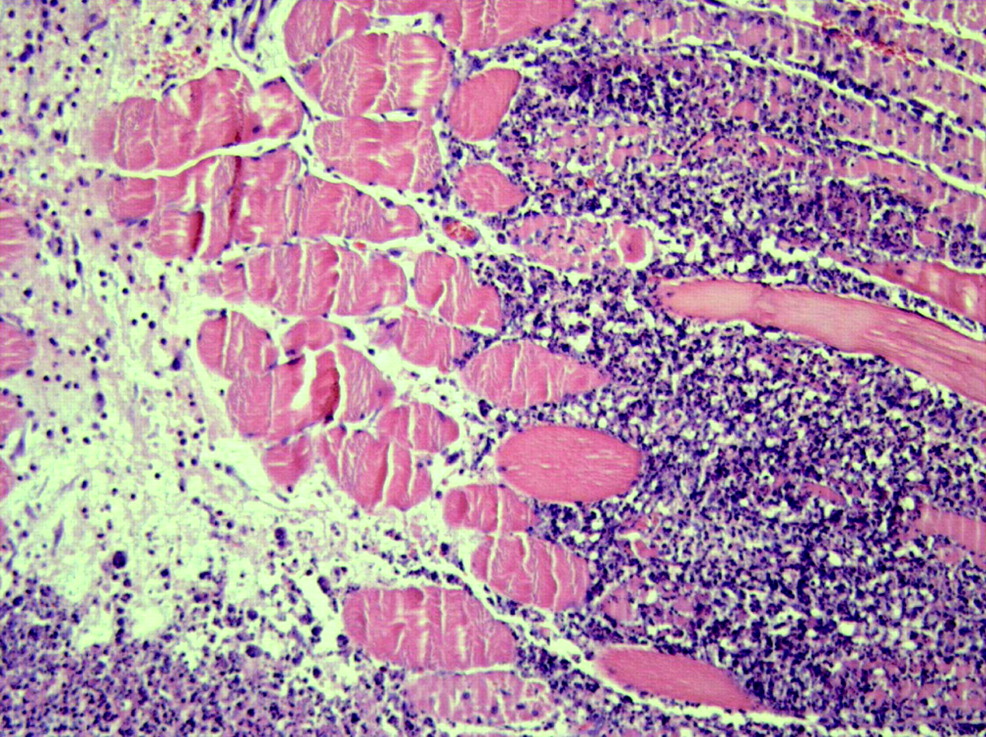
Microscopic image of a specimen of inflamed rat muscle, 24 h after injection of turpentine (hematoxylin and eosin, ×400).
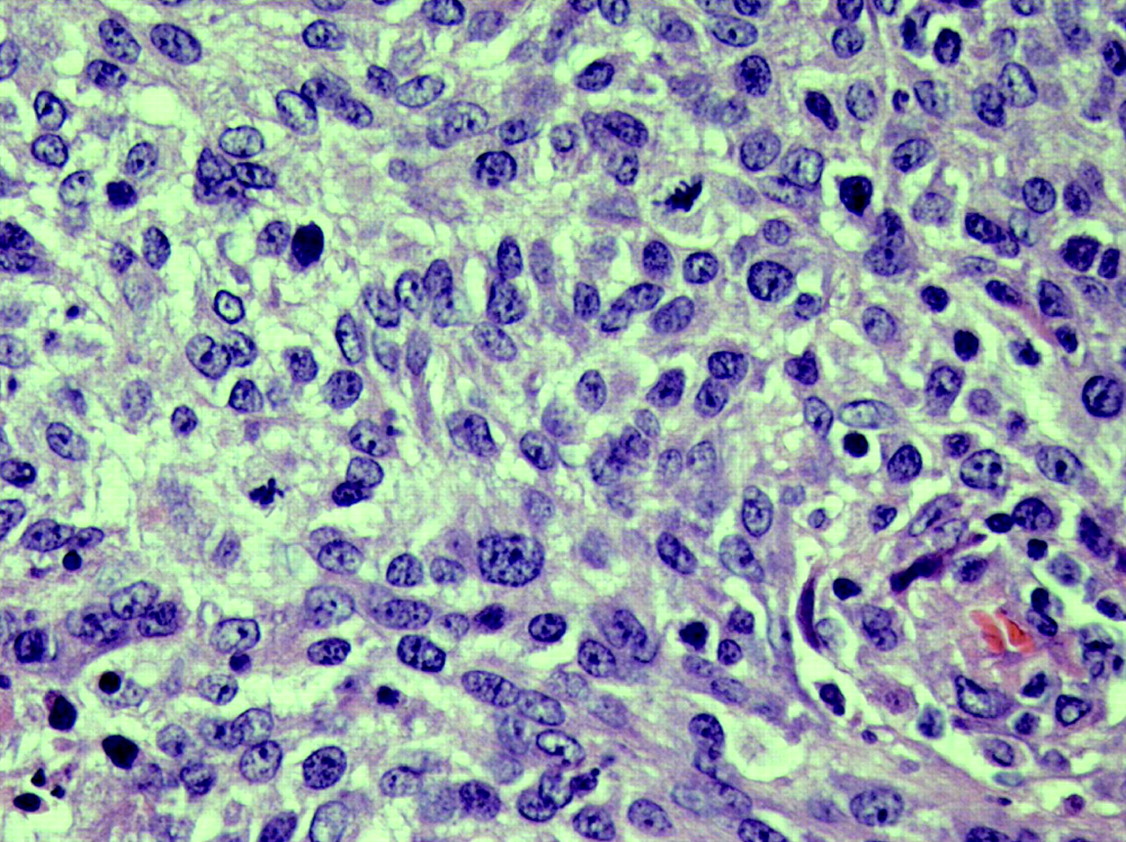
Histologic examination of the excised C6 tumors showed a malignant mesenchymal tumor (Fig. 2). Spindled tumor cells with pleomorphic, hyperchromatic