


Abstract
It is well known that 18F-FDG PET has a high average false-negative rate of 40%–50% in the detection of hepatocellular carcinoma (HCC). This is not an acceptable accuracy, particularly in countries where this tumor is prevalent. In this study, we evaluated prospectively the characteristics of 11C-acetate and 18F-FDG metabolism in HCC and other liver masses. Methods: Fifty-seven patients were recruited into this study, with masses consisting of 39 HCC; 3 cholangiocarcinomas; 10 hepatic metastases from lung, breast, colon, and carcinoid primary malignancies; and 5 benign pathologies, including focal nodular hyperplasia (FNH), adenoma, and hemangioma. All patients, except 2 with typical findings of hemangioma and 3 clinically obvious metastases, were confirmed histopathologically by liver biopsy or resection. All patients fasted for at least 6 h and blood glucose concentration was measured before they underwent dual PET radiopharmaceutical evaluation of the upper abdomen with 11C-acetate and 18F-FDG. Results: In the subgroup of HCC patients with the number of lesions ≤ 3 (32 patients; 55 lesions; mean size ± SD, 3.5 ± 1.9 cm), the sensitivity of detection by 11C-acetate is 87.3% (11C-acetate maximum SUV [SUVmax] = 7.32 ± 2.02, with a lesion-to-normal liver ratio of 1.96 ± 0.63), whereas the sensitivity of detection by 18F-FDG is only 47.3%, and 34% lesions show uptake of both tracers. None of the lesions was negative for both tracers (100% sensitivity using both tracers). In some lesions and in the subgroup of HCC patients (n = 7) with multifocal or diffuse disease, dual-tracer uptake by different parts of the tumor is demonstrated. Histopathologic correlation suggests that the well-differentiated HCC tumors are detected by 11C-acetate and the poorly differentiated types are detected by 18F-FDG. All 16 non-HCC malignant (cholangiocarcinoma and metastatic) liver lesions do not show abnormal 11C-acetate metabolism. Of the benign liver lesions, only FNH shows mildly increased 11C-acetate activities (11C-acetate SUVmax = 3.59, with a lesion-to-normal liver ratio of 1.25). Conclusion: 11C-Acetate has a high sensitivity and specificity as a radiotracer complementary to 18F-FDG in PET imaging of HCC and evaluation of other liver masses.
Hepatocarcinoma (HCC) is 1 of the top 3 causes of cancer death in many Asian countries, including China, Taiwan, Singapore, and Japan. The disease is also believed to be showing an upward trend in America because of the increasing frequency of hepatitis C viral infection (1), and it is also a common cause of cancer death among Asian immigrants. The predisposing factors include hepatitis B antigen carrier status, chronic hepatitis C, cirrhosis, alcohol, and other hepatotoxins. Basic investigation includes a screening blood test for elevated α-fetoprotein concentration. The conventional method of detection for HCC is by structural imaging, most commonly and economically by sonography, followed by contrast CT and MRI (2–4). In the past decades, the use of PET, with 18F-FDG as the functional probe, has been found to be successful in the evaluation of many forms of solid malignancies. However, it is well known that 18F-FDG is far from being a universal tracer on the basis of the understanding that tumor kinetics may vary and increased glycolysis may not be the preferred kinetic pathway in some tumors. It is understood that HCC is one of the known tumors that may exhibit a net glycolysis similar to or even lower than that of normal liver parenchyma and therefore may escape detection (5–13). The average reported false-negative rate using 18F-FDG PET in HCC approaches 40%–50% (6,10,11,14). In countries where this tumor is prevalent, this low sensitivity has been a major weakness of 18F-FDG PET in the evaluation of liver masses. Several research studies in the recent years have demonstrated that 11C-acetate may be a useful tracer for urologic tumors (15,16). Because there are no data in the literature regarding the use of this tracer in liver masses, this study was designed to evaluate prospectively the characteristics of 11C-acetate metabolism in HCC and some selective liver pathology. Its potential use as a radiotracer complementary to 18F-FDG in the detection of HCC was investigated.
MATERIALS AND METHODS
Patients
Fifty-seven patients (37 men, 20 women; age range, 27–88 y; mean age, 60 y) with liver masses were recruited into this study, with masses consisting of 39 HCC, 3 cholangiocarcinomas (primary adenocarcinoma), 2 metastases from lung, 3 metastases from colon, 2 metastases from breast, 3 metastatic carcinoid tumors, 2 focal nodular hyperplasia (FNH), 1 adenoma, and 2 hemangiomas. All patients, except 2 with typical findings of hemangioma and 3 clinically obvious metastases, were confirmed histopathologically by liver biopsy 1–3 wk before or after PET imaging or by operative tumor resection. All patients underwent PET imaging of the upper abdomen with 11C-acetate and 18F-FDG on the same day or within 7 d between the 2 scans. All patients fasted for at least 6 h and blood glucose concentration was measured before imaging. Forty patients were hepatitis B antigen positive.
11C-Acetate Synthesis, Injection, and Imaging
11C-Acetate was prepared by modifying the methodology and setup proposed by Norenberg et al. (17). A dose of 555 MBq (15 mCi) 11C-acetate was administered intravenously, and regional imaging of the upper abdomen in 2 positions was performed at 10 min after injection using an ECAT EXACT 47 PET scanner (model 921; CTI/Siemens, Inc., Knoxville, TN). The axial field of view was 16.2 cm. Both transmission and emission scans were obtained with a total of 10-min acquisition time for each position. Attenuation correction was performed with the standardized ordered-subsets expectation maximization technique. Reconstructed transaxial spatial resolution was about 4.4 mm. These images were compared with the anatomic images (CT or MRI).
