


Abstract
The first aim of our study was to compare the role of 18F-FDG PET/CT with that of CT alone in detecting the primary cause of ascites. A secondary aim was to compare the value of 18F-FDG PET/CT with that of CT alone in detecting abdominal cavity metastasis. Finally, we analyzed the receiver-operating-characteristic (ROC) curves of maximal standardized uptake values (SUVmax), serum carcinoembryonic antigen, CA19-9, and CA12-5 for differential diagnostic abilities. Methods: The 18F-FDG PET/CT scans of 40 patients with ascites of undetermined origin, including 30 patients with malignant diseases and 10 with benign lesions, were reviewed for the presence of ascites. Among the 40 patients, 34 had received their diagnosis by pathologic examination and 6 by clinical follow-up. We also assessed the 18F-FDG PET/CT scans of 20 healthy volunteers for comparison. All 18F-FDG PET/CT images were visually interpreted, and the SUVmax was measured. We compared the mean diameter of true-positive lesions with that of false-negative lesions. The diagnostic abilities of SUVmax, serum carcinoembryonic antigen, CA19-9, and CA12-5 were compared using the ROC curve. Results: The sensitivity, specificity, and accuracy of PET/CT in detecting the primary cause of ascites were 63.3% (19/30), 70.0% (7/10), and 65.0% (26/40), respectively, and those of CT alone were 36.7% (11/30), 80% (8/10), and 47.5% (19/40), respectively (sensitivity, P < 0.05). The sensitivity of PET/CT was higher than that of CT alone for detecting abdominal cavity metastasis (86.4% vs. 27.3%, P < 0.01). The SUVmax in patients with malignant primary and metastatic lesions was significantly higher than that in healthy volunteers and in patients with benign ascites (P < 0.05). The mean maximal diameter of false-negative lesions was significantly smaller than that of true-positive lesions (P < 0.05). In ROC analysis, the areas under the curve of SUVmax, serum carcinoembryonic antigen, CA19-9, and CA12-5 were 0.803 (P < 0.01), 0.773 (P < 0.05), 0.552 (P > 0.05), and 0.220 (P < 0.01), respectively. Conclusion: 18F-FDG PET/CT assisted in detecting the original cause of ascites. The differential diagnostic ability of 18F-FDG PET/CT was superior to that of CT alone, tumor markers, and cytology. More attention should be paid to peritoneal tuberculosis, which can markedly accumulate 18F-FDG and mimic peritoneal carcinoma.
Ascites is a common clinical problem that can be caused by several different diseases (1–4). Approximately 75% of ascites is secondary to hepatic cirrhosis, 10%−12% of ascites is caused by carcinoma, and 8%−10% is caused by peritoneal tuberculosis, renal disease, or pancreatic disease (1,2). Unfortunately, the differential diagnosis of ascites always leads to confusion and an inability to exclude many of the potential causes in many patients. Serum and fluid biochemical tests, fluid cytology, and peritoneal biopsy have low positive rates. Laparoscopy, although having a higher diagnostic accuracy (82.2%−96.6%) (5), is limited because of its invasiveness and sampling error. Currently, the preoperative imaging procedure of choice for diagnosis of peritoneal metastasis is conventional CT, which has been found to have widely ranging sensitivities: 17% (6) to 54% (7).
18F-FDG PET is a noninvasive diagnostic technique utilizing biochemical metabolic differences between benign and malignant tissues. Integrated PET/CT combines functional imaging and anatomic imaging and has increased diagnostic accuracy. To date, few studies have reported the role of 18F-FDG PET/CT in the evaluation of ascites. This study assessed the role of 18F-FDG PET/CT in determining the cause of ascites and in differential diagnosis.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of patients who were referred for 18F-FDG PET/CT in 2007 or 2008 to determine the primary cause of ascites and differentiate malignant from benign ascites. Forty patients (21 men, 19 women; age range, 24–81 y; mean age ± SD, 55 ± 13 y) with ascites of unknown origin were included. To be included in the study, the patients had to fall into 1 of 3 categories.
Patients in the first category had negative cytology findings for the ascitic fluid and, except for the ascites, negative findings on other noninvasive examinations such as CT, ultrasound, and endoscopy. The primary cause of the ascites was undetermined, and whether the ascites was malignant or benign was uncertain. There were 22 patients in this category of inclusion criteria.
Patients in the second category also had negative cytology findings. Other noninvasive examinations detected abnormal lesions but could not confirm whether they were the primary cause of the ascites or whether the ascites was malignant or benign. There were 13 patients in this category, including patients with low-density lesions in the liver (n = 5), lesions in the pancreas (n = 1), gastrointestinal wall thickening (n = 3), abnormal ovarian enlargement (n = 1), a lung nodule (n = 1), and peritoneal tubercles (n = 2).
There were 5 patients in the third category of inclusion criteria. These patients had cytologic findings positive for malignancy, but noninvasive examinations could not detect the primary cause of the malignancy.
We also retrospectively assessed 18F-FDG PET/CT scans from 20 healthy volunteers for comparison. Written consent to both scans and to review of medical records was obtained from all participating patients. Among the 40 patients, 34 were diagnosed by pathologic examinations and 6 by clinical follow-up. Among the 30 patients with malignant ascites, pathologic examination was able to confirm the presence of primary carcinoma in 26 patients but, even with laparoscopy or laparotomy, failed to find the cause of the malignant ascites in the other 4 patients. Abdominal cavity metastasis was confirmed by pathology in 22 patients with malignant ascites. Among the 10 patients with benign ascites, pathologic examinations confirmed the cause in 4 patients. In the other 6 patients, the cause of the ascites, including peritoneal tuberculosis (n = 4), bacterial peritonitis (n = 1), and hepatic cirrhosis (n = 1), was diagnosed by clinical follow-up over 6 mo. Tissues for pathologic examination were obtained by surgery in 10 patients, puncture biopsy in 12 patients, laparoscopy in 6 patients, and laparotomy in 6 patients. All patients recruited for this study underwent PET/CT, tests of serum tumor markers, and cytologic examination of ascitic fluid.
PET/CT
18F-FDG PET/CT was performed on a Discovery STE16 system (GE Healthcare). The axial field view of this system is 15.6 cm. Patients were required to fast for at least 4 h before undergoing imaging, and the serum glucose level was kept under 7.4 mmol/L. A whole-body image was obtained approximately 50 min after the intravenous administration of 5–6 MBq of 18F-FDG per kilogram of body weight. Six or 7 bed positions that included the head to the thigh were imaged. Emission images were acquired for 3 min per bed position.
CT was performed on the same scanner (Discovery STE16) without contrast administration. The CT scan data were collected with 160–280 mAs (adjusted to the patient's body weight) and a gantry rotation speed of 0.8 s. All CT scans were obtained using 3.75-mm-thick axial sections. Integrated PET and CT images were obtained automatically on Xeleris (GE Healthcare) or Advantage workstations (GE Healthcare).
We compared the PET/CT and the CT diagnostic results.
