


Abstract
This study aimed to assess the prognostic value of 18F-FDG uptake in hepatocellular carcinoma (HCC) patients who had transarterial chemoembolization (TACE) or concurrent intraarterial chemotherapy with external-beam radiotherapy (CCRT) and to compare the prognosis between patients treated with TACE and those with CCRT according to 18F-FDG uptake. Methods: Two hundred fourteen intermediate–to–advanced-stage HCC patients without extrahepatic metastasis who underwent staging 18F-FDG PET/CT before TACE (153 patients) or CCRT (61 patients) were recruited from 7 hospitals. Progression-free survival (PFS) and overall survival (OS) were compared using an optimal cutoff value for tumor-to-normal liver uptake ratio (TLR). Further, PFS and OS were compared according to treatment modalities (TACE vs. CCRT) using the same TLR cutoff value. Results: On multivariate analysis, age and TLR were independent prognostic factors for PFS (P < 0.050). For OS, Child–Pugh classification and TLR were independent prognostic factors (P < 0.050). When the TLR was greater than 2.0, patients treated with CCRT showed significantly better PFS and OS than those treated with TACE after adjusting for tumor size and number (P = 0.014, for all). In contrast, there was no significant difference in PFS and OS between patients treated with TACE or CCRT when the TLR was 2.0 or less. Conclusion: 18F-FDG uptake was an independent prognostic factor for PFS and OS in HCC patients treated with TACE or CCRT. Especially, in HCCs with high 18F-FDG uptake, patients treated with CCRT showed better survival than those treated with TACE. 18F-FDG PET/CT may help determine the treatment modality for intermediate–to–advanced-stage HCCs.
- hepatocellular carcinoma
- prognosis
- 18F-FDG PET
- transarterial chemoembolization
- concurrent chemoradiotherapy
For patients with hepatocellular carcinoma (HCC), the Barcelona Clinic Liver Cancer (BCLC) staging system has been used to select the optimal treatment and predict the prognosis (1). In patients with very early–to–early stage HCC, curative surgical resection can be performed, and a 5-y survival rate of more than 60% has been reported (2). With only about 30% of patients able to undergo curative treatments, most HCC patients are referred for noncurative treatments (1,3). For intermediate–to–advanced-stage HCC patients without extrahepatic metastasis, transarterial chemoembolization (TACE) is the first-line treatment (1,4,5); however, diverse treatment modalities have been used to improve the treatment response and prognosis (6,7). Local radiotherapy has been effective in controlling HCC progression (8), and concurrent intraarterial chemotherapy with external-beam radiotherapy (CCRT) has recently been considered as an attractive alternative treatment strategy for locally advanced HCC (9–11).
18F-FDG PET/CT has been effective for staging and detecting extrahepatic metastasis and recurrence in HCC patients, although 18F-FDG PET/CT shows low sensitivity for detecting intrahepatic HCCs (12–14). More importantly, as the degree of 18F-FDG uptake is associated with tumor differentiation and aggressiveness (15,16), treatment response and prognosis appear to differ between HCCs with high and low 18F-FDG uptake (17,18). However, no study has evaluated the potential of 18F-FDG uptake in deciding treatment modalities with better prognosis in HCC patients.
The purpose of this retrospective multicenter cohort study was to assess the prognostic value of 18F-FDG uptake in intermediate–to–advanced-stage HCC patients without extrahepatic metastasis and to compare prognosis between patients treated with TACE and those treated with CCRT as an initial treatment according to 18F-FDG uptake.
MATERIALS AND METHODS
Patients
This retrospective, multicenter cohort study was approved by the institutional review boards of 7 participating university hospitals (Dongsan Medical Center, Incheon St. Mary’s Hospital, Kyung Hee University Hospital, Samsung Medical Center, Seoul St. Mary’s Hospital, Uijeongbu St. Mary’s Hospital, and Yonsei University Health System), and the requirement to obtain informed consent was waived.
We retrospectively reviewed the medical records of 847 patients with HCC who underwent staging 18F-FDG PET/CT before treatment between January 2009 and December 2010 at the 7 participating institutions (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Of these patients, 214 patients were enrolled in the study according to the following inclusion criteria (Fig. 1): patients with HCC diagnosis by histopathology or noninvasive diagnostic criteria of the American Association for the Study of Liver Disease guidelines (3), no treatment before 18F-FDG PET/CT, BCLC stage B or C, no extrahepatic metastasis on staging work-up studies, and patients who underwent TACE or CCRT as an initial treatment. Routine staging work-up including physical examination, blood tests, contrast-enhanced liver CT, 18F-FDG PET/CT, and liver MRI (if needed) were completed before initial treatment. All the clinical data of enrolled patients were collected and managed with an Internet-based Clinical Research and Trial Management System of the Korea National Institute of Health.
