


Abstract
Because 18F-FDG PET has insufficient sensitivity for the detection of hepatocellular carcinoma (HCC), 11C-acetate PET has been proposed as another technique for this use. We prospectively evaluated the value of PET/CT using these 2 tracers for the detection of primary and metastatic HCC. Methods: One hundred twelve patients (99 with HCC, 13 with cholangiocellular carcinoma) underwent biopsy and 18F-FDG and 11C-acetate PET/CT. Results: The overall sensitivities of 18F-FDG, 11C-acetate, and dual-tracer PET/CT in the detection of 110 lesions in 90 patients with primary HCC were 60.9%, 75.4%, and 82.7%, respectively. Elevated serum α-fetoprotein levels, an advanced tumor stage, portal vein tumor thrombosis, large tumors, and multiple tumors were significantly associated with positive 18F-FDG PET/CT results. Uptake of 11C-acetate was associated with large and multiple tumors. For 18F-FDG, the sensitivities according to tumor size (1–2, 2–5, and ≥5 cm) were 27.2%, 47.8%, and 92.8%, respectively; for 11C-acetate, these respective values were 31.8%, 78.2%, and 95.2%. 18F-FDG was more sensitive in the detection of poorly differentiated HCC. Overall survival was lower in patients with 18F-FDG PET/CT positive for all indexed lesions than in those with FDG negative or partially positive through the entire follow-up period. In analysis based on biopsied lesions, the sensitivity of 18F-FDG PET/CT was 64.4% for primary HCC and 84.4% for 11C-acetate PET/CT. The overall sensitivities of 18F-FDG, 11C-acetate, and dual-tracer PET/CT for 35 metastatic HCCs were 85.7%, 77.0%, and 85.7%, respectively. There was no significant difference in the sensitivity of tracers according to metastatic tumor size, location, or differentiation. Conclusion: The addition of 11C-acetate to 18F-FDG PET/CT increases the overall sensitivity for the detection of primary HCC but not for the detection of extrahepatic metastases. 18F-FDG, 11C-acetate, and dual-tracer PET/CT have a low sensitivity for the detection of small primary HCC, but 18F-FDG PET/CT has a relatively high sensitivity for the detection of extrahepatic metastases of HCC.
The prognosis of patients with hepatocellular carcinoma (HCC) is related to tumor stage at presentation and underlying liver function. Reliable staging of HCC is a fundamental precondition for deciding on the treatment modality, and the Barcelona Clinic Liver Cancer (BCLC) staging system links tumor stage with treatment modality (1). In particular, accurate characterization of primary and metastatic HCC, showing the tendency toward early vascular invasion of the tumor (2), is critical for proper treatment (2). Imaging studies by dynamic CT and contrast-enhanced MRI are important in the diagnosis and staging of HCC (1,3,4), but there is no consensus on which imaging tests are proper for detecting extrahepatic metastases. Whole-body PET has been used in a portion of HCC patients, but its usefulness has not yet been established.
Because whole-body combined PET/CT using 18F-FDG effectively detects numerous cancerous lesions (5), this method was expected to improve the accuracy of HCC staging. However, the high level of glucose-6-phosphatase in liver tissue leads to the release of FDG-6-phosphate, resulting in reduced accumulation in differentiated HCCs (6). Thus, 18F-FDG PET has an average false-negative rate of 40%−50% for the detection of HCC (7), and data on the role of PET/CT in the detection of HCC metastasis are limited (7–9).
11C-labeled acetate PET effectively detects urologic malignancies (10). This tracer enters the Krebs cycle as a substrate for β-oxidation in fatty acid synthesis and cholesterol synthesis. Fatty acid synthesis is believed to be the major reason for uptake of 11C-acetate by liver tumors. Recently, a Chinese study reported that 11C-acetate PET has improved sensitivity for detection of well-differentiated HCCs and that none of the primary HCC lesions was negative for 18F-FDG and 11C-acetate tracers (6). However, that study did not analyze sensitivity with regard to clinical and tumor characteristics, including underlying liver function and tumor stage. PET/CT is used mainly to screen for tumor metastasis, and its use is increasing because of an increasing number of candidates for curative treatment such as liver transplantation. Previous studies of PET/CT in patients with primary and metastatic HCC enrolled few patients or were retrospective (7–9,11,12).
The aim of this prospective study was to validate the value of 18F-FDG and 11C-acetate PET/CT for the detection of primary and metastatic HCC in 112 patients admitted to our center for diagnosis and treatment of primary liver cancer.
MATERIALS AND METHODS
Patients
Between June 2006 and April 2007, 112 patients diagnosed with primary liver cancer at the National Cancer Center Hospital (Goyang, South Korea) were prospectively enrolled. All patients gave informed consent, and the study was approved by the Internal Review Board at the hospital. All patients had newly diagnosed HCC, cholangiocellular carcinoma (CCC), or a newly diagnosed distant metastasis after curative resection of HCC that was performed 6 mo before this study. Patients underwent 18F-FDG and 11C-acetate PET/CT free of charge before treatment. Clinical diagnosis of primary HCC was based on the guidelines of the Korean Liver Cancer Study Group and the National Cancer Center of Korea (13). CCC was diagnosed by pathologic examination and exclusion of other metastatic adenocarcinomas. All 112 patients were examined by spiral CT, and imaging was confirmed pathologically by liver biopsy or operative tumor resection that was performed 1 wk before or after PET/CT. Liver biopsy was performed on a typical index lesion. The inclusion criteria of subjects were as follows: age between 18 and 80 y, Eastern Cooperative Oncology Group performance status of 0–2, adequate liver function (Child–Pugh classification A or B), and adequate renal function (serum creatinine < 1.4 mg/dL). Patients were excluded if they had any other malignancy, a concurrent nonmalignant severe illness, or a psychiatric disorder.
Metastatic HCC lesions were screened and followed by chest radiography and routine spiral liver CT that covered the area from the hila of the lungs through the symphysis pubis or (in the case of suspected positive symptoms) by additional bone scanning and brain MRI. HCC metastasis was confirmed by histopathologic diagnosis (in the case of tumor resection or biopsy), by follow-up chest spiral CT with compatible nodules (when there was no clinical evidence of a benign tumor or inflammation), or by bone MRI or bone CT. Intraabdominal metastases and brain metastases were diagnosed by routine spiral liver CT and brain MRI. An intraabdominal lymph node metastasis was considered to be present when the node was more than 1 cm in diameter.
The absence of HCC metastasis was confirmed by the serum level of α-fetoprotein and by imaging (chest radiography and routine spiral liver CT covering the area from the hila of the lungs through the symphysis pubis) performed at the 3-mo follow-up.
Imaging Studies and Biopsy
Routine spiral CT was performed with multidetector CT scanners (Lightspeed pro-16; GE Healthcare). Images were acquired in a craniocaudal direction from the hila of the lungs through the symphysis pubis with 1.25 × 16 mm beam collimation and a reconstruction interval of 3.0 mm. Hepatic artery–phase imaging was initiated 25 s after contrast medium injection. After administration of the contrast medium, the portal vein phase and equilibrium phase were acquired at 70 and 180 s, respectively.