Visual Interpretation
Any abnormal focal lesion of increased 18F-FDG uptake greater than the surrounding background activity of the organ being examined was interpreted as a possible site of malignant disease, except when gastrointestinal or visceral physiologic uptake was present.
All 18F-FDG PET/CT images were displayed on hard copy and at the workstation. Image interpretation of 18F-FDG PET/CT was based on the consensus of 2 nuclear medicine physicians. 18F-FDG PET manifestations included abnormally intense focal uptake, irregularly distributed intense uptake, nodular or curvilinear uptake in the left subphrenic space, and nodular or curvilinear uptake along the liver surface. We then assessed the diagnostic accuracy of 18F-FDG PET/CT versus CT alone in the detection of original lesions and abdominal cavity metastases.
CT images were displayed as a hard copy and interpreted in a masked fashion. The CT manifestations of the primary origin were evaluated according to the standard CT diagnostic routine. Abdominal cavity metastasis included peritoneal and ascitic fluid metastases; soft-tissue permeation by fatty, nodular to bulky, pancakelike tumors in the abdominal cavity; a stellate pattern in the mesentery; and peritoneal implants along the perihepatic, subdiaphragmatic, anterior, or lateral margins of the abdominal cavity.
Semiquantitative Analysis
The attenuation-corrected images were semiquantitatively analyzed using maximal standardized uptake value (SUVmax). For the semiquantitative analysis, regions of interest measuring 1.0 ± 0.5 cm2 were drawn over the areas of maximal activity in each lesion. The SUV was calculated as (activity in region of interest, in mCi/mL)/(injected dose, in mCi/weight, in kilograms).
Using the Xeleris workstation, we calculated the SUVmax in regions of interest over the area of most intense uptake in patients with malignant ascites, patients with benign ascites, and healthy volunteers.
The method used to measure normal uptake in the abdominal cavity was as follows: On the axial PET/CT scan at the level of the inferior border of the liver, we measured multiple sites in the abdominal cavity, except for areas that showed gastrointestinal and visceral physiologic uptake. We selected the maximal value as the SUVmax for each patient. The SUVmax of the normal abdominal cavity was calculated as the mean + 2 SDs of the SUVmax of the physiologic uptake in 10 healthy volunteers.
Because lesions were always irregular, we measured 3–5 diameters of 1 lesion on the Xeleris workstation and selected the maximal diameter.
Definitions
If a suspected PET/CT (or CT alone) abnormality was confirmed by pathology, the PET/CT (or CT alone) result was defined as true-positive. If a suspected PET/CT (or CT alone) abnormality was not confirmed by pathology, the PET/CT (or CT alone) result was defined as false-positive. If PET/CT (or CT alone) had negative findings but a tumor was later identified, the PET/CT result was defined as false-negative. In 4 cases of malignant ascites with an unknown primary, the PET/CT result was defined as false-negative because metastasis was later confirmed. Especially for detecting primary tumor, if there were multiple hot spots in several organs and it was not possible to define 1 lesion as the most likely primary tumor, the PET/CT result was considered negative (true-negative or false-negative based on the results of pathology or clinical follow-up).
Statistical Analysis
The χ2 test was used to test the sensitivity, specificity, negative or positive predictive value, and accuracy of 18F-FDG PET/CT and of CT alone in detecting primary lesions and abdominal cavity metastases causing ascites. One-way ANOVA was used for analyses of SUVmax for normal peritoneum, benign lesions, abdominal cavity metastases, and malignant primary lesions. The Student t test was used to compare lesion sizes in true-positive and false-negative groups. Correlations between SUVmax and the maximal diameters of lesions were examined by the Pearson test. Differences in continuous diagnostic variables for differential diagnosis of SUVmax, serum carcinoembryonic antigen, CA19-9, and CA12-5 were assessed using receiver-operating-characteristic (ROC) analysis. A higher ROC area under the curve indicates better discriminatory power. All statistical analyses were performed using SPSS software (version 13.0; SPSS Inc.). A P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
Distribution of Primary Sites
Among the 40 patients, 30 were found to have malignant diseases, including gastrointestinal cancer (n = 11), ovarian cancer (n = 5), hepatocarcinoma (n = 5), a malignant disease of unknown primary (n = 4), pancreatic cancer (n = 1), peritoneal mesothelioma (n = 1), lung cancer (n = 1), hepatic lymphoma (n = 1), and a postoperative recurrence of appendix cancer (n = 1). The other 10 patients were found to have benign lesions, including peritoneal tuberculosis (n = 6), bacterial peritonitis (n = 2), hepatic cirrhosis (n = 1), and nephritic syndrome (n = 1).
Detection of Primary Lesions
Among 30 patients with malignant ascites, PET/CT detected the primary lesion for 19 (63.3%). Eleven results were false-negative as confirmed by pathology, including 4 cases of unknown primary (36.4%, 4/11), 3 cases of gastrointestinal signet-ring carcinoma (27.3%, 3/11), 2 cases of ovarian poorly differentiated adenocarcinoma (18.2%, 2/11), 1 case of gastric adenocarcinoma (9.1%, 1/11), and 1 case of peritoneal mesothelioma. There were 3 patients with false-positive results. In the first patient, increased 18F-FDG uptake in the colon and abdominal cavity had been considered to represent colon cancer with abdominal cavity metastasis. But the patient was finally confirmed to have colonitis by colonoscopy and peritoneal tuberculosis by laparoscopy. The second patient showed uptake in the liver and abdominal cavity, suggesting a malignant primary site. However, puncture biopsy confirmed that the uptake was caused by bacterial peritonitis and a hepatic abscess. The third patient showed high peritoneal uptake, which had been thought to be mesothelioma but was finally confirmed by puncture biopsy to be peritoneal tuberculosis.
CT alone was positive for primary lesions in 11 of 30 patients with malignant ascites (36.7%). PET/CT had results discordant with CT alone for primary lesions in 8 of 19 patients with false-negative CT findings, including 5 cases of gastrointestinal carcinoma, 2 cases of ovarian adenocarcinoma, and 1 case of recurrent appendix cancer. For the other 11 patients, PET/CT also had false-negative results, which were concordant with CT alone. Among 3 patients with false-positive PET results, 2 had false-positive CT results. One was a case of peritoneal tuberculosis with colonitis, and the other was a case of bacterial peritonitis with hepatic abscess. CT was true-negative in another case of peritoneal tuberculosis.
Figure 1 shows 1 patient with discordant results for CT and PET/CT. For this patient, the primary tumor was difficult to confirm on CT, whereas PET detected high uptake in the stomach, suggesting a primary tumor, which was finally confirmed by colonoscopy.