18F-FDG Synthesis, Injection, and Imaging
18F-FDG synthesis was based on the standard technique of Hamacher et al. (18) (CTI Corp. chemical synthesizer). A dose of 37–555 MBq (10–15 mCi) 18F-FDG was injected intravenously. For those patients undergoing the same-day protocol, 18F-FDG was injected at 10–15 min after 11C-acetate imaging (40–45 min after initial 11C-acetate injection). Regional imaging of the upper abdomen of the same patient began at 45–60 min after 18F-FDG administration. This allowed a total of 85–105 min after the initial injection of 11C-acetate—thus, >4–5 decay half-lives of 11C (20 min). For the first few cases with positive 11C-acetate uptake in the tumor lesions, imaging at 85–100 min before 18F-FDG injection was performed to confirm little or no significant residual activities before this technique was adopted for all subsequent patients (the most intense pancreatic uptake of 11C-acetate was not seen on all 18F-FDG PET images). Instrumentation, imaging, reconstruction, and semiquantitative analysis were similar to the specifications as stated above.
Interpretation Criteria and Statistical Analysis
The hepatic masses were referred to the CT or MR images for lesion-to-lesion comparison. A lesion was regarded as positive for 18F-FDG or 11C-acetate on the basis of visual judgment of the degree of increased metabolism, supported by calculation of the standardized uptake value (SUV). A lesion was considered negative for the PET tracer (18F-FDG or 11C-acetate) when it was isointense with nontumor tissue by visual inspection, supported by a lesion-to-liver SUV ratio of <1.20. Both maximum and average values were calculated. The region of interest (ROI) was drawn automatically at 75% threshold of the maximum lesion count around the tumor. The same ROI was used to evaluate the SUV of nontumor liver tissue in the same patient. For those patients whose lesion was seen with only 1 type of PET tracer, the same ROI was applied at the same level on the transaxial images of the other PET tracer after direct visual alignment of both sets of images. For the subgroup of patients with multifocal or diffuse disease, the ROI was drawn either automatically or manually around the representative lesions or areas. In some of these patients with advanced or infiltrative disease, semiquantitative evaluation was not possible or was possible only in some lesions, and nontumor tissue could be defined only as liver tissue with no apparent tumor on