


Abstract
Somatostatin receptor imaging is a valuable tool in the diagnosis, follow-up, and treatment planning of neuroendocrine tumor (NET). PET-based tracers using 68Ga as the radioisotope have in most centers replaced SPECT-based tracers as the gold standard. 64Cu-DOTATATE is a new PET tracer that has been shown to be far superior to the SPECT tracer 111In-diethylenetriaminepentaacetic acid-octreotide. Because of the advantages of 64Cu over 68Ga, we hypothesized that the tracer has a higher sensitivity than 68Ga-based tracers. To test this hypothesis, we compared on a head-to-head basis the diagnostic performance of 64Cu-DOTATATE with that of 68Ga-DOTATOC in NET patients. Methods: Fifty-nine NET patients were scanned with both 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT and compared on a head-to-head basis. Discordant lesions were verified during at least 30 mo of follow-up. Results: A total of 701 lesions were concordantly detected on both 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT scans, whereas an additional 68 lesions were found by only one of the scans. 64Cu-DOTATATE showed 42 lesions not found on 68Ga-DOTATOC, of which 33 were found to be true-positive on follow-up. 68Ga-DOTATOC showed 26 lesions not found on 64Cu-DOTATATE, of which 7 were found to be true-positive on follow-up. False-positives were mainly lymph node lesions. Accordingly, 83% of the additional true lesions found on only one of the scans were found by 64Cu-DOTATATE. On a patient-basis, additional true lesions were found by 64Cu-DOTATATE and 68Ga-DOTATOC in 13 and 3 patients, respectively. All patients with additional lesions also had concordant lesions found by both scans. Conclusion: 64Cu-DOTATATE has advantages over 68Ga-DOTATOC in the detection of lesions in NET patients. Although patient-based sensitivity was the same for 64Cu-DOTATATE and 68Ga-DOTATOC in this cohort, significantly more lesions were detected by 64Cu-DOTATATE. Furthermore, the shelf life of more than 24 h and the scanning window of at least 3 h make 64Cu-DOTATATE favorable and easy to use in the clinical setting.
The diagnosis of neuroendocrine tumors (NETs) is a challenging process since the symptoms are highly variable and the tumors are often small and can arise in any part of the body.
On average, there is 5- to 7-y delay from first symptoms to diagnosis in patients with NETs (1), and by then, 20%–50% of the patients have developed metastatic disease (2). Therefore, to reduce unnecessary delay, there is a great need for an early diagnosis by a sensitive and easy accessible diagnostic imaging method. Furthermore, sensitive imaging modalities are crucial in the long-term surveillance of NETs to detect possible progression at an early stage in order to rapidly change the treatment strategy.
One common feature of most NETs is the expression of abundant somatostatin receptors on the surface of tumor cells, which makes molecular imaging with radionuclide-coupled somatostatin analogs a strong diagnostic tool (3). Five subtypes of somatostatin receptor have been identified: sst1–sst5 (4). In NETs, mainly sst2 is expressed and to a lesser degree sst1 and sst5. It is less common to find sst3 and sst4 (5–7). Several radiotracers comprising a somatostatin analog chelated to a radioisotope have been developed for somatostatin receptor imaging. Even small modifications of the amino acid sequences, as well as the conjugation to a chelator and the choice of isotope, lead to changes in the affinity toward the different somatostatin receptors (8,9). Imaging of somatostatin receptors in NETs was initially achieved by γ-cameras using either planar or SPECT technique, and in most of North America this is still the case using 111In-diethylenetriaminepentaacetic acid (DTPA)-octreotide.
The PET-based tracers, however, have major advantages over γ-emitting tracers, in terms of both detection rate and the quantitative nature (9–14). The Nordic guidelines state that PET is preferred over SPECT in the diagnostic work-up of NETs. In the European Neuroendocrine Tumor Society consensus guidelines, this recommendation of somatostatin receptor PET is supported mainly for low-proliferation gastroenteropancreatic tumors but also for neuroendocrine carcinomas with a Ki-67 of below 55% and for low-grade lung NETs (15–19).
Many NET centers in Europe, including Copenhagen, have switched to PET-based imaging of NETs using mainly 68Ga as the positron-emitting radioisotope coupled to different somatostatin analogs. The three most widely used are 68Ga-DOTANOC, which has binding affinity mainly for sst2, sst3, and sst5; 68Ga-DOTATOC, which has binding affinity mainly for sst2 and sst5; and 68Ga-DOTATATE, which binds mainly to sst2 but with the highest affinity of all (3). The U.S. Food and Drug Administration approved 68Ga-DOTATATE for diagnostic imaging of NETs in June 2016.
