


Abstract
Prostate-specific membrane antigen (PSMA) may be targeted for both diagnostic and therapeutic purposes in the management of prostate cancer (PCa). In preclinical models, androgen blockade (AB) increases expression of PSMA in both hormone-sensitive and castrate-resistant xenotypes. The aim of this study was to evaluate the effect of AB treatment on 68Ga-PSMA-11 PET imaging in hormone-naive (luteinizing hormone-releasing hormone [LHRH] ± bicalutamide) and in castrate-resistant men (enzalutamide or abiraterone) with metastatic PCa. Methods: Serial 68Ga-PSMA-11 PET was prospectively performed at baseline and on days 9, 18, and 28 in 8 men with measurable metastatic hormone-sensitive PCa commencing LHRH ± bicalutamide (cohort 1) and 7 men with castrate-resistant PCa commencing either enzalutamide or abiraterone (cohort 2). Gleason score, age, time since diagnosis, and prior treatments were documented. Testosterone and prostate-specific antigen (PSA) were measured at baseline and all imaging time points. PET/CT was quantitatively analyzed for SUVmax, SUVmean, and total tumor volume. Results: In cohort 1, a median 30% (interquartile range [IQR], 5–61) reduction in SUVmax was recorded by day 9 after AB. A reduction from baseline SUVmax occurred in 86.5% (6/7) men by day 9 (P < 0.04), with an associated PSA response in 100% men (P < 0.03). Total tumor volume reduced in all men by 74.5% (IQR, 27–97) (P < 0.02). After day 9, PSMA response heterogeneity was noted, with persistently high or increasing SUVmax in 37.5% (3/8) and marked reduction in 62.5% (5/8). In cohort 2, a median 45% (IQR, 12.7–66) increase in intensity of PSMA SUV was recorded by day 9 after AB. All men demonstrated an increase in SUVmax and SUVmean on PSMA PET compared with baseline (P < 0.04). This increase at day 9 plateaued by day 28. PSA responses were more delayed in cohort 2 (−15% [IQR, 70−138]), with 2 of 7 men demonstrating PSA progression. Conclusion: There is rapid dichotomous response on 68Ga-PSMA PET imaging to AB-dependent on the presence of a hormone-sensitive or castrate-resistant PCa phenotype. This has important implications for interpretation of PSMA PET, and in the timing and sequencing of PSMA-targeted therapy.
Prostate-specific membrane antigen (PSMA) is a transmembrane glycoprotein on the cell surface of prostate cancers (PCas) that can be effectively targeted for both PET diagnostic and therapeutic purposes in the management of PCa. The PSMA receptor has an oncogenic signaling role in the PCa cell, acting on glutamate receptors and activating the Pi3K and Akt growth pathways (1–3). Androgen blockade (AB) appears to increase expression of PSMA in cell line and mouse models in both hormone-sensitive and castrate-resistant states (4). However, there is a paucity of information on the effect of AB on PSMA PET intensity in vivo, the impact of this effect on the PET imaging results of men commencing androgen deprivation therapy, and the timing of these changes. The aim of this study was to prospectively evaluate the impact of commencing AB on 68Ga-PSMA-11 PET quantitative parameters in men with metastatic disease in the hormone-sensitive setting, or with enzalutamide or abiraterone in men with castrate-resistant PCa.
MATERIALS AND METHODS
Patient Selection
Between August 2017 and July 2018, 15 men with histologically confirmed, Gleason score (GS) 7–10 PCa with metastatic disease on conventional imaging were prospectively consented and enrolled in the study. Men were recruited to 1 of 2 cohorts: cohort 1 (n = 8) included those with newly diagnosed hormone-sensitive PCa commencing treatment (luteinizing hormone-releasing hormone [LHRH] ± bicalutamide). Cohort 2 (n = 7) included men with castrate-resistant PCa commencing AB with either enzalutamide or abiraterone. Castrate-resistant disease was defined as disease progression despite castrate levels of testosterone (<1.7 nmol/L). Demographic and clinical features including patient age, GS, time since diagnosis, and prior lines of treatment were documented. Prostate-specific antigen (PSA) and testosterone levels were measured at baseline and at all imaging time points. Written informed consent was obtained from all patients before enrolment, and this prospective trial was approved by the St. Vincent’s Hospital Human Research and Ethics Committee (HREC/17/SVH/25).
