


Neoadjuvant chemotherapy (NAC) in breast cancer (BC) allows more patients to undergo breast-conserving surgery and increases the chances of surgery in patients with primary inoperable disease. NAC also provides information on the efficacy of chemotherapy (1). Pathologic complete response (pCR) after NAC is associated with improved patient survival, especially in aggressive tumor subgroups such as human epidermal growth factor receptor 2 (HER2)–positive and triple-negative breast cancers (TNBC, lack of estrogen receptor and progesterone receptor, and no HER2 overexpression) (2). Therefore, to obtain pCR is currently a main objective in patients treated with NAC.
Early assessment of response to NAC should be potentially helpful, as it might result in the cessation of inefficient chemotherapy and allow refinement of treatment. Various studies showed the ability of the change of tumor SUVmax under therapy (ΔSUVmax) to early assess response to NAC. Four metaanalyses have been published in the last few years, showing a sensitivity for 18F-FDG PET imaging close to 80%–85% and a little less specificity (3–6). Two other metaanalyses compared PET with MRI (7,8). One showed that PET was more sensitive and MRI more specific to predict pCR (7). The second showed that PET performed during NAC outperformed MRI with higher specificity (0.69 vs. 0.42) and fairly similar pooled sensitivity (0.91 vs. 0.89) (8). Despite the relatively high sensitivity, interim PET/CT in breast cancer has not yet gained a wide audience, as opposed to other similar settings in diseases such as Hodgkin disease and aggressive non-Hodgkin lymphomas (9). This is in part due to a lack of consensus that early evaluation of response can be used to direct change in therapy in the BC neoadjuvant setting. However, in the HER2-positive BC subgroup, the multicenter randomized phase 2 trial AVATAXHER showed the helpfulness of 18F-FDG PET early assessment to optimize NAC (10). Of 142 patients, 69 were predicted to be responders to standard therapy according to the change in 18F-FDG uptake after 1 cycle. In these patients, the pCR rate was 53.6%. Of the 73 patients predicted to be poor responders, the pCR rate was 24.0% with standard treatment alone and increased to 43.8% when bevacizumab was added (10).
Early treatment response assessment could also be of help in the TNBC subgroup. Several reports highlighted the high accuracy of the early change in the SUVmax to predict pCR (11,12) and outcome (13,14) in TNBC patients. In another recent study, ΔSUVmax outperformed tumor blood flow (15).
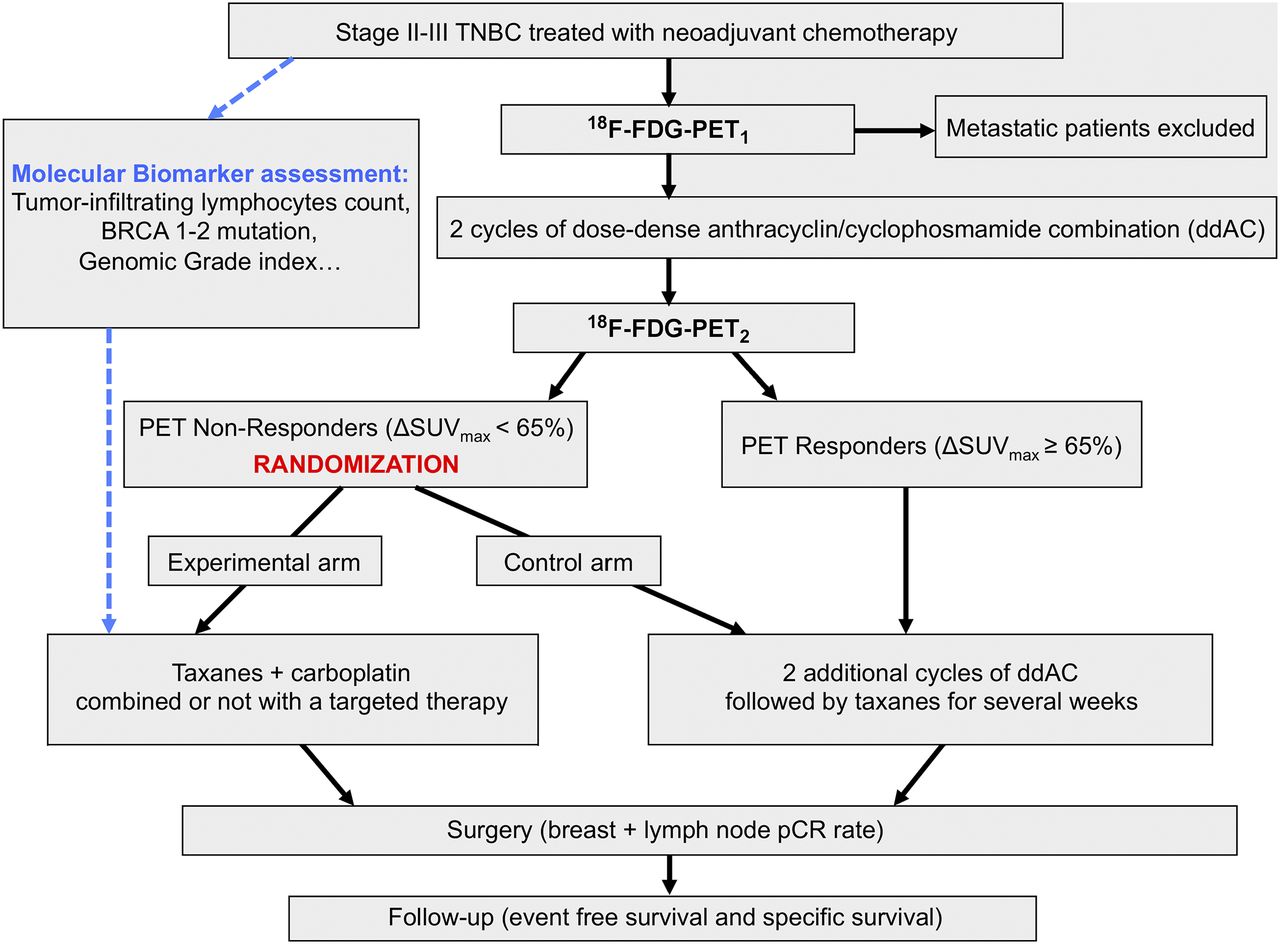
The current standard NAC in TNBC includes anthracycline–cyclophosmamide (AC) combination followed by taxanes, with dose-dense (dd) regimens suggested as potentially more efficient than standard doses (16). In TNBC patients treated by ddAC, we observed a pCR rate at surgery of 69% in patients predicted to be responders with 18F-FDG PET/CT (decrease of the tumor SUVmax after 2 cycles ≥ 65%) versus only 8% in predicted nonresponders (ΔSUVmax < 65%) (14). Alternative treatment could be used in nonresponders with the aim to increase the pCR rate. In the GeparSixto (17) and the CALGB 40603 trials (18), carboplatin showed high efficacy in TNBC patients but with greater toxicity. Additional data suggested the use of carboplatin improved the disease-free survival only in the GeparSixto study (19,20). Therefore, carboplatin is not a standard of care at this time, but it should be given in selected patients. In addition to 18F-FDG PET, molecular biomarkers determined on tumor biopsy (such as BRCA mutations, tumor-infiltrating lymphocyte count, and genomic grade index) could be of help in selecting patients for specific treatments (21). Figure 1 represents an example of a trial in which 18F-FDG PET/CT (with or without molecular biomarker) could be used to optimize NAC regimen in patients predicted to be nonresponders after 2 initial cycles of ddAC. In patients predicted to be poor responders, the association of carboplatin + taxanes ± targeted therapy will be compared with the pursuit of the ddAC regimen followed by taxanes. Some targeted therapies combined with chemotherapy are promising in TNBC patients. For example, Poly (ADP-ribose) polymerase (PARP) inhibitors, such as veliparib, have potential antineoplastic effects. I-SPY 2 is a multicenter, phase 2 platform trial that evaluates novel neoadjuvant therapies. Results from this platform trial showed that veliparib + carboplatin resulted in higher rates of pCR than standard therapy alone (22). However, the effects of carboplatin and veliparib were not evaluated separately. In another trial, the phase 3 Brightness study, the pCR rate was higher in patients treated with the paclitaxel + carboplatin + veliparib combination than in women receiving paclitaxel alone (P < 0.0001), but not compared with patients receiving paclitaxel + carboplatin (P = 0.36) (23). Another PARP inhibitor (olaparib) is currently being tested in TNBC patients (ClinicalTrials.gov identifier NCT03150576 and NCT02789332). Immunotherapy is also being actively investigated in TNBC, with preliminary promising results. Pembrolizumab added to standard therapy improved pCR rates in TNBC patients who meet I-SPY 2 eligibility (24). Other ongoing trials are currently testing the anti–PD-1/anti–PD-L1 therapy (e.g., ClinicalTrials.gov identifier NCT03281954, NCT02883062, NCT03197935, and NCT03036488). The addition of bevacizumab could also increase the pCR rate, but it is associated with higher rates of toxicity (18) and it seems not to improve patient survival (25).
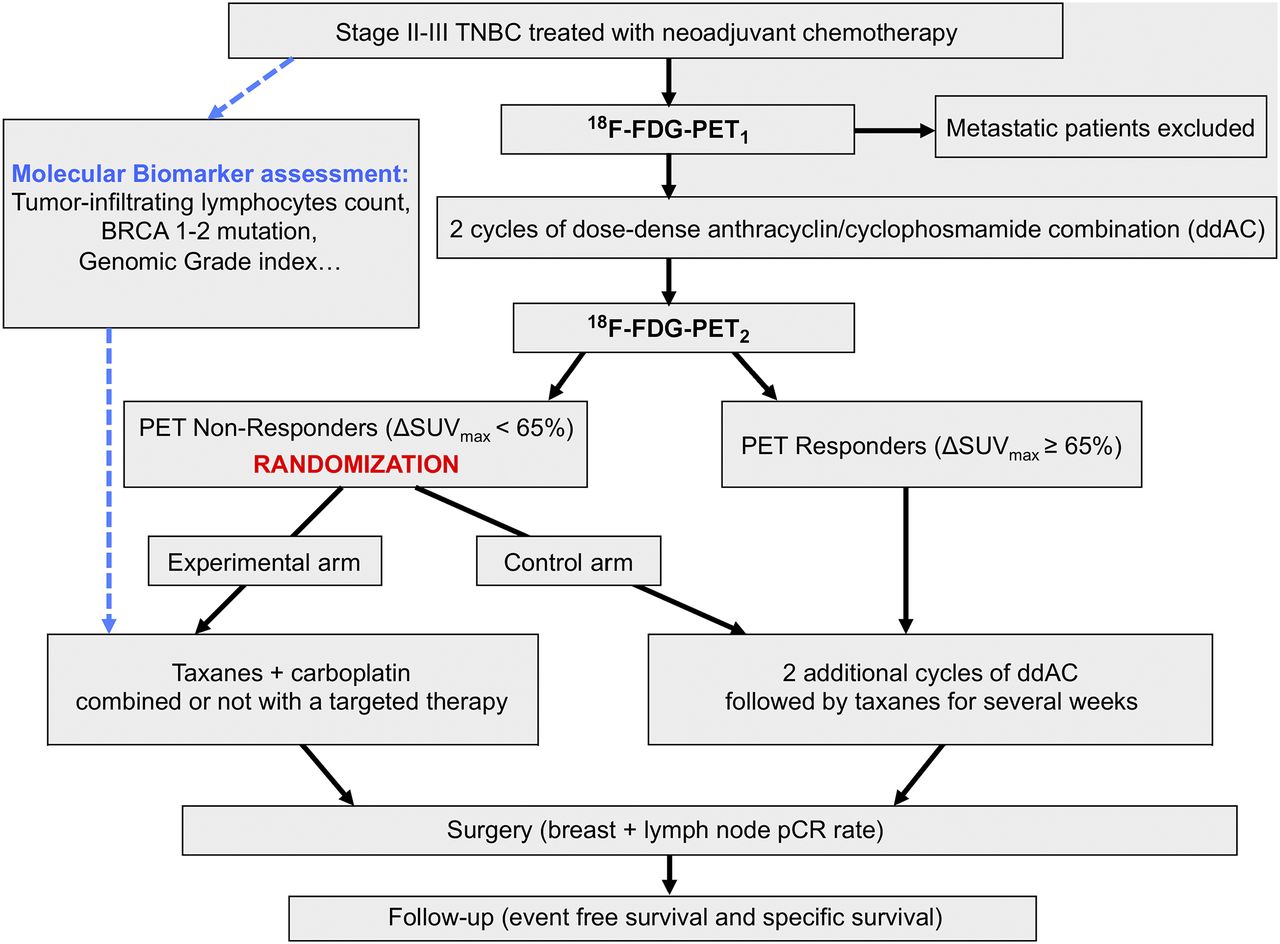
Example of a trial in which 18F-FDG PET/CT is used to optimize NAC treatment in TNBC patients predicted to be nonresponders after 2 cycles of ddAC regimen.
In conclusion, the high accuracy of ΔSUVmax to predict pCR and patient outcome has been observed in several studies. Alternative treatments being currently tested in TNBC patients treated with NAC, ΔSUVmax could be used to optimize treatment in such therapeutic trials.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 19, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 3, 2018.
- Accepted for publication April 12, 2018.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.