


Abstract
This study investigated whether 18F-FDG PET/CT performed at baseline and during neoadjuvant chemotherapy (NAC) was able to early depict estrogen receptor–positive/human epidermal growth factor receptor 2–negative (ER+/HER2−) breast cancer patients with poor clinical outcome. Methods: The NAC regimen consisted of 4 cycles of epirubicin plus cyclophosphamide, followed by 4 courses of docetaxel. The patients underwent 18F-FDG PET/CT at baseline and after 2 cycles of chemotherapy. After completion of NAC, all patients had breast surgery with axillary lymph node dissection. We assessed the impact of 2 PET parameters, maximum standardized uptake values (SUVmax) and total lesion glycolysis, on event-free survival (EFS). Results: Ninety-eight consecutive patients with clinical stage II or III ER+/HER2− breast cancer were included. 18F-FDG PET/CT revealed distant metastases in 14 patients (14%). Overall survival was significantly shorter in these patients than in the 84 patients classified as M0 at baseline 18F-FDG PET/CT (P < 0.001). In M0 patients, a high SUVmax at baseline was associated with shorter EFS (P < 0.001). Twelve patients had a tumor SUVmax of 10 or greater and a 3-y EFS of 49% (vs. 92% in patients with baseline SUVmax < 10). A low change in SUVmax between 18F-FDG PET/CT examination before starting NAC and after the second cycle of chemotherapy was also associated with recurrence (P = 0.033), as was a low change in total lesion glycolysis (P < 0.001). Contrarily to PET-based prediction, the extent of pathologic response after completion of NAC (partial/complete vs. nonresponders) was poorly correlated to the risk of relapse. Conclusion: Baseline tumor 18F-FDG uptake and modifications after 2 cycles of NAC are prognostic of outcome in patients with ER+/HER2− breast cancer.
Neoadjuvant chemotherapy (NAC) is commonly offered to patients with stage II/III breast cancer (BC). This strategy allows more patients to undergo breast-conserving surgery and provides information on the efficacy of chemotherapy. Pathologic complete response (pCR) after NAC (absence of residual invasive cells in the primary tumor and axillary lymph nodes) is correlated with better survival (1). However, the relation between pathologic response and outcome is strong in aggressive subtypes such as the triple-negative (TN) phenotype but less so in the estrogen receptor–positive/human epidermal growth factor receptor 2–negative (ER+/HER2–) BC subgroup (1). Indeed, pCR is rare in this subtype (1). Therefore, there is a need for better predictors of patients’ outcomes in ER+/HER2– BC.
Early change in 18F-FDG uptake, as measured on PET/CT, can help predict response to NAC and prognosis. For example, in the TN phenotype we found a strong correlation between the decrease in the standardized uptake values (SUVs) after 2 courses of NAC, expressed as ΔSUV, and event-free survival (EFS) (2). However, the predictive value of ΔSUV could be lower in the ER+/HER2– subtype (3) because this subtype is somewhat less 18F-FDG–avid at baseline than TN tumors and less responsive to chemotherapy. We hypothesized that PET parameters taking into account metabolic volume measurements in addition to 18F-FDG uptake could be helpful in this specific subtype. Indeed, in a pilot study from our institution we reported that total lesion glycolysis (TLG) may help to early predict tumor regression and pathologic findings after NAC (4). In the present study, which includes a large number of patients and follow-up data, we assessed the impact of 18F-FDG parameters on EFS.
MATERIALS AND METHODS
Study Design
We performed ancillary analysis of prospectively acquired data in the frame of the ASAINT study. ASAINT aimed at evaluating the role of 18F-FDG PET/CT in patients with stage II or III BC undergoing NAC. The purpose of the present ancillary analysis was to evaluate the impact of PET-derived parameters in the subgroup of patients with ER+/HER2– breast carcinoma. The study was approved by the institutional review board, with waivers of informed written consent for this ad-hoc analysis of image-derived data.
From July 2007 to April 2013, 98 consecutive patients with initially diagnosed clinical stage II or III ER+/HER2– breast carcinoma prospectively underwent 18F-FDG PET/CT examination before starting NAC (PET1) and after the second cycle of chemotherapy (PET2). The total number of chemotherapy cycles was 8. After surgery, patients received external-beam radiation therapy (tailored to disease stage and the type of breast surgery) and hormone therapy; patients were followed at the breast disease unit of Saint-Louis Hospital, in Paris.