MRI was performed on a 1.5-T superconducting scanner (Sigma; GE Healthcare) with a torso coil for signal reception. Baseline MRI was performed, and dynamic imaging was performed before and after administration of gadopentetate dimeglumine (Magnevist; Schering). Superparamagnetic iron oxide–enhanced MRI was performed immediately after gadolinium-enhanced dynamic MRI. For superparamagnetic iron oxide–enhanced MRI, ferumoxides (Feridex I.V.; Advanced Magnetics) were administered and images were obtained at 30 s (hepatic artery phase), 70 s (portal vein phase), and 3–5 min (delayed phase). Spiral CT and contrast-enhanced MRI were evaluated by 2 expert radiologists.
Sonographically guided percutaneous core biopsies were performed using a freehand technique. All biopsies were performed with a 3.5- to 5-MHz convex probe (Acuson Sequia 512; Siemens Medical Solutions) with 18-gauge automated core biopsy needles (Acecut; TSK). Specimens were routinely processed and were stained with hematoxylin and eosin and by the Masson trichrome method. HCC was diagnosed according to the criteria of the International Working Party (14).
18F-FDG and 11C-Acetate PET/CT
11C-acetate was synthesized using a fully automated custom-made radiochemistry module based on the solid-phase extraction method of Roeda et al. (15). 18F-FDG was synthesized at our hospital using an automated radiochemistry module (Chemical Process Control Unit; CTI/Siemens).
PET studies were performed with a dedicated PET scanner (Biograph LSO; Siemens Medical Systems) or a PET/CT scanner (Discovery LS; GE Healthcare). For the Biograph LSO scanner, we used a scout view with 30 mA and 130 kVp, followed by a spiral CT scan with an effective milliamperage of 50, 130 kVp, a 5-mm section width, a 4-mm collimation, a 12-mm table feed per rotation, 0.8 s per rotation, and the patient's arms raised. For the Discovery LS scanner, we used a scout view with 30 mA and 120 kVp, followed by a spiral CT scan with a 0.8-s rotation time, 80 mA, 140 kVp, a 5-mm section thickness, a 4.25-mm interval in high-speed mode, and the patient's arms at the sides of the torso. PET images were acquired after CT scans at 3 min per bed position of 11.2 cm in the 3-dimensional acquisition mode (Biograph LSO) or 4 min per bed position of 14.2 cm in the 2-dimensional acquisition mode (Discovery LS). CT images were reconstructed onto a 512 × 512 matrix and converted into 511-keV-equivalent attenuation factors for attenuation correction. PET images were reconstructed onto a 128 × 128 matrix using ordered-subsets expectation maximization and attenuation correction. The standardized uptake value (SUV) was calculated as (decay-corrected activity [kBq] per milliliter of tissue volume)/(injected 18F-FDG activity [kBq]/body mass [g]). The SUVs of lesions were obtained by placing regions of interest manually around the lesion. The maximum SUV within a region of interest was used to minimize partial-volume effects.
All patients were normoglycemic and had fasted, except for water and medications, for at least 8 h before the PET studies. 11C-acetate PET/CT was performed first, and 18F-FDG PET/CT was performed at least 4 h later.
11C-Acetate PET/CT.
Whole-body static PET/CT scans, obtained 20 min after intravenous injection of about 370–555 MBq (10–15 mCi) of 11C-acetate, were acquired from the cerebellum to the upper third of the femur with 6–7 frames. To enhance and standardize tumor uptake of 18F-FDG, we had the patients continue to fast after 11C-acetate PET/CT until the end of the 18F-FDG PET/CT study.
18F-FDG PET/CT.
The patients were kept well hydrated because 18F-FDG is excreted through the kidney and urinary bladder. Twenty milligrams of furosemide were administered intravenously within 10 min of the 18F-FDG injection, and then 500 mL of water were given. 18F-FDG (444–740 MBq [12–20 mCi]) was injected intravenously 4 h after 11C-acetate PET/CT. Patients were encouraged to rest during the 18F-FDG uptake period. Sixty minutes after 18F-FDG injection, whole-body static PET/CT was performed using the same method as for whole-body 11C-acetate PET/CT.
PET/CT Analysis
Separate CT and PET scan data were accurately coregistered. PET, PET/CT, and CT images were reviewed using a dedicated workstation and software (eNtegra; GE Healthcare, and e.Soft; Siemens Medical Solutions). With this system, 3-dimensional displays (transaxial, coronal, and sagittal) were available, as were maximum-intensity projections of the PET data. PET/CT scans were interpreted by 2 nuclear medicine physicians, who were unaware of the results of other imaging studies on these patients. Intrahepatic primary lesions were interpreted visually using a 3-point grading system (isometabolic, hypermetabolic, and hypometabolic) that compared data with tracer uptake by normal liver parenchyma for 11C-acetate and 18F-FDG PET. If a lesion was hypermetabolic on at least 1 image from 11C-acetate or 18F-FDG PET, it was assumed to be a malignant hepatic mass. Extrahepatic lesions were interpreted visually using a 5-point scale: 0, no visible accumulation; 1, less accumulation than in the liver; 2, accumulation about the same as in the liver; 3, more accumulation than in the liver but less than in the brain cortex; 4, accumulation comparable to that of the brain cortex (16). An extrahepatic lesion was considered to be malignant when its accumulation of 18F-FDG or 11C-acetate was over 3 on this scale.
Interpretation and Statistical Analysis
To assess the diagnostic accuracy of 18F-FDG and 11C-acetate PET/CT, we calculated values in a lesion-to-lesion analysis for all primary liver cancer lesions, lymph nodes, and distant metastases. All analyzed lesions were larger than 1 cm and were interpreted according to the criteria described above for spiral CT or contrast-enhanced MRI. Patient-based analysis was also performed. For the subgroup of patients with more than 4 lesions or with diffuse infiltrative tumors, the index lesion was assigned as the representative lesion or area before PET/CT analysis. Liver biopsy sites were identified if biopsies were performed before PET/CT analysis.
The data were analyzed using STATA software, version 9.1 (StataCorp LP). The Pearson χ2 test and Fisher exact test were used for categoric variables, and the Student t test was used for continuous variables. The results of all continuous variables are expressed as the mean ± SD. The Kaplan–Meier method was used to estimate overall survival curves, and survival curves were compared using the log-rank test. Results were considered significant if the P value was less than 0.05.