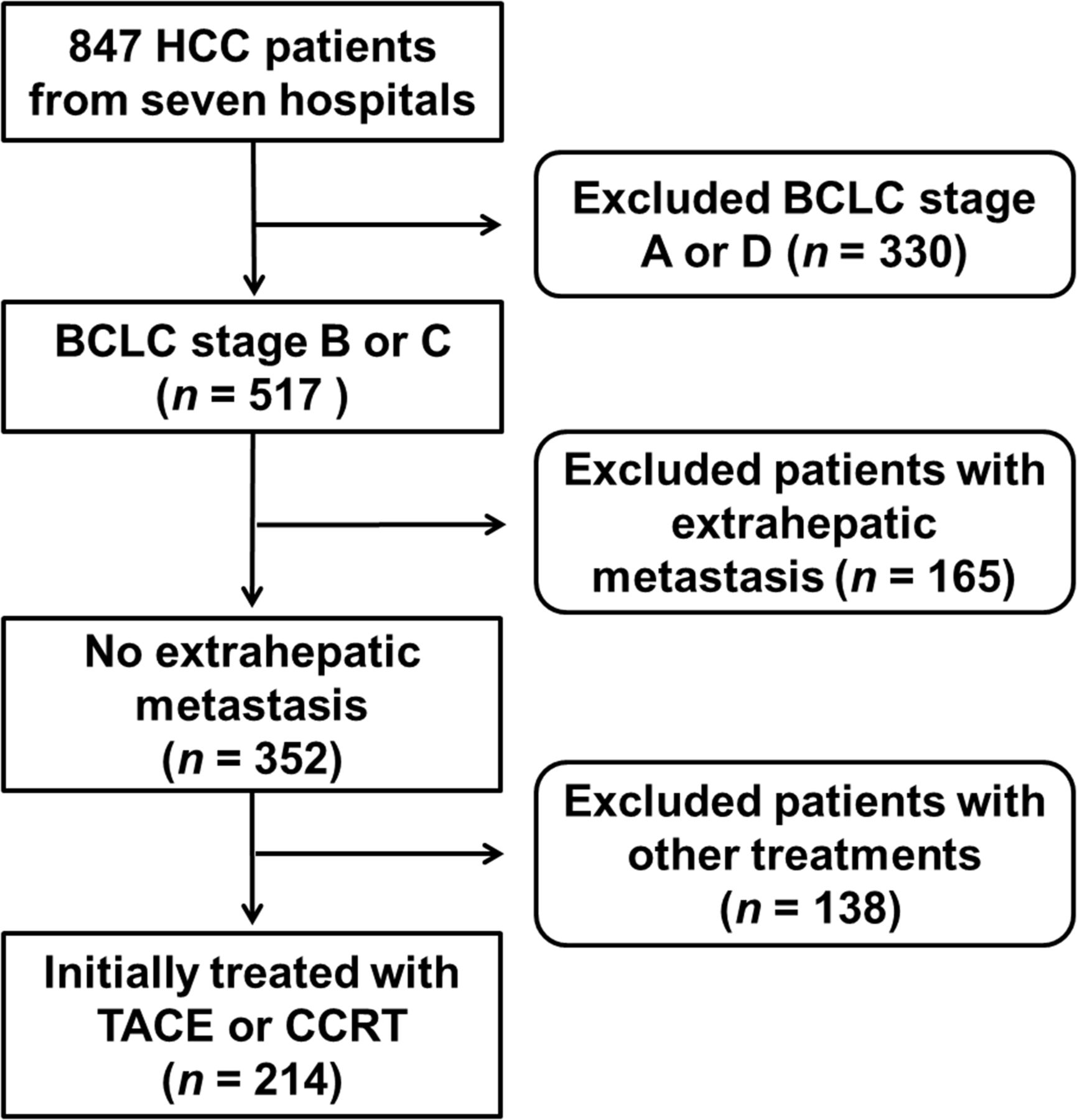
Flowchart of patient selection.
18F-FDG PET/CT
18F-FDG PET/CT was performed with a dedicated PET/CT scanner (Discovery Ste [GE Healthcare] for Dongsan Medical Center, Incheon St. Mary’s Hospital, Samsung Medical Center, and Yonsei University Health System; Gemini TF16 [Philips Healthcare] for Kyung Hee University Hospital; Biograph TruePoint [Siemens Healthcare] for Seoul St. Mary’s Hospital, Uijeongbu St. Mary’s Hospital, and Yonsei University Health System; and Biography Duo [Siemens Healthcare] for Seoul St. Mary’s Hospital). All patients fasted for at least 6 h before intravenous administration of 18F-FDG, and the blood glucose levels of enrolled patients, which were measured before the injection of 18F-FDG, were 140 mg/dL or less. A dose of 5.5 MBq/kg of 18F-FDG was intravenously administered for Discovery STe and 6.0 MBq/kg for Biograph TruePoint and Biograph Duo, and 333 MBq of 18F-FDG were administered for Gemini TF16. In all institutions, 60 min after injection of 18F-FDG, a PET/CT scan was acquired from the cerebellum to the proximal thighs. First, a CT scan was obtained without contrast enhancement. Immediately after CT acquisition, a PET scan was obtained in 3-dimensional mode. PET images were reconstructed with an iterative reconstruction algorithm using CT images for attenuation correction.
