


Abstract
The purpose of this study was to retrospectively investigate the feasibility of 11C-choline PET, compared with 18F-FDG PET, for the detection of hepatocellular carcinoma (HCC). Methods: A total of 16 HCC lesions in 12 patients were examined with both 11C-choline PET and 18F-FDG PET. Tumor lesions were identified as areas of focally increased uptake, exceeding that of surrounding noncancerous liver tissue. For semiquantitative analysis, the tumor-to-liver (T/L) ratio was calculated by dividing the maximal standardized uptake value (SUV) in HCC lesions by the mean SUV in noncancerous liver tissue. Results: 11C-choline PET showed a slightly higher detection rate than did 18F-FDG PET for detection of HCC (63% vs. 50%, respectively), although this difference was not statistically significant. 11C-choline PET had a better detection rate for moderately differentiated HCC lesions but not for those poorly differentiated (75% vs. 25%, respectively). In contrast, 18F-FDG PET exhibited the opposite behavior, with corresponding detection rates of 42% and 75%, respectively. The mean 11C-choline SUV and T/L ratio in moderately differentiated HCC lesions were higher than those in poorly differentiated HCC lesions. In contrast, the mean 18F-FDG SUV and T/L ratio in poorly differentiated HCC were higher than those in moderately differentiated HCC. These differences, however, were also not statistically significant. Conclusion: 11C-choline PET had a better detection rate for moderately differentiated HCC lesions but not for poorly differentiated HCC lesions, whereas 18F-FDG PET produced the opposite result. 11C-choline is a potential tracer to complement 18F-FDG in detection of HCC lesions.
PET with 18F-FDG is a well-established functional diagnostic oncologic imaging technique that provides glucose metabolism information about lesions (1). However, it is known that 18F-FDG PET is not sensitive enough in the detection of hepatocellular carcinoma (HCC), especially in cases of low-grade HCC (2,3). Because the enzymatic activity of low-grade HCC resembles that of normal hepatocytes, the degree of 18F-FDG uptake in these tumors is low (4).
Recently, 11C-choline has been introduced as a new tumor-seeking agent for evaluation of a variety of malignant tumors (5–8). Choline is incorporated into cells through phosphorylcholine synthesis and is integrated into the cell membrane phospholipids (9). Malignant tumors may show a high proliferation and increased metabolism of cell membrane components, which will lead to an increased uptake of choline (10). To our knowledge, no reports have been published regarding the use of 11C-choline PET in the detection of HCC.
The purpose of the present study was to retrospectively investigate the feasibility of 11C-choline PET, compared with 18F-FDG PET, for the detection of HCC.
MATERIALS AND METHODS
Patients
This study was approved by our institutional review board, and written informed consent was obtained from all patients.
A total of 12 consecutive preoperative patients (5 men, 7 women; mean age, 71 y; age range, 58–78 y) with HCC who underwent both 11C-choline and 18F-FDG PET studies between February 2007 and February 2008 were retrospectively selected. Two patients were positive for hepatitis B virus surface antigen, 7 patients were positive for hepatitis C virus antibody, and 3 patients were negative for both. Nine patients had not been treated, and the other 3 patients had received transcatheter arterial embolization therapy more than 10 d before the PET study (mean interval, 33 d). Surgery was performed after the PET study (mean interval, 22 d). The grade of HCC differentiation was estimated according to Edmondson–Steiner classification (11).
Radiotracer Synthesis
11C-choline and 18F-FDG were produced using a cyclotron (HM-18; Sumitomo Heavy Industries Co.). 11C-choline was produced by proton bombardment of 14N2. The resultant 11CO2 was reduced to 11C-methanol by lithium aluminum hydride and subsequently converted to 11C-methyl iodide by addition of hydrogen iodide by a modified method of Pascali et al. (12). The radiochemical purity of the produced 11C-choline was greater than 99%. 18F-FDG was produced by proton bombardment of 18O-enriched water by a modified method of Toorongian et al. (13). The radiochemical purity of the produced 18F-FDG was greater than 95%.
PET
All acquisitions were performed using a scanner (ECAT EXACT HR+; Siemens/CTI Inc.). The imaging system enabled simultaneous acquisition of 63 transverse PET images per field of view (FOV), for a total axial FOV of 15.5 cm. In-plane resolution was approximately 4.6 mm, with an axial resolution of approximately 3.5-mm full width at half maximum. PET scans were performed in the 3-dimensional mode. A transmission scan was obtained using a 68Ge rod source to provide attenuation correction. PET images were reconstructed with ordered-subsets expectation maximization, using 2 iterations and 8 subsets.