The main objective of the present study was to examine the association between PET image–derived parameters at baseline and after 2 cycles of NAC and EFS in ER+/HER2– BC patients without distant metastasis on 18F-FDG PET. Additional objectives were to examine the association between baseline 18F-FDG uptake and tumor characteristics; to assess the value of baseline PET/CT in terms of detection of occult distant metastases and its impact on survival; and to examine associations between EFS and clinical, biologic, and pathologic factors.
Tumor Histology and Immunohistochemistry
The BC diagnosis was made using a core-needle biopsy before NAC. Tumor grade used the modified Scarff–Bloom–Richardson (SBR) system. Tumors were ER-positive if showing moderate or high positivity (2+ or 3+) of at least 10% of cells. The same criteria were used for progesterone receptors (PRs). Tumors were HER2-positive if more than 30% of cells showed definite membrane staining. Control by fluorescence in situ hybridization or silver in situ hybridization was done for ambiguous cases. Only patients with ER+/HER2– tumors were included in the present analysis.
Treatment
Patients with no distant metastases on baseline PET/CT received NAC with EC-D (4 cycles of epirubicin [75 mg/m2] plus cyclophosphamide [750 mg/m2] administered every 3 wk, followed by 4 courses of docetaxel [100 mg/m2]). No neoadjuvant hormone therapy was used. After completion of NAC, all the patients underwent breast surgery (breast-conserving surgery or mastectomy according to clinical response to NAC) with axillary lymph node dissection. After surgery, these patients received locoregional radiation therapy and adjuvant hormone therapy for 5 y (tamoxifen in premenopausal women or aromatase inhibitors in postmenopausal women).
Patients with distant metastases at baseline staging had hormone therapy and chemotherapy tailored to their disease and physical condition and sometimes local treatments such as radiation therapy of bone metastases.
18F-FDG PET/CT Imaging and PET-Derived Metabolic Parameters
Patients fasted for 6 h, and blood glucose level had to be less than 7 mmol/L. 18F-FDG (5 MBq/kg) was administered intravenously in the arm opposite to the breast tumor and using a venous line to prevent extravasations. Imaging started 60 min after injection and was performed from mid-thigh level to the base of the skull with the arms raised. The Gemini XL PET/CT scanner combines a germanium oxyorthosilicate–based PET device and a 16-slice Brilliance CT device (Philips). CT data were acquired first (120 kV; 100 mAs; no contrast-enhancement). PET emission data were acquired in a 3-dimensional (3D) mode, with 2 min per bed position, and reconstructed using a 3D row-action maximum-likelihood algorithm with a 4 × 4 × 4 mm voxel grid. The attenuation-corrected images were normalized for injected dose and body weight and subsequently converted into SUVs, defined as (tracer concentration [kBq/mL])/(injected activity [kBq]/patient body weight [g]).
All PET-derived parameters were extracted from PET1 and PET2 images. For each patient, the tumor was identified by a nuclear medicine specialist, and the SUVmax (value of the voxel with the highest SUV) was measured.
The metabolically active tumor volume was automatically delineated in a 3D region of interest containing the tumor, using the fuzzy locally adaptive Bayesian (FLAB) algorithm (3,5). This method computes a probability for each voxel within the 3D region of interest to belong to a given class (e.g., tumor or background) by taking into account its value, the statistical distributions within the region of interest, and values of its 26 neighbors in 3D. TLG was defined as metabolically active tumor volume × mean SUV.
The percentage change of each parameter between baseline and after the second NAC cycle (Δparam, %) was calculated as Δparam = 100 × (param_PET2 – param_PET1)/param_PET1.
Pathology Assessment
pCR was defined as no evidence of residual invasive cancer in breast tissues and lymph nodes (ypT0/is ypN0). Absence of carcinoma in situ was not mandatory to define pCR (1).
Because pCR is rare in estrogen-positive tumors, we also examined the impact on patients’ outcome of (complete or partial) pathologic response versus nonresponse. Pathologic response (complete or partial) was defined as a more than 50% therapeutic effect in the breast and no invaded lymph nodes or evidence of a therapeutic effect in the lymph nodes (Sataloff TA NA-B, TA NC, or TB NA-B-C) (4).
Progression-Free Survival (PFS), EFS, and Overall Survival (OS)
The date of baseline PET acquisition was considered as the beginning of follow-up.
PFS and OS were examined in patients with occult metastases on baseline PET/CT and compared with M0 patients.
EFS was examined in all patients free of distant metastases at baseline staging and in specific subgroups. Events included local, regional, or distant recurrences or death, whichever occurred first. During NAC, patients were examined each 2 cycles. After breast surgery, patients had follow-up clinical visits every 4 mo for 2 y, then twice yearly.