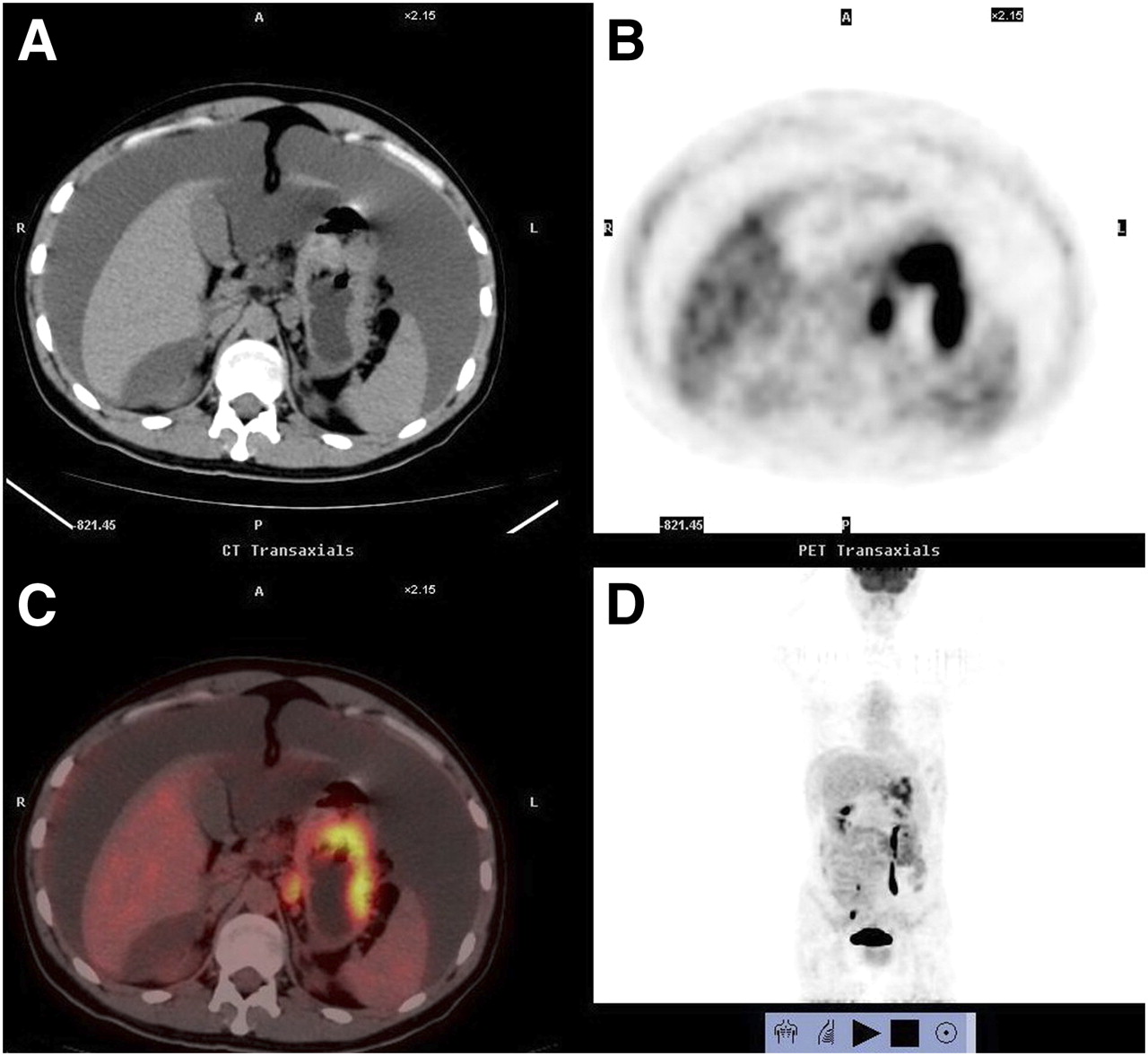
Images of 25-y-old man who presented with ascites for 1 mo: axial CT (A), axial PET (B), axial fused PET/CT (C), and 3-dimensional PET (D). Cytology of ascitic fluid was positive for malignancy, but noninvasive examinations could not detect primary cause of malignant ascites. PET/CT images showed high uptake in gastric area (SUVmax of 8.0, maximal diameter of 6.6 cm). Abdominal cavity metastasis showed smudging sign. After PET/CT examination, gastroscopy was repeated and biopsy confirmed malignant gastric lesion.
The sensitivity, specificity, and accuracy of PET/CT in detecting the primary cause of ascites were 63.3% (19/30), 70.0% (7/10), and 65.0% (26/40), respectively, and those of CT alone were 36.7% (11/30), 80% (8/10), and 47.5% (19/40), respectively (sensitivity, P < 0.05) (Table 1).
Results of CT and PET/CT in Detection of Primary Lesion Causing Ascites
The SUVmax of malignant primary lesions was significantly higher than that of benign lesions (6.45 ± 4.46 vs. 3.49 ± 3.12, P < 0.05) (Fig. 2).
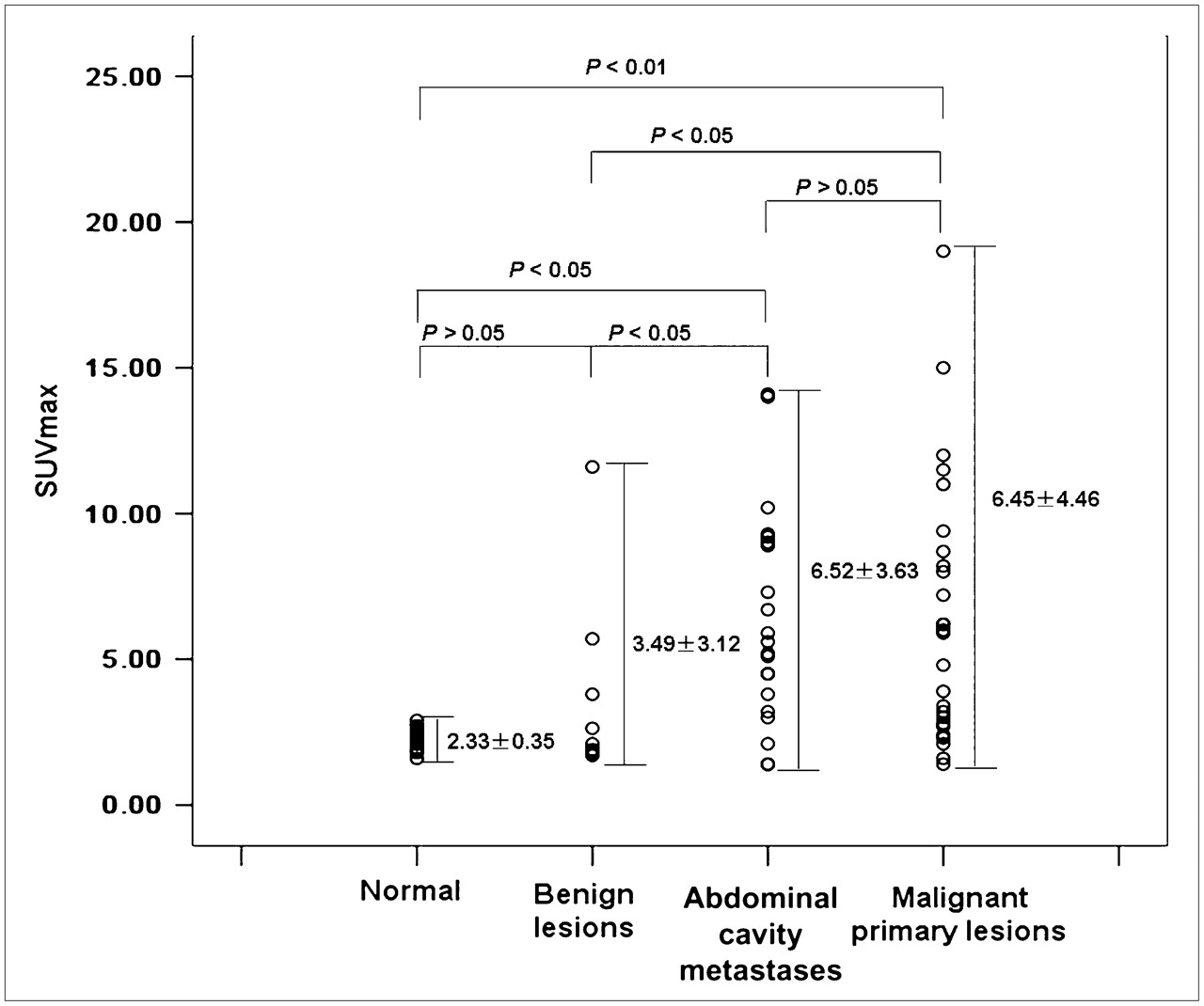
Comparison of SUVmax in peritoneum of healthy volunteers (normal), benign ascites lesions, abdominal cavity metastases, and malignant primary lesions.