CT or MRI and on PET imaging. The biopsy sites were identified if biopsies were performed before PET imaging. Statistical analysis with an unpaired Student t test was performed on (a) the 11C-acetate-positive HCC lesions to check for any significant difference with the benign lesions, (b) the non-HCC malignant lesions with normal liver tissue, and (c) the average lesion-to-liver ratios among the HCC patients with ≤3 tumor lesions (group Ia, as defined below) according to cellular differentiation. Partial-volume effect correction was not performed because only 3 lesions in this study were between 1.7 and 2.0 cm in size.
RESULTS
These 57 patients were divided into 3 groups: Group I consisted of 39 patients with biopsy-confirmed HCC; group II consisted of 13 patients with non-HCC malignancies (3 cholangiocarcinomas, 10 secondary tumors in liver); group III consisted of 5 patients with benign liver lesions (hemangioma, adenoma, FNH). Group I patients were further subdivided into 2 groups: group Ia (n = 32), those patients who had ≤3 lesions and disease was confined within the hepatic parenchyma; and group Ib (n = 7), those patients with >3 lesions, including those with diffusely infiltrating or multifocal disease, vascular invasion, and extrahepatic metastasis.
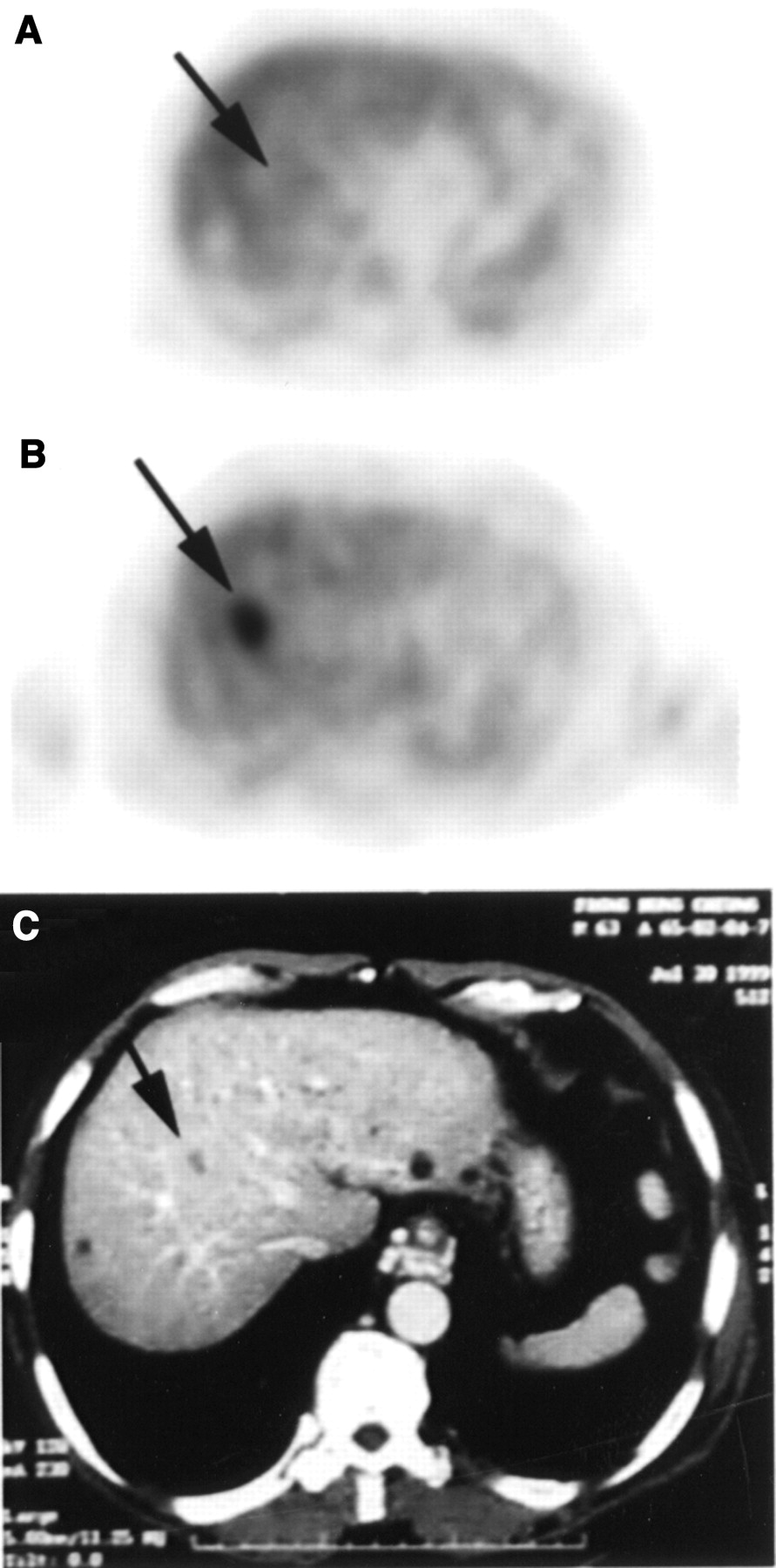
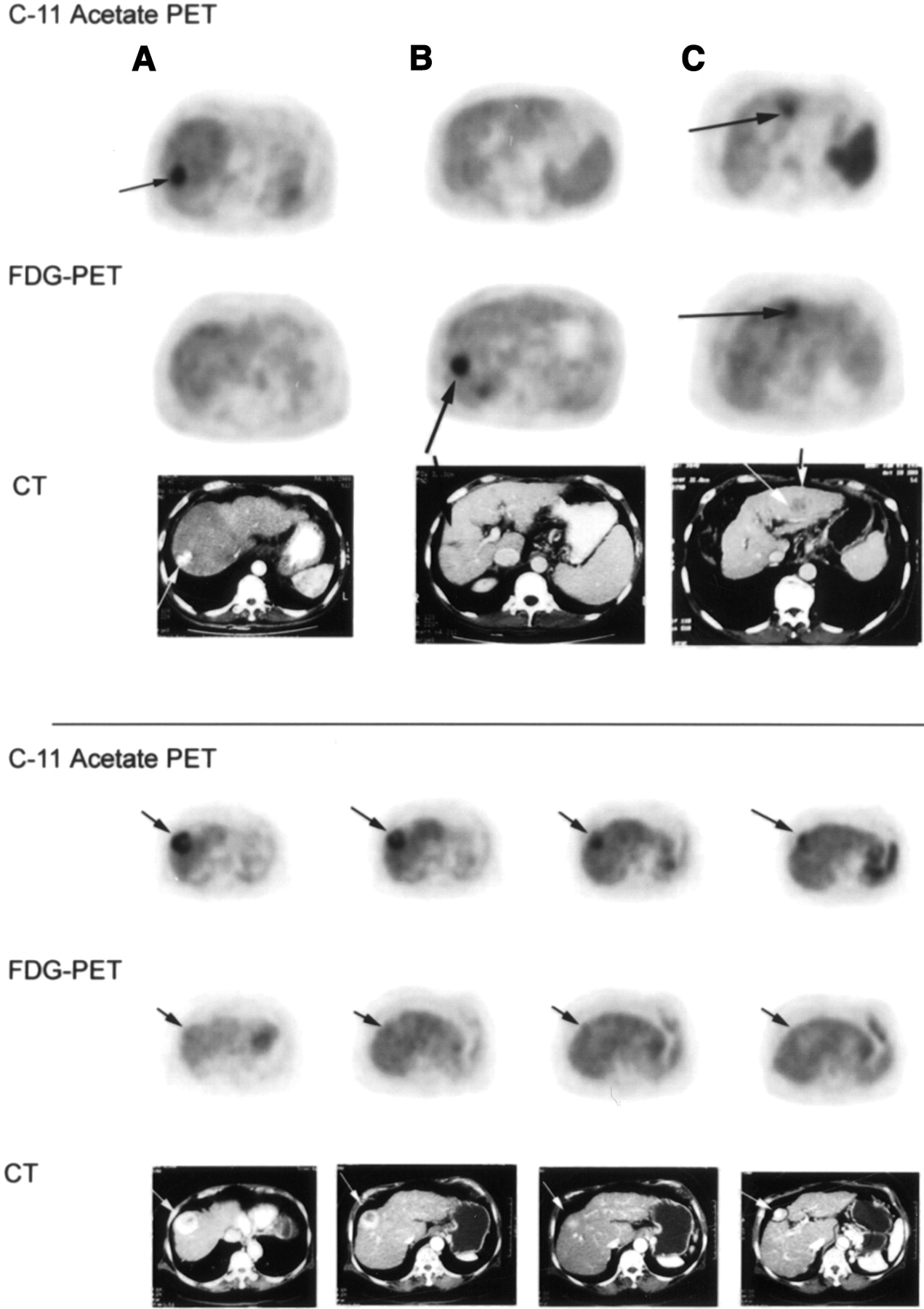
In group Ia, there were 32 patients with a total of 55 hepatic lesions. Of these 55 HCC lesions, 29 were positive only for 11C-acetate (Fig. 1A), 7 were positive only for 18F-FDG (Fig. 1B), and 19 were positive for both (Fig. 1C). Lesion size ranged from 1.7 to 11.1 cm (mean size, 3.5 ± 1.9 cm). On the basis of this subgroup statistics, the sensitivity for detection of HCC by 11C-acetate was 87.3% (lesions positive only for 11C-acetate plus lesions positive for both 11C-acetate and 18F-FDG; n = 48). Whereas for 18F-FDG, the sensitivity for detection of HCC was only 47.3% (lesions positive only for 18F-FDG plus lesions positive for both; n = 26). Results are summarized in Table 1. About 34.5% (n = 19) of these HCC lesions showed increased metabolism of both radiotracers, and some lesions appeared to be complementary (different tracer uptake in different parts of the same tumor lesion, as shown in a patient in Fig. 2). The average 11C-acetate maximum SUV [SUVmax] in group Ia HCC lesions was 7.32 ± 2.02 (mean ± SD; range, 4.11–13.28), with an average lesion-to-liver ratio of 1.96 ± 0.63 (SE = 0.11 at t0.025).