Statistical Analysis
All distributions were expressed as median and range (minimum, maximum) for quantitative data or count (percentage) for categoric data. Associations between baseline tumor SUVmax and clinical or histologic/biologic parameters (e.g., presence or absence of distant metastases, tumor grade, PR expression) were examined with the Wilcoxon rank-sum test.
Survival curves were estimated using the Kaplan–Meier method. We used the log-rank test to examine the association between presence or absence of distant metastases at baseline 18F-FDG PET/CT staging and patients’ outcome. We also used the log-rank test to examine the relation between PET-derived image parameters (SUVmax and TLG measured at PET1 and PET2 and their changes between the 2 examinations) and EFS. Optimal PET parameter cutoff values for predicting EFS were determined at 3 y of follow-up with the Youden index method.
Finally, the relation between histologic/pathologic or biologic tumor characteristics (histologic type, SBR grade, PR expression, pathologic findings) and EFS were examined with the log-rank test.
All tests were 2-sided, and P values below 0.05 were considered statistically significant. Analyses were performed using R (version 3.0.2) statistical software (The R Foundation for Statistical Computing).
RESULTS
Table 1 shows the main characteristics of the 98 patients with ER+/HER2– breast carcinoma. Invasive ductal carcinoma (IDC) was the most frequent histologic type (89%); most tumors were grade 2 (67%) and PR-positive (65%). At clinical or ultrasound examination, 60 patients (61%) had findings suggestive of nodal involvement.
Overall Characteristics of 98 ER+/HER2– BC Patients
Relation of Baseline 18F-FDG PET/CT Findings with Tumor Characteristics and Patients’ Outcome
18F-FDG uptake was higher in IDC than in invasive lobular carcinoma (median SUVmax, 6.8 vs. 4.0; P = 0.018) (Table 2). Grade 3 tumors showed a higher uptake than lower grade (grade 1 + grade 2) tumors (median SUVmax, 8.3 vs. 5.4; P = 0.003). No significant association was found between tumor SUVmax and PR expression (P = 0.1). Neither clinical T score nor N score was associated with the degree of 18F-FDG uptake. Also, breast tumor SUVmax was not significantly different between patients with or without occult distant metastases on PET/CT (Table 2).
Relation Between Some Clinical or Tumor Characteristics and Tumor SUVmax in 98 Patients
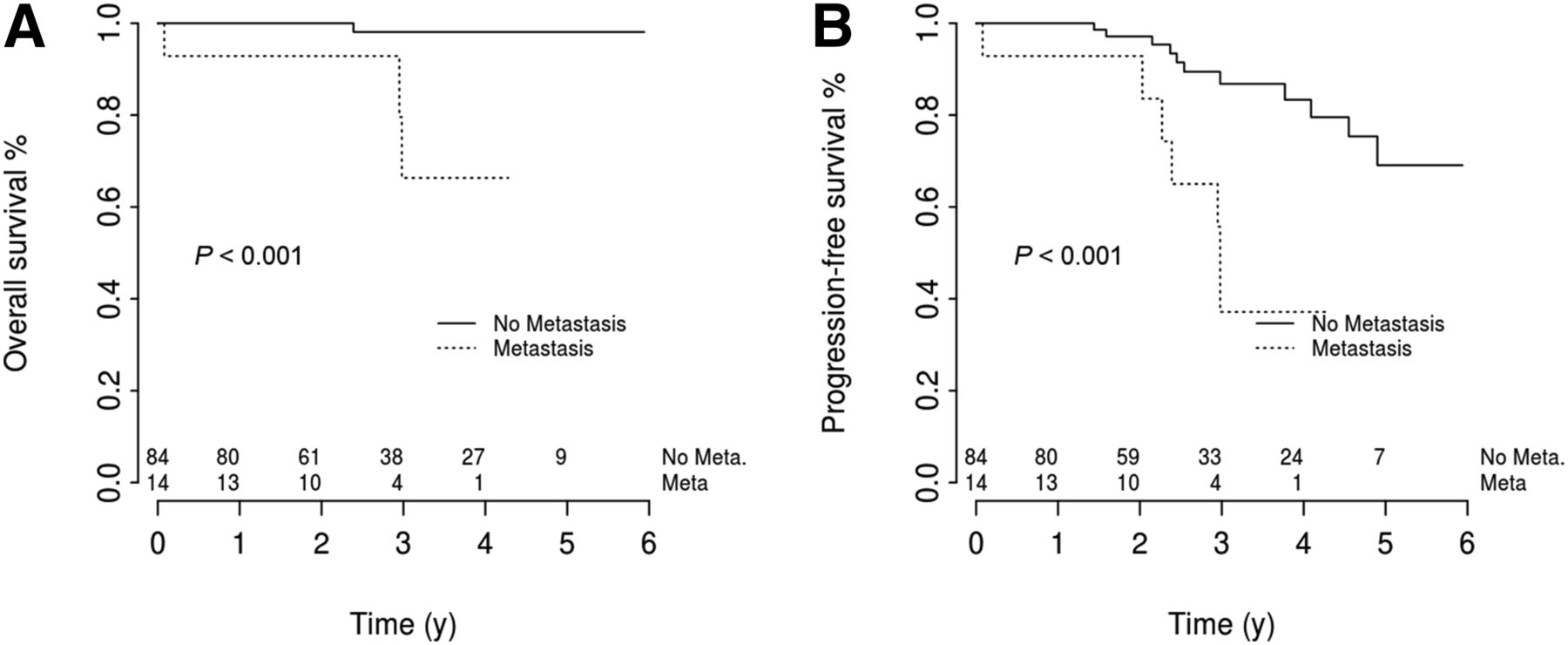
18F-FDG PET/CT revealed occult distant metastases in 14 patients (14%). PFS and OS were significantly shorter in these patients than in the 84 patients classified as M0 at baseline 18F-FDG PET/CT (P < 0.001) (Fig. 1).