nuclei were arranged in short bundles. Many mitoses were found (range, 25–40 per 2 mm2). Small areas of tumor necrosis were seen, composing less than 10% of the total tumor volume.
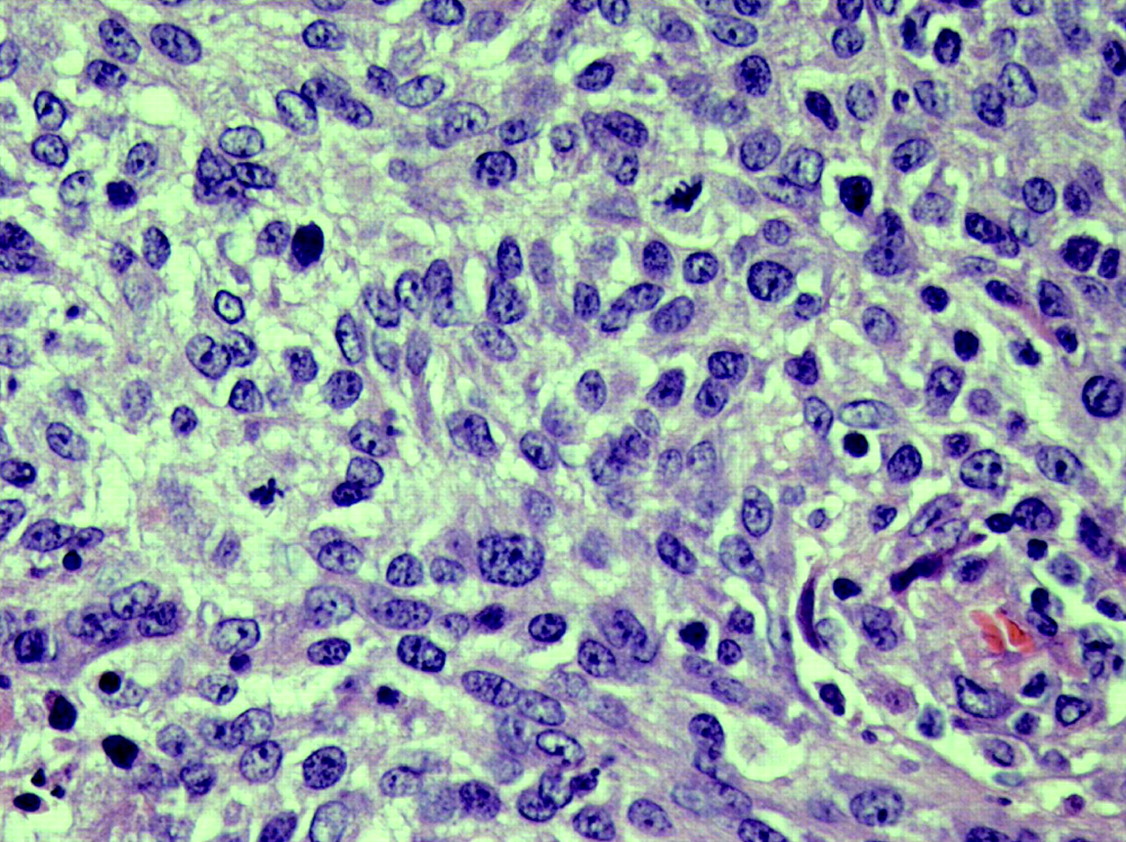
Microscopic image of a specimen of rat tumor, 11 d after inoculation of C6 cells (hematoxylin and eosin, ×400).