Patients were instructed to fast for at least 5 h before the PET scan. For 18F-FDG PET, a normal blood glucose level in the peripheral blood was ensured. Five minutes after an intravenous injection of 11C-choline (6 MBq/kg) or 60 min after an intravenous injection of 18F-FDG (3.5 MBq/kg), attenuation-corrected whole-body scanning was performed from the skull base to the proximal thighs, with 2 and 3 min allowed per bed position for transmission and emission scans, respectively.
The 2 PET scans were acquired within 2 wk. No treatment was performed during this period of PET.
Data Analysis
PET and maximum-intensity-projection images were reviewed on a workstation (Sun Microsystems; Siemens/CTI Inc.) in the transverse, coronal, and sagittal planes. Each scan was interpreted independently by 2 experienced nuclear physicians who were unaware of clinical data and information pertaining to the corresponding scan, except for the results of the CT scan. CT scans were assessed for the exact localization of HCC lesions. Any difference of opinion was resolved by consensus.
Tumor lesions were identified as areas of focally increased uptake, exceeding that of surrounding noncancerous liver tissue. For semiquantitative analysis, regions of interest (ROIs) were placed over the entire 11C-choline– or 18F-FDG–avid lesion including the largest amount of radioactivity using the transverse PET image. For HCC lesions not visible on both or either of the 2 PET scans, an ROI was drawn on the respective scans in the region corresponding to the area of abnormality on the CT scan. For the noncancerous liver tissue ROI, a circular 2-cm ROI was placed on the noncancerous liver tissue. The standardized uptake value (SUV) was calculated by using the following formula: SUV = cdc/(di/w), where cdc is the decay-corrected tracer tissue concentration (in Bq/g); di is the injected dose (in Bq); and w is the patient's body weight (in g). The maximal SUV in the HCC lesion ROI and the mean SUV in the noncancerous liver tissue ROI were calculated for each ROI. As a contrast value, the tumor-to-liver (T/L) ratio was also calculated by dividing the HCC lesions SUV by the noncancerous liver tissue SUV.
Statistical Analysis
The detection rates of HCC using 11C-choline and 18F-FDG were compared using the paired χ2 test. Differences in semiquantitative parameters were analyzed by a Mann–Whitney U test and Wilcoxon signed rank test for unpaired and paired observations, respectively. Semiquantitative data were expressed as mean ± SD. Differences were considered statistically significant at the level of P < 0.05.
RESULTS
A total of 10 patients had a single lesion, and the remaining 2 patients had 3 lesions each. The histologic grade of HCC was moderately differentiated (grade II) in 12 lesions and poorly differentiated (grade III) in 4 lesions. Of all 16 HCC lesions, 8 were detected by 11C-choline PET only, 6 were detected by 18F-FDG PET only, and 2 were detected by both modalities. Figures 1–3⇓⇓ show typical cases of HCC lesion detection by 11C-choline only, by 18F-FDG only, and by both imaging techniques. Although 11C-choline PET showed a slightly higher detection rate than did 18F-FDG PET for detection of HCC (63% vs. 50%), the difference was not statistically significant.

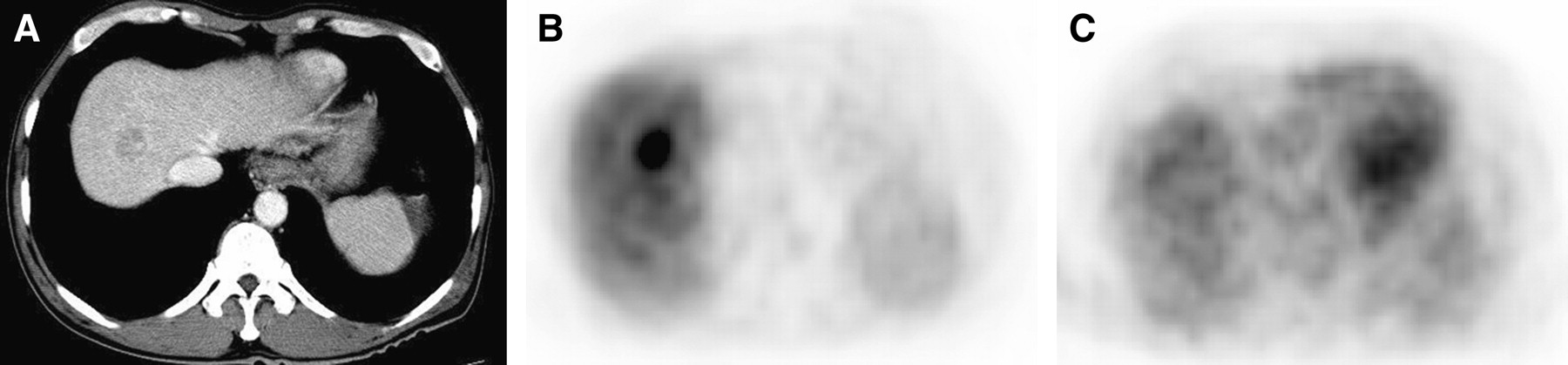
Images of 58-y-old man with moderately differentiated HCC. (A) Transverse CT image with contrast enhancement shows low-density mass in right lobe. (B) Transverse 11C-choline PET image shows increased uptake in lesion, compared with surrounding noncancerous liver tissue (SUV, 17.62; T/L ratio, 2.32). (C) Transverse 18F-FDG PET image shows no significant uptake in lesion, compared with surrounding noncancerous liver tissue (SUV, 3.10; T/L ratio, 1.34).