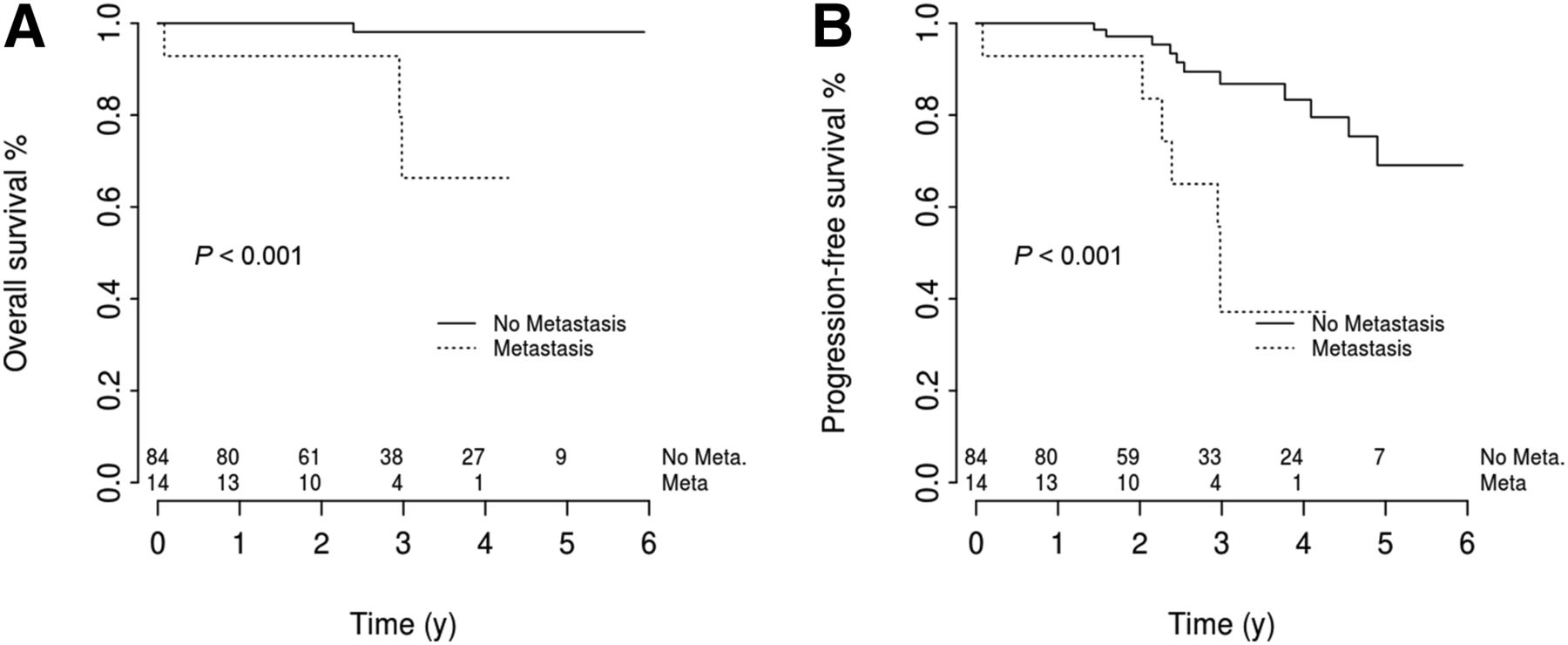
OS (A) and PFS (B) according to presence or absence of distant metastases at baseline 18F-FDG PET/CT staging in 98 patients with ER+/HER2– breast carcinoma.