Transaxial sections of liver in 4 patients compare 11C-acetate PET with 18F-FDG PET and CT. (Top) Left patient (A) has well-differentiated HCC in right lobe that shows markedly increased 11C-acetate metabolism but no 18F-FDG accumulation. Middle patient (B) has poorly differentiated HCC in right lobe that shows moderately increased 18F-FDG metabolism and only minimal 11C-acetate activities. Right patient (C) with moderately differentiated HCC in left lobe shows dual tracer uptake. (Bottom) Transaxial sections of liver in another typical patient with HCC show 2 tumor lesions negative on 18F-FDG PET but clearly identified by 11C-acetate PET.

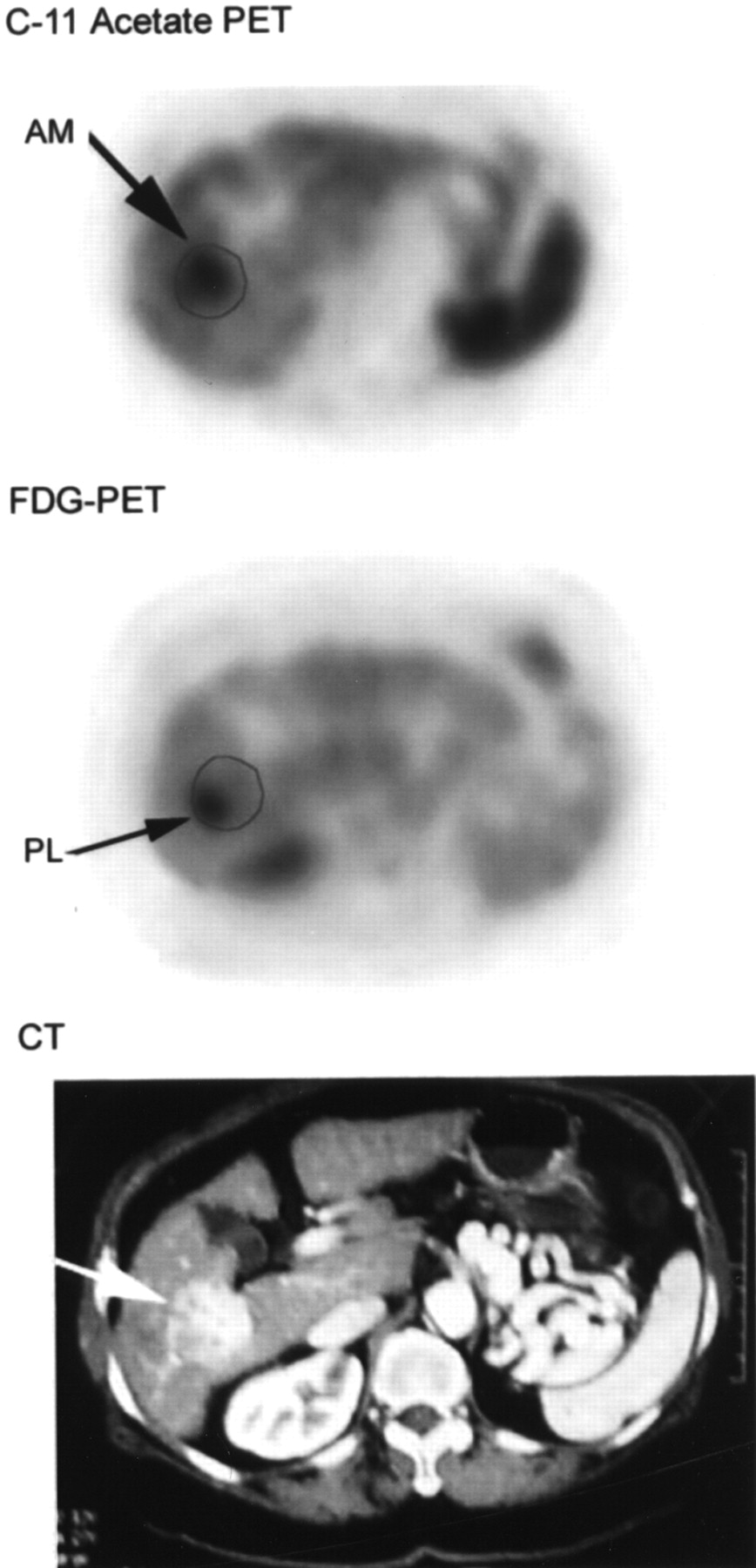
Transaxial sections of liver in patient with moderately differentiated HCC of right lobe. CT shows heterogeneous contrast enhancement within tumor. 11C-Acetate PET shows focally accentuated acetate metabolism at anteromedial (AM) part of tumor, whereas 18F-FDG PET shows increased glycolysis at posterolateral (PL) part of tumor. Actual boundary of tumor, mapped from CT image, is drawn to scale on 11C-acetate and 18F-FDG PET images.