PSMA PET/CT
Serial 68Ga-PSMA PET scans were obtained at baseline and on days 9, 18, and 28 after commencing AB. 68Ga-HBEDD-CC PSMA-11 (68Ga-PSMA) was produced on-site compliant with good laboratory practice procedure using a TRASIS automated radiopharmacy cassette. Radiopharmacy quality control was undertaken using a high-pressure liquid chromatography method. Patients were injected with 2.0 MBq of 68GaPSMA per kilogram, with imaging parameters (dose, time after injection, and imaging protocols) repeated identically at each time point for each patient enrolled. All PET CT imaging was undertaken using a Phillips Ingenuity TOF-PET/64 slice CT scanner. A non–contrast-enhanced CT scan was acquired 60 min after tracer injection using the following CT parameters: 2 mm slice thickness soft-tissue reconstruction kernel, 120 keV and 50 mAs, pitch of 0.828, 600 mm field of view, and a 512 matrix. Immediately after CT scanning, a whole-body PET scan was acquired for 2 min per bed position. The emission data were corrected for randoms, scatter, and decay using the Phillips Body-dynamic.xml and Body.xml reconstruction protocol.
Image Quantitation
Visual and quantitative image analyses was undertaken using MIM Maestro software at each time point. The total number of PSMA-avid metastatic lesions, intensity, and total metabolic tumor volume were measured. SUVmax and mean SUVmean were recorded for each lesion, and on whole-body assessment to obtain a total-body SUVmax, SUVmean and total metabolic tumor volume (mLs). Salivary gland SUVmax on PSMA PET was documented at each time point for each patient.
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics and outcomes of interest. The Wilcoxon signed-rank test was used for comparison of nonparametric data. All tests were 2-sided, and a P value of 0.05 or less was considered statistically significant. Statistical analysis was performed with SPSS Statistics, version 24.0 (SPSS Inc.).
RESULTS
Baseline Characteristics
In total, 15 men with histologically confirmed PCa underwent serial 68Ga-PSMA PET scans after commencement of AB. Baseline clinical characteristics and previous treatments are summarized in Table 1.
Patient Characteristics
Cohort 1 (Hormone-Sensitive PCa)
LHRH alone was commenced in 1 of 8 and LHRH + bicalutamide (50 mg daily) in 7 of 8 men (Table 1). All men completed baseline scans before commencing AB. Eighty-seven percent (7/8) of men completed the days 9 and 18 scans and 100% the day 28 scan. All scans were undertaken within 5 d of the predetermined time points.
Molecular Imaging Response
There was a median 30% (interquartile range [IQR], 5–61) reduction in SUVmax by day 9 from baseline (P < 0.04) (Table 2). A reduction from baseline SUVmax occurred in 86.5% (6/7) of men by day 9 (Fig. 1). One patient had an increase in SUVmax at day 9, with subsequent reduction by days 18 and 28 (Fig. 2). After day 9, 68Ga-PSMA response heterogeneity was noted, with persistently high or increasing SUVmax in 37.5% (3/8) and marked reduction in 62.5% (5/8) (Figs. 2 and 3). Total body tumor volume reduced significantly over the 28 d of the study in all men (–74.5% [IQR, –27%–97%]) (P < 0.02).