The maximal diameter of 19 PET/CT true-positive primary lesions ranged from 1.5 to 18.3 cm, and that of 7 false-negative primary lesions ranged from 1.2 to 3.6 cm. The mean maximal diameter of false-negative primary lesions was significantly smaller than that of true-positive lesions (2.21 ± 0.82 cm vs. 6.65 ± 5.44 cm, P < 0.05).
Detection of Abdominal Cavity Metastasis
Twenty-two patients with malignant ascites had abdominal cavity metastases; 19 cases were detected by PET/CT (86.4%), 6 by CT alone (27.3%), and 5 by a cytologic examination of ascitic fluid (22.7%). The sensitivity of PET/CT was higher than that of CT alone in detecting abdominal cavity metastases (86.4% vs. 27.3%, P < 0.01) (Table 2).
Results of CT and PET/CT in Detection of Abdominal Cavity Metastasis
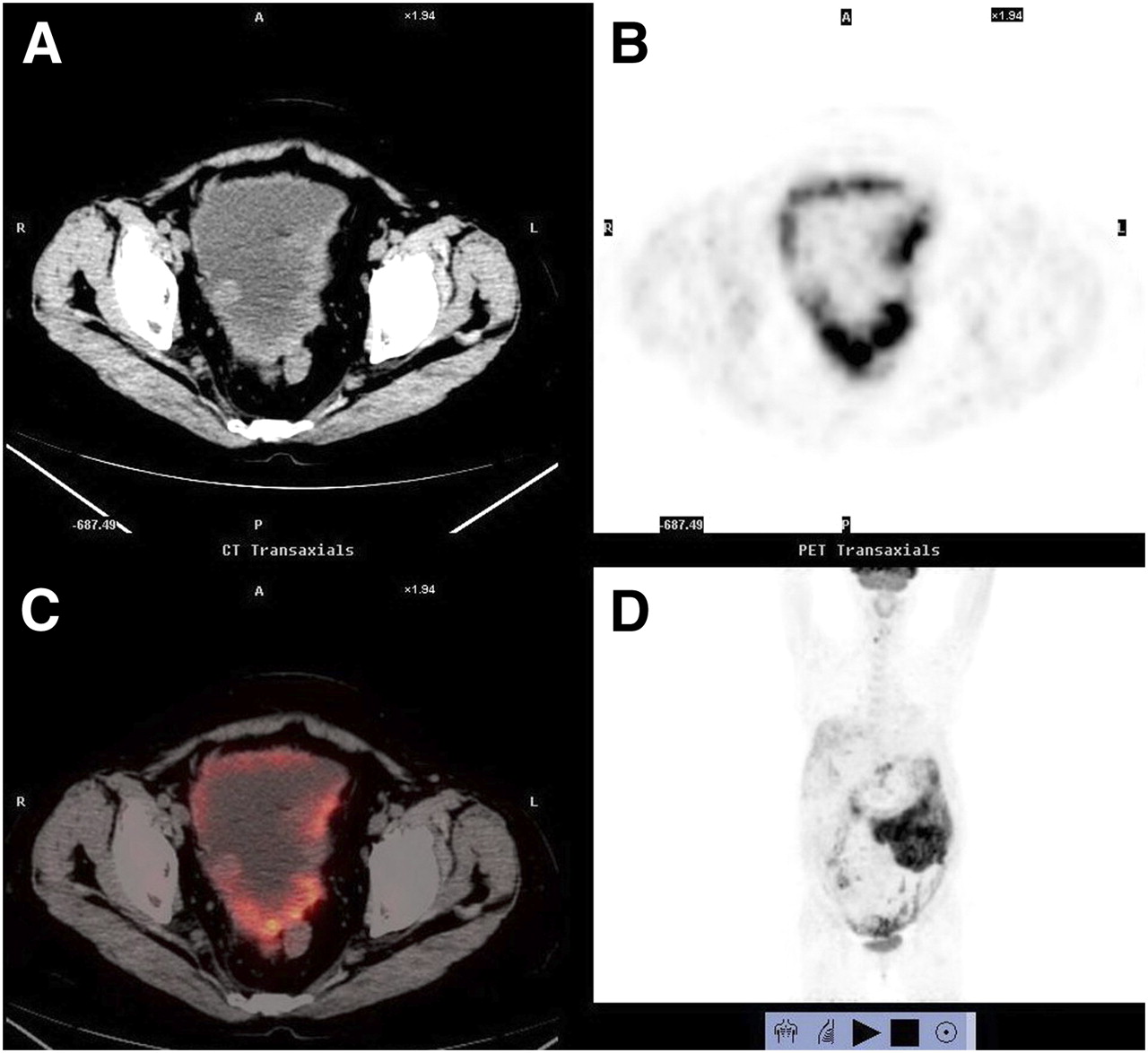
In 7 of these 19 patients with malignant ascites, the primary lesions were negative but abdominal cavity metastases positive on 18F-FDG PET/CT. The PET/CT images of 1 patient with ovarian cancer are shown in Figure 3. In this patient, the primary lesions were negative but abdominal cavity metastases were positive. In 12 patients, both the primary lesions and the metastases were positive. In only 3 patients were both the primary lesions and the metastases negative, including 1 patient with an unknown primary, 1 patient with intestinal signet-ring carcinoma, and 1 patient with gastric adenocarcinoma. Both primary and peritoneal lesions were false-positive in 3 patients, including 1 with peritoneal tuberculosis with colonitis, 1 with bacterial peritonitis with hepatic abscess, and 1 with peritoneal tuberculosis. In 2 patients with peritoneal tuberculosis, uptake of 18F-FDG was high, mimicking peritoneal carcinoma (Fig. 4).