TACE and CCRT
In patients without portal vein tumor thrombosis, TACE was considered to be the standard treatment; however, in patients with large tumors of 10.0 cm or more, CCRT was recommended. In patients with portal vein tumor thrombosis, TACE or CCRT was recommended according to the clinical conditions of the patients. The median interval between 18F-FDG PET/CT and the initial treatment was 3.0 d (range, 1.0–45.0 d). For patients treated with TACE, celiac and superior mesenteric angiography was initially performed to evaluate tumor-feeding arteries and portal vein tumor thrombosis. Afterward, the feeding artery was selectively catheterized and the chemotherapeutic agents were administered as an oil emulsion, followed by the embolic materials. In patients with residual viable HCC on follow-up imaging studies, repeated TACE was performed. For patients treated with CCRT, 3-dimensional conformal radiotherapy was initially performed at a total dose of 45 Gy in 25 fractions of 1.8 Gy over 5 wk. Concurrent continuous-infusion hepatic arterial 5-fluorouracil was delivered during the first and fifth weeks of radiotherapy through a percutaneous hepatic arterial catheter. One month after CCRT, 5-fluorouracil and cisplatin were administered every 4 wk for 3–12 cycles according to treatment response. After initial treatment, all patients were closely monitored based on physical examinations, serum α-fetoprotein (AFP) level, and liver CT. The median duration of clinical follow-up was 10.7 mo (range, 0.3–67.4 mo).
Image Analysis
The 18F-FDG PET/CT, contrast-enhanced liver CT, and liver MR images of 847 HCC patients were transferred using the Digital Imaging and Communications in Medicine protocol and stored on a server at the designated center (National Cancer Center, Goyang-si Gyeonggi-do, Korea). The PET/CT images of 214 patients enrolled in the study were retrospectively reviewed by 2 board-certified nuclear medicine physicians. Discrepancies between the interpreters were resolved by a consensus reading. First, the PET/CT and contrast-enhanced CT images of all patients were visually assessed and registered using a fusion module provided by the commercially available imaging software (MIM-6.4; MIM Software Inc.). Afterward, a spheric-shaped volume of interest was drawn for each HCC on contrast-enhanced CT images, and the SUVmax was calculated as follows: (decay-corrected activity [kBq]/tissue volume [mL])/(injected 18F-FDG activity [kBq]/body mass [g]). In patients with multiple HCC lesions, the tumor showing the highest SUVmax was measured. For the measurement of 18F-FDG uptake in the normal liver, 3 spheric-shaped, 1-cm-sized volumes of interest were drawn in the liver, 2 in the right lobe, and 1 in the left lobe, at a location for which the HCC was not detected on contrast-enhanced CT or MRI. The SUVmean of the 3 volumes of interest was calculated and defined as the SUVmean of the normal liver. The uptake ratio of SUVmax of HCC to mean SUVmean of the normal liver (tumor–to–normal liver uptake ratio [TLR]) was calculated for each patient.
Statistical Analysis
Characteristics of patient groups treated with TACE or CCRT were compared using the Student t test and the χ2 test. Kaplan–Meier survival analysis was performed to calculate the cumulative progression-free survival (PFS) and overall survival (OS). Survival time was defined as the time from initial treatment to the date of the detection of disease progression (for PFS) or death (for OS) or to the date of the last follow-up visit. Disease progression was defined as progressive disease (≥20% increase in the size of known HCC lesions from baseline or occurrence of newly developed metastases on follow-up imaging studies) according to RECIST, version 1.1. The prognostic values of the variables were assessed using a log-rank test in univariate analysis and a Cox proportional hazards regression test in multivariate analysis. All continuous variables were dichotomized according to specific cutoff values. The optimal cutoff values were determined using receiver-operating-characteristic curve analysis. Cumulative PFS and OS stratified by the TLR cutoff value were compared between the patients treated with TACE and those with CCRT using Kaplan–Meier survival analysis with a log-rank test. Statistical analyses were performed using SPSS (version 20.0 for Windows, SPSS Inc.), and P values less than 0.050 were considered statistically significant.