Relation Between PET-Derived Parameters and EFS in M0 Patients
Of the 84 M0 patients, 2 in whom tumor metabolic volume could not be delineated on baseline PET (SUVmax ≤ 2) were excluded, except for correlations between EFS and baseline uptake. Characteristics of the 82 M0 patients who form the basis of the analysis are summarized in Table 3.
Overall Characteristics of 82 ER+/HER2– BC Patients Without Distant Metastases at Baseline Staging
Median follow-up was 35 mo. Eleven patients relapsed during the follow-up. There was a significant association between PET-derived parameters and EFS.
A high SUVmax at baseline was associated with shorter EFS (P < 0.001; Fig. 2A). The Youden Index method allowed identification of a cutoff value of 10. The 12 patients with a baseline tumor SUVmax of 10 or greater showed a high rate of relapse. Their 3-y EFS was 49% versus 92% in patients with a lower baseline SUVmax (Fig. 2A).
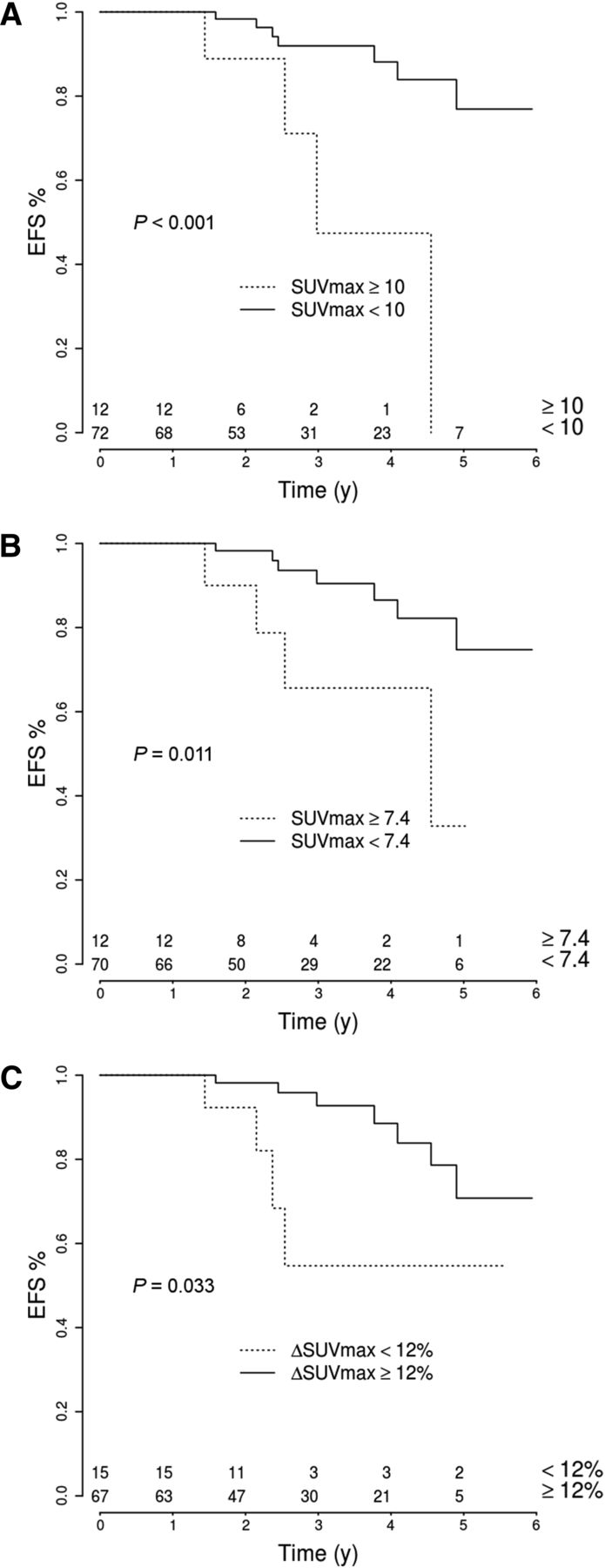
Relation between breast tumor SUVmax and EFS in 82 patients with ER+/HER2– BC. (A) SUVmax at baseline (PET1). (B) SUVmax after 2 courses of chemotherapy (PET2). (C) Change of SUVmax between PET1 and PET2 (ΔSUVmax).