Recently, we introduced 64Cu-DOTATATE as a new PET tracer for somatostatin receptor imaging. Compared with 111In-DTPA-octreotide, it was superior in both radiation dose and lesion detection rates when tested on a head-to-head basis in 112 patients (14,20). The lower positron range of 64Cu than of 68Ga theoretically leads to a better spatial resolution, and the physical half-life of 12.7 h makes 64Cu-DOTATATE attractive for routine use in a clinical imaging setting. In Copenhagen, the currently used tracer is 68Ga-DOTATOC. The aim of the present study was therefore to compare, on a head-to-head basis, 64Cu-DOTATATE with 68Ga-DOTATOC, one of the PET tracers currently used most often for NETs. To determine whether discrepant lesions were true or false, clinical follow-up for 2 y as a minimum was undertaken.
MATERIALS AND METHODS
Study Design and Patients
Sixty patients, of whom 59 were evaluable, were prospectively enrolled in this study from the Departments of Clinical Endocrinology and Gastrointestinal Surgery in the Neuroendocrine Tumor Center of Excellence at Rigshospitalet, Copenhagen. All recruited patients were followed at the Center, and the inclusion criteria were primary staging or restaging. The study was approved by the Regional Scientific Ethical Committee (H-D-2008-045), and all participating patients signed an informed consent form. From June 2012 until March 2013, 60 patients underwent both 68Ga-DOTATOC PET/CT and 64Cu-DOTATATE PET/CT within 1 wk. Follow-up ended August 2015 for evaluation of whether discrepant lesions found by only one of the two PET tracers were true- or false-positive.
Synthesis and Radiolabeling of 64Cu-DOTATOC and 68Ga-DOTATATE
64Cu-DOTATATE was produced as previously described and approved under good manufacturing practice (20).
The 68Ga-DOTATOC synthesis based on the acetone method was fully automated using a Modular Lab system (Eckert & Ziegler) and performed according to manufacturer instructions. Chemicals were obtained from Rotem. The radiochemical purity of 68Ga-DOTATOC was more than 95%.
Image Acquisition
A 200-MBq injection of 64Cu-DOTATATE was administered intravenously, and PET/CT was performed after 60 min. For the 68Ga-DOTATOC scan, a 150-MBq injection was administered intravenously, and PET/CT was performed after 45 min. A Biograph 40 or 64 PET/CT scanner was used (Siemens Medical Systems). The same scanner was used for both patient scans. The CT component of the 64Cu-DOTATATE PET/CT scan was of diagnostic quality and included intravenous contrast material; the other was low dose (120 kV; effective exposure, 40 mAs). Both PET/CT scans were performed within 1 wk of each other (1–5 d apart).
The PET scan was acquired in 3-dimensional list mode for 3 min per bed position, and the patients were positioned with arms above the head and scanned from forehead to midthigh. The PET reconstruction settings were CT-based attenuation correction, resolution recovery (point-spread function, TrueX algorithm [Siemens]), and time-of-flight technique (3 iterations, 21 subsets, zoom of 1.0). A gaussian filter of 2 mm in full width at half maximum was then applied to all images after reconstruction. The PET slice thickness was 2 mm.
Image Analysis
An experienced team with a nuclear medicine specialist and a radiologist evaluated the images in consensus. In all cases, foci were identified on the PET scan, and the CT scan was used mainly to confirm the anatomic location of PET foci. All lesions on the 64Cu-DOTATATE and 68Ga-DOTATOC scans were compared, and discordant additional lesions were noted for each of the scans.
Lesion sites were divided into regions or groups: liver, pancreas, intestines, lung, bones, lymph nodes, carcinomatosis, and other (ovaries, mamma, soft tissue, and other less common regions). The number of PET-positive lesions (≤20) in each region was counted, and the SUVmax of one concordant lesion in each region was noted. Furthermore, SUVmax was identified for several reference areas (liver, bone, lung, muscle, spleen, pancreas, intestine, and pituitary) in both scans. To compute tumor-to-background ratios (TBRs), background SUVs for organs (liver, lung, pancreas, bones, and intestines) were obtained from nondiseased areas within the same organ. The fifth vertebra was used as background for bone lesions when no SUV for reference bone was available in the same area. A muscle reference was used as background for lymph node TBR and, if no intestinal reference was available, also for carcinomatosis TBR. All TBRs of corresponding 64Cu-DOTATATE and 68Ga-DOTATOC scans were computed from the same background area on the two scans.