RESULTS
Patient Characteristics
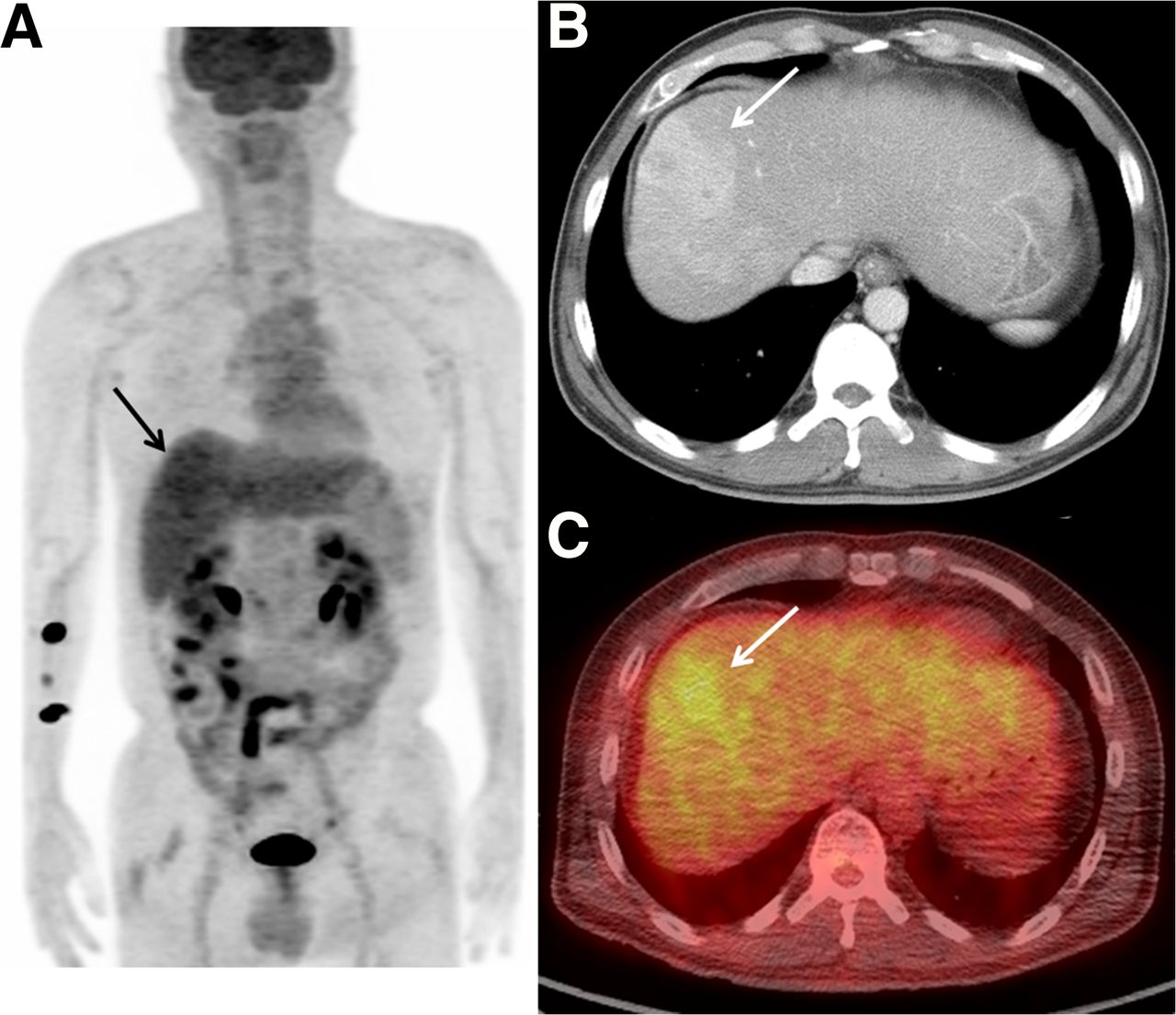
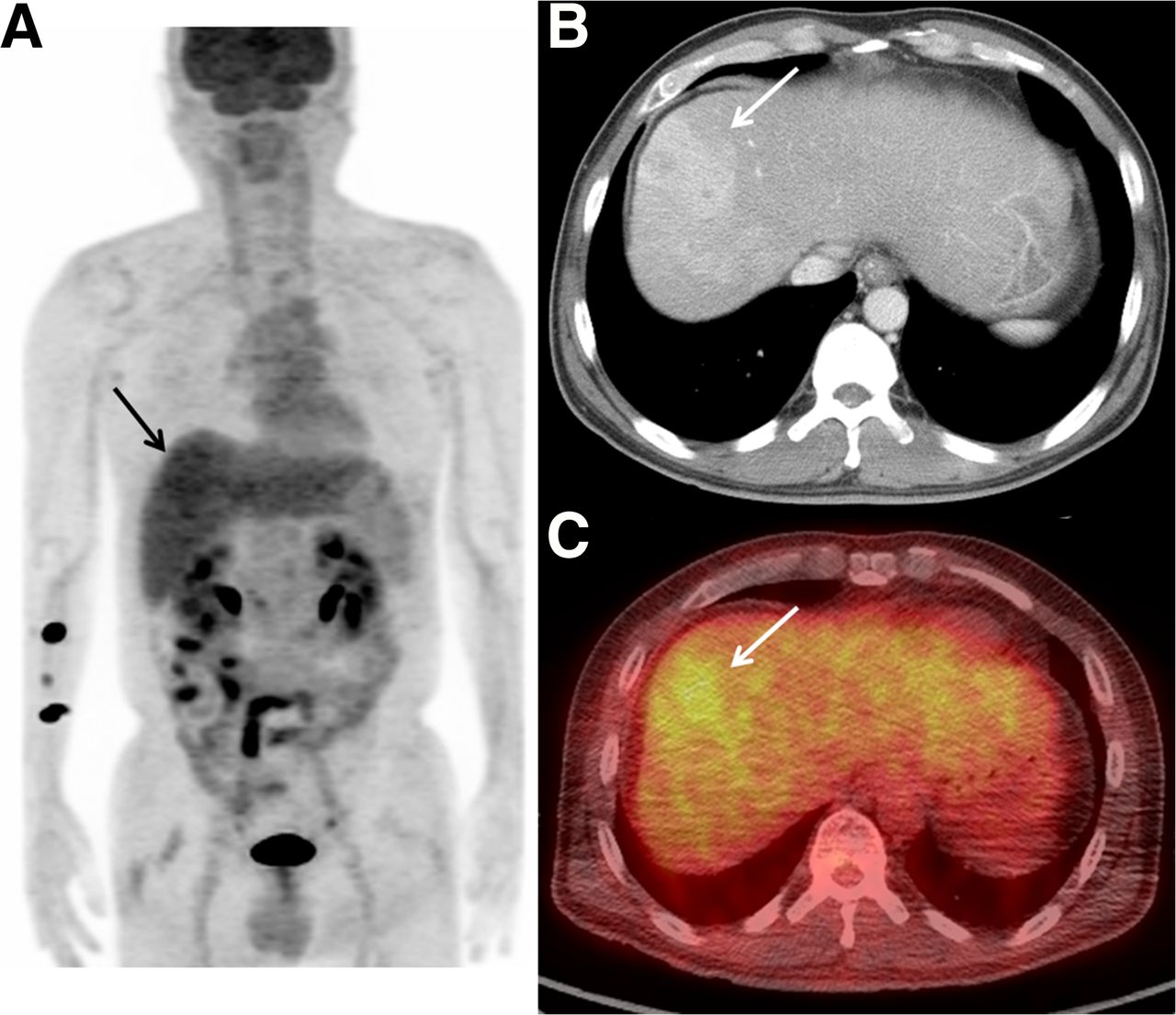
The characteristics of enrolled patients are shown in Table 1. Of 214 patients, 108 patients (50.5%) had portal vein tumor thrombus and were classified as BCLC stage C, whereas the remaining 106 patients (49.5%) were stage B. As an initial treatment, 153 patients (71.5%) underwent TACE and the remaining 61 patients (28.5%) underwent CCRT. The patient group treated with CCRT (Fig. 2) had a significantly larger tumor size, higher TLR, and higher proportion of portal vein tumor thrombosis (P < 0.050); meanwhile, the patient group with TACE (Fig. 3) showed a higher proportion of multiple tumors (P < 0.001). During follow-up, 152 patients (71.0%) experienced disease progression, and 172 patients (80.4%) died. The median PFS and OS were 7.5 and 12.4 mo, respectively.
Patient Characteristics

Maximal-intensity-projection image (A) and transaxial fused image (C) of 18F-FDG PET/CT and a contrast-enhanced liver CT (B) image of a 65-y-old man with BCLC stage B HCC. Contrast-enhanced CT image (B) shows enhanced HCC lesion with internal necrosis in right lobe of liver (arrow). PET/CT image (C) shows intensely increased 18F-FDG uptake in mass, with TLR of 6.6 (arrow). Patient underwent TACE, and cancer progressed with pulmonary metastases 2.0 mo after TACE. Patient died 8.2 mo after initial treatment.