PET Images
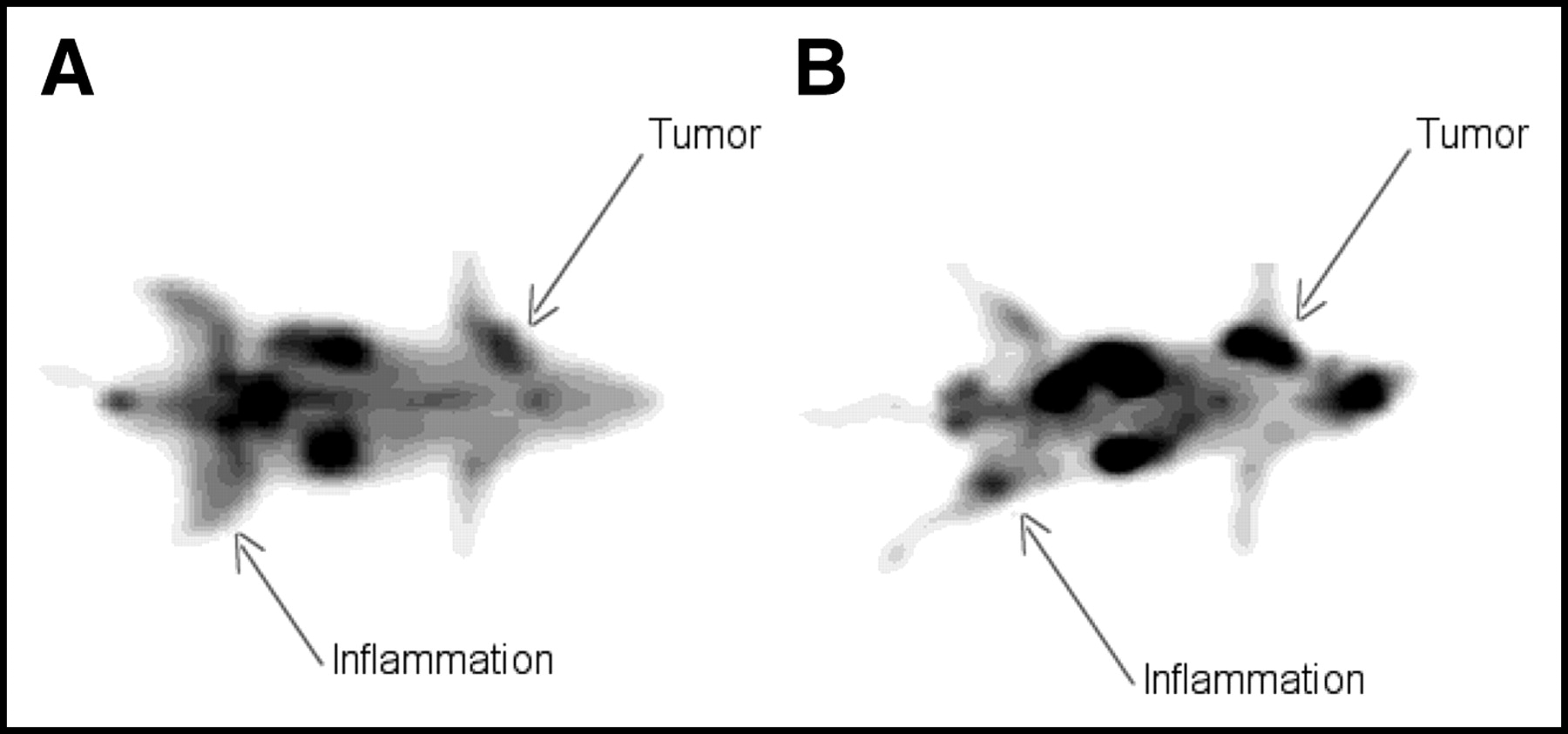
PET images, obtained with the 2 tracers, of tumor- and inflammation-bearing rats are shown in Figure 3. The head of each animal is on the right, and the rats are seen from below. Both 18F-FLT and 18F-FDG clearly revealed the C6 tumor in the right shoulder. 18F-FDG showed high, physiologic uptake in the brain, in contrast to 18F-FLT. The inflammation in the left hind leg was revealed with 18F-FDG but not with 18F-FLT.