Comparison of Clinical and Imaging Parameters between Baseline, Day 9, and Day 28 After Commencing AB in both Hormone-Sensitive (C1) and Castrate-Resistant (C2) Disease States
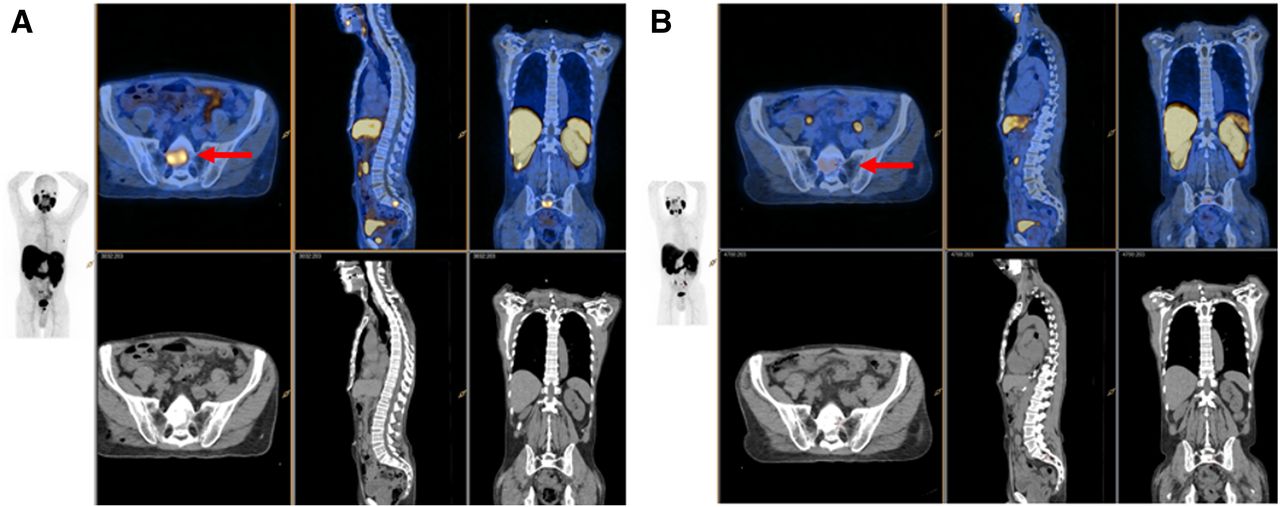
Metastatic bone disease demonstrated marked reduction in PSMA SUVmax from baseline ([A] SUVmax 8) to day 9 ([B] SUVmax 3) (red arrow), in response to LHRH + bicalutamide (patient C in Fig. 2).
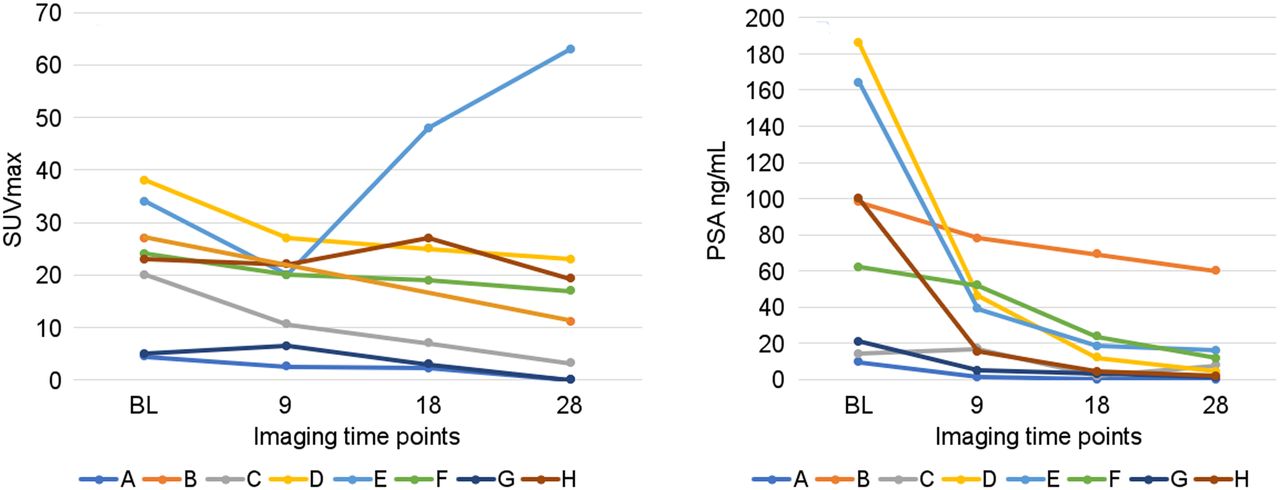
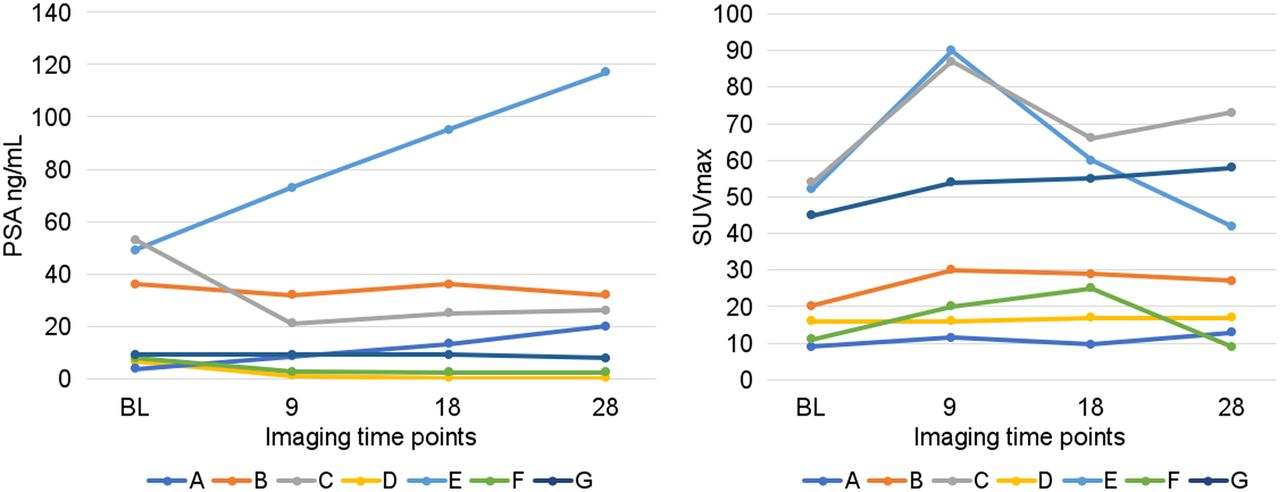
Serial-time-point PSMA PET imaging measuring SUVmax (A) and serial serum PSA (B) in men with hormone-sensitive PCa commencing LHRH ± bicalutamide.

A man with newly diagnosed extensive bone metastases on PSMA PET (patient E in Fig. 2). PSMA SUVmax of 35 at baseline (A) initially showed a reduction to an SUVmax of 20 at day 9 (B). This then increased to an SUVmax of 65 at day 28 (C), although the total volume of disease was significantly reduced by day 28. There was a marked PSA response to treatment (−90%), although PSA response was short lived on follow-up.