Maximal-intensity-projection image (A) and transaxial fused image (C) of 18F-FDG PET/CT and contrast-enhanced liver CT (B) image of a 54-y-old man with HCC. On contrast-enhanced CT image (B), infiltrative HCC is shown (arrow). HCC reveals mildly increased 18F-FDG uptake, with TLR of 1.6 (arrow). Patient was diagnosed at BCLC stage C due to portal vein tumor thrombosis on CT images and underwent CCRT. HCC progressed with intrahepatic metastases 15.6 mo after CCRT, and patient died 19.8 mo after initial treatment.
Prognostic Significance of 18F-FDG PET and Clinical Factors
Age, sex, etiology, Child–Pugh classification, treatment modality, tumor size and number, portal vein tumor thrombosis, serum AFP level, and TLR were evaluated as variables in survival analysis. The cutoff values, determined by receiver-operating-characteristic curve analyses, for age, tumor size, serum AFP level, and TLR were 60 y, 6.0 cm, 500.0 ng/dL, and 2.0, respectively. The prognostic significance of the variables for PFS and OS is shown in Tables 2 and 3. On univariate analysis, age, tumor size, portal vein tumor thrombosis, and TLR (Fig. 4A) were significant prognostic factors for PFS (P < 0.050). For OS, Child–Pugh classification, serum AFP level, tumor size, portal vein tumor thrombosis, and TLR (Fig. 4B) were significant prognostic factors (P < 0.050).