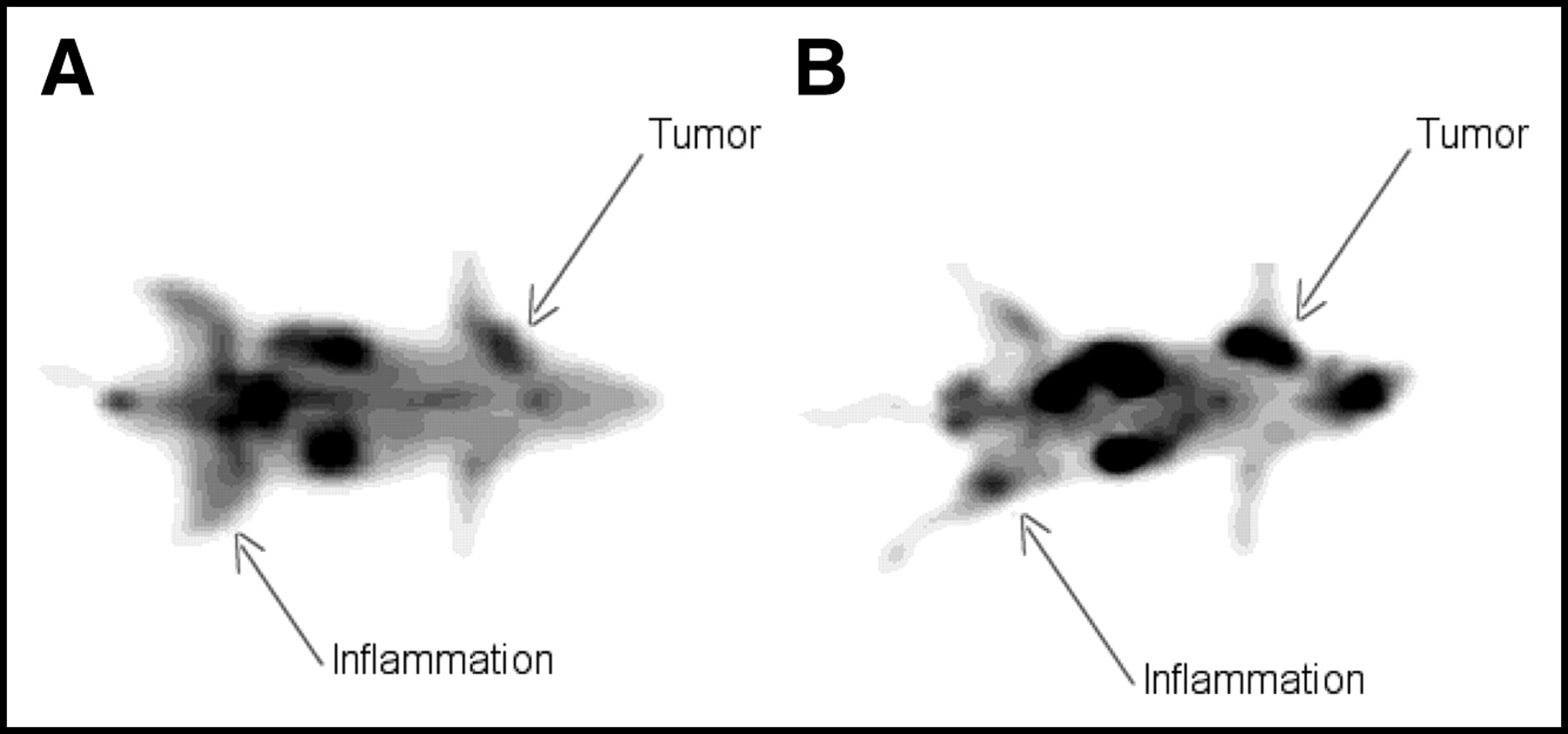
PET images obtained 110–130 min after injection of 30 MBq of 18F-FLT (A) and 18F-FDG (B) into rats. 18F-FLT reveals only the tumor, whereas both tumor and inflammation are visible after injection of 18F-FDG.