A high residual SUVmax after 2 cycles of chemotherapy entailed a high risk of recurrence (P = 0.011; Fig. 2B). Again, a low change in SUVmax between PET1 and PET2 (<12% decrease) was associated with recurrence (P = 0.033; Fig. 2C).
TLG was also predictive of EFS. High TLG at baseline or after 2 courses of NAC was associated with decreased EFS (respectively, P = 0.032 and 0.017; Figs. 3A and 3B). Again, a modest decrease, or an increase in TLG after 2 cycles of chemotherapy (as it occurred in 14 patients), was associated with a high risk of relapse (P < 0.001; Fig. 3C).
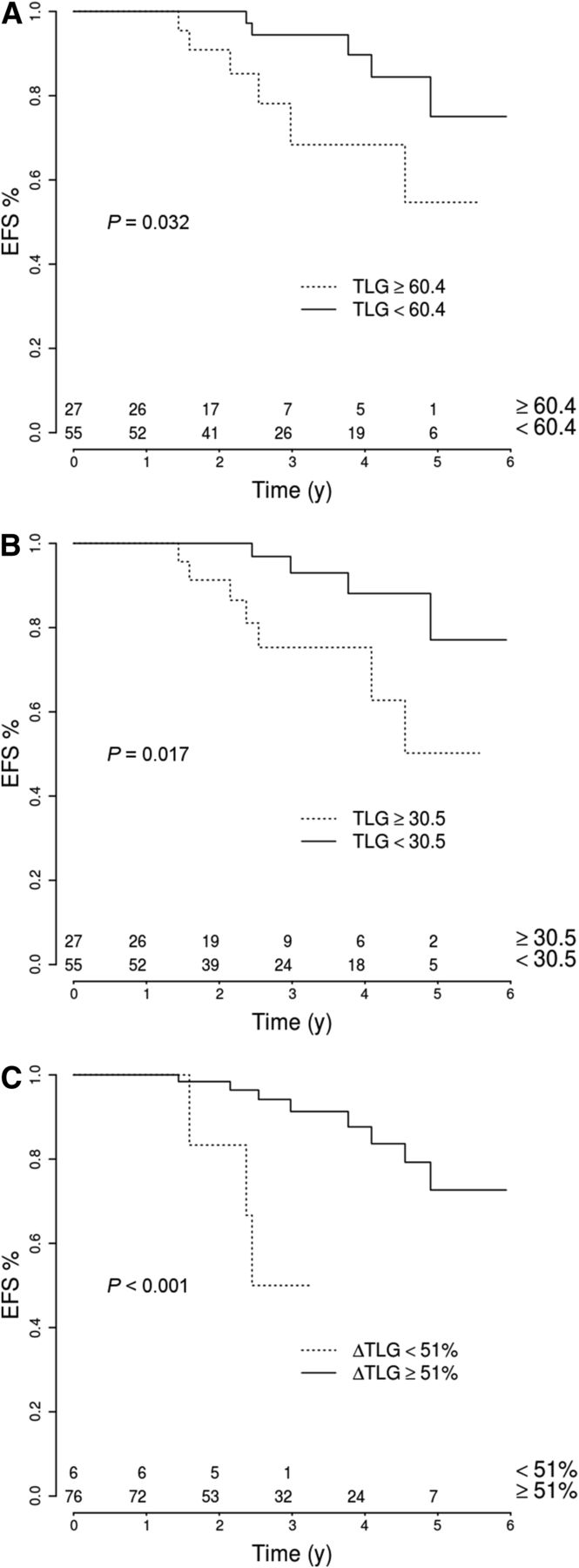
Relation between primary tumor TLG and EFS in 82 patients with ER+/HER2– BC. (A) TLG at baseline (PET1). (B) TLG value after 2 courses of chemotherapy (PET2). (C) Change of TLG between PET1 and PET2 (ΔTLG).
Relation Between Baseline Tumor Characteristics or Pathology Findings After NAC and EFS
Among baseline tumor characteristics determined on initial biopsy, only PR status was associated with EFS, with a higher risk of relapse in patients with PR-negative tumors (P = 0.019; Fig. 4). Neither histologic type (IDC vs. invasive lobular carcinoma; P = 0.93) nor SBR grade (grade 3 vs. grade 1 + 2; P = 0.25) was significantly related to EFS (Fig. 4). There was also no significant association between patient age and EFS (hazard ratio, 0.95 [95% confidence interval, 0.91–1.003]; P = 0.066).