PSA Response
There was a marked reduction in PSA in response to commencing AB by day 28 (−91% [IQR, –97.7%–57%]) (Fig. 4). This biochemical response was also observed in those men with an increase or stable 68Ga-PSMA SUVmax in response to AB (90% PSA reduction in these 2 men). Testosterone dropped rapidly and was <1.0 nmol/mL by day 28 in all men.
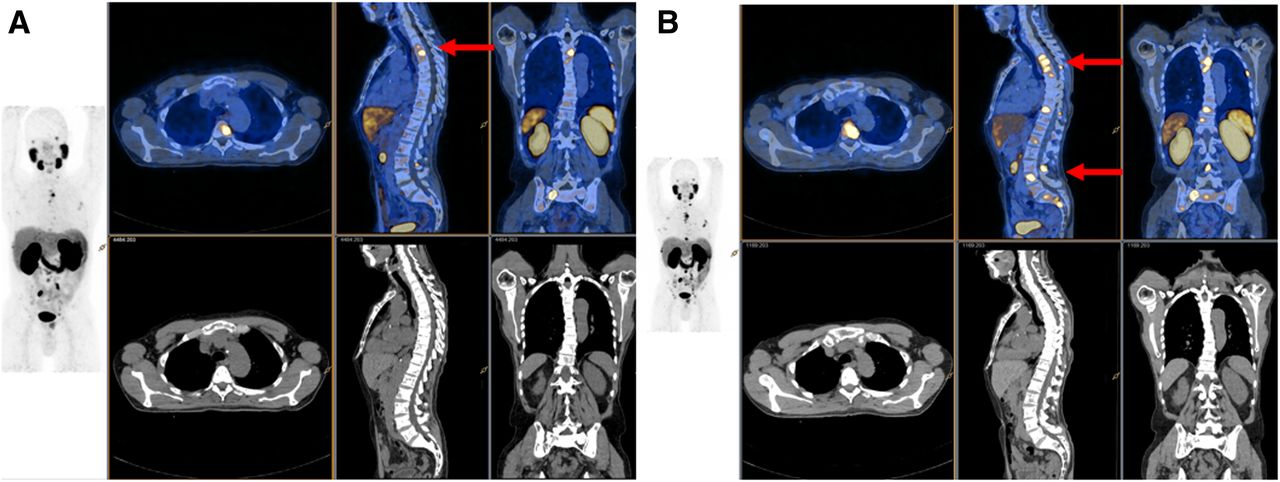
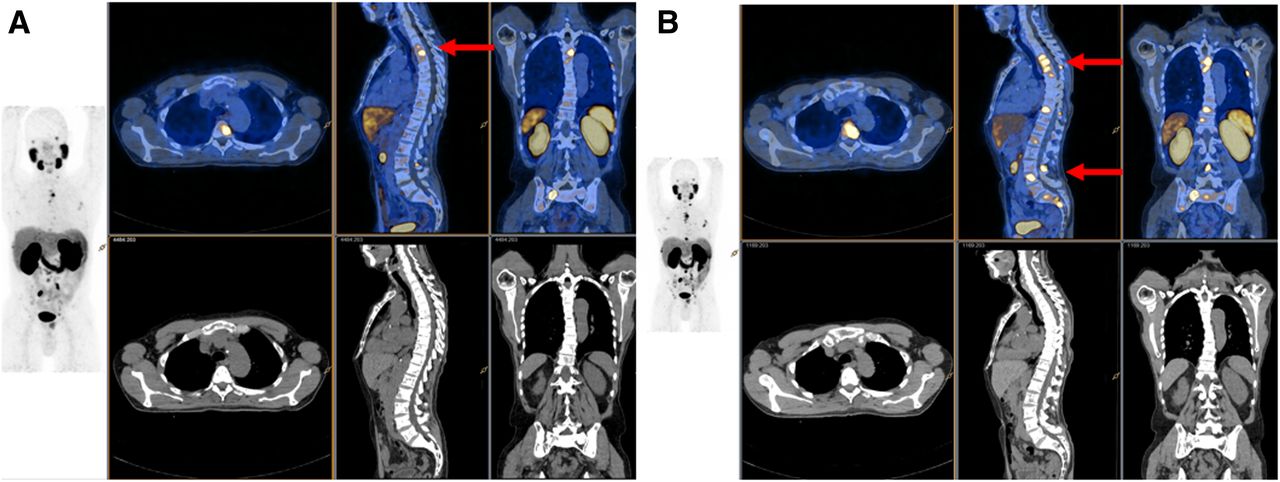
All men with mCRPC experienced an increase in PSMA SUVmax and SUVmean in response to androgen-signaling inhibition. This man (patient B in Fig. 5) had an increase in SUVmax from 20 at baseline (A) to 30 at day 9 (B) and an increase in the number of metastatic lesions visible on PSMA PET (red arrows).
Cohort 2 (Castrate-Resistant PCa)
All men in cohort 2 had failed previous treatment with LHRH and had not yet received a second-generation androgen-signaling inhibitor. Two (of 7) had received docetaxel. All men commenced treatment with either enzalutamide (6/7) or abiraterone (1/7) 1 d after baseline 68Ga-PSMA PET and continued treatment throughout the trial. All men in cohort 2 underwent baseline and days 18 and 28 imaging. Six (of 7) completed day 9 imaging.
Molecular Imaging Response
A median 45% (IQR, 12.7–66) increase in SUVmax was recorded by day 9 after AB (Table 2). All men demonstrated an increase in SUVmax and mean on 68Ga-PSMA PET at day 9 compared with baseline (P < 0.04). This increase in SUVmax plateaued by days 18 and 28 (Fig. 5).

Increase in PSMA SUVmax was noted in all men with mCRPC commencing androgen-signaling inhibition. PSA response in men with mCRPC commencing androgen-signaling inhibition after LHRH was slower, with 2 of 7 demonstrating progression of PSA on treatment.
PSA Response
Median baseline PSA in this cohort was 9.2 (IQR, 4.9–490). PSA response to treatment was more delayed in cohort 2 (Fig. 5) compared with cohort 1. There was no change in PSA by day 9, but a median drop in PSA of 15% (IQR,−70%–+138%) by day 28. Two men in cohort 2 demonstrated PSA progression while on study.
Salivary gland activity was measured in all men at all time points and was not significantly different from baseline in either cohort.
DISCUSSION
PSMA is a transmembrane glycoprotein that is overexpressed on nearly all PCa cells and that has become an attractive target for both the imaging and the therapy of PCa at many stages of this disease (5–10). Cell line and small-animal work has demonstrated that the PSMA receptor is manipulable with receptor density influenced by androgen receptor blockade (4,11–14). The fact that external factors such as AB are capable of influencing PSMA receptor density has a considerable impact on 68Ga-PSMA PET’s value as a diagnostic agent, its ability to monitor treatment response, and its use as a therapeutic target. This study confirms that 68Ga-PSMA PET is significantly influenced by the presence of AB, that this manipulation of the68Ga-PSMA intensity occurs early after commencing treatment, and that the effect of AB on PSMA PET is highly dependent on the castration sensitivity of the PCa cells at the time of imaging.
PSMA expression on the PCa cell surface has repeatedly been reported to increase with androgen receptor inhibition in vitro (10–12). Evans et al. demonstrated that PSMA expression is increased with both orchidectomy and enzalutamide in mice bearing PSMA-expressing xenografts (11). Hope et al. confirmed that PSMA intensity increased significantly with AB in LNCaP-AR xenograft mouse models, and demonstrated an increase in PSMA in a man with PCa despite a concomitant reduction in PSA in response to 4 wk of AB (12). An increase in PSMA messenger RNA was measured with antiandrogen treatment in castrate-sensitive, castrate-resistant, and abiraterone-tolerant castrate-resistant cell lines (4). These previous findings are quite different from what we found in vivo using serial 68Ga-PSMA PET in hormone-naive men. This study demonstrated that a significant reduction in 68Ga-PSMA intensity occurred in 86% of men as early as day 9 after commencing initial treatment with AB. This finding was unexpected, given the in vitro findings and is probably multifactorial. A reduction in PSMA intensity in men commencing first-line AB is likely explained by the strong antiproliferative effect of AB on most PCa phenotypes in the early (hormone-naive) stages of disease. The marked reduction in 68Ga-PSMA intensity echoed the marked reduction in PSA levels in these men. Although there may have been a cellular increase in PSMA receptor activity in some cells, the marked involutory response of hormone-naive PCa cells to AB has overshadowed this, with a resultant overall rapid reduction in 68Ga-PSMA PET intensity. Furthermore, it may be that the mouse xenotypes and cell lines used previously have represented a more aggressive, less treatment-responsive PCa phenotype than those of the men enrolled in this study.
This rapid reduction in 68Ga-PSMA PET intensity identified in men with hormone-sensitive disease commencing AB has important clinical considerations. PSMA PET imaging may significantly underestimate the volume of metastatic disease in hormone-naive men who have commenced on AB even within 9 d. Accurate staging with PSMA PET must therefore occur before commencing AB to ensure adequate imaging sensitivity.
In contrast, all men with metastatic castration-resistant prostate cancer (mCRPC) commencing androgen-signaling inhibition demonstrated an increase in intensity of 68Ga-PSMA PET by day 9 compared with baseline. This finding is consistent with the preclinical results seen in mouse and cell line work, likely due to the slower treatment response of PCa to second- (or third-) line treatment. This increase in 68Ga-PSMA quantitative intensity scores in response to androgen-signaling inhibitors has several clinical implications. The knowledge that PSMA receptors can upregulate in men with mCRPC must be factored into any interpretation of serial 68Ga-PSMA PET imaging for treatment response in men who have commenced androgen-signaling inhibitors.