Images of 70-y-old woman with poorly differentiated HCC. (A) Transverse CT image with contrast enhancement shows low-density mass in right lobe. (B) Transverse 11C-choline PET image shows no significant uptake in tumor, compared with surrounding noncancerous liver tissue (SUV, 8.64; T/L ratio, 0.93). (C) Transverse 18F-FDG PET image shows increased uptake in tumor, compared with surrounding noncancerous liver tissue (SUV, 15.20; T/L ratio, 5.26).

Images of 58-y-old woman with moderately differentiated HCC. (A) Transverse CT image with contrast enhancement shows low-density mass in right lobe. (B) Transverse 11C-choline PET image shows increased uptake in tumor, compared with surrounding noncancerous liver tissue (SUV, 13.12; T/L ratio, 1.59). (C) Transverse 18F-FDG PET image shows slightly increased uptake in tumor, compared with surrounding noncancerous liver tissue (SUV, 4.65; T/L ratio, 1.38).
The mean (±SD) 11C-choline SUV was 15.23 ± 5.94 and the mean (±SD) T/L ratio was 1.46 ± 0.60 in all HCC lesions. The means (±SD) of the 18F-FDG SUV and T/L ratio were 4.80 ± 3.00 and 1.78 ± 1.08, respectively, in all HCC lesions. No significant difference was found between the 11C-choline and 18F-FDG T/L ratios in any HCC lesions.
A total of 9 of 12 (75%) moderately differentiated lesions could be visualized by 11C-choline PET, whereas only 5 of 12 (42%) such lesions could be detected by 18F-FDG PET. Thus, 11C-choline PET tended to be more sensitive than did 18F-FDG PET for moderately differentiated HCC lesions, although this difference was not statistically significant. In contrast, only 1 of 4 (25%) poorly differentiated lesions could be visualized by 11C-choline PET, and 3 such lesions (75%) were detected by 18F-FDG PET. Thus, 18F-FDG PET tended to be more sensitive than did 11C-choline PET for poorly differentiated HCC lesions, although this difference was also not statistically significant.
The mean (±SD) 11C-choline SUV and T/L ratio in moderately differentiated HCC lesions (16.79 ± 4.92 and 1.58 ± 0.53, respectively) were higher than those in poorly differentiated HCC lesions (10.56 ± 7.01 and 1.09 ± 0.72, respectively), but the differences were not statistically significant. In contrast, the mean (±SD) 18F-FDG SUV and T/L ratio in poorly differentiated HCC lesions (7.25 ± 5.37 and 2.61 ± 1.85, respectively) were higher than those in moderately differentiated HCC lesions (3.99 ± 1.33 and 1.50 ± 0.57, respectively), but the differences were not statistically significant.
DISCUSSION
In the present study of 12 patients with HCC, 11C-choline PET showed a slightly higher overall detection rate than did 18F-FDG PET for detection of HCC lesions (63% vs. 50%, respectively), although this difference was not statistically significant. In particular, for detection of moderately differentiated HCC lesions, the detection rates for 11C-choline PET and 18F-FDG PET were 75% versus 42%, respectively.
18F-FDG PET is a useful diagnostic method for metastatic liver tumors (14). A meta-analysis found excellent sensitivity (96%) and specificity (99%) for 18F-FDG PET in detecting hepatic metastasis from colorectal cancer (15). For HCC lesions, however, several investigators have shown that the sensitivity of 18F-FDG PET is not sufficiently high (50%–55%) (2,3,14,16). In the present study, the detection rate was only 50% for detection of HCC lesions by 18F-FDG PET, which is well in agreement with the results in previous reports (2,3,14,16). The activity of glucose-6-phosphatase is reported to vary widely, according to a differentiation grade of HCC: well-differentiated HCC cells are histologically closer to the normal liver cells than to the undifferentiated types (4,17). Thus, the abundance of glucose-6-phosphatase may render these tumors undetectable. However, a high positive rate of 18F-FDG accumulation has been reported in undifferentiated HCC lesions (16). Previous studies have also shown that the SUV and T/L ratio using 18F-FDG PET are significantly higher in poorly differentiated HCC lesions than in well-differentiated and moderately differentiated types and, therefore, reflect the degree of HCC differentiation (4,17). In the present study, a similar tendency was seen with tumor grade, although no statistical significance was detected.