RESULTS
Patient Characteristics
The characteristics of the 112 patients (99 with HCC, 13 with CCC) are summarized in Table 1. The mean age was 57.6 ± 10.4 y (range, 34–85 y), and the sex ratio (M:F) was 3.7:1. Eighty-three patients (74.1%) tested positive for the hepatitis B surface antigen. Ten patients had hepatitis C, 10 had a history of alcohol abuse, and 10 had non-B/non-C/nonalcoholic etiologies. One hundred one patients had a Child–Pugh classification of A. Nine patients who underwent surgical resection had distant metastases but no primary liver lesions; hence we analyzed 90 patients for primary tumor characteristics. Analysis of the maximal diameter of tumors showed that 7 patients (7.8%) had lesions 1–2 cm in diameter, 42 patients (46.7%) had lesions 2–5 cm in diameter, and 41 patients (45.5%) had lesions 5 cm or more in diameter. Analysis of the number of nodules showed that 46 patients (51.1%) had 1 nodule, 11 patients (12.2%) had 2 nodules, 3 patients (3.3%) had 3 nodules, and 30 patients (33.3%) had more than 3 nodules. Of the 99 HCC patients, 7 had biopsy specimens that were inadequate for evaluation of tumor differentiation. We evaluated the other 92 patients (83 with primary HCC, 9 with metastatic HCC) using the Edmonson–Steiner grading system. Nine patients were grade I, 51 were grade II, 29 were grade III, and 3 were grade IV. Serum α-fetoprotein levels less than 20 ng/mL were detected in 43 HCC patients (43.4%). Using the modified Union Internationale Contre le Cancer (International Union Against Cancer) (UICC) staging system, we enrolled 5 (5.1%) stage I patients, 37 (37.3%) stage II patients, 16 (16.2%) stage III patients, 13 (13.1%) stage IVa patients, and 28 (28.3%) stage IVb patients. According to the BCLC staging system, 21 patients (21.4%) were in very early or early stage HCC, 35 patients (35.7%) were in intermediate stage HCC, and 43 patients (44%) in advanced or terminal stage HCC (Table 1).
Baseline Characteristics
Lesion Uptake of PET/CT: Patient-Based Analysis