Summary of 55 HCC Lesions Detected by 11C-Acetate and 18F-FDG in Patients of Group Ia (≤3 HCC Lesions per Patient Liver)
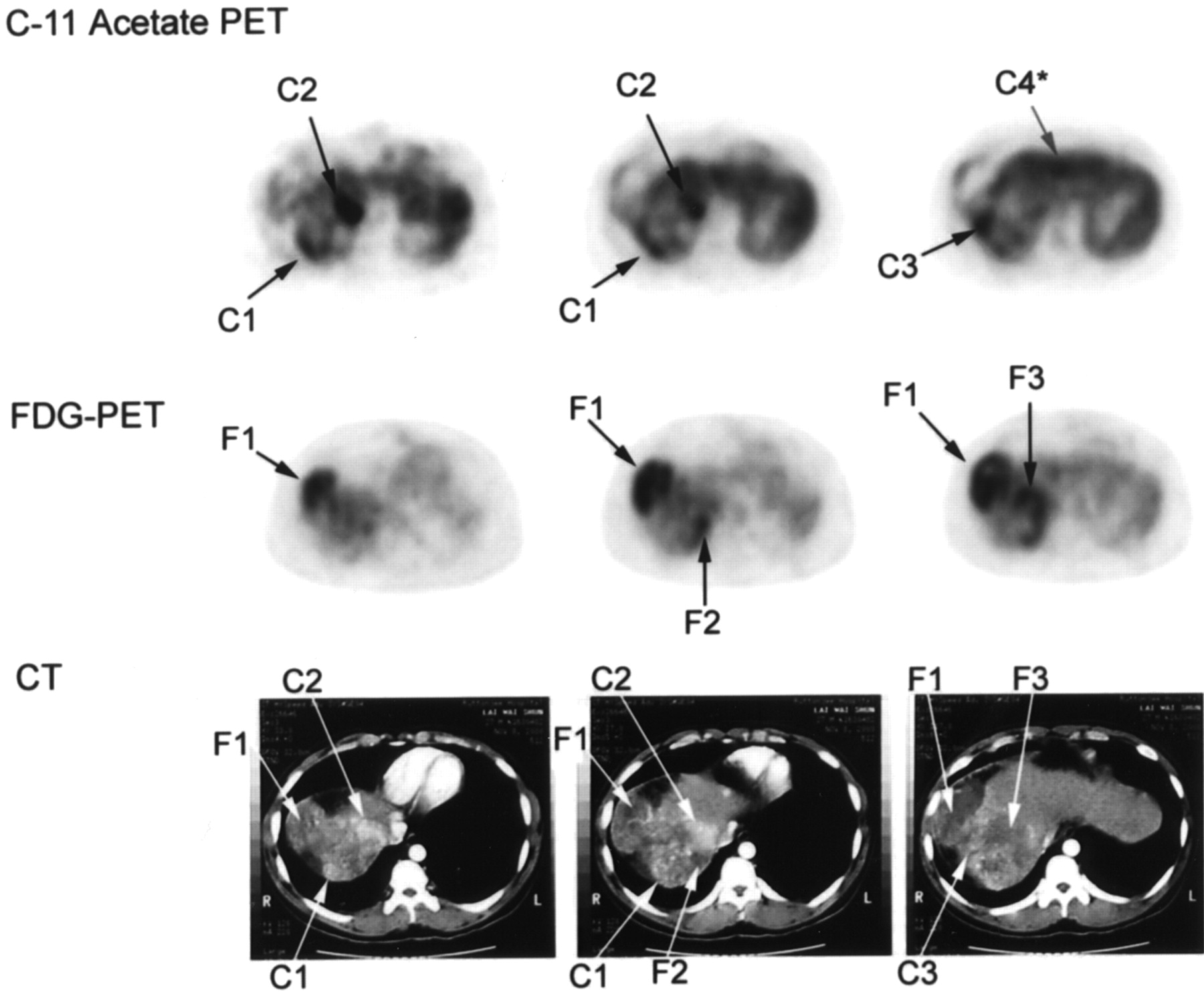
The observation that these 2 tracers were complementary in some lesions was also demonstrated by the 7 patients in group Ib—that is, the patient subgroup with advanced, metastatic, or late-stage disease (Fig. 3). Six of these patients showed poorly differentiated or moderate-to-poorly differentiated pathology. Systematic quantitative evaluation of this group of patients was not possible because many tumor lesions were either infiltrative or poorly demarcated. In some cases, normal liver tissue could not be reliably defined. Therefore, the lesion-to-liver ratio was not calculated, and only qualitative results are discussed. We also observed that the vascular (portal or venous) metastases were more avid for 18F-FDG than for 11C-acetate (Fig. 4A). Extrahepatic metastasis was also more clearly demonstrated and greater in number with the 18F-FDG tracer, except in a case of brain metastasis, which was detected by 11C-acetate imaging but was negative on 18F-FDG imaging (Fig. 4B, with surgical confirmation of metastatic moderately differentiated HCC in the right frontal lobe).

Three transaxial sections of liver in patient with multifocal HCC disease show complementary characteristics of 11C-acetate and 18F-FDG in PET imaging. 11C-Acetate-avid tumor lesions are marked by “C” and 18F-FDG-avid lesions are marked by “F.”

(A) Transaxial sections of liver show detection of portal metastasis by 18F-FDG but not by 11C-acetate PET in patient with advanced HCC and poorly differentiated tumor cells. (B) Transaxial sections of brain show metastatic nodule in right frontal lobe from primary, moderately differentiated HCC (confirmed by surgery). This is seen as lesion of increased 11C-acetate metabolism but is almost completely hypometabolic on 18F-FDG PET. Note surrounding edema on 18F-FDG images and background of no activities in normal brain tissue on 11C-acetate images.
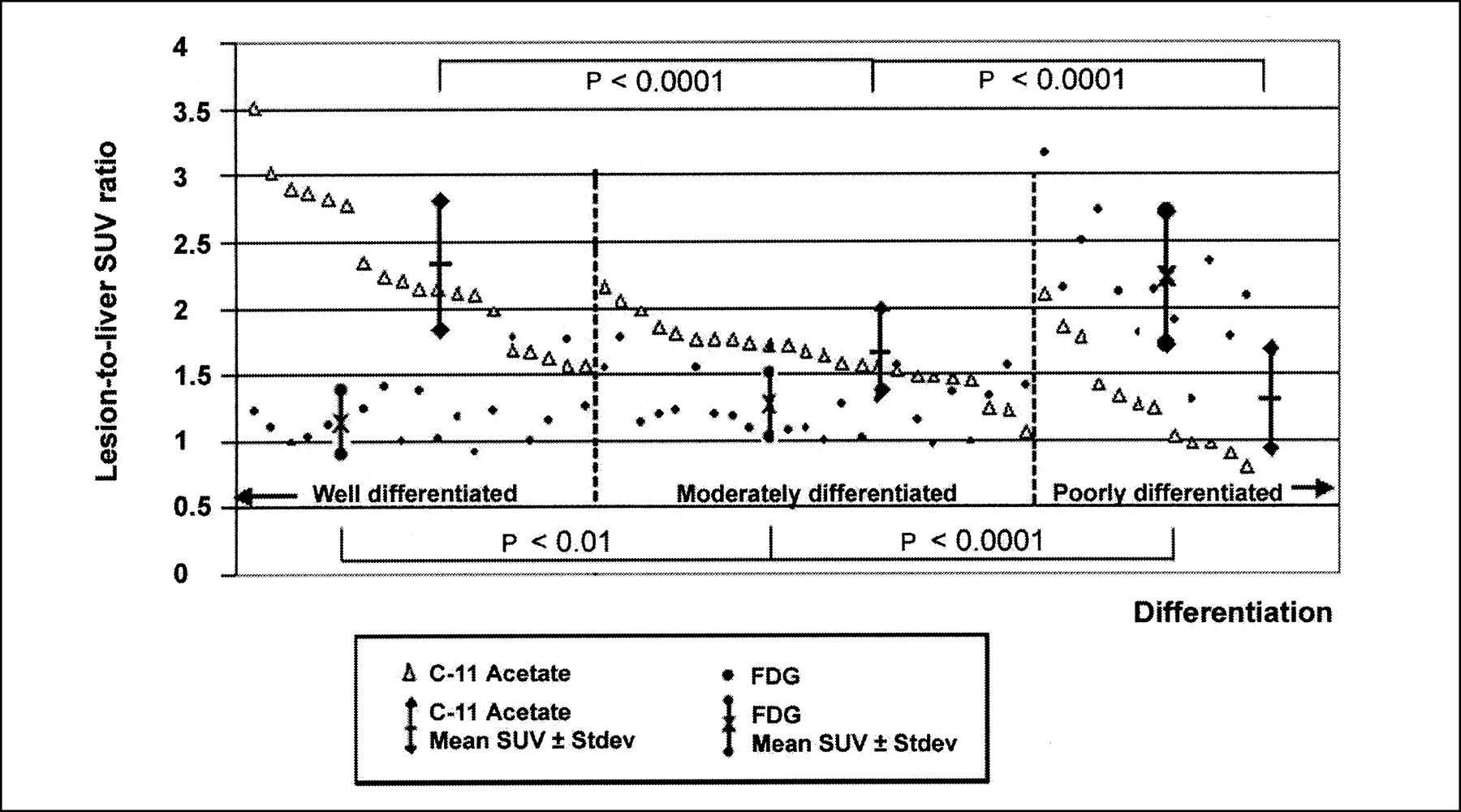
When the group Ia lesions were examined pathologically, they were categorized into 3 large groups according to cellular differentiation: well, moderate, and poor. Some tumors were reported as well-to-moderately differentiated and moderate-to-poorly differentiated. Because the pathologic categorization might have interobserver variations and there were no fine criteria between the overlapping groups, the well-to-moderately differentiated tumors were put into the well-differentiated group, and the moderate-to-poorly differentiated tumors were categorized with the poorly differentiated group for the purpose of statistical analysis. The mean lesion-to-liver SUV ratios were calculated for each group and the results are summarized in Table 2. Individual lesion-to-liver SUV ratios versus the 3 groups of differentiation are plotted in Figure 5 (sorted in descending order of 11C-acetate SUV ratios within each group). Statistical analysis of the mean SUV ratios showed significant differences (P < 0.01 to P < 0.0001) between the well- and moderately differentiated groups and between the moderate and poorly differentiated groups for each tracer.

Composite chart plots lesion-to-liver SUV ratio of all HCC lesions for patients in group Ia (with ≤3 HCC lesions) against 3 large groups of cellular differentiation. There is no fine line of transition between grades of differentiation; dashed vertical line represents rough transitional zone of visual grading reported by pathologists. Each set of vertical data points is paired: ▵, 11C-acetate; •, 18F-FDG. Values are sorted in descending order of 11C-acetate SUV ratios in each group.
Summary of Mean Lesion-to-Liver SUV Ratios in 3 Groups of Differentiation in Group Ia HCC Lesions
All the patients in group II (3 cholangiocarcinomas, 10 metastatic liver tumors) showed increased 18F-FDG metabolism in all 16 metastatic liver lesions from colon, lung, breast, and carcinoid malignancies as well as cholangiocarcinoma (pure primary hepatic adenocarcinoma). However, no abnormal 11C-acetate was detected in all of these lesions. The SUV for 11C-acetate in these metastatic lesions showed no statistical difference from nontumor hepatic parenchyma (t.025 × SE ≫ μ1 − μ2 at 95% confidence). It was interesting to note within this series of study, even in the 3 cases of cholangiocarcinoma (pure primary adenocarcinoma with no HCC components), 11C-acetate PET showed no abnormal uptake (Fig. 6). The specificity for 11C-acetate in this group of patients was by far 100% at this stage of evaluation.
Transaxial 11C-acetate PET (A), 18F-FDG PET (B), and CT (C) sections of patient with cholangiocarcinoma (pure adenocarcinoma) show no abnormal 11C-acetate metabolism but show increased 18F-FDG activity within tumor.
Group III patients had benign liver pathologies. Two of these patients had typical findings on MRI or CT and labeled red blood cell imaging for cavernous hemangioma. These hemangioma lesions were not metabolically distinguishable from normal hepatic parenchyma on 18F-FDG PET evaluation, but they were readily identified as hypometabolic foci on 11C-acetate PET imaging (partly because normal hepatic parenchyma showed more 11C-acetate activity than 18F-FDG activity). The patient with a single hepatic adenoma (3.2 × 3.0 cm) showed no abnormal 11C-acetate or 18F-FDG uptake. In the 2 patients with FNH, both had mildly increased 11C-acetate uptake. One demonstrated mildly increased 18F-FDG metabolism, whereas the other showed no abnormal 18F-FDG uptake. The patient with the larger FNH lesion (6.2 × 5.6 cm) showed a 11C-acetate SUVmax of 3.59 and a lesion-to-liver SUV ratio of 1.25 (P < 0.001 in comparison with 11C-acetate-avid HCC lesions). Results of the SUV and lesion-to-liver ratio for these 3 groups of patients (except group Ib) are summarized in Table 3.