Median Survival Time and Significance of Prognostic Factors for PFS
Median Survival Time and Significance of Prognostic Factors for OS
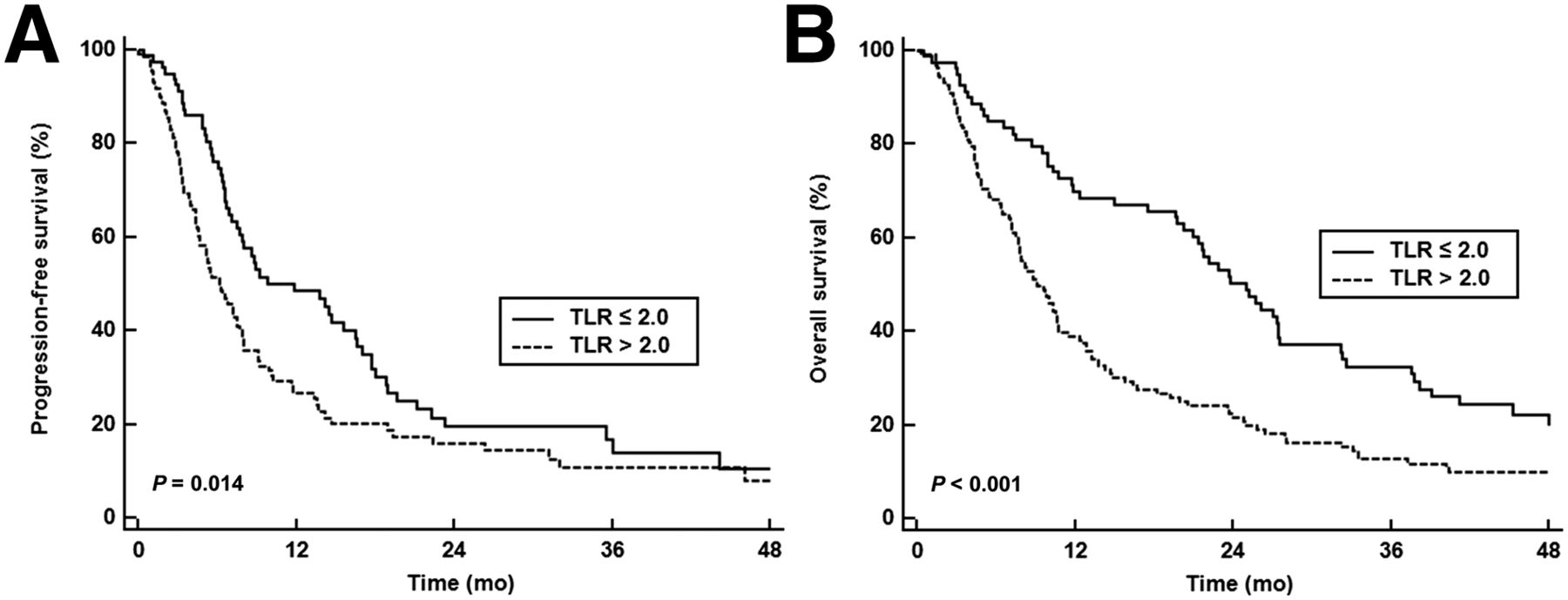
Cumulative PFS (A) and OS (B) curves according to TLR of HCC.
On multivariate analyses using significant variables in the univariate analyses, age and TLR were independent prognostic factors for PFS (Table 2; P < 0.050), and Child–Pugh classification and TLR were determined to be significant prognostic factors for OS (Table 3; P < 0.050).
Comparison of Prognosis Between TACE and CCRT Stratified by 18F-FDG Uptake
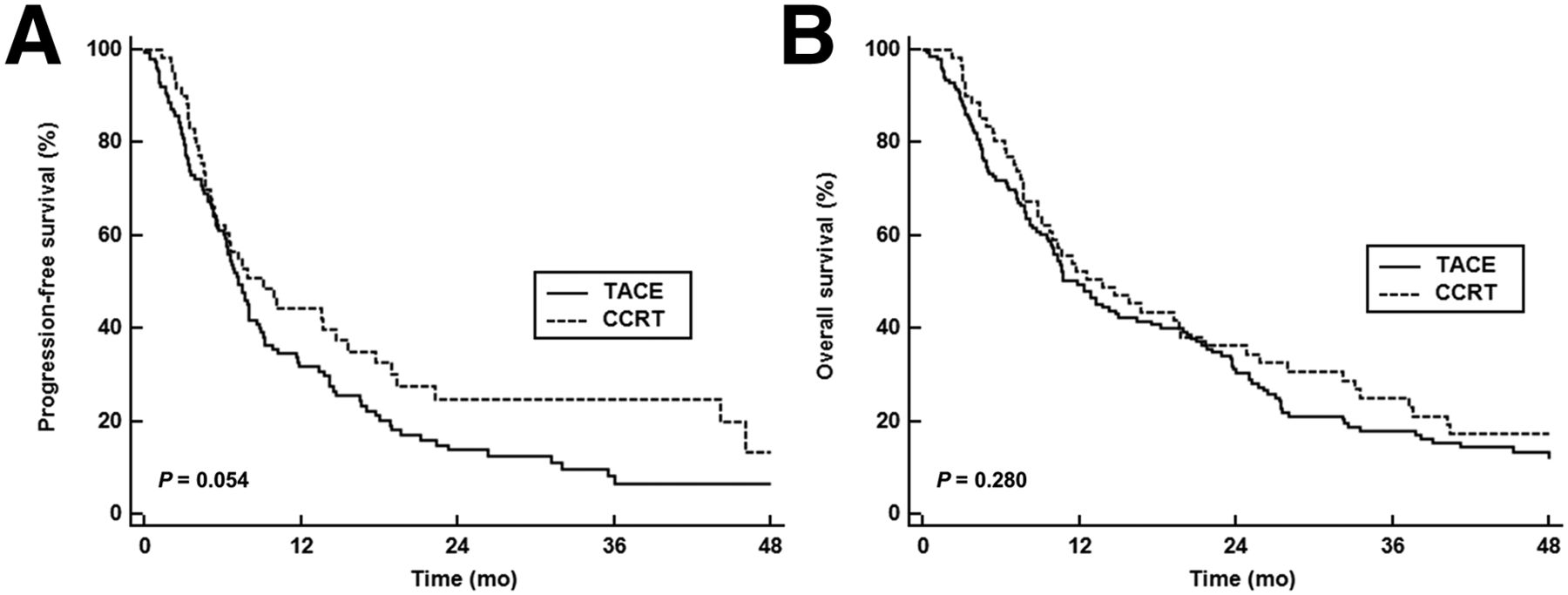
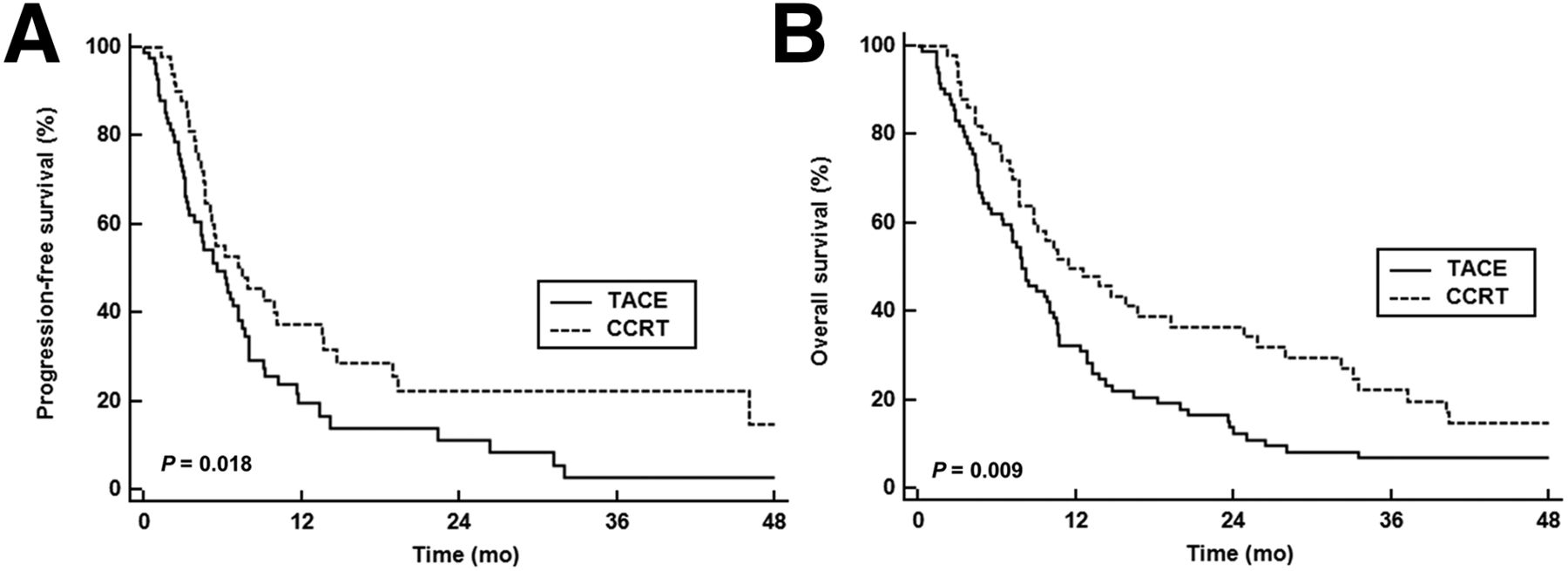
There was no significant difference in PFS (Fig. 5A) and OS (Fig. 5B) between TACE and CCRT in all patients (P = 0.054 for PFS and P = 0.280 for OS). PFS and OS between patients treated with TACE and those with CCRT were compared according to the TLR cutoff value (Table 4). In the patient group with a TLR greater than 2.0, the patients treated with CCRT showed a significantly better PFS (P = 0.018, Fig. 6A) and OS (P = 0.009, Fig. 6B) than the patients treated with TACE. The median OS for patients treated with CCRT was 11.4 mo, whereas the median OS for patients treated with TACE was only 7.9 mo. Because both tumor size and number can potentially act as confounding factors, we further evaluated an association between treatment modality and prognosis after adjusting for tumor size and number. Even after adjusting for tumor size and number, the patients treated with CCRT still showed a lower progression risk (P = 0.014; hazard ratio, 0.61; 95% confidence interval, 0.41–0.90) and a lower mortality risk (P = 0.014; hazard ratio, 0.58; 95% confidence interval, 0.37–0.89) than those treated with TACE. In contrast, there were no significant differences in PFS (P = 0.187) and OS (P = 0.927) between patients treated with TACE and those with CCRT in the patient group with a TLR of 2.0 or less.

Cumulative PFS (A) and OS (B) curves in patients treated with TACE or CCRT.
Median Survival for Patients Treated with CCRT and TACE According to TLR

Cumulative PFS (A) and OS (B) curves in patients with TLR greater than 2.0 according to treatment (TACE or CCRT).