Among the 99 HCC patients, we evaluated all positive results from 18F-FDG and 11C-acetate PET/CT (Tables 2 and 3; Fig. 1). Because the number of index lesions varied from 1 to 4 in each patient, we classified analysis of PET positives in all lesions and partial lesions. In our patient-based analysis, a PET-positive result indicates a positive result for all index lesions. The following factors were significantly associated with uptake of 18F-FDG findings on PET/CT: level of serum α-fetoprotein, modified UICC stage, BCLC stage, tumor size, number of tumors, and presence of portal vein invasion. Higher levels of serum α-fetoprotein and larger tumors were associated with positive 18F-FDG PET/CT results (P < 0.001). None of the 7 patients with small tumors (<2 cm in diameter), 18 of 42 patients (43%) with tumors 2–5 cm in diameter, and 32 of 41 patients (78%) with tumors larger than 5 cm had positive findings for all index lesions on 18F-FDG PET/CT. However, the differences between these groups were not statistically significant (Table 3). None of the patients in modified UICC stage I and none of the patients in the very early BCLC stage had positive findings on 18F-FDG PET/CT. In contrast, 11 of 13 patients (85%) in modified UICC stage IVa and 31 of 42 patients (74%) in the advanced BCLC stage had positive findings on 18F-FDG PET/CT. Figure 2 shows the association between 18F-FDG PET/CT and overall survival in HCC patients. Patients with positive 18F-FDG PET/CT findings for all indexed lesions had significantly lower survival than did patients with negative or partially positive 18F-FDG PET/CT findings (P = 0.0421).
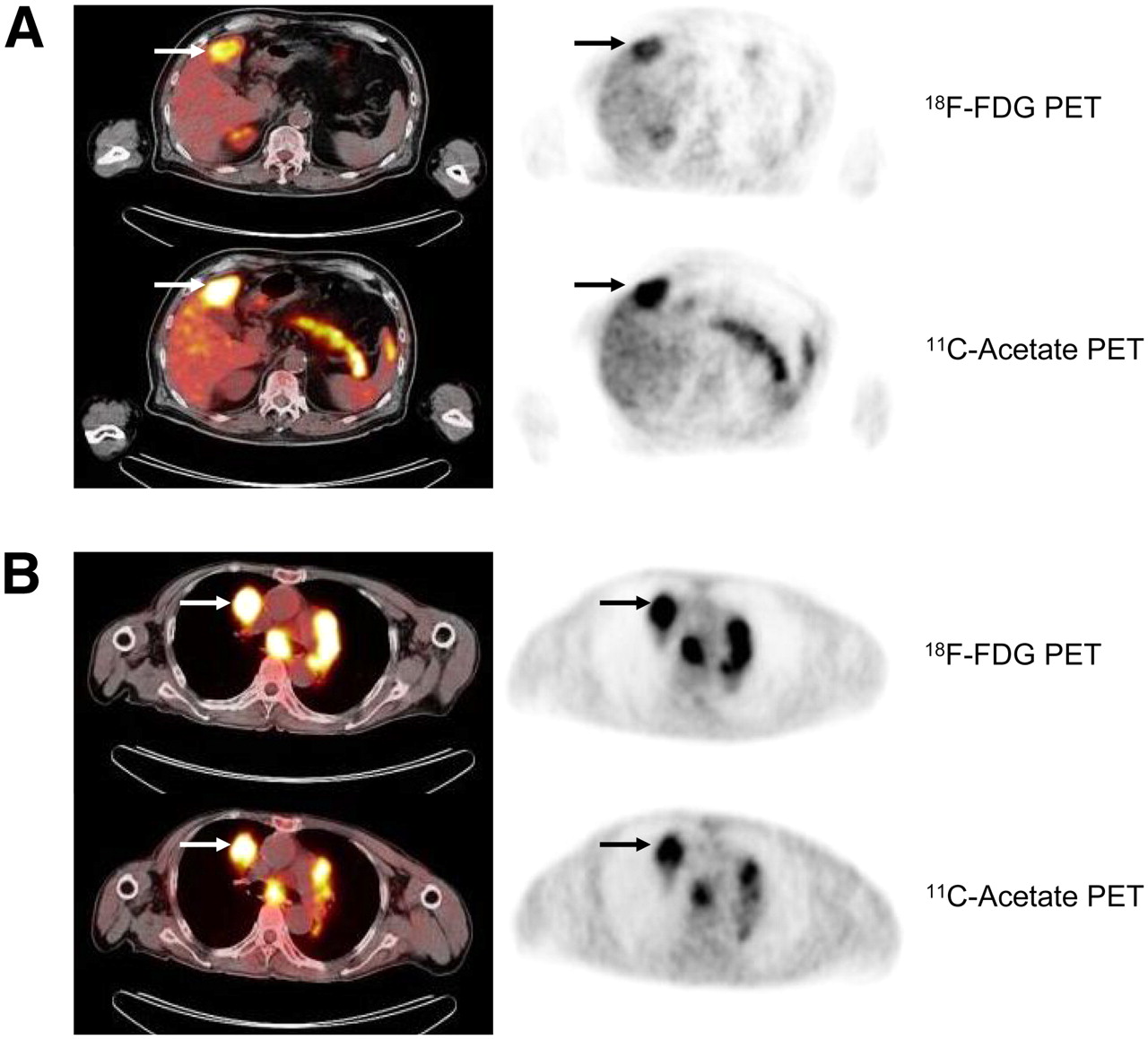
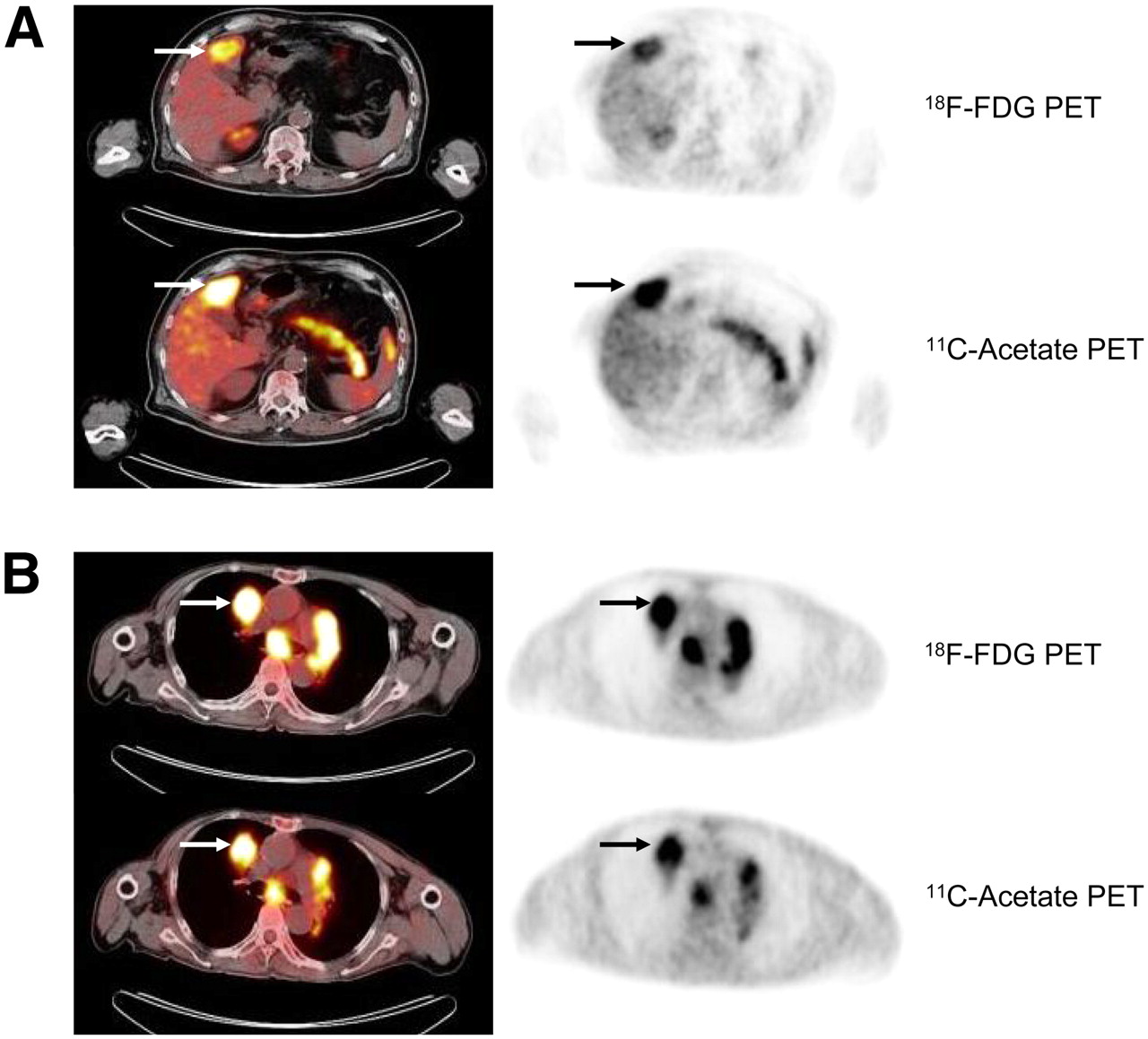
Detection of HCC with 18F-FDG PET/CT and 11C-acetate PET/CT on transaxial sections of liver and chest. Panels on left show PET/CT, and panels on right show PET. (A) Primary HCC of liver was markedly positive for uptake with both tracers (arrows). (B) Metastatic HCC of upper lobe of right lung was markedly positive for uptake with both tracers (arrows).
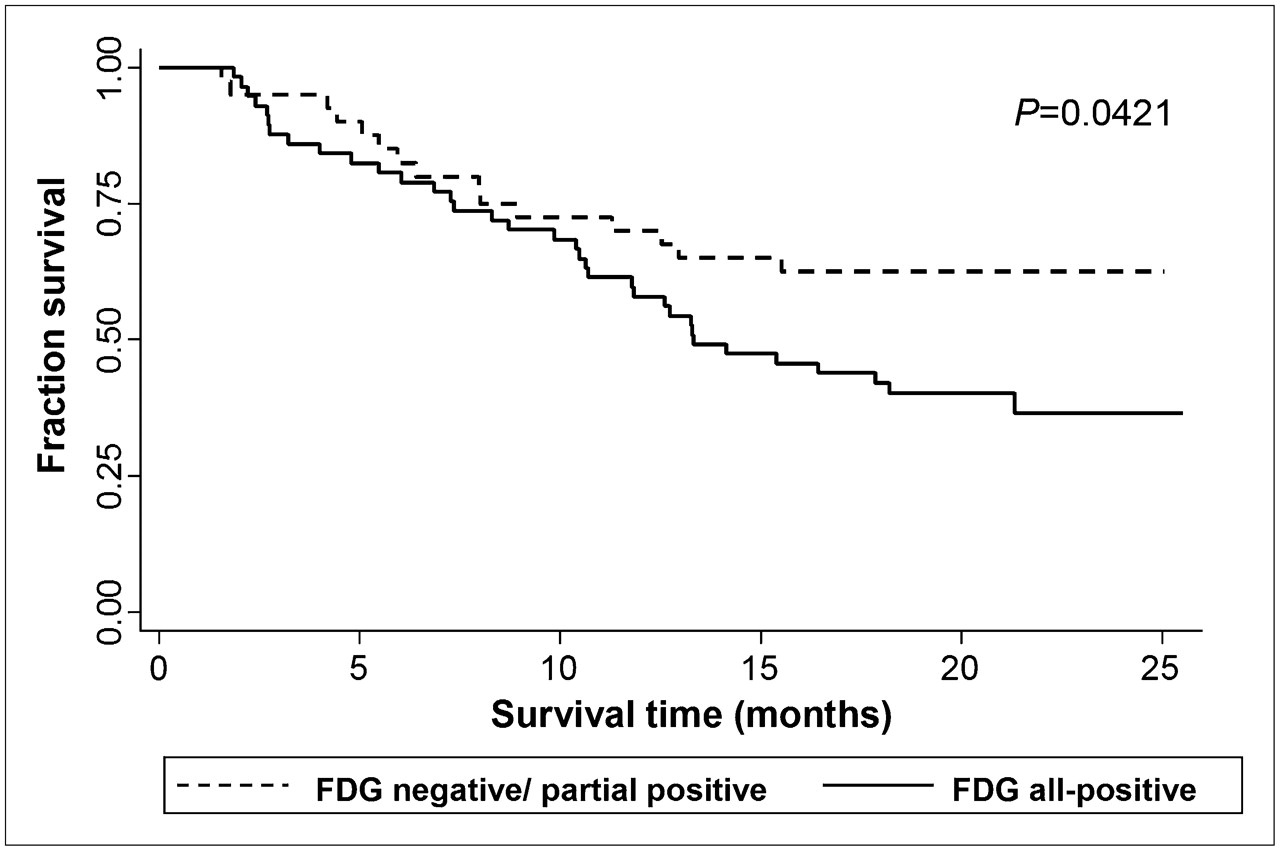
Overall survival after diagnosis of HCC. Kaplan–Meier survival plots are classified by positivity of 18F-FDG. Overall survival was lower in patients with positive 18F-FDG findings than in those with negative or partially positive 18F-FDG findings through entire follow-up period. P values were calculated using log-rank test.