Relation between EFS and histologic tumor type (A), tumor grade (B), PR expression (C), and response as assessed by pathology findings after NAC (D).
At completion of NAC, of the 84 M0 patients, only 4 had pCR (absence of invasive cancer in breast and lymph nodes); 35 patients showed partial response and 45 were nonresponders. No relapse was observed in the 4 women whose tumors reached pCR. There was no association between the extent of pathologic response (complete + partial vs. nonresponse) and EFS (P = 0.65) (Fig. 4D).
Baseline 18F-FDG uptake was not predictive of pathologic response (partial + complete response vs. nonresponse). Median SUVmax was 7.1 in patients with pathologic response and 5.8 in nonresponders (P = 0.30). The change in SUV after 2 courses of NAC was associated with pathologic response; ΔSUVmax was −48% (median value) in patients with pathologic response and −32% in nonresponders (P < 0.001). ΔTLG was also predictive of pathologic response (P < 0.001).
DISCUSSION
ER+/HER2– breast carcinoma is associated with less intense 18F-FDG uptake than some other phenotypes such as TN BC (6,7). Nevertheless, whole-body 18F-FDG PET/CT imaging proved efficient at depicting occult metastases. In this series of 98 women with clinical stage II–III ER+/HER2– breast carcinoma, PET/CT detected distant metastases in 14 cases (14%). PFS and OS were significantly shorter in these patients (Fig. 1), confirming previous observations in populations with mixed BC phenotypes (8,9).
We performed interim PET after 2 courses of NAC. The objective was to assess the ability of PET to predict response early. Early prediction would help avoid unnecessary side effects in the case of ineffective treatment (10). For those patients with low difference in SUV between PET1 and PET2, we cannot answer whether a scan after the last therapy would have made a more profound change in SUV. We did not make further evaluation at the end of chemotherapy. However, evaluation at the end of NAC cannot provide the opportunity to change treatment. Moreover, studies that investigated PET performance at different time points showed that PET has a lower sensitivity to predict residual disease when performed at the end of chemotherapy (11).
A major finding of our study was that PET-derived parameters (SUVmax and TLG) simply measured at baseline or their evolution after 2 cycles of NAC were predictive of EFS in the 82 M0 patients (Figs. 2 and 3). In the same patients, the extent of pathologic response (complete + partial vs. nonresponse) was not predictive of EFS (Fig. 4D). Among baseline tumor characteristics, PR negativity was associated with a higher risk of relapse, in agreement with other reported series (12). Histologic subtype and the SBR tumor grade were not predictive of EFS (Fig. 4).
pCR to NAC is known to be rare in ER+/HER− BC (only 5% of patients in the present series). When pathologic response was categorized into complete + partial response versus nonresponse, the extent of pathologic response was not predictive of patients’ outcome. Contrarily to the extent of pathology response at the end of NAC, early metabolic response as assessed by ΔSUVmax or ΔTLG after 2 cycles of NAC offered powerful prognostic value. Poor metabolic response was significantly associated with recurrence. These data suggest that early metabolic response at the breast tumor level might be representative of the impact of chemotherapy on occult micrometastatic disease.
One important finding of our study is that patients with a high baseline tumor uptake had a high risk of early recurrence. The 3-y EFS was 49% in patients with baseline tumor SUVmax of 10 or greater (vs. 92% in patients with baseline SUVmax < 10). This result might have implications in terms of using more intensive chemotherapy or novel treatment strategies within the context of clinical trials, in the case of a tumor with a high baseline 18F-FDG uptake. Enhanced surveillance may also be recommended to these patients.
In our investigation of optimal PET parameters to be used to assess response to NAC in BC, we chose to categorize patients into 3 subgroups: TN, HER2+, and ER+/HER2– BCs, which are based on immunohistochemistry tests and define subgroups receiving a homogeneous treatment regimen (2,4,13). However, other categorizations could be considered and, in particular, hormone-positive BC can also be dichotomized into luminal A (ER+/HER2– BC tumor, with low grade and low proliferation) and luminal B (which regroups high proliferative ER+/HER2– breast carcinoma and some ER+/HER2-overexpressing tumors). We, however, decided to restrict analysis to ER+/HER2– BC and exclude HER2+ tumors because these patients receive specific targeted treatments (trastuzumab) and have specific 18F-FDG PET response characteristics to NAC (13,14).