The use of 11C-choline PET has been reported for the detection of tumors in organs such as the brain and prostate, in which 18F-FDG lacks sensitivity (5,6). However, to the best of our knowledge, no study has reported on the use of 11C-choline PET for the evaluation of HCC lesions. The precise uptake mechanism of 11C-choline in tumor cells is not well known. It has been suggested that tumor cells are characterized by their ability to incorporate choline actively to produce phosphatidylcholine, a cell membrane constituent, to facilitate rapid cell duplication (6). When 11C-choline is incorporated in tumors, it is rapidly phosphorylated (yielding 11C-phosphorylcholine) and chemically trapped inside the cell membranes (6).
In the present study, the overall detection rate of HCC lesions using 11C-choline PET was slightly better than that using 18F-FDG PET. This detection rate appears to be dependent on tumor differentiation, as demonstrated by a higher detection rate for moderately versus poorly differentiated HCC lesions using 11C-choline PET and 18F-FDG PET. These results suggest that the 2 tracers may complement each other in the detection of HCC lesions. Similar findings have been reported using 18F-fluorocholine (18) and 11C-acetate, a tracer assumed to be related to lipid synthesis (19), in HCC lesions. To overcome the limited utility of the 11C tracer due to its short half-life (∼20 min), 18F-fluorocholine has been developed. Talbot et al. showed that the sensitivity of 18F-fluorocholine (100%) for the detection of HCC lesions was better than that of 18F-FDG (55.6%) (18). A trend toward a higher 18F-fluorocholine SUV in well-differentiated HCC lesions than in poorly differentiated HCC lesions is demonstrated, although the difference was not statistically significant (18). Ho et al. reported that the overall sensitivity of 11C-acetate (87.3%) for the detection of HCC lesions was better than that of 18F-FDG (47.3%) (19). However, 11C-acetate was not sensitive for the detection of poorly differentiated HCC lesions (19). Furthermore, a statistically significant relationship between tumor differentiation and T/L ratio for 18F-FDG PET and 11C-acetate PET exists (19). Ho et al. also evaluated the sensitivity of metastatic HCC lesions with both 11C-acetate and 18F-FDG, compared with that of 18F-FDG or 11C-acetate alone (20). In their results, dual-tracer PET/CT showed an excellent sensitivity (98%) (18F-FDG PET/CT had 79% and 11C-acetate PET/CT had 64%) (20). The detection rate for HCC lesions in the present study was slightly lower than that obtained in these previous studies (18,19). One of the reasons for this difference may be because of the small sample size and the construction of the sample in the present study versus the previous studies (18,19). The percentage of well-differentiated HCC lesions in the previous studies was 33%–35% (18,19), although we had no well-differentiated HCC lesions. Furthermore, because the background 18F-fluorocholine levels in the liver parenchyma are low, areas exhibiting their accumulations can be visualized in good contrast to other areas.
A limitation of the present study was the small size of the sample, in which we had no well-differentiated and very few poorly differentiated HCC lesions. This may explain the lack of statistical significance of differences observed. Three patients had received transcatheter arterial embolization therapy before the PET study. The detection rates of HCC lesions were analyzed using visual, not SUV, analysis. The value of the present data is also limited by the retrospective character of the study. Further prospective studies involving a larger number of patients are required to determine the clinical usefulness of 11C-choline PET for detection of HCC lesions.
CONCLUSION
11C-choline PET had a better detection rate for moderately differentiated HCC lesions but not for poorly differentiated HCC lesions, whereas 18F-FDG PET demonstrated the opposite behavior. The use of 11C-choline as a tracer complementary to 18F-FDG in detection of HCC lesions seems to be a possibility.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 13, 2008.
- Accepted for publication April 16, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preliminary Study of 11C-Choline PET/CT for T Staging of Locally Advanced Nasopharyngeal Carcinoma: Comparison with 18F-FDG PET/CT
- Detection of Hepatocellular Carcinoma with PET/CT: A Prospective Comparison of 18F-Fluorocholine and 18F-FDG in Patients with Cirrhosis or Chronic Liver Disease
- Reproducibility of [11C]Choline-Positron Emission Tomography and Effect of Trastuzumab
- Imaging of Proliferation in Hepatocellular Carcinoma with the In Vivo Marker 18F-Fluorothymidine
- Prediction of Tumor Recurrence by 18F-FDG PET in Liver Transplantation for Hepatocellular Carcinoma
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET