


Abstract
Triple-negative breast cancer, an aggressive subtype, represents 15% of invasive breast tumors. This prospective study investigated whether early changes in 18F-FDG tumor uptake during neoadjuvant chemotherapy (NAC) can predict outcomes. Methods: Twenty (M0) patients underwent 18F-FDG PET/CT at baseline and after the second cycle. NAC was continued irrespective of PET results. Results: At surgery, 6 patients had a pathologic complete response, whereas 14 had residual tumor. Four patients showed early relapse (in the 2 y after surgery). There were 11 metabolic responders and 9 nonresponders using a 42% decrease in maximum standardized uptake value as a cutoff. In nonresponding patients, the risk of residual tumor at surgery was 100% (vs. 45% in responders; P = 0.014), and the risk of early relapse was 44% (vs. 0%; P = 0.024). Conclusion: A less than 42% decrease in 18F-FDG uptake at 2 cycles means residual tumor at the end of NAC and a high risk of early relapse.
Triple-negative breast cancer (TNBC) accounts for 15% of invasive breast cancers and is characterized by the lack of estrogen and progesterone receptors and the absence of HER2 overexpression (1). Patients with TNBC have a relatively poor outcome, with higher relapse rates than for other breast tumor types (1). However, these aggressive tumors have more intrinsic responsiveness to neoadjuvant chemotherapy (NAC) than estrogen receptor–positive tumors (2). Also, TNBC patients with a pathologic complete response (pCR) after NAC have a good prognosis (3). In the M.D. Anderson series, TNBC patients who achieved a pCR (22%) had a 3-y overall survival of 94%, not significantly different from other tumor types (98%; P = 0.24), whereas those with residual tumor at surgery had a 3-y survival of only 68% (vs. 88% for other tumor types; P = 0.0001) (3). Therefore, obtaining a pCR is an important objective when TNBC patients are offered preoperative chemotherapy.
Metabolic evaluation with 18F-FDG PET early in the course of treatment of some aggressive lymphomas, such as diffuse large B-cell lymphoma and Hodgkin disease, proved to be a powerful predictor of outcome (4). Many trials now use early 18F-FDG assessment to switch lymphoma patients with an unfavorable response toward intensification of chemotherapy or alternative treatments (5). In breast cancer, several studies have evidenced a correlation between early changes in 18F-FDG uptake after 1 or 2 courses of chemotherapy and the extent of pathologic response at completion of NAC (Rousseau et al. (6), Berriolo-Riedinger et al. (7), and Schwarz-Dose et al. (8), among others). However, the ability to implement PET as a surrogate marker for treatment efficacy in clinical practice remains unclear because of substantial heterogeneities across studies and also because breast cancer cannot be examined as a single entity (9). Breast cancer comprises different groups of tumors with different response rates to chemotherapy, different risks of relapse, different treatment options, and different prognoses. We have therefore suggested that the clinical aims of early 18F-FDG monitoring and the criteria used to assess efficacy should be examined in specific subgroups (9).
This study investigated the value of interim PET in TNBC.
MATERIALS AND METHODS
Patients
During 30 mo, 20 consecutive patients with stage II or III breast carcinoma and a triple-negative phenotype underwent an 18F-FDG PET/CT study before starting NAC and then after the second cycle. Four patients with distant metastases identified at initial staging were not included. After completion of NAC, all patients underwent breast-conserving surgery or mastectomy and dissection of axillary lymph nodes. The study was performed according to the guidelines of the institutional ethical committee.
NAC
Fourteen patients received 4 cycles of epirubicin (75 mg/m2) plus cyclophosphamide (750 mg/m2) administered every 3 wk, followed by 4 courses of docetaxel (100 mg/m2). The last 6 included patients receiving epirubicin (75 mg/m2) plus cyclophosphamide (1,200 mg/m2) every 2 wk for 6 cycles (10).
18F-FDG PET/CT
Patients fasted for 6 h. Blood glucose level had to be less than 7 mmol/L. 18F-FDG (5 MBq/kg) was administered into the arm opposite to the breast tumor using a venous line to prevent extravasations. Imaging started 60 min after injection and was performed from mid-thigh level to the base of the skull with the arms raised. The Gemini XL PET/CT instrument combines a germanium oxyorthosilicate–based PET scanner and a 16-slice Brilliance CT scanner (Philips). CT data were acquired first (120 kV, 100 mAs, no contrast enhancement). PET emission data were acquired in a 3-dimensional mode, with 2 min per bed position, and reconstructed using a 3-dimensional row-action maximum-likelihood algorithm. The attenuation-corrected images were normalized for injected dose and body weight and converted into standardized uptake values (SUVs). The SUV was defined as (tracer concentration [kBq/mL])/(injected activity [kBq]/patient body weight [g]).
PET/CT images were interpreted by 2 nuclear medicine specialists masked to the patient's record. Images were displayed on the Extended Brilliance workstation (Philips). The SUV was measured by manually marking a circular region of interest in the 3 planes (coronal, sagittal, and axial) around the tumor (3-dimensional region of interest). The maximum SUV (SUVmax within the region of interest) was used for the study analysis.
The change in SUV after 2 cycles of chemotherapy was expressed as ΔSUVmax (%) = 100 × (second-cycle SUVmax − baseline SUVmax)/baseline SUVmax.
Tumor Histology and Immunohistochemistry Analysis
Breast cancer was diagnosed using core-needle biopsy. Histologic grade was determined using the modified Scarff–Bloom–Richardson grading for invasive carcinoma.
Tumors were defined as triple-negative on the basis of immunohistochemical test results performed on formalin-fixed, paraffin-embedded tissues, using specific antibodies and an automated immunostainer (XT Immunostainer; Ventana). Tumors were considered to overexpress HER2 if more than 30% of invasive tumor cells showed definite membrane staining resulting in a so-called fishnet appearance; control by FISH (fluorescence in situ hybridization) or SISH (silver enhanced in situ hybridization) was done for ambiguous cases. Tumors were considered estrogen receptor– and progesterone receptor–negative if there was less than 10% staining.
Pathology Assessment at Completion of NAC
pCR was defined as no evidence of residual invasive cancer, both in breast tissues and in lymph nodes (11,12). The absence of carcinoma in situ was not mandatory to define pCR (11).
Disease-Free Survival (DFS)
DFS was calculated from the time of surgery. Events included local, regional, or distant recurrences or death, whichever occurred first.
Statistical Analysis
Analyses were performed using R 2.12.0 statistical software (The R Foundation for Statistical Computing).
RESULTS
Patients and tumor characteristics of the 20 TNBC patients included in this study are summarized in Table 1.
Overall Characteristics of TNBC Patients
Pathologic Response
At completion of NAC, breast-conserving surgery was performed in 6 patients and mastectomy in 14 patients. All patients had axillary lymph node dissection. Histopathology revealed pCR in 6 patients (30%), whereas 14 patients (70%) had residual disease (non-pCR).
Change in SUV and Pathologic Response
Table 2 shows individual data for each patient including baseline PET and interim PET SUV results, ΔSUV, results of surgery, and disease outcome.
Individual Outcomes for 20 Patients with TNBC
At baseline, SUVmax values ranged between 1.5 and 27.0 (mean, 11.2). After 2 courses of chemotherapy, SUVmax ranged between 1.1 and 30.6 (mean, 5.8).
The mean ΔSUVmax (ΔSUV) between initial and interim PET was −45% (range, −91% to +13%). The mean ΔSUV was −73% in patients who achieved a pCR versus −33% in patients who did not (P = 0.0008 with t test). Figure 1 shows initial and interim 18F-FDG PET/CT results in a patient who had a pCR. The ability of ΔSUV to predict pathology findings (non-pCR vs. pCR) was derived by computing the area under the receiver-operating-characteristic curve, yielding an area under the curve of 0.881 (Fig. 2).

A 53-y-old patient with TNBC (patient 1; Table 2). Triple-negative tumor was 80-mm grade 3 invasive ductal carcinoma of right breast, invading areola (T4N1M0; stage IIIB). (A and B) Transaxial CT and fused PET/CT images of primary tumor at baseline. (C and D) Corresponding images after 2 courses of NAC. At baseline, SUVmax of 23.3 is measured at breast tumor level. After 2 courses of chemotherapy, there is residual uptake, with SUVmax of 3.7 (ΔSUV, −84%). At completion of chemotherapy (after 2 additional courses of epirubicin [75 mg/m2] plus cyclophosphamide [750 mg/m2] and 4 courses of docetaxel [100 mg/m2]), breast mastectomy shows pCR, with absence of residual tumor cells in breast and no cancer cells in 9 lymph nodes removed at axillary dissection.
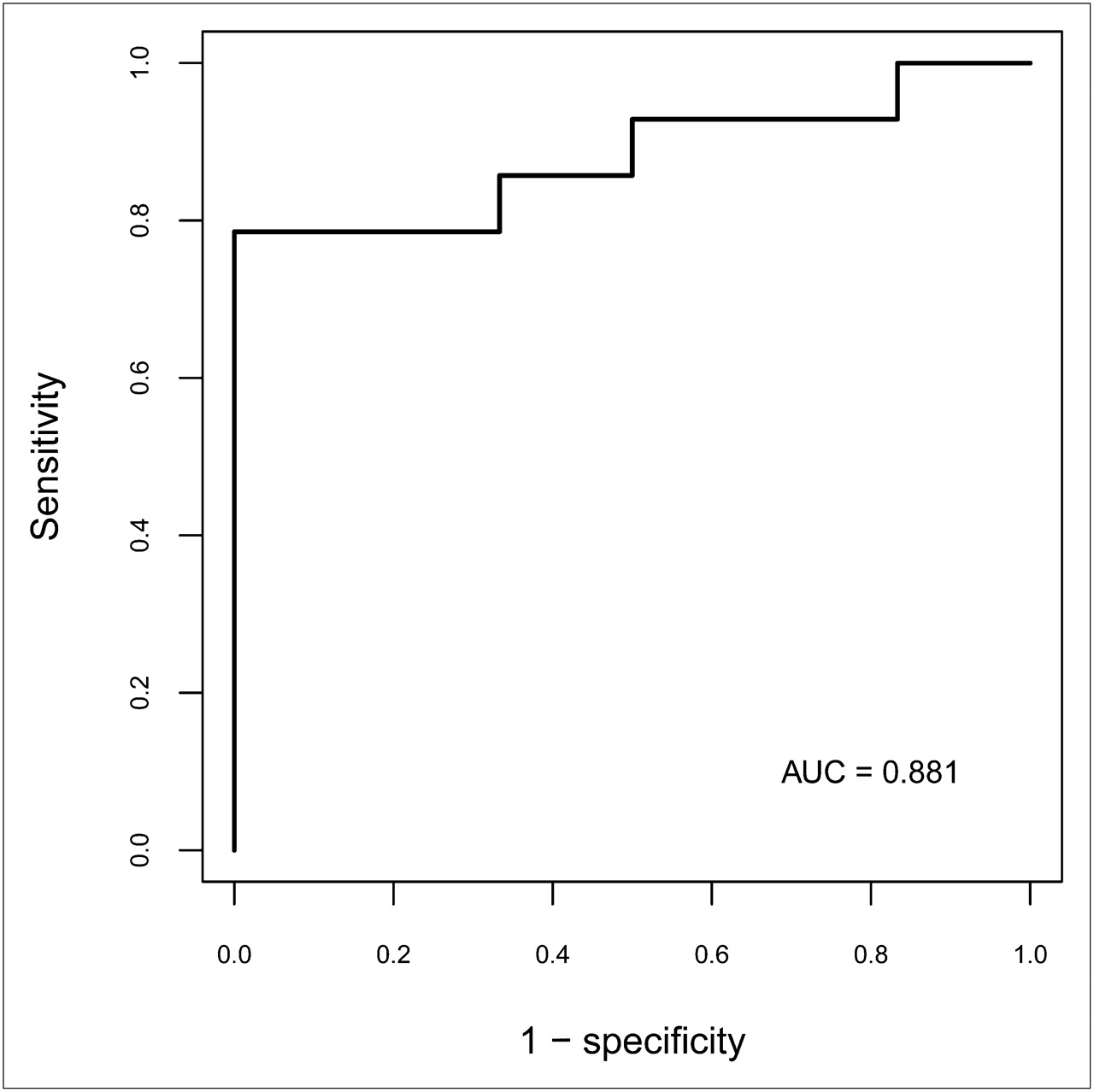
Capacity of ΔSUV at 2 cycles to predict residual tumor (non-pCR) at surgery after completion of NAC, derived by the area under the receiver-operating-characteristic curve (AUC).
No correlation was found between histopathologic response and SUVmax at baseline (P = 0.22; Wilcoxon rank sum test) or after the second cycle of chemotherapy (P = 0.30); only the change in SUV was predictive.
Change in SUV and DFS
The mean follow-up after surgery was 20 mo (range, 7–37 mo). The 2-y DFS was 77%. Four patients experienced early relapse; 2 of them died (Table 2).
No correlation was found between relapse events and SUVmax at baseline (P = 0.54; Wilcoxon rank sum test) or after the second cycle of chemotherapy (P = 0.42).
Screening for different cutoffs identified a cutoff of a 42% decrease in SUVmax as the best predictor of DFS. Figure 3 shows the Kaplan–Meier DFS curves for metabolic responders (≥42% decrease) and nonresponders (<42% decrease). None of the 11 metabolic responders relapsed, including 5 patients who did not achieve a pCR.

Kaplan–Meier DFS curves for metabolic responders (≥42% decrease) and metabolic nonresponders (<42% decrease).
Choice of Cutoff
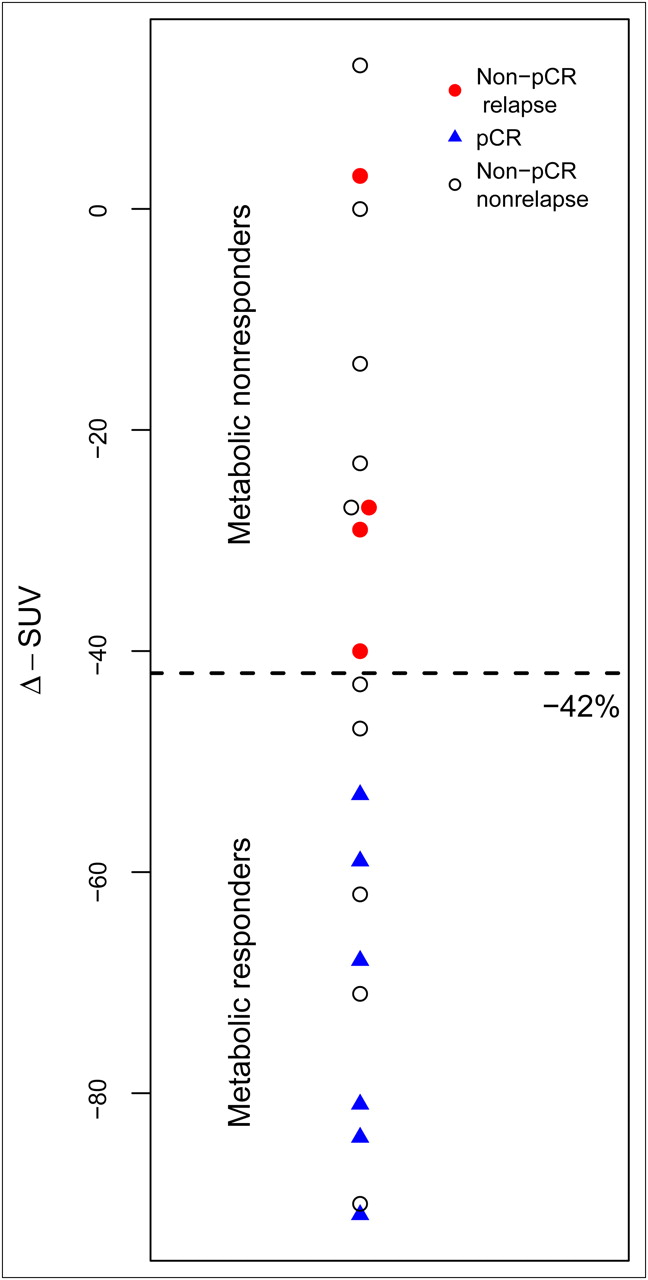
Figure 4 shows the distributions of pCR, non-pCR, and relapses, according to the decrease in SUVmax at 2 cycles. The cutoff of 42% is drawn on the graph. With this division, there were 11 metabolic responders and 9 nonresponders. Residual tumor (non-pCR) was found in 100% of nonreponders versus 45% of responders (P = 0.014; Fisher exact test). The sensitivity for identification of non-pCR was 64% (9/14), and specificity was 100% (6/6). The relapse rate was 44% for nonresponders and 0% for responders (P = 0.024; log rank).

Pathology results and relapses according to decrease in SUVmax after 2 cycles of chemotherapy. Graph shows distribution of pCR (blue triangles) and non-pCR (circles). Red-filled circles correspond to relapses. Open circles correspond to non-pCR patients who did not relapse.
When using a cutoff of a 50% decrease in SUVmax, sensitivity for non-pCR increased (79%). However, the positive predictive value for relapse decreased (36%).
DISCUSSION
In this prospective study, an interim 18F-FDG PET examination after 2 cycles of NAC was predictive of pathologic response (Fig. 2) and DFS (Fig. 3) in patients with TNBC, an aggressive subtype of breast cancer.
At completion of NAC, residual tumor was found in 70% and pCR in 30% of patients, which is similar to other reports (1–3,13). The mean ΔSUV at 2 cycles was −33% in patients with residual tumor versus −73% in those who achieved a pCR (P = 0.0008).
Four patients (20%) presented early relapse. All 4 patients had little modification of SUV (mean ΔSUVmax, −23%). Threshold screening identified a cutoff of a 42% decrease in SUVmax as the best predictor of outcomes. With this cutoff, 9 of 20 patients were nonresponders. In them, the risk of a non-pCR was 100% (vs. 45% in responders; P = 0.014), and the risk of early relapse was 44% (vs. 0%; log rank P = 0.024).
A less stringent cutoff to define nonresponders (<50% decrease in SUVmax) offered higher sensitivity in identifying non-pCR cases. However, the predictive value for relapse decreased. When interim 18F-FDG PET is used as a surrogate for poor response to NAC, a stringent cutoff is needed to avoid a change in treatment when it might benefit. This 42% cutoff needs to be validated using an independent dataset.
Poor metabolic response at 2 cycles (<42% decrease in SUV) was more predictive of relapse (4/9) than was a non-pCR at completion of NAC (4/14). Importantly, early assessment might offer an opportunity to change strategy in the case of inefficacy.
Novel treatment strategies are being investigated. We reported a 10-y DFS rate of 76% in TNBC patients using cyclophosphamide dose intensification (10). Several ongoing studies involve new cytotoxic agents or targeted therapies (14). Inherent defects in DNA repair make TNBC a rational target for therapy based on polymerase (adenosine diphosphate-ribose) polymerase (PARP) (1); PARP inhibitors, with or without combination with platinum salts, are now at the forefront of clinical research in TNBC patients (15).
Triple-negative tumors are recognized to be 18F-FDG–avid (16–18). High SUV at baseline facilitates metabolic assessment with PET. Baseline values were low in 2 of our patients (patients 8 and 15), rendering metabolic evaluation more difficult (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org). We did not exclude these patients to avoid potential bias. Nevertheless, exclusion of these 2 patients would not change the findings of this study. The mean ΔSUV at 2 cycles was −34% in patients with residual tumor versus −73% in those who achieved a pCR (P = 0.003). The risk of early relapse was 43% (3/7) in nonresponders vs 0% in the 11 responders (P = 0.025) (Supplemental Fig. 2) using a cutoff of a 42% decrease in SUVmax.
Regarding alternative techniques with potential for early evaluation of response, there are some encouraging data with MRI (19,20).
Our single-institution study included 20 women with triple-negative tumor referred for NAC (usually when >3 cm). Although the number of patients is small, and follow-up relatively short (mean, 20 mo), the findings clearly point to the excellent predictive power of ΔSUV to early identify poor responders to the planned chemotherapy. A multiinstitutional study should be performed to validate these findings before interim PET is used as a surrogate marker in clinical trials involving novel therapeutic strategies.
CONCLUSION
In patients with TNBC, the change in 18F-FDG tumor uptake after 2 cycles of NAC offers powerful stratification of patient outcomes. It early identifies poor metabolic responders who would end up with residual tumor at the end of the planned NAC regimen and who have a high risk of early relapse.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
While preparing this manuscript, we lost our friend and colleague, Prof. Jean-Luc Moretti, head of the Nuclear Medicine Department. Part of this study was presented at the 2011 Society of Nuclear Medicine annual meeting, Henry B. Gonzalez Convention Centre, San Antonio, TX, June 4–8. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication June 13, 2011.
- Accepted for publication September 29, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Now Is the Time to Use 18F-FDG PET/CT to Optimize Neoadjuvant Treatment in Triple-Negative Breast Cancer!
- Complete Metabolic Response on Interim 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography to Predict Long-Term Survival in Patients with Breast Cancer Undergoing Neoadjuvant Chemotherapy
- 18F-FDG PET/CT for the Early Evaluation of Response to Neoadjuvant Treatment in Triple-Negative Breast Cancer: Influence of the Chemotherapy Regimen
- Nuclear Breast Imaging: Clinical Results and Future Directions
- Quo Vadis: PET and Single-Photon Molecular Breast Imaging
- Identification of Biomarkers Including 18FDG-PET/CT for Early Prediction of Response to Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer
- Baseline Tumor 18F-FDG Uptake and Modifications After 2 Cycles of Neoadjuvant Chemotherapy Are Prognostic of Outcome in ER+/HER2- Breast Cancer
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- TBCRC 008: Early Change in 18F-FDG Uptake on PET Predicts Response to Preoperative Systemic Therapy in Human Epidermal Growth Factor Receptor 2-Negative Primary Operable Breast Cancer
- 18F-FDG PET/CT for Early Prediction of Response to Neoadjuvant Lapatinib, Trastuzumab, and Their Combination in HER2-Positive Breast Cancer: Results from Neo-ALTTO
- Comparison Between 18F-FDG PET Image-Derived Indices for Early Prediction of Response to Neoadjuvant Chemotherapy in Breast Cancer