Our findings on the prognostic value of PET parameters in ER+/HER2– BC confirm and extend on previous reports. Koolen et al. observed that the change in SUV of the primary tumor early after the beginning of NAC can predict pathologic response in ER+/HER2– BC, but no information was available on the relation between changes of 18F-FDG uptake and EFS (15). In 31 ER+/HER2– BC patients, Zucchini et al. found that the change in SUVmax between baseline PET and PET performed after 2 courses of NAC was predictive of disease-free survival (16). More recently, in 61 ER+/HER2– BC patients without distant metastases, Humbert et al. found that patients with hypermetabolic tumors (SUV of breast tumor > liver SUV) had a higher risk of relapse than patients with tumors with weak 18F-FDG uptake (P = 0.04) (17). They showed that prediction was improved when an additional PET criterion (namely 18F-FDG decrease after 1 course of chemotherapy) was applied. Patients with a hypermetabolic tumor at baseline with a low SUVmax decrease after 1 course (baseline tumor SUV > hepatic SUV and ΔSUV < 16%) had a distinctly high risk of recurrence (P = 0.001). Our data are in agreement. The 12 patients with a baseline tumor SUVmax of 10 or greater showed a high rate of relapse. Their 3-y EFS was 49% versus 92% in patients with lower baseline SUVmax (P < 0.001) (Fig. 2A). Our results show also evidence on the role of another PET parameter, TLG. Because the extent of tumor response to NAC of ER+/HER2– BC is somewhat limited, we hypothesized that PET parameters taking into account metabolic volume measurement in addition to 18F-FDG uptake could be helpful. Our study suggests that TLG is a reliable prognostic tool in this specific subgroup of BC patients and deserves further investigation (Fig. 3).
Multigene recurrence scores (such as Oncotype DX) were used in some studies to select patients for chemotherapy but are less helpful to predict recurrence in patients who have received NAC.
Our study has some limitations. This was a single-institution experience. The follow-up period is still limited (median, 35 mo). Many recurrences in patients with ER+/HER2– tumors can occur between 5 and 10 y after treatment, or even later. Because the number of patients with recurrence was limited (n = 11), we could not perform a multivariate regression analysis that includes PET parameters and PR status (the only significant biologic parameter). Thus, while we provide important data on the role of 18F-FDG PET parameters in predicting patients at high risk of early relapse, our patient follow-up is ongoing. The prediction of late recurrence would be helpful for better selecting patients who might benefit from extended endocrine therapy (18).
We excluded 2 patients because of weak 18F-FDG uptake. A minimal baseline uptake is necessary to measure decrease after treatment. Importantly, our study addressed patients with large or locally advanced breast tumors referred for NAC, and only 2 patients had T1 tumors. Because small tumors can be less 18F-FDG–avid and PET measurements can be hampered by partial-volume effects, the procedure described in this paper cannot be translated to patients with T1 lesions.
We did not correlate metabolic changes on interim PET with molecular or metabolomic changes on tissue samples; obtaining a second breast biopsy from patients during NAC would be difficult.
TLG was determined according to the sophisticated fuzzy locally adaptive Bayesian approach (5). This approach has demonstrated its accuracy, robustness, and reproducibility in clinical practice (3). However, our results with TLG could have been different if we had used a less robust, threshold-based approach.
CONCLUSION
In this series of patients with large or locally advanced ER+/HER2– BC, baseline staging with 18F-FDG PET/CT identified 14% of patients with occult distant metastases who had a poor PFS and poor OS. Moreover, in M0 patients, our data show that PET-derived parameters (SUVmax and TLG) measured at baseline or after 2 courses of NAC can be predictive of EFS. These findings, if confirmed, can be helpful to plan patient follow-up but also to select high-risk patients within trials investigating novel treatment strategies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work has received a French government support granted to the CominLabs “excellence laboratory, LabEx” and managed by the National Research Agency in the “Investing for the Future” program under reference Nb. ANR-10-LABX-07-01. This study was also in part supported by an academic grant (“Translational research in oncology” INCa-DHOS-5697). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 16, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 12, 2015.
- Accepted for publication March 10, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Influence of the Amino Acid Transporter LAT1 on Patient Prognosis and the Relationships between Tumor Immunometabolic and Proliferative Features Depend on Menopausal Status in Breast Cancer
- FDG PET and FES PET Predict PFS on Endocrine Therapy--Response
- Complete Metabolic Response on Interim 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography to Predict Long-Term Survival in Patients with Breast Cancer Undergoing Neoadjuvant Chemotherapy
- 18F-Fluoroestradiol PET to Predict the Response to Neoadjuvant Treatment of Luminal Breast Cancer
- 18F-FDG PET/CT for Staging and Restaging of Breast Cancer
- 18F-FDG PET/CT for Monitoring of Treatment Response in Breast Cancer