Lesion Uptake of 18F-FDG and 11C-Acetate on PET/CT: Patient-Based Analysis of 99 Patients with Primary and Metastatic HCC
Lesion Uptake of 18F-FDG and 11C-Acetate on PET/CT: Patient-Based Analysis of 90 Patients with Primary HCC
The significant factors for uptake of 11C-acetate were tumor size and number of tumors (Tables 2 and 3). Any clinical factors and staging were not associated with uptake of 11C-acetate PET/CT. In contrast to our 18F-FDG PET/CT results, in 2 of 5 patients (40%) in modified UICC stage I and 31 of 37 patients (84%) in modified UICC stage II, all lesions were positive on 11C-acetate PET/CT. In 2 of 7 patients (29%) with small tumors (diameter < 2 cm) and 29 of 42 patients (69%) with 2- to 5-cm tumors, all lesions were positive on 11C-acetate PET/CT (P = 0.003; Table 3). Compared with 18F-FDG PET/CT, 11C-acetate PET/CT showed positive findings for all lesions in more patients with the following characteristics: the male sex, a performance status of 0, a serum α-fetoprotein level of less than 20 ng/mL, hepatitis B virus positive, modified UICC stage II, an intermediate-sized (2–5 cm) tumor, a single tumor, a well-defined tumor, and no portal vein invasion (P < 0.05). The positivity of 11C-acetate PET/CT was not related to the survival of HCC patients (P = 0.7271).
Sensitivity for Detection of Primary Liver Cancer by PET/CT: Lesion-Based Analysis
Among the 110 lesions of the 90 patients with primary HCC, we evaluated the lesions that were positive on 18F-FDG and 11C-acetate PET/CT (Table 4; Fig. 3). Tumor size, number of tumors, and tumor differentiation were significantly associated with the sensitivity for detection of primary HCC on 18F-FDG PET/CT (P < 0.05). The sensitivity for detection of HCC by 18F-FDG PET/CT was 27.2%, 47.8%, and 92.8% in index lesions sized 1–2 cm, 2–5 cm, and 5 cm or more, respectively. Twenty-seven of 46 single lesions (58.8%) and 26 of 33 index lesions (79%) in patients who had more than 3 lesions were positive on 18F-FDG PET/CT. 18F-FDG PET/CT had significantly higher sensitivity for poorly differentiated HCC (Edmonson–Steiner grades III and IV) than for well-differentiated HCC (grades I and II; P < 0.001).
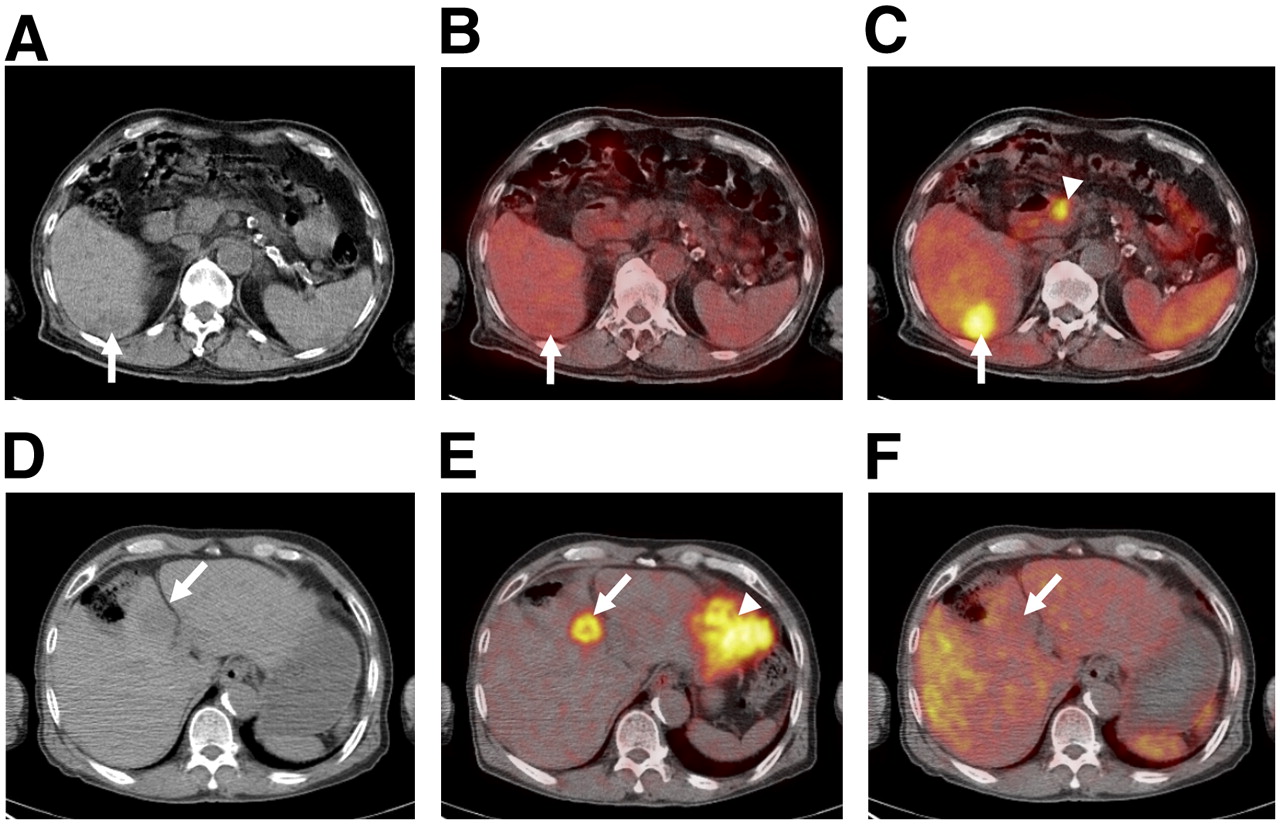
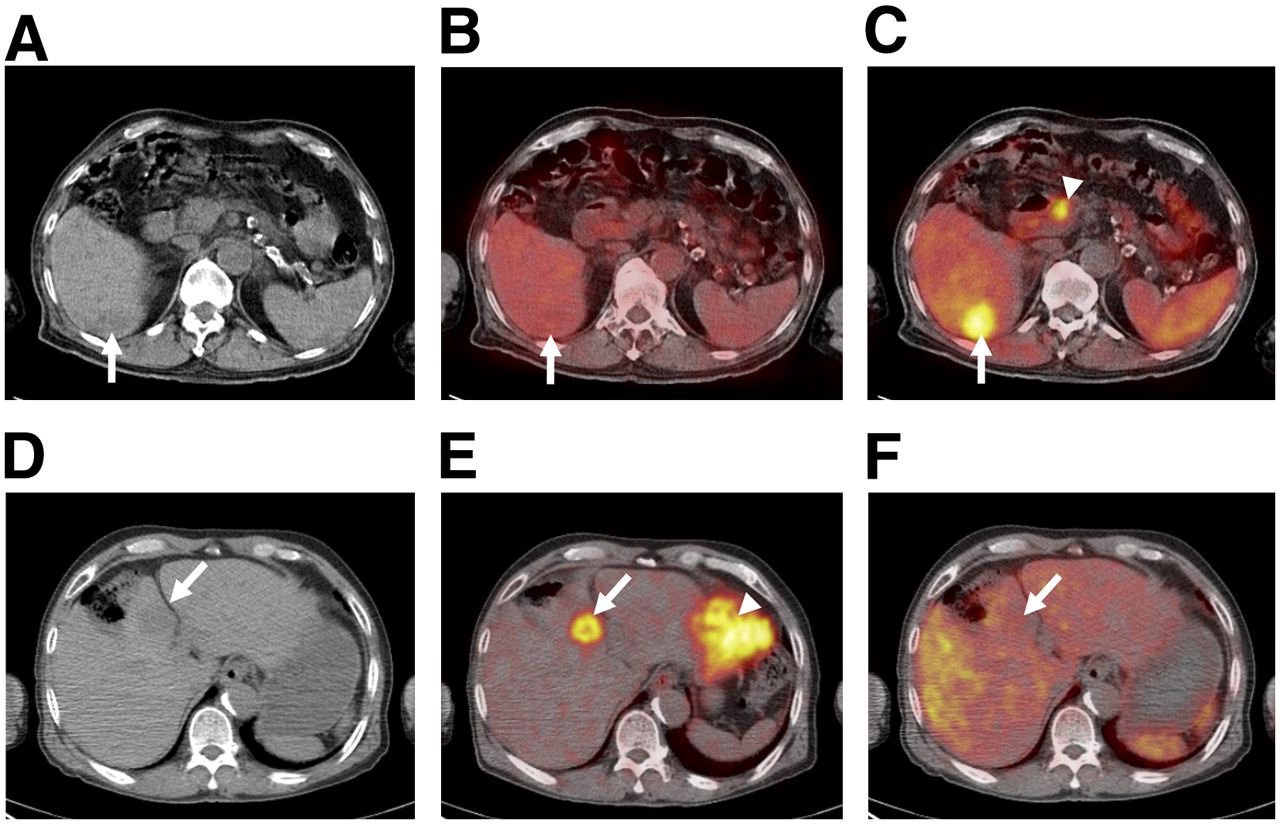
(A–C) Transaxial PET/CT images of 71-y-old man in whom HCC of Edmondson and Steiner's grade 1 was diagnosed. Unenhanced CT image shows hypoattenuating lesion in right lobe (arrow) (A), 18F-FDG PET/CT image shows no focal 18F-FDG accumulation in tumor (arrow) (B), and 11C-acetate PET/CT image shows focally increased uptake of 11C-acetate in tumor (arrow) and physiologic 11C-acetate uptake in pancreas (arrowhead) (C). (D–F) Transaxial PET/CT images of 65-y-old man with HCC of Edmondson and Steiner's grade 3. Unenhanced CT image shows hypoattenuating lesion (arrow) (D), 18F-FDG PET/CT image shows focal 18F-FDG accumulation in tumor (arrow) and physiologic FDG uptake in myocardium (arrowhead) (E), and 11C-acetate PET/CT image shows less intense accumulation in tumor (arrow) than in surrounding hepatic region (F).