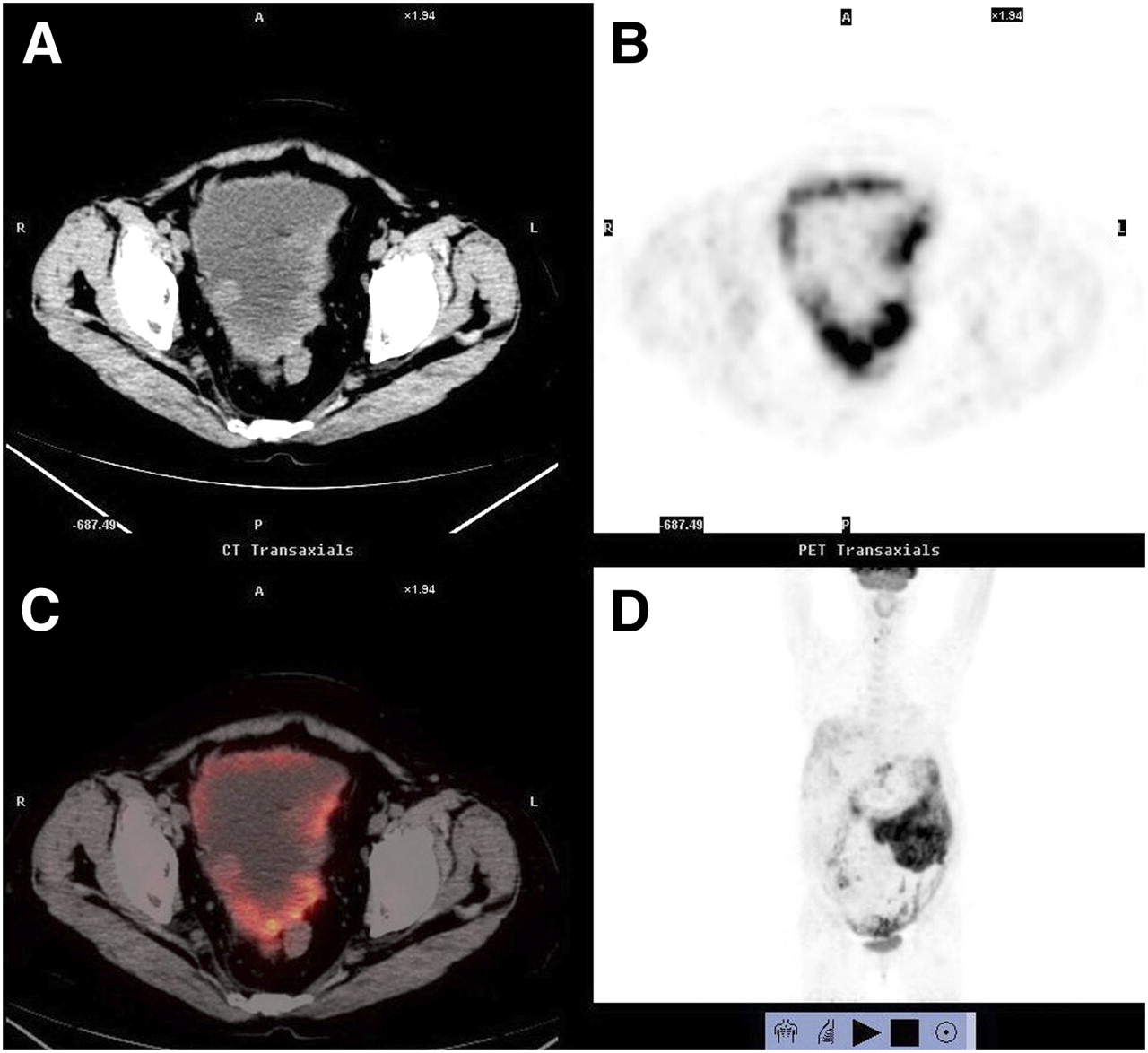
PET/CT images of 65-y-old woman with ascites for 1 mo: axial CT (A), axial PET (B), axial fused PET/CT (C), and 3-dimensional PET (D). Patient had serum CA12-5 of 210 and carcinoembryonic antigen of 10.5. Cytology of ascitic fluid was positive for malignancy, but noninvasive examinations could not detect primary cause. PET/CT failed to find primary cancer but showed diffuse nodular-shadow signs and omental-caking sign. High uptake (SUVmax of 14.1, maximal diameter of 13.1 cm) in abdominal cavity helped to confirm ascites to be malignant. Laparotomy and pathology confirmed that primary cancer and metastases in abdominal cavity were poorly differentiated right ovarian adenocarcinoma.

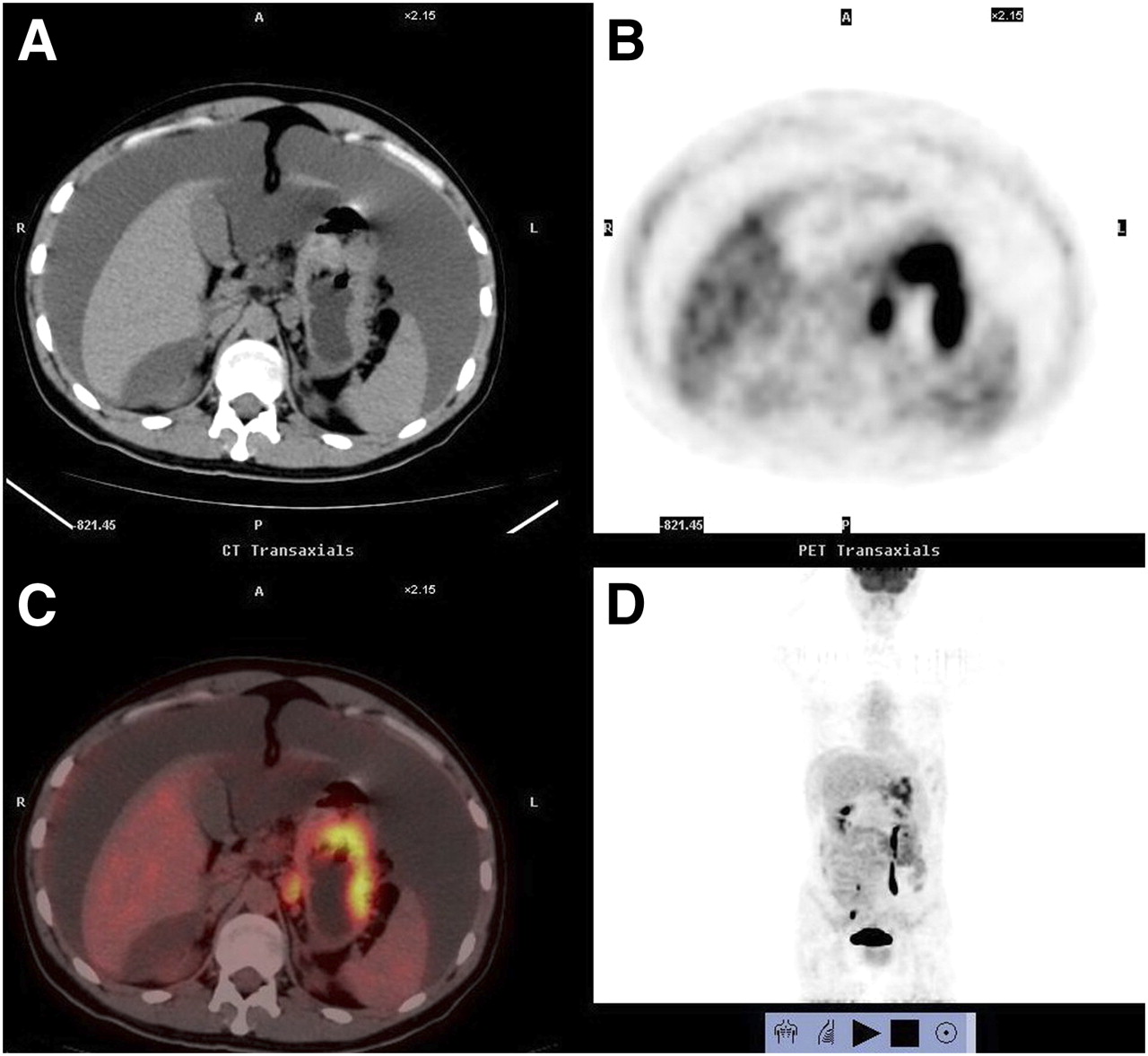
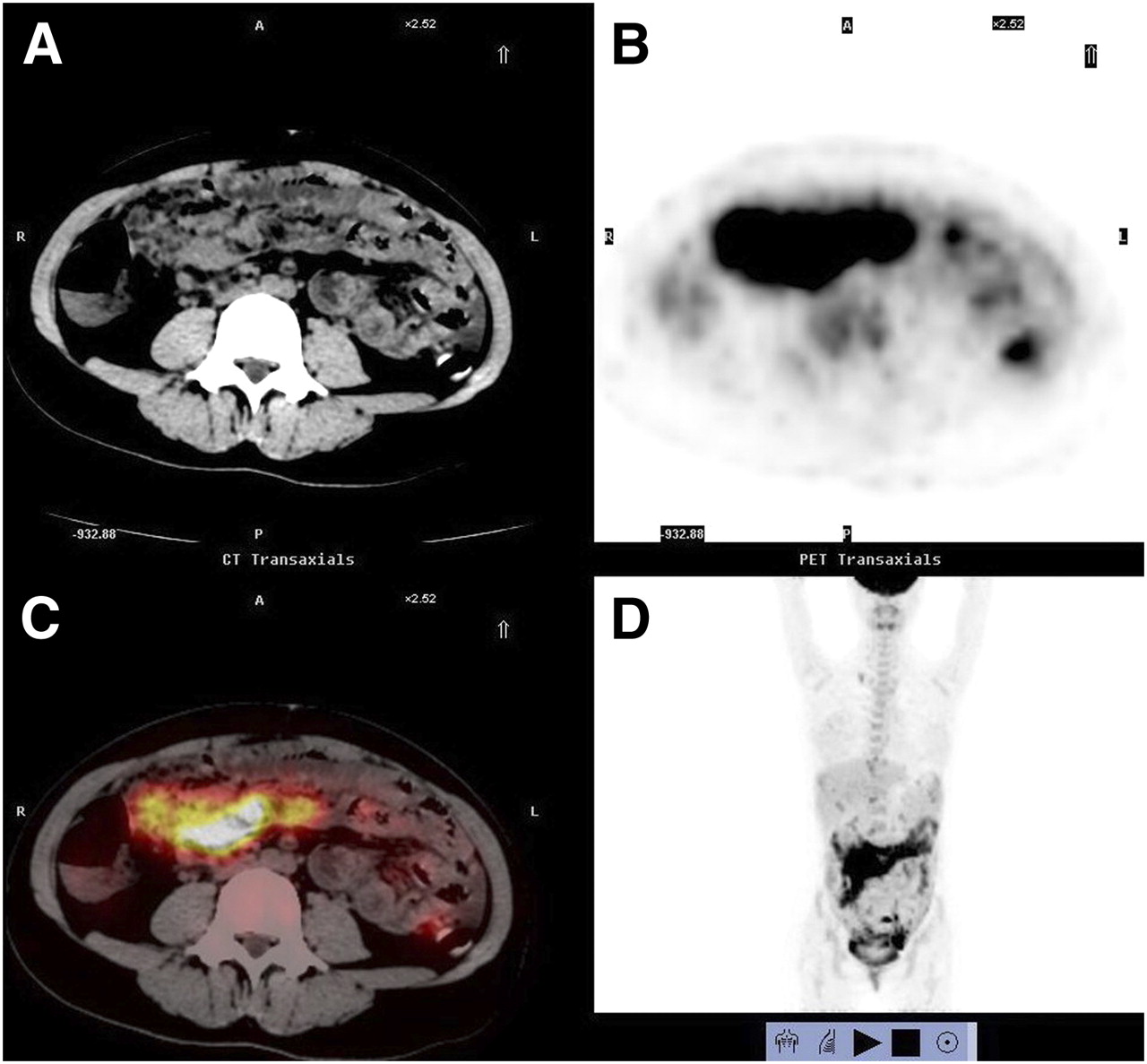
PET/CT images of false-positive case, 32-y-old woman who presented with ascites for 1 mo: axial CT (A), axial PET (B), axial fused PET/CT (C), and 3-dimensional PET (D). Patient had serum CA12-5 of 1,579, normal carcinoembryonic antigen, normal CA19-9, and history of fever and night sweats 3 wk previously. Cytology of ascitic fluid and purified protein derivatives test were negative for malignancy. PET/CT showed