Another clinically relevant implication of the findings from this study is the potential synergistic interaction with androgen-signaling inhibitors and PSMA-targeted treatments. A recent publication on LnCAP cell lines demonstrated increased uptake and internalization of 177Lu-PSMA in PCa cells pretreated with enzalutamide (13). There is also an association between 68Ga-PSMA PET quantitative intensity scores and treatment response to177Lu-PSMA (15). The increase in 68Ga-PSMA intensity with AB reported in men with mCRPC in this study suggests that combination treatment (177Lu-PSMA + androgen-signaling inhibitors) may be more effective than 177Lu-PSMA alone in mCRPC. Prospective trials are needed to confirm this.
Although there was a relatively homogeneous response on 68Ga-PSMA PET at day 9, subsequent imaging time points demonstrated more heterogeneous results. Several men with hormone-naive PCa demonstrated an increase in 68Ga-PSMA SUVmax by day 28 at some tumor sites, although overall 68Ga-PSMA total tumor volume had continued to reduce in line with their PSA. It is possible that 68Ga-PSMA PET may be able to identify early castrate-resistant clones well before a consequent rise in PSA. Further prospective evaluation of 68Ga-PSMA PET as a prognostic indicator in metastatic PCa may better help delineate the significance of these early findings.
This study had limitations. The number of men enrolled in the 2 prospective cohorts were small, and as such this study was designed to be hypothesis-generating rather than definitive. Despite the small numbers, the study was able to demonstrate that there is significant change in PSMA intensity scores that occurs early (within 9 d) after commencing either AB. Larger prospective trials are needed to more fully evaluate heterogeneity of response to androgen-signaling inhibition across a variety of PCa phenotypes.
The study evaluated 68Ga-PSMA intensity on serial scans using SUVmax and SUVmean in addition to total metabolic tumor volume using an automated software program (MIM). SUV can have significant variations between institutions and at different time points. Attention was paid to ensuring identical regions of interest were assessed for quantitation. Care was also taken within the trial protocol to ensure injected dose, camera, and scan timing were identical to baseline for each time point image. Furthermore, evaluation of salivary gland activity was uniform between scans and did not demonstrate variation with AB, acting as a useful control.
CONCLUSION
There is rapid dichotomous response on 68Ga-PSMA PET imaging to AB dependent on the presence of a hormone-sensitive or castrate-resistant PCa phenotype. This has important implications for interpretation of PSMA PET imaging and in the timing and sequencing of PSMA-targeted therapy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 14, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 6, 2018.
- Accepted for publication November 28, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploring the Flare Phenomenon in Patients with Castration-Resistant Prostate Cancer: Enzalutamide-Induced PSMA Upregulation Observed on PSMA PET
- Clinical, Pathologic, and Imaging Variables Associated with Prostate Cancer Detection by PSMA PET/CT and Multiparametric MRI
- Prostate-Specific Membrane Antigen-Targeted Imaging and Its Correlation with HOXB13 Expression
- PSMA PET/CT for Response Assessment and Overall Survival Prediction in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Androgen Receptor Pathway Inhibitors
- Antihormonal-Treatment Status Affects 68Ga-PSMA-HBED-CC PET Biodistribution in Patients with Prostate Cancer
- Using 68Ga-PSMA-11 PET/CT for Therapy Response Assessment in Patients with Metastatic Castration-Resistant Prostate Cancer: Application of EAU/EANM Recommendations in Clinical Practice
- Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging
- Radionuclide Therapy in Prostate Cancer: From Standalone to Combination PSMA Theranostics
- Prospective, Single-Arm Trial Evaluating Changes in Uptake Patterns on Prostate-Specific Membrane Antigen-Targeted 18F-DCFPyL PET/CT in Patients with Castration-Resistant Prostate Cancer Starting Abiraterone or Enzalutamide
- Darolutamide Potentiates the Antitumor Efficacy of a PSMA-targeted Thorium-227 Conjugate by a Dual Mode of Action in Prostate Cancer Models
- Nuclear Medicine Beyond VISION
- Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer
- Proposal for Systemic-Therapy Response-Assessment Criteria at the Time of PSMA PET/CT Imaging: The PSMA PET Progression Criteria
- Detection Rate and Localization of Prostate Cancer Recurrence Using 68Ga-PSMA-11 PET/MRI in Patients with Low PSA Values <= 0.5 ng/mL