Sensitivity of 18F-FDG and 11C-Acetate PET/CT in 90 Patients with Primary HCC: Lesion-Based Analysis of 110 Lesions
The sensitivity of 11C-acetate PET/CT for the detection of primary HCC was significantly associated with tumor size and number of tumors (Table 4). The sensitivity for detection of primary HCC on 11C-acetate PET/CT was 31.8%, 78.2%, and 95.2% in index lesions sized 1–2 cm, 2–5 cm, and 5 cm or more, respectively. Larger tumors were associated with significantly greater sensitivity (P < 0.001). Thirty-seven of 46 single lesions (80.4%) and 28 of 33 index lesions in patients with multiple lesions (84.8%) were positive for 11C-acetate uptake on PET/CT. Comparison of the 2 PET modalities indicates that 11C-acetate PET/CT had significantly higher sensitivity for detection of medium-sized tumors (2–5 cm), single tumors, and well-differentiated tumors (P < 0.05). The statistics for the maximum SUV of the 110 index lesions are summarized in Table 5.
Maximum SUV of 110 Index Lesions Considered to Be Positive in 90 Patients with Primary HCC
For detection of the 110 index lesions in patients with primary HCC, the sensitivity of 18F-FDG PET/CT was 60.9%, the sensitivity of 11C-acetate PET/CT was 75.4%, and the sensitivity of dual tracers was 82.7%. Among the 90 HCC lesions that underwent biopsy, 18F-FDG PET/CT detected 58 lesions (a sensitivity of 64.4%) and 11C-acetate PET/CT detected 76 lesions (a sensitivity of 84.4%). Of the 13 CCC lesions that underwent biopsy, all were positive by 18F-FDG PET/CT (a sensitivity of 100%) and 9 were positive by 11C-acetate PET/CT (a sensitivity of 69.2%).
Sensitivity for Detection of Metastatic HCC by PET/CT
For the 28 patients with modified UICC stage IVb HCC, patient-based analysis indicated that 19 (68%) were positive for 18F-FDG and 18 (64%) were positive for 11C-acetate. In this analysis, “positive” indicated positive for all index lesions and metastases in each patient (Table 2).
For lesion-based analysis, we evaluated the sensitivity of PET/CT in the detection of 35 metastatic HCC index lesions in 28 patients (Table 6). The locations of distant metastases were lung (20 lesions), bone (6 lesions), adrenal gland (4 lesions), abdominal peritoneum (3 lesions), brain (1 lesion), and left atrium of the heart (1 lesion). The overall sensitivity of 18F-FDG and 11C-acetate PET/CT in 35 index lesions of 28 patients with metastatic HCC was 85.7%, 77.0%, and 85.7% by 18F-FDG alone, 11C-acetate alone, and both tracers, respectively. All positive lesions detected by 11C-acetate (Fig. 4) were also positive on 18F-FDG PET/CT. Additionally, 5 index lesions of the lymph node metastases 1 cm or larger were evaluated, 3 of which were positive on 18F-FDG and 11C-acetate PET/CT.