diffuse high uptake in abdominal cavity (SUVmax of 11.6, maximal diameter of 17.4 cm) and omental-caking sign, mimicking malignant lesions. Laparoscopy at another hospital confirmed that patient had peritoneal tuberculosis, and she recovered after antituberculosis treatment.
Patterns of Abdominal Cavity Metastasis
On PET/CT images, abdominal cavity metastases demonstrated focal, nodular, or diffuse infiltrative high uptake, forming smudging signs (Fig. 1), nodular-shadow signs (Fig. 3), and omental-caking signs (Fig. 3).
The SUVmax of abdominal cavity metastasis was significantly higher than that of physiologic uptake (in healthy volunteers) (6.52 ± 3.63 vs. 2.33 ± 0.35, P < 0.01) and of benign ascites (3.49 ± 3.12, P < 0.05) (Fig. 2). The SUVmax threshold was calculated as the mean + 2 SDs of the SUVmax of physiologic uptake in healthy volunteers (2.33 + 0.7 = 3.03). Figure 2 shows that the SD of SUVmax was large. The SUVmax of most benign lesions was smaller than 3.0, whereas that of some tuberculosis diseases was much greater (1.5–11.6). In 30 malignant diseases, the SUVmax of most malignant lesions was larger than 3.0 (1.4–14.1), whereas 3 false-negative cases had an SUVmax smaller than 3.0 (1.4, 2.1, and 2.6).
The maximal diameter of the 22 abdominal cavity metastases ranged from 0.5 to 22.3 cm, with a mean of 5.43 ± 5.99 cm. The maximal diameter of the 19 PET/CT true-positive abdominal cavity metastases ranged from 1.1 to 22.3 cm, and that of the 3 false-negative metastases was 0.5, 0.7, and 1.2 cm. The mean maximal diameter of false-negative metastases was significantly smaller than that of true-positive metastases (0.8 ± 0.36 cm vs. 5.53 ± 5.99 cm, P < 0.05). Furthermore, we found a correlation between SUVmax and the maximal diameter of malignant lesions by using the Pearson test (r = 0.600, P = 0.000).
ROC Curves
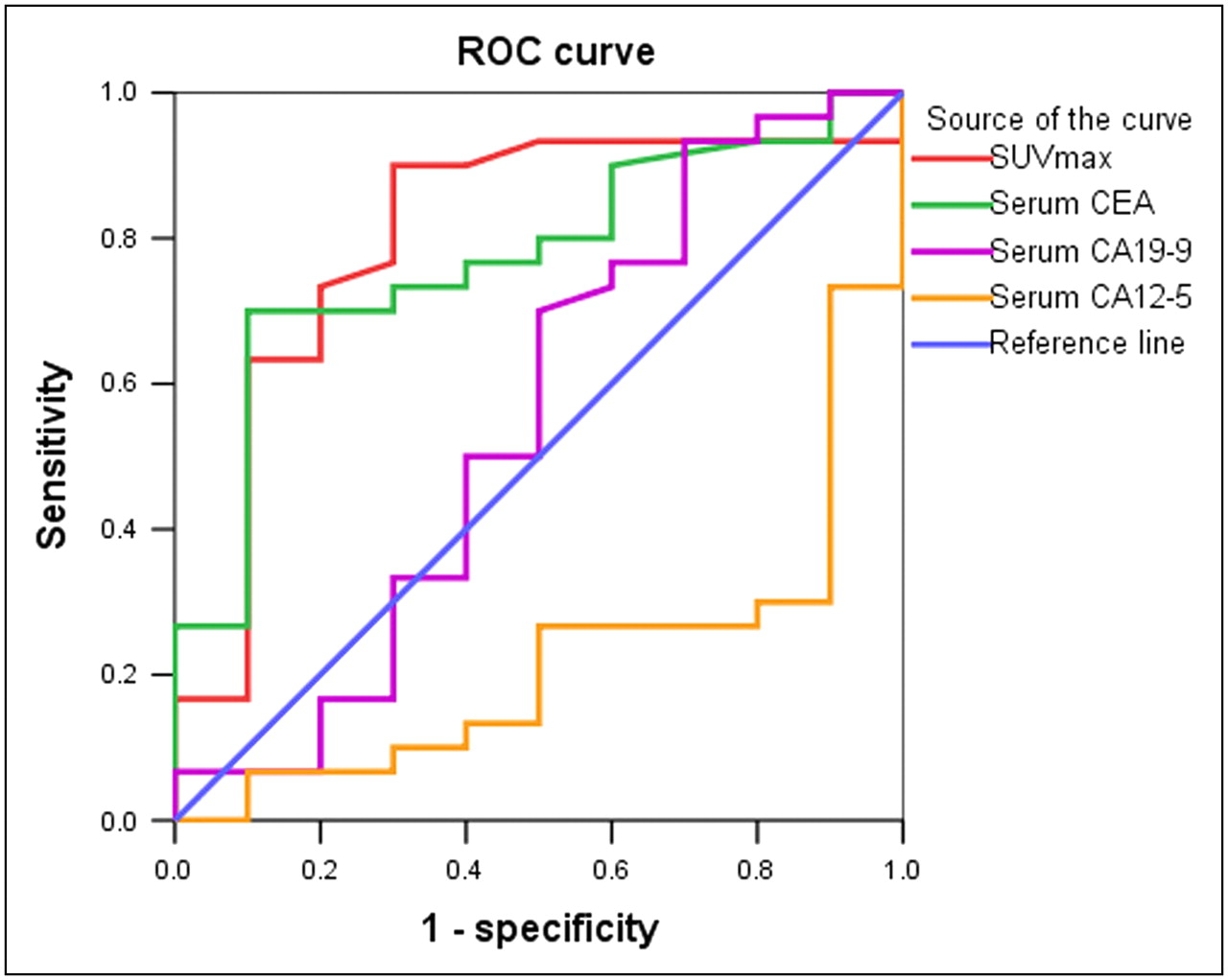
The ROC curves of different modalities for differentiating malignant from benign ascites are shown in Figure 5. In ROC analysis, the areas under the curve of SUVmax, serum CEA, CA19-9, and CA12-5 were 0.803 (P < 0.01), 0.773 (P < 0.05), 0.552 (P > 0.05), and 0.220 (P < 0.01). The area under the curve of PET/CT was the largest (P < 0.01), whereas that of CA12-5 was the smallest (P < 0.01).

ROC curve of SUVmax, serum carcinoembryonic antigen (CEA), CA19-9, and CA12-5 in differential diagnosis of ascites.
DISCUSSION
Value in Detecting Primary Lesions
Ascites may be caused by various diseases. In this study, the most common cause of ascites was gastrointestinal cancer, followed by peritoneal tuberculosis, hepatocarcinoma, and ovarian cancer.
Biochemical tests, cytology, ultrasound, and CT examinations are the most common diagnostic modalities for ascites, but each has some limitations. 18F-FDG PET can be used to detect increased uptake in malignancies. Moreover, ascites is known to be a multisystem disease caused by all kinds of diseases from the entire body. Thus, PET/CT offers the advantage of locating both the primary disease site and metastases because of its high sensitivity in several tumors and its ability to provide whole-body imaging, as previous reports have shown (8–10).
Few published reports have discussed the role of PET/CT in detecting the primary cause of ascites, and most (11–13) have focused on the ability to detect peritoneal carcinomatosis. However, early diagnosis of the primary etiology of malignant ascites is crucial for developing a proper clinical treatment plan and predicting the prognosis. Therefore, we first aimed to evaluate the role of PET/CT in locating the primary disease site of ascites. Previously published reports (8–10) showed that 18F-FDG PET could identify the primary tumor in 6%−55% of patients with metastatic carcinoma of unknown primary. In our study, the sensitivity of PET/CT for detecting the primary lesions of ascites was 63.3%, higher than previously reported. The use of combined PET/CT was the main reason for the increased sensitivity. Accurate anatomic localization of functional abnormalities seen with PET is known to be problematic. Most cases of ascites showed diffused high uptake in abdominal cavity metastases (as shown in Figs. 1 and 3), making it difficult to distinguish primary lesions from metastases. PET/CT helps to distinguish primary lesions from metastases and locates primary lesions accurately.
The sensitivity of PET/CT for detecting primary lesions was also higher than that of CT alone (P < 0.01). PET/CT detected 19 primary lesions (63.3%), whereas CT found only 11. For 8 patients, including 5 with gastrointestinal cancer, 2 with ovarian adenocarcinoma, and 1 with recurrent appendix cancer, PET/CT was true-positive in detecting the primary cause but CT alone failed to find the lesions. The sensitivity of CT was impaired by gastrointestinal motility, bowel feces, and limited density resolution (11,14). PET/CT was of great help under such conditions.
However, PET/CT still had false-negative or false-positive results. In our study, PET/CT had 11 false-negative results for primary lesions. The sensitivity of PET/CT depends on the level of 18F-FDG accumulation in the tumor, the size of the tumor, and the signal-to-nose ratio. On this basis, the false-negative findings in this study likely had 3 causes. First, we identified particular histologic subtypes exhibiting poor accumulation of 18F-FDG and causing false-negative findings. Eleven false-negative results in detecting primary tumors were in cases of signet-ring carcinoma, adenocarcinoma, poorly differentiated ovarian adenocarcinoma, and mesothelioma. One reason for low uptake in these cases is low expression of glucose transporter 1 (15), a low ratio of hexokinase to glucophosphatase. Second, our study showed that the size of the tumor also affected the sensitivity of PET/CT in detecting the primary etiology. The mean maximal diameter of false-negative primary lesions was significantly smaller than that of true-positive lesions (2.21 ± 0.82 cm vs. 6.65 ± 5.44 cm, P < 0.05). Previous reports and our study showed that 18F-FDG accumulation in tumors correlated with tumor size (16). The false-negative rate increased as tumor size decreased (17). Third, PET/CT may have failed to find primary lesions because tumors grew slowly or their growth was restricted by the immune system. In our study, the primary lesions in 4 cases of malignant ascites were not detected even by laparotomy.
There were 3 false-positive results, including 1 case of colonitis, 1 hepatic abscess, and 1 case of tuberculosis. Our study showed that increased glucose metabolism by inflammatory tissues was the main source of false-positive 18F-FDG PET findings. 18F-FDG accumulated at sites of infection, inflammation, and granulomatous diseases by overexpression of distinct facultative glucose transporter isotypes (mainly glucose transporters 1 and 3) and by an overproduction of glycolytic enzymes in inflammatory cells (18,19).
Value in Detecting Abdominal Cavity Metastases
PET/CT has an advantage in detecting the primary cause of ascites, although in some cases the primary lesions do not accumulate 18F-FDG, and differential diagnosis is then first required. For this reason, we evaluated differential diagnosis with PET/CT and considered not only malignant ascites but also benign ascites, especially tuberculosis. Previous reports (11–13) focused on peritoneal carcinomas and did not consider benign lesions.
The sensitivity of PET/CT was higher in detecting abdominal cavity metastases than in detecting primary lesions. In 7 patients with malignant ascites in our study, differential diagnosis was aided by the fact that the primary lesions did not accumulate 18F-FDG but abdominal cavity metastases did. If PET/CT showed a marked accumulation of 18F-FDG in abdominal cavity metastases, we could correctly diagnose malignancy regardless of whether a primary lesion was found.
The sensitivity of PET/CT in our study was 86.4%, higher than in previous studies. Suzuki et al. (12) and Turlakow et al. (13) reported that the sensitivity of peritoneal metastasis detection with PET plus CT ranged from 66.7% to 78%. One reason for increased sensitivity in our study was application of a different scan modality—the third difference from previous studies. Patients in our study underwent PET/CT examination with the same equipment and at the same time. Acquiring both CT and PET images on the same scanner obviates software registration and accurately aligns anatomic and functional images in a single scan. Previous studies (11–13) performed PET and CT examinations separately using different equipment and with a time lag between the CT and PET acquisitions, affecting sensitivity. Another reason for the increased sensitivity in our study was that we took advantage of combining history, tumor markers, and other imaging and clinical data to increase diagnostic accuracy.
Our results showed that the sensitivity of PET/CT in detecting abdominal cavity metastases was also affected by tumor size. The mean maximal diameter of false-negative metastases was significantly smaller than that of true-positive metastases (P < 0.05).
Besides abdominal cavity metastases, some benign diseases can also accumulate 18F-FDG and can cause false-positive results. Our study had 3 false-positive results, including 2 cases of peritoneal tuberculosis and 1 case of bacterial peritonitis. Peritoneal tuberculosis showed a high uptake of 18F-FDG, mimicking peritoneal carcinoma, as previously reported (20–22). One case of peritoneal tuberculosis is shown in Figure 4. In tuberculosis, 18F-FDG PET is expected to show positive findings because the cellular infiltrate is composed mainly of lymphocytes and macrophages. These activated inflammatory cells have a marked increase of glycolysis because the hexose monophosphate shunt is stimulated by phagocytosis (20–22).
The mechanisms of abdominal cavity metastasis are still controversial: previous studies (4,13) have reported that metastases disseminate throughout the peritoneum in several ways, such as direct spread along the peritoneal ligaments, mesentery, and omentum; seeding through the ascites; lymphatic extension; and embolic hematogenous spread.
A few reports have described characteristic 18F-FDG PET images of patients with abdominal cavity metastasis (11–13). Characteristic images have been said to exhibit focal, nodular, or diffuse infiltrative high uptake, as this study showed, forming smudging signs (Fig. 1), nodular-shadow signs (Fig. 3), and omental-caking signs (Fig. 3).
SUVmax Distribution
SUVmax is a semiquantitative index indicating glucose consumption. SUVmax analysis may help in the differentiation of malignant ascites from benign ascites, because the SUVmax of malignant ascites is significantly higher than that of physiologic peritoneal uptake (in healthy volunteers) and benign ascites. However, we found the SD of SUVmax in malignant diseases to be large and to overlap in benign and malignant ascites, indicating the complexity and difficulty of PET/CT diagnosis. The SUVmax in some tuberculosis diseases was high (Fig. 4). Furthermore, SUVmax correlates with tumor size (P < 0.01).
ROC Curve Analysis
PET/CT also exhibits false-negative (or -positive) results, and thus, combining PET/CT with other examinations, such as tumor markers, may be helpful under certain conditions. We compared PET/CT with other examinations by ROC as one of our innovations. The area under the curve of SUVmax was the largest, whereas that of CA12-5 was the smallest, indicating that PET/CT had the best discriminatory power. Six tuberculosis patients had an elevated CA12-5 level in this study, as is consistent with previous reports showing that the presence of ascites and high levels of CA12-5 do not necessarily indicate malignant lesions in reproductive women (21,22). Under such conditions, serum carcinoembryonic antigen may be helpful in the differential diagnosis.
CONCLUSION
We found that 18F-FDG PET/CT, although having limitations such as a high cost, facilitated differential diagnosis and detection of the original cause of ascites. However, in our study, the use of PET/CT allowed for correct diagnosis and timely treatment of many patients—advantages that, in the long run, will lower costs and benefit patients.
Acknowledgments
We thank Professor Bingshun Wang from the Biostatistics Department of Shanghai Jiaotong University School of Medicine for help with statistical analysis. This work was supported by Shanghai Leading Academic Discipline Project S30203.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 27, 2008.
- Accepted for publication December 19, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}