Summary of SUV and Lesion-to-Liver SUV Ratio for Individual Group Lesions in 18F-FDG and 11C-Acetate Metabolism
DISCUSSION
In patients with a high pretest likelihood of having HCC (positive hepatitis B or C status, cirrhosis, elevated α-fetoprotein concentration), the radiologic diagnosis of HCC is usually not difficult to make. It is related partly to the fact that today the incidence of benign hepatic lesions such as FNH and adenoma is rather low, and, in fact, FNH is frequently an entity diagnosed by exclusion because of the concern of biopsy sampling error. However, various trials and combinations of techniques regarding different imaging methods exist in the literature in an attempt to increase the accuracy of detecting and diagnosing atypical lesions and tumors of <2-cm size (19–25). This is particularly true in patients with a low or intermediate likelihood of having the disease (negative status of hepatitis B surface antigen, borderline or normal α-fetoprotein concentration).
Cirrhosis is another known variable that causes confounding degrees of contrast-enhanced appearances on both conventional and helical CT (26–28), primarily related to the coexistence of regenerating and dysplastic nodules. Peterson and Baron (27) reported a low detection accuracy of 37%–45% based on recent screening studies on large cirrhotic populations. In those patients with cirrhotic livers and small lesions, the diagnosis of HCC can be difficult to make.
The role of 18F-FDG PET in the detection and diagnosis of HCC is well known to be very limited. Okazumi et al. (11) proposed that HCC may be classified into 3 “metabolic” types according to the avidity of the tumor cells for 18F-FDG. The net accumulation of 18F-FDG-6-phosphate is determined both by the phosphorylation kinase activity (reflected by the kinetic rate constant k3) and by the abundance of the glucose-6-phosphatase activity (k4). In many forms of tumor tissue, 18F-FDG is “metabolically trapped” because 18F-FDG-6-phosphate can neither pass on to the next step of glycolysis nor back diffuse to the circulation because of the low concentration of glucose-6-phosphatase enzyme (k4 approaches zero). In normal liver parenchyma, the concentration of glucose-6-phosphatase is relatively high (nonzero k4). This actually may account for the fact that the intensity of normal liver is only mild on 18F-FDG PET imaging (SUV usually ∼2.0), contrary to its role as the powerhouse of the human body. Okazumi et al. found that the type 1 hepatocellular carcinoma cells have a lower k4/k3 ratio and may show increased uptake on 18F-FDG PET imaging like many other forms of malignancy. Type 2 hepatocellular carcinoma cells have a k4/k3 ratio similar to that of normal hepatocytes and therefore may be isointense on 18F-FDG PET imaging. Type 3 tumor cells have a higher k4/k3 ratio and are actually hypointense. The combination of type 2 and type 3 tumors constitutes about a 43% false-negative rate in Okazumi’s group. In our study, the false-negative rate by account of tumor lesions is 52.7%, slightly higher than their reported value as well as those by others (6,10).
In fact, the degree and nature of tumor cell differentiation are known to affect the amount of 18F-FDG accumulation in cells, as suggested by other investigators with smaller samples in their studies (8,12,14). Early research on rat hepatomas had suggested that the patterns of glycolytic enzymes might reflect hepatoma cell growth, function, and graded dedifferentiation (29). Because well-differentiated hepatocellular carcinoma cells are histologically closer to the normal liver cells than to the undifferentiated types, the abundance of glucose-6-phosphatase enzyme may render these tumors undetectable. This relationship is strongly suggested by data in this study. Figure 5 shows that there is a statistically significant relationship of cellular differentiation with the tumor’s avidity for 18F-FDG and 11C-acetate metabolism in terms of the lesion-to-liver SUV ratio. The well-differentiated and well-to-moderately differentiated types tend to be negative for 18F-FDG; whereas the poorly differentiated and moderate-to-poorly differentiated types show increased 18F-FDG metabolism.
The use of 11C-acetate in tumor imaging has been suggested recently in urologic malignancies (15,16). Possible biochemical paths of acetate incorporation or accumulation include (a) entering the Krebs cycle from acetyl coenzyme A (acetyl CoA) or as an intermediate metabolite, (b) esterification to form acetyl CoA as a major precursor in β-oxidation for fatty acid synthesis, (c) combining with glycine in heme synthesis, and (d) through citrate for cholesterol synthesis. Of all of these possible metabolic pathways, participation in free fatty acid (lipid) synthesis is believed to be the dominant method of incorporation in tumors. Yoshimoto et al. (30) suggested that this mechanism of tumor uptake was different from that of myocardium, in which 11C-acetate was channeled mainly to the Krebs cycle. The results of this study suggest that 11C-acetate is able to detect the entire proportion of HCC lesions that are negative on 18F-FDG imaging. In those tumors that are both 11C-acetate and 18F-FDG positive (the moderately differentiated type), some cases suggest that these tracers are taken up by different parts of the tumor (Figs. 2 and 3). Therefore, mixed metabolic constituents and kinetics are likely to be present within the same tumor at variable degrees. These 2 tracers are probably complementary to each other in the detection of HCC. The lesion-to-liver SUV ratios for 11C-acetate and 18F-FDG have a statistically significant relationship to each other in tumor cellular differentiation (Fig. 5). In the detection of individual tumor lesions (partial or whole tumor), the overall ability of 11C-acetate is better than that of 18F-FDG, with a detection sensitivity of 87.3% versus 47.3% using 18F-FDG. This relative accuracy appears to be highly dependent on tumor cellular differentiation. For HCC with ≤3 tumor lesions, tumor cells show a variable degree of differentiation with 60%–70% in the well- and moderately differentiated category. As tumor cells become more aggressive in later or advanced stages, cellular kinetic also change. The poor- or less well-differentiated tumor cells begin to retain 18F-FDG. In our study, all of the group Ib patients showed more 18F-FDG accumulation in their primary liver tumors and metastases, including vascular, nodal and distant metastases (except 1 case with a surgically confirmed moderately differentiated brain metastasis, as depicted in Fig. 4). Furthermore, the finding of a strong complementary relationship of 11C-acetate and 18F-FDG in the evaluation of HCC appears to be very important to the use of PET imaging in the monitoring of therapy in patients with this tumor.