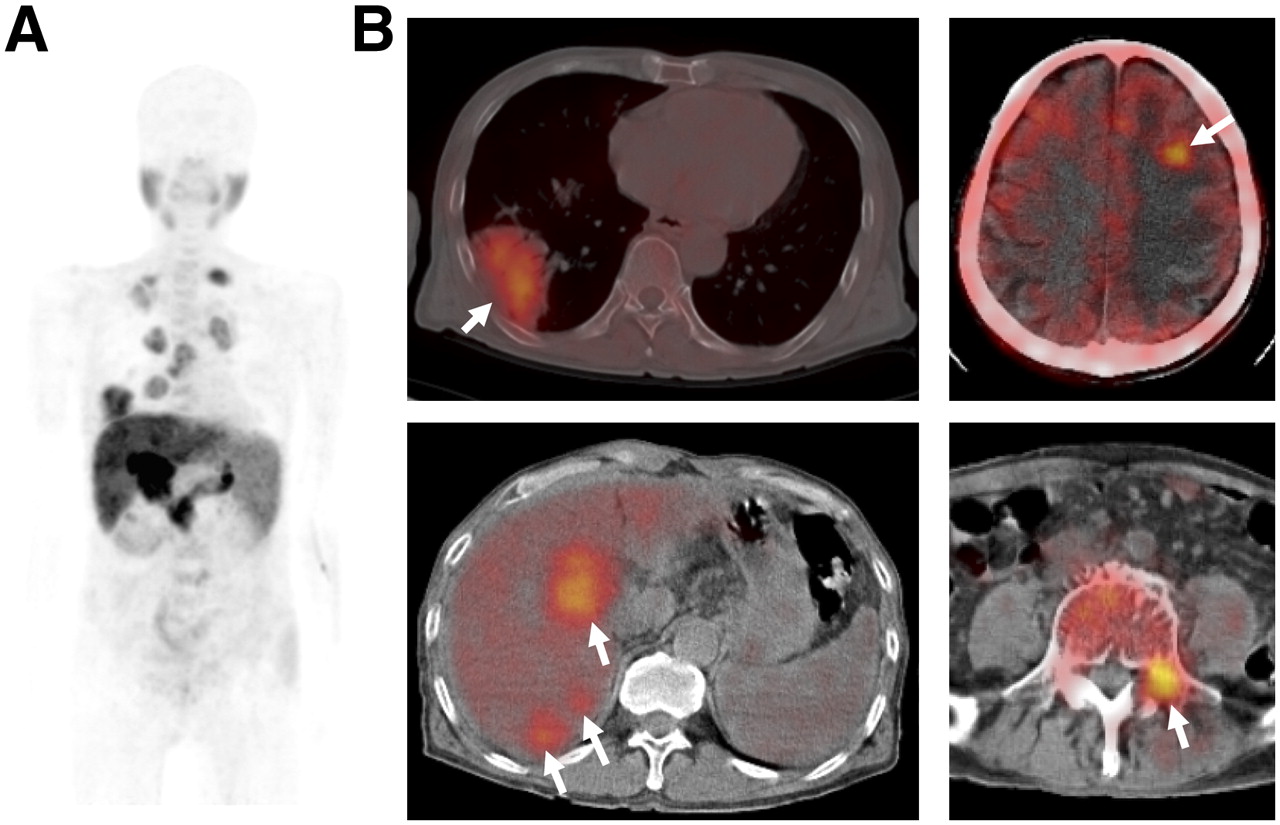
Transaxial PET/CT images of 63-y-old man in whom HCC of Edmondson and Steiner's grade 2 was diagnosed. 11C-acetate PET maximal-intensity image (A) and integrated PET/CT images (B) show HCC in liver and multiple metastatic lesions (arrows) in brain, lung, and spine.
Sensitivity of 18F-FDG and 11C-Acetate PET/CT in 28 Patients with Metastatic HCC: Lesion-Based Analysis of 35 Index Lesions
Of 20 small metastatic lesions (1–2 cm in diameter), 16 (80%) were detected on 18F-FDG PET/CT and 13 (65%) on 11C-acetate PET/CT. The sensitivity of both PET/CT tracers in the 15 metastatic lesions 2 cm or larger was the same: 93%. 18F-FDG PET/CT detected 100% of HCC metastases in bone (6 cases) and the abdominal peritoneum (3 cases). 18F-FDG PET/CT and 11C-acetate PET/CT detected 80% and 70% of lung metastases, respectively. Tumor differentiation did not show any significant differences in positive findings between the 2 modalities (90% vs. 90.9% in grades I and II and 76.9% vs. 53.8% in grades III and IV). In a comparison with poorly differentiated HCC, metastatic tumors from well-differentiated HCC had a greater number of positive results with 11C-acetate (P = 0.032). There was no significant difference between the 2 tracers in sensitivity for metastatic tumor size, location, or differentiation (Table 6).
DISCUSSION
PET/CT is used in HCC patients to detect extrahepatic metastases (11,17), predict outcome after resection (18,19), select liver transplantation candidates (20), and assess residual tumors after treatment with transcatheter arterial chemoembolization or radiofrequency ablation (21). The usefulness of these applications depends on the ability of PET/CT to detect small or atypical lesions—those for which no diagnostic studies with spiral CT or contrast-enhanced MRI are available, those in the liver, and those in extrahepatic areas. Previous studies, which enrolled few patients or were retrospective, reported inadequate sensitivity for 18F-FDG PET/CT in the detection of primary HCC (22–26) and suggested the addition of 11C-acetate PET/CT to improve the accuracy of PET/CT (6). However, these studies did not provide sufficient clinical detail for hepatologists and oncologists, the primary users of PET/CT for liver tumors.
In this study, the overall sensitivity for the detection of primary HCC was 60.9% for 18F-FDG alone, 75.4% for 11C-acetate alone, and 82.7% for both tracers. Although dual-tracer PET/CT had better sensitivity, the results of tumor size–based analysis were disappointing. For 1- to 2-cm HCCs, the sensitivity was 27.2% with 18F-FDG PET/CT and 31.8% with 11C-acetate PET/CT. Patient-based analysis indicated that none of the 5 patients with stage I HCC (modified UICC system) or very early stage HCC (BCLC system) had positive findings on 18F-FDG PET/CT (Table 2). Therefore, 18F-FDG and 11C-acetate PET/CT appear not to be useful for the detection of small lesions in the liver. The morphologic distinction of small HCC tumors from other regenerative nodules and premalignant dysplastic nodules can be difficult. Several PET/CT studies have suggested that differentiation of these nodules is possible, but our results do not support this conclusion. Biopsy-based analysis indicated that the sensitivity was 64.4% by 18F-FDG PET/CT and 84.4% by 11C-acetate PET/CT, apparently better than the overall sensitivity. However, we cannot exclude selection bias such as selection of a larger tumor for biopsy as an indexed lesion. Comparison with other benign tumors is not reasonable in clinical settings, and we therefore designed this study for only HCC and CCC patients. This study design (99 HCC patients, 13 CCC patients), therefore, could be considered as a case-only design, allowing computation of only the test sensitivity. All 13 cases of CCC had positive findings on 18F-FDG PET/CT. Although a previous study reported that 11C-acetate did not accumulate in CCC (6), the number of patients in this study was only 3, and 9 of our 13 CCC patients had positive findings on 11C-acetete PET/CT. Further study of the accuracy of 11C-acetate PET/CT in CCC may be required.
We found that both tracers were more readily taken up when there were large tumors or a large number of tumors. Our patient-based analysis indicated that clinical factors (age, sex, etiology, performance, Child–Pugh class) did not affect tracer uptake. Serum α-fetoprotein level and tumor stage (by the modified UICC and the BCLC systems) affected uptake only of 18F-FDG. For analyzing accuracy in the detection of small tumors or extrahepatic metastases, we prospectively enrolled more patients who had modified UICC stage I, II, and IVb, compared with the patient population of our previous report (27). A high rate of positive findings on 18F-FDG PET has been reported in patients with elevated serum α-fetoprotein levels (7) and in patients with poorly differentiated HCC (28).
Our study also showed a high positive rate for both 18F-FDG PET/CT and 11C-acetate PET/CT in poorly differentiated HCC. 11C-acetate accumulation was significantly better than 18F-FDG accumulation in well-differentiated HCC (50% vs. 71.4%), but there was no difference between the tracers in poorly differentiated HCC (Table 4). These results differ from those of a previous report (6), possibly because we used a different protocol for classifying tumor differentiation (2 categories in this study). However, in comparing the 2 tracers, 11C-acetate PET/CT yielded better results in male patients, in patients with better performance status, and in hepatitis B virus–positive patients. These results could be related to the biologic characteristics of the tumors and requires further study. A previous study reported that the 2-y recurrence-free survival rate of 18F-FDG PET/CT–negative HCC patients was significantly higher than that of 18F-FDG–positive HCC patients after liver transplantation (20). In this study, patients with positive 18F-FDG PET/CT findings for all indexed lesions had a significantly lower survival rate (Fig. 2). Because uptake of 18F-FDG PET/CT was associated with the level of serum α-fetoprotein, modified UICC stage, BCLC stage, tumor size, number of tumors, and presence or absence of portal vein invasion, multivariate analysis did not reveal positive 18F-FDG findings to be an independent risk factor for survival.
18F-FDG PET/CT might be useful in the evaluation of extrahepatic metastases, although data supporting this possibility are limited (7–9,11,12). To our knowledge, our study is the first that has prospectively evaluated the sensitivity of dual-tracer PET/CT for the detection of HCC metastases. Our patient-based analysis indicated that only 68% of stage IVb HCC patients (modified UICC system) had positive 18F-FDG findings for all lesions, including primary and metastatic HCC (Table 2). The finding of no 18F-FDG uptake by primary HCC lesions decreased the positive rate in this patient-based analysis. However, our lesion-based analysis of 35 indexed extrahepatic metastases indicated that 18F-FDG PET/CT detected 80% of lung metastases and 100% of bone metastases (Table 6). Lung and bone are the 2 major sites of HCC metastases. A metastatic tumor diameter greater than 1 cm had no effect on the sensitivity of detection by either tracer, and well-differentiated tumors were more likely to test positive with 11C-acetate. In contrast to detection of primary 1- to 2-cm HCCs, 18F-FDG PET/CT was more sensitive than 11C-acetate PET/CT for detecting metastases, although this difference was not statistically significant (Table 6). For metastatic HCC, dual-tracer PET/CT was not superior to 18F-FDG alone. A previous comparison of bone scintigraphy and 18F-FDG PET/CT reported that PET/CT was more sensitive, but that study provided no data about HCC (29). Evaluating the usefulness of 18F-FDG PET/CT for screening extrahepatic HCC metastases requires a further cost–benefit study.
Our study had some limitations. Histopathologic confirmation of metastases (the gold standard) was not possible in all cases. In our prospective study, we screened for metastatic HCC lesions and followed up with imaging studies or additional methods. The absence of HCC metastasis was confirmed by the level of serum α-fetoprotein and by imaging (chest radiography and routine spiral liver CT covering from the hila of the lungs through the symphysis pubis) performed at the 3-mo follow-up. The criteria we used to determine metastasis may have resulted in some underestimation, even though the study was prospective. Lymph node metastasis is not rare in advanced HCC (30), but confirmation of metastases to lymph nodes smaller than 1 cm in diameter is not possible through an imaging study. Moreover, previous transarterial chemoembolization, hepatitis, endoscopic procedures on varices, and peritonitis, all of which are common in HCC patients, can increase lymph node size. In our study, 3 of 5 index lesions of lymph nodes greater than 1 cm in diameter tested positive on both 18F-FDG PET/CT and 11C-acetate PET/CT (data not shown).
In summary, this study prospectively investigated the value of 18F-FDG and 11C-acetate PET/CT in the detection of primary and metastatic HCC. The addition of 11C-acetate to 18F-FDG PET/CT increases overall sensitivity in the detection of primary HCC but not of extrahepatic metastases. 18F-FDG PET/CT and 11C-acetate PET/CT have a low sensitivity in the detection of small primary HCCs, but 18F-FDG PET/CT has a comparatively high sensitivity in the detection of extrahepatic metastases. These results suggest that 18F-FDG PET/CT and 11C-acetate PET/CT appear not to be useful for the detection of small primary HCC but that 18F-FDG PET/CT may be useful for the screening of extrahepatic metastases of HCC.
Acknowledgments
We thank Dr. Ho Young Lee for his kind support with the interpretation of PET/CT scans. This work was financially supported by grant 0640390-1 from the National Cancer Center, Korea.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 10, 2008.
- Accepted for publication August 22, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [68Ga]Ga-RAYZ-8009: A Peptide PET Tracer for Targeting HCC in Humans
- Monitoring Response to Transarterial Chemoembolization in Hepatocellular Carcinoma Using 18F-Fluorothymidine PET
- Comparison of FDG-PET/CT for Cancer Detection in Populations With Different Risks of Underlying Malignancy
- 18F-FDG PET/CT Can Predict Survival of Advanced Hepatocellular Carcinoma Patients: A Multicenter Retrospective Cohort Study
- Radiation Dosimetry of Whole-Body Dual-Tracer 18F-FDG and 11C-Acetate PET/CT for Hepatocellular Carcinoma
- Underestimated Role of 18F-FDG PET for HCC Evaluation and Promise of 18F-FDG PET/MR Imaging in This Setting
- Oncologic PET/MRI, Part 1: Tumors of the Brain, Head and Neck, Chest, Abdomen, and Pelvis
- Detection of Hepatocellular Carcinoma with PET/CT: A Prospective Comparison of 18F-Fluorocholine and 18F-FDG in Patients with Cirrhosis or Chronic Liver Disease
- Imaging of Proliferation in Hepatocellular Carcinoma with the In Vivo Marker 18F-Fluorothymidine
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types