DISCUSSION
In the present multicenter retrospective study, the prognostic value of 18F-FDG uptake for each tumor was assessed in intermediate–to–advanced-stage HCC patients who underwent TACE or CCRT. Currently, the value of 18F-FDG uptake as an independent prognostic factor is controversial in this group of patients (18–22); however, in this study, we found that the TLR of HCC was a significant independent prognostic factor for both PFS and OS. The patients with a TLR of 2.0 or less had a median PFS of 9.8 mo and a median OS of 24 mo, whereas a median PFS of 6.2 mo and a median OS of less than 10 mo were found in patients with a TLR greater than 2.0. Furthermore, in patients with a TLR greater than 2.0, patients treated with CCRT showed significantly lower disease progression and mortality risk than those treated with TACE.
It is important to know whether 18F-FDG uptake on PET/CT at the time of staging is associated with clinical outcomes. However, the more clinically relevant question might be whether the finding would be helpful in selecting treatments with subsequent changes in patient prognosis. In this regard, we assessed the difference in clinical outcomes between TACE and CCRT according to the 18F-FDG uptake of HCC. In the patient group with a TLR greater than 2.0, patients treated with TACE showed a significantly worse PFS and OS than patients treated with CCRT even after adjusting for tumor size and number. TACE is considered as the treatment of choice for intermediate-to-advanced HCC without extrahepatic metastases (1,4,5). However, it could be that it is insufficient for achieving a complete response in large advanced HCCs (23). In fact, hepatic artery perfusion, which is related to successful TACE, is negatively correlated with 18F-FDG uptake of HCC and has been found to significantly decrease in aggressive HCC (24–26).
Unlike TACE, CCRT, a concurrent selective regional chemotherapy with regional radiotherapy, has been shown to be an attractive, alternative treatment modality that intensifies the effect of local therapy while minimizing therapy-related complications (9,10). In this study, patients treated with CCRT had larger tumors but significantly better PFS and OS than those with TACE. Given that the response to the initial treatment is a strong predictor for clinical outcome (27), CCRT seems promising for intermediate-to-advanced HCCs with increased 18F-FDG uptake. Recently, multimodality treatment involving radiotherapy has been proven to be effective in improving local tumor control in the setting of neoadjuvant, adjuvant, and definitive treatment (9,28,29). In multimodality treatment, chemotherapy can control micrometastasis as well as play the role of a radiosensitizer (30). Because HCCs with aggressive features and rapid tumor growth show high 18F-FDG uptake (15,31), the efficacy of multimodality treatment might be more prominent in patients with a high 18F-FDG uptake than that of monotherapy. This hypothesis may explain why patients treated with CCRT, a multimodality treatment, had better PFS and OS than those with TACE as a monotherapy, particularly among patients with a high18F-FDG uptake.
In the patient group with low 18F-FDG uptake, no significantly different prognosis was noted between TACE and CCRT, implying that the prognosis of well-differentiated or indolent HCCs might be less affected by the treatment modality. However, in this study, the 18F-FDG uptake of most patients was above the cutoff value and only a small number of patients were included in the patient group with low 18F-FDG uptake. Therefore, more studies with a larger population are needed to compare the prognosis between treatments in patients with a low 18F-FDG uptake.
There were several limitations in this study. First, because this was a retrospective cohort study, the results were potentially predisposed to selection bias due to the lack of randomization. Further prospective, multicenter, randomized, registration studies are needed to confirm the results of the present study. Second, volumetric parameters such as metabolic tumor volume and total lesion glycolysis rather than 18F-FDG uptake alone have acted as better prognostic factors in various kinds of cancers (32,33); however, there is no consensus on how to measure the volumetric parameters of HCC (18). Therefore, only the TLR was measured in the study. Last, PET/CT images were acquired from multiple scanners at multiple medical centers. Regardless of the technical feasibility of the standardization of scanners with a phantom, this can often be impractical in routine clinical practice because of the complexity of the procedures. Instead, use of the TLR can be a beneficial, alternative PET/CT parameter that involves normalizing tumor values to the internal reference organ value.
CONCLUSION
In the present multicenter, retrospective, cohort study, 18F-FDG uptake of HCCs was proven to be an independent prognostic factor for PFS and OS in intermediate–to–advanced-stage HCC patients without extrahepatic metastasis who underwent TACE or CCRT. More important, only among patients with a high 18F-FDG uptake, those treated with CCRT had a significantly better PFS and OS than those treated with TACE. In contrast, there were no significant differences in PFS and OS between CCRT and TACE in patients with low 18F-FDG uptake. These results may support further prospective studies evaluating the value of CCRT as an alternative initial treatment for intermediate-to-advanced HCC patients with a high 18F-FDG uptake.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This research was supported by the Korean Society of Nuclear Medicine Clinical Trial Network (KSNM CTN) working group funded by the Korean Society of Nuclear Medicine (KSNM-CTN-2014-02-1). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 7, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 24, 2015.
- Accepted for publication November 20, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of Baseline 68Ga-FAPI and 18F-FDG PET/CT for Prediction of Response and Clinical Outcome in Patients with Unresectable Hepatocellular Carcinoma Treated with PD-1 Inhibitor and Lenvatinib
- 18F-FDG PET/CT Can Predict Survival of Advanced Hepatocellular Carcinoma Patients: A Multicenter Retrospective Cohort Study