DISCUSSION
This study confirmed that the standardized uptake value of 18F-FLT in inflammatory tissue is lower than that of 18F-FDG (Table 1; Fig. 3). Although the tumor uptake of 18F-FLT is also considerably lower than that of 18F-FDG (Table 1), the selectivity of 18F-FLT for tumor versus inflammation is nevertheless higher than that of glucose analog: 10.6- versus 3.5-fold at 120 min after injection, when the data are corrected for background activity (Table 2). Thus, the hypothesis that 18F-FLT has a higher tumor specificity was confirmed in our animal model.
Standardized uptake values of 18F-FDG in C6 tumors were 2-fold higher than those of 18F-FLT. Tumor-to-muscle ratios of 18F-FDG (13.2 ± 3.0) were clearly superior to those of 18F-FLT (3.8 ± 1.3). These results are in accordance with clinical data from 18F-FDG and 18F-FLT PET scans, in which colorectal cancers have been found to display a 2-fold higher standardized uptake value of 18F-FDG than of 18F-FLT (25).
However, 18F-FDG showed relatively poor selectivity for distinguishing tumor from inflammatory tissue. The inflamed thigh was clearly visualized in a PET image (Fig. 3). Tissue uptake of 18F-FDG was 4.8-fold greater in inflamed muscle than in the contralateral healthy leg, and the selectivity index of 18F-FDG for tumor versus inflammation was 3.5 (Table 2). Because only part of the volume of the inflamed muscle samples consisted of neutrophils and macrophages, 18F-FDG uptake in these inflammatory cells may have been >10-fold greater than in normal muscle cells.
18F-FLT showed better tumor selectivity in our model than did 18F-FDG. In a PET image (Fig. 3), the inflamed thigh showed tracer uptake similar to that in the contralateral healthy thigh. Biodistribution studies indicated that accumulation of 18F-FLT in inflamed muscle was not significantly different from that in noninflamed tissue of the contralateral thigh (ratio, 1.3 ± 0.4; Table 2). The selectivity index of 18F-FLT for tumor versus inflammation was 10.6 or greater (Table 2).
In Wistar rats, the glucose analog showed a biodistribution that was expected on the basis of clinical 18F-FDG PET scans, that is, high and physiologic uptake in brain and heart, besides renal excretion and accumulation in urine (Table 1). In contrast to 18F-FDG, 18F-FLT accumulated mainly in bone marrow (Table 1). Low levels of radioactivity in the brain were probably due to the slow transportation of 18F-FLT across the blood-brain barrier or to the low activity of thymidine kinase in the brain.
The data presented in the tables indicate that endogenous thymidine can strongly affect in vivo uptake of 18F-FLT. Low tissue uptake of 18F-FLT in untreated rats is probably a consequence of high levels of endogenous thymidine in rodent serum (26), since previous infusion of thymidine phosphorylase significantly increased uptake of the radiolabeled nucleoside in target organs (Table 1). Thymidine may compete with 18F-FLT for the active site of nucleoside carriers in cell membranes (27) and also for the active site of the trapping enzyme, thymidine kinase 1. The affinity of human thymidine kinase 1 for thymidine has been reported to be 4-fold higher (0.5 μmol/L) than is the affinity for 18F-FLT (2.1 μmol/L) (21).
Apparently, substantial plasma concentrations of endogenous thymidine can suppress 18F-FLT uptake in most tissues (Table 1). In contrast to rats, humans have much (9- to 16-fold) lower levels of serum thymidine (0.01–0.02 μg/mL vs. 0.15–0.27 μg/mL) (26). Therefore, 18F-FLT PET scans of cancer patients show adequate image contrast (19,20,25,28,29).
After infusion of a thymidine-degrading enzyme, physiologic accumulation of 18F-FLT to levels greater than those in plasma was observed in C6 tumors, bone, bone marrow, large and small intestine, and spleen (Table 1). Many of these organs contain rapidly dividing tissue (malignant cells in the tumor, bone marrow in the skeleton, mucosa in the intestines). Thus, in pretreated rats, 18F-FLT behaved as a tracer of cellular proliferation. This finding is in accordance with reports from the literature suggesting a significant correlation between standardized uptake values of 18F-FLT and proliferative activity of various lesions (28,30,31). In vitro studies have shown that 18F-FLT uptake is related to thymidine kinase-1 activity and the percentage of cells in S-phase (16,17). 18F-FDG accumulated in the same rapidly dividing tissues as did 18F-FLT (Table 2) and showed even higher standardized uptake values in tumor and large intestine.
CONCLUSION
In our animal model, 18F-FLT revealed only tumor, whereas 18F-FDG delineated both tumor and inflammation. On the basis of these animal data, 18F-FLT scans of oncologic patients can be expected to show more false-negative findings (because of lower tumor uptake) and fewer false-positive findings (because of negligible accumulation in granulocytes) than do whole-body 18F-FDG scans.
Acknowledgments
We thank Dr. Tony Lahoutte (Free University of Brussels) for valuable information on the turpentine inflammation model; Drs. Anthony F. Shields (Karmanos Cancer Institute), Peter S. Conti, and James R. Bading (University of Southern California) for their suggestion that we lower endogenous thymidine levels by intravenous infusion of thymidine phosphorylase; and Biotechnicians Hans Bartels, Ar Jansen, and Arie Nijmeijer (Central Animal Laboratory, University of Groningen) for expert technical assistance. This work was supported by the Dutch Cancer Society (Koningin Wilhelmina Fonds, KWF, grant 2000-2299)
Footnotes
Received Sep. 23, 2003; revision accepted Dec. 2, 2003.
For correspondence or reprints contact: Philip H. Elsinga, PET Center, Groningen University Hospital, P.O. Box 30001, 9700RB Groningen, The Netherlands.
E-mail: p.h.elsinga{at}pet.azg.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Monitoring Response to Transarterial Chemoembolization in Hepatocellular Carcinoma Using 18F-Fluorothymidine PET
- Depicting Changes in Tumor Biology in Response to Cetuximab Monotherapy or Combination Therapy by Apoptosis and Proliferation Imaging Using 18F-ICMT-11 and 18F-FLT PET
- [18F]CFA as a clinically translatable probe for PET imaging of deoxycytidine kinase activity
- Mapping Radiation Injury and Recovery in Bone Marrow Using 18F-FLT PET/CT and USPIO MRI in a Rat Model
- Predictive Value of Early-Stage Uptake of 3'-Deoxy-3'-18F-Fluorothymidine in Cancer Cells Treated with Charged Particle Irradiation
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- Variability of Proliferation and Diffusion in Different Lung Cancer Models as Measured by 3'-Deoxy-3'-18F-Fluorothymidine PET and Diffusion-Weighted MR Imaging
- Stratification of 18F-Labeled PET Imaging Agents for the Assessment of Antiangiogenic Therapy Responses in Tumors
- Mammary Cancer Bone Metastasis Follow-up Using Multimodal Small-Animal MR and PET Imaging
- Serial Diffusion MRI to Monitor and Model Treatment Response of the Targeted Nanotherapy CRLX101
- Evaluation of 4'-[Methyl-11C]Thiothymidine in a Rodent Tumor and Inflammation Model
- Tumor 3'-Deoxy-3'-18F-Fluorothymidine (18F-FLT) Uptake by PET Correlates with Thymidine Kinase 1 Expression: Static and Kinetic Analysis of 18F-FLT PET Studies in Lung Tumors
- Biodistribution and Uptake of 3'-Deoxy-3'-Fluorothymidine in ENT1-Knockout Mice and in an ENT1-Knockdown Tumor Model
- Novel PET Probes Specific for Deoxycytidine Kinase
- PET/CT with 18F-FLT: Does It Improve the Therapeutic Management of Metastatic Germ Cell Tumors?
- Evaluation of Treatment-Associated Inflammatory Response on Diffusion-Weighted Magnetic Resonance Imaging and 2-[18F]-Fluoro-2-Deoxy-D-Glucose-Positron Emission Tomography Imaging Biomarkers
- In Vitro and In Vivo Properties of Dihydrophthalazine Antifolates, a Novel Family of Antibacterial Drugs
- Kinetic Analysis of 3'-Deoxy-3'-18F-Fluorothymidine (18F-FLT) in Head and Neck Cancer Patients Before and Early After Initiation of Chemoradiation Therapy
- Idiopathic Pulmonary Fibrosis and Diffuse Parenchymal Lung Disease: Implications from Initial Experience with 18F-FDG PET/CT
- The Role of 18F-FDG PET/CT in the Evaluation of Ascites of Undetermined Origin
- Integrin {alpha}v{beta}3-Targeted Radioimmunotherapy of Glioblastoma Multiforme
- Gene Expression Patterns and Tumor Uptake of 18F-FDG, 18F-FLT, and 18F-FEC in PET/MRI of an Orthotopic Mouse Xenotransplantation Model of Pancreatic Cancer
- Imaging of Cell Proliferation: Status and Prospects
- Imaging Bone and Soft Tissue Tumors with the Proliferation Marker [18F]Fluorodeoxythymidine
- Imaging Pharmacodynamics of the {alpha}-Folate Receptor-Targeted Thymidylate Synthase Inhibitor BGC 945
- A Multicenter Clinical Trial on the Diagnostic Value of Dual-Tracer PET/CT in Pulmonary Lesions Using 3'-Deoxy-3'-18F-Fluorothymidine and 18F-FDG
- Preclinical Efficacy of the c-Met Inhibitor CE-355621 in a U87 MG Mouse Xenograft Model Evaluated by 18F-FDG Small-Animal PET
- Usefulness of 11C-Methionine for Differentiating Tumors from Granulomas in Experimental Rat Models: A Comparison with 18F-FDG and 18F-FLT
- 18F-Fluorodeoxythymidine PET for Evaluating the Response to Hyperthermic Isolated Limb Perfusion for Locally Advanced Soft-Tissue Sarcomas
- Evaluation of 4'-[Methyl-14C]Thiothymidine for In Vivo DNA Synthesis Imaging
- 18F-FLT PET in Hematologic Disorders: A Novel Technique to Analyze the Bone Marrow Compartment
- Early Detection of Chemoradioresponse in Esophageal Carcinoma by 3'-Deoxy-3'-3H-Fluorothymidine Using Preclinical Tumor Models
- 18F-FDG PET After Radiofrequency Ablation: Is Timing Everything?
- Molecular Imaging with 123I-FIAU, 18F-FUdR, 18F-FET, and 18F-FDG for Monitoring Herpes Simplex Virus Type 1 Thymidine Kinase and Ganciclovir Prodrug Activation Gene Therapy of Cancer
- Comparison of Sigma-Ligands and Metabolic PET Tracers for Differentiating Tumor from Inflammation
- Reproducibility of 3'-Deoxy-3'-18F-Fluorothymidine MicroPET Studies in Tumor Xenografts in Mice
- Early Detection of Tumor Response to Chemotherapy by 3'-Deoxy-3'-[18F]Fluorothymidine Positron Emission Tomography: The Effect of Cisplatin on a Fibrosarcoma Tumor Model In vivo
- Tumor Imaging with 2 {sigma}-Receptor Ligands, 18F-FE-SA5845 and 11C-SA4503: A Feasibility Study