The other interesting observation is that 11C-acetate may be quite specific for HCC in the evaluation of liver lesions. Our study showed that 11C-acetate is negative in hemangioma; cholangiocarcinoma (pure primary adenocarcinoma of liver without HCC components); secondary carcinomas from colon, breast, and lung; as well as carcinoid tumors. This specificity can be highly useful in the preliminary evaluation of unknown liver masses. When both tracers are positive or positive only for 11C-acetate, the likelihood for the tumor mass to be HCC is very high. On the other hand, when a liver mass is positive only for 18F-FDG but is negative for 11C-acetate, the possibility of non-HCC malignancy or poorly differentiated HCC should be considered. In case both tracers are negative, benign pathology is more likely. Two cases of FNH showed only mildly increased 11C-acetate metabolism. The lesion with the higher lesion-to-liver SUV ratio showed a value of 1.25, statistically lower than the average value of all of the 11C-acetate-positive HCC cases in this study (1.96 ± 0.63; P < 0.001).
It is not possible to include all other liver lesions in a single study; therefore, we studied only 2 FNH cases and 1 case of adenoma. In addition, other pathology such as fibrolamellar HCC and liver abscess have not yet been studied. In the next stage of evaluation, patients with smaller HCC lesions of <2-cm size and more severely cirrhotic livers may be investigated. The findings reported here and concurrent work on the kinetic modeling of 11C-acetate in HCC may add to the understanding of the molecular basis of this tumor. A reliable diagnostic PET radiopharmaceutical is important for formulating and monitoring therapeutic treatment of this tumor.
CONCLUSION
HCC is a malignancy of high prevalence and grave prognosis. In this prospective study, our preliminary data have shown that 11C-acetate PET not only is significantly more sensitive than 18F-FDG PET in the detection of individual HCC lesions but also appears to be quite specific. Our findings also suggest that tumor detection by these 2 tracers is dependent on histologic differentiation. Therefore, 11C-acetate may likely be a promising tracer in complementing the deficiency of 18F-FDG in PET imaging of liver masses.
Acknowledgments
The authors thank the Hospital Board of the Hong Kong Sanatorium and Hospital for their support of this work, Jacky Cheung and Kin-Chung Liu for preparation of the PET radiopharmaceuticals, May Chan and the technologists for clinical assistance, and Maria Yeung and Jennifer Choi for finalizing this manuscript.
Footnotes
Received Mar. 6, 2002; revision accepted Jul. 9, 2002.
For correspondence or reprints contact: Chi-Lai Ho, MBBS, Department of Nuclear Medicine and PET, Hong Kong Sanatorium and Hospital, 2 Village Rd., Happy Valley, Hong Kong, China.
E-mail: garrettho{at}hksh.org.hk
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Monitoring Response to Transarterial Chemoembolization in Hepatocellular Carcinoma Using 18F-Fluorothymidine PET
- 3D-printed automation for optimized PET radiochemistry
- Transcriptomics Associates Molecular Features with 18F-Fluorocholine PET/CT Imaging Phenotype and Its Potential Relationship to Survival in Hepatocellular Carcinoma
- Antitumor T-cell Reconditioning: Improving Metabolic Fitness for Optimal Cancer Immunotherapy
- Radiation Dosimetry of Whole-Body Dual-Tracer 18F-FDG and 11C-Acetate PET/CT for Hepatocellular Carcinoma
- Prognostic Significance of 18F-FDG Uptake in Hepatocellular Carcinoma Treated with Transarterial Chemoembolization or Concurrent Chemoradiotherapy: A Multicenter Retrospective Cohort Study
- The Role of 18F-FDG Accumulation and Arterial Enhancement as Biomarkers in the Assessment of Typing, Grading and Staging of Hepatocellular Carcinoma Using 18F-FDG-PET/CT with Integrated Dual-phase CT Angiography
- Late Imaging with [1-11C]Acetate Improves Detection of Tumor Fatty Acid Synthesis with PET
- Reply: Underestimated Role of 18F-FDG PET for HCC Evaluation and Promise of 18F-FDG PET/MR Imaging in This Setting
- 11C-Acetate and 18F-FDG PET/CT for Clinical Staging and Selection of Patients with Hepatocellular Carcinoma for Liver Transplantation on the Basis of Milan Criteria: Surgeon's Perspective
- An NMR Metabolomics Approach for the Diagnosis of Leptomeningeal Carcinomatosis
- Detection of Hepatocellular Carcinoma with PET/CT: A Prospective Comparison of 18F-Fluorocholine and 18F-FDG in Patients with Cirrhosis or Chronic Liver Disease
- 1-11C-Acetate Versus 18F-FDG PET in Detection of Meningioma and Monitoring the Effect of {gamma}-Knife Radiosurgery
- Imaging of Proliferation in Hepatocellular Carcinoma with the In Vivo Marker 18F-Fluorothymidine
- The Importance of Acetyl Coenzyme A Synthetase for 11C-Acetate Uptake and Cell Survival in Hepatocellular Carcinoma
- Prediction of Tumor Recurrence by 18F-FDG PET in Liver Transplantation for Hepatocellular Carcinoma
- A Prospective Evaluation of 18F-FDG and 11C-Acetate PET/CT for Detection of Primary and Metastatic Hepatocellular Carcinoma
- Detection of Hepatocellular Carcinoma Using 11C-Choline PET: Comparison with 18F-FDG PET
- Clinical applications and advances of positron emission tomography with fluorine-18-fluorodeoxyglucose (18F-FDG) in the diagnosis of liver neoplasms
- Dual-Tracer PET/CT Imaging in Evaluation of Metastatic Hepatocellular Carcinoma
- 18F-Fluoroacetate: A Potential Acetate Analog for Prostate Tumor Imaging--In Vivo Evaluation of 18F-Fluoroacetate Versus 11C-Acetate
- Different Glucose Uptake and Glycolytic Mechanisms Between Hepatocellular Carcinoma and Intrahepatic Mass-Forming Cholangiocarcinoma with Increased 18F-FDG Uptake
- Application of Intravenous Contrast in PET/CT: Does It Really Introduce Significant Attenuation Correction Error?
- Diagnostic biopsy for hepatocellular carcinoma in cirrhosis: useful, necessary, dangerous, or academic sport?
- 11C-Acetate: A New Tracer for the Evaluation of Hepatocellular Carcinoma