Clinical follow-up was more than 2 y. Discordant lesions were controlled by comparison to all available later images of the patients (68Ga-DOTATOC PET/CT, CT, and MR) to verify the lesions as true- or false-positive findings.
Statistical Analysis
Dedicated statistical software was used for analysis (SPSS Statistics, version 22.0; IBM Corp.). For comparison of discrepant lesions using different PET tracers in the same patient, we applied the McNemar test for paired proportions corrected for continuity. The probability that a discordant observation was found by 64Cu-DOTATATE was reported with the exact binomial confidence interval. The t test for paired samples was used to compare SUVmax for the two scans and to compare the TBRs.
RESULTS
One patient was omitted from the study at the quality check because the 68Ga-DOTATOC had been subcutaneously injected. The characteristics of the remaining 59 patients are listed in Table 1. The 64Cu-DOTATATE and 68Ga-DOTATOC PET scans were compared at 3 levels (lesion-, region-, and patient-based). An overview of lesions and regions in patients with discordant scans is given in Table 2. The total number of lesions and the number of true-discordant lesions are listed in Table 3.
Characteristics of the 59 Patients
Patients with Discordant Lesions on 64Cu-DOTATATE or 68Ga-DOTATOC PET
Comparison of Concordant and True-Positive Discordant Lesions Found by Concurrent 64Cu-DOTATATE and 68Ga-DOTATOC PET in the 59 Patients with NETs
Lesions
In total, 701 PET-positive lesions were found by both tracers (concordant lesions), whereas an additional 68 lesions were found by only one tracer (discordant lesions).
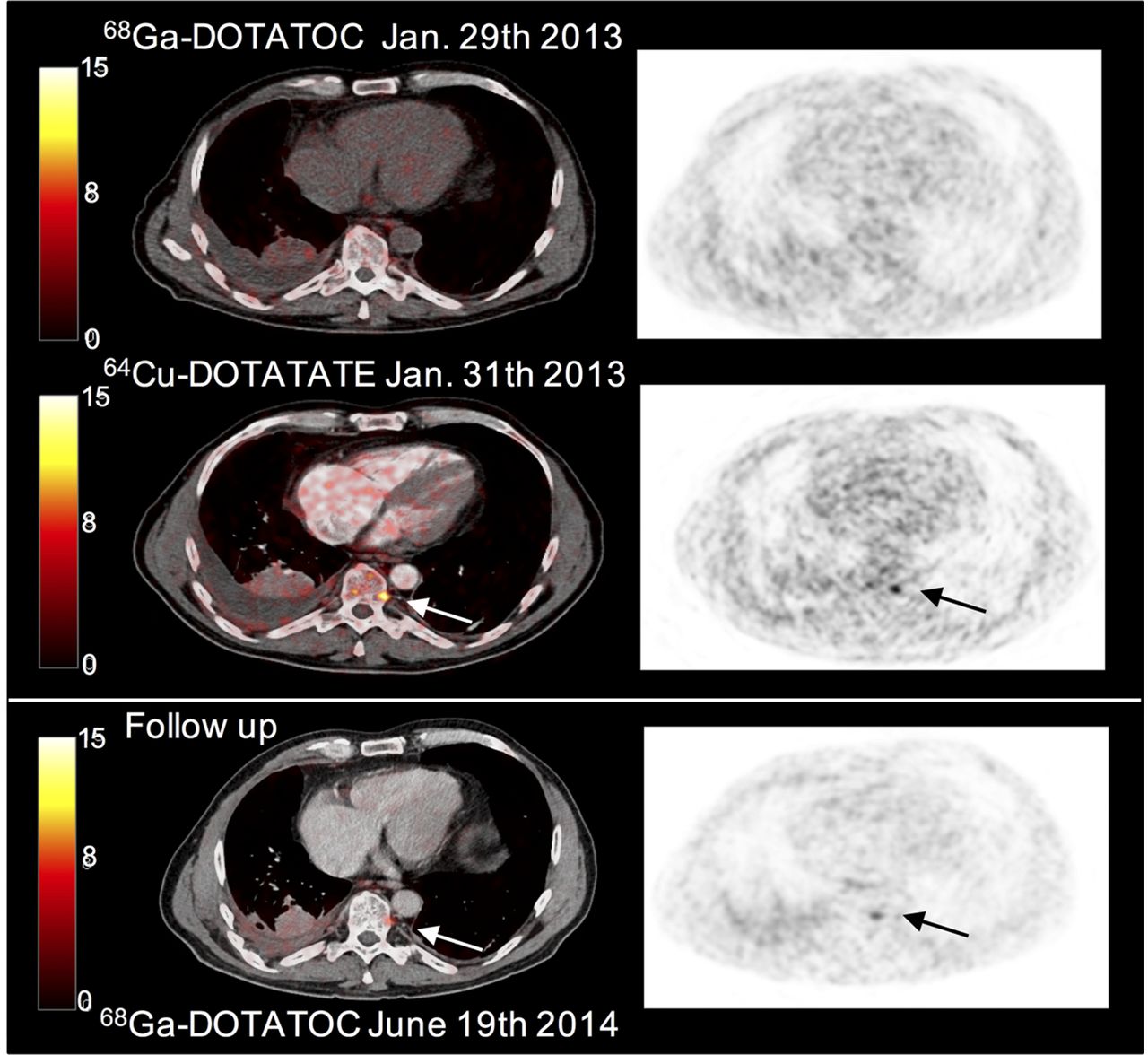
For the 22 patients with divergent scans, all lesions found by the two tracers are listed in Table 2 according to tumor type, histology, region, and follow-up. 64Cu-DOTATATE found 42 discordant lesions, and 33 of these were confirmed during follow-up to be true-positive. A patient with a discordant bone lesion found only by 64Cu-DOTATATE is seen in Figure 1. In this case, the true-positive nature of the finding was confirmed by positivity on a second 68Ga-DOTATOC scan performed during follow-up 18 mo later. 68Ga-DOTATOC found 26 discordant lesions, and 7 were confirmed to be true-positive (Table 2). Thus, 64Cu-DOTATATE found significantly more true-positive discordant lesions than 68Ga-DOTATOC (33 additional lesions vs. 7, P < 0.001). Of the true-positive discordant lesions, 83% were revealed by 64Cu-DOTATATE but only 17% by 68Ga-DOTATOC.
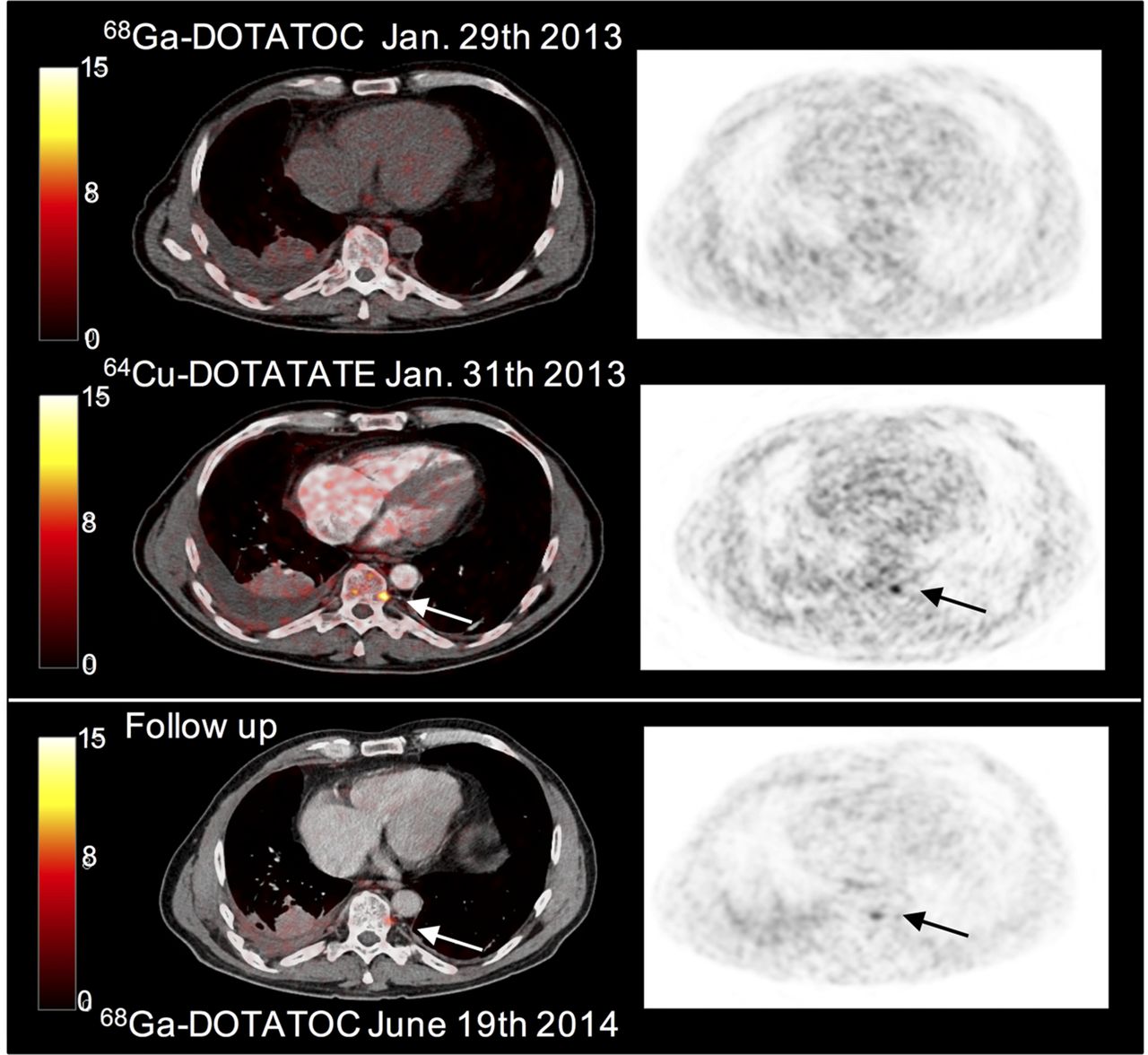
Initial PET/CT (left) and PET (right) scans show an additional bone lesion (arrow) with 64Cu-DOTATATE. Follow-up with 68Ga-DOTATOC confirms that finding was true-positive.
Regions
The additional true lesions found by 64Cu-DOTATATE were located in bones, liver, lymph nodes, pancreas, or soft tissue or were carcinomatosis, whereas the additional true lesions found by 68Ga-DOTATOC were located in liver, lymph nodes, and bone.
The probability that 64Cu-DOTATATE would find a true-positive discordant lesion in bone was 85%. All discordant true-positive findings of carcinomatosis (n = 7) were detected by 64Cu-DOTATATE.
Most false-positive discordant foci (16/19) that were in both scans were located in lymph nodes and, to a lesser degree, in bone (Tables 2 and 3). There were significantly more false-positive discordant findings on 68Ga-DOTATOC scans than on 64Cu-DOTATATE scans (18/26 vs. 1/42).
Patients
Discrepant lesions between the 64Cu-DOTATATE and 68Ga-DOTATOC scans were found in a total of 22 patients (Table 2). Most additional lesions were found by 64Cu-DOTATATE (in 14 patients), whereas 68Ga-DOTATOC found additional lesions in 8 patients.
Follow-up confirmed that in 13 of 14 patients, 64Cu-DOTATATE was true-positive for additional lesions, whereas a single PET-positive lymph node in the last patient (patient 30, Table 2) could not be verified.
In 3 of the 8 patients with additional lesions found by 68Ga-DOTATOC, they were confirmed to be true-positive on follow-up. The additional lesions in the remaining 5 patients were not found on later imaging (68Ga-DOTATOC, CT, or MR) and thus were considered false-positive. Altogether, significantly more patients (13 vs. 3) had additional true-positive lesions found by 64Cu-DOTATATE (P = 0.013).
In 37 of the 59 patients, the 64Cu-DOTATATE and 68Ga-DOTATOC scans were concordant. The 2 lung NETs and 26 other NETs had multiple concordant lesions. In one of the patients, concordant positive lymph nodes turned out to be false-positive on follow-up, whereas the rest were considered true-positive. Nine patients showed no lesions on either of the scans, and they were confirmed to be true-negative on follow-up.
Although additional true lesions were found in 13 patients by 64Cu-DOTATATE and in 3 patients by 68Ga-DOTATOC, the sensitivity to diagnose NET disease in a patient was 100% (95% confidence interval [CI], 93%–100%), the specificity was 90% (95% CI, 56%–100%), the positive predictive value was 98% (95% CI, 90%–100%), and the negative predictive value was 100% (95% CI, 66%–100%) in both scans because concordant lesions were also found in all patients with additional lesions (Table 2). One example of such a patient is shown in Figure 2, where additional foci are seen in the intestinal region on the 64Cu-DOTATATE scan. However, the diagnosis of primary intestinal tumor with widespread metastases was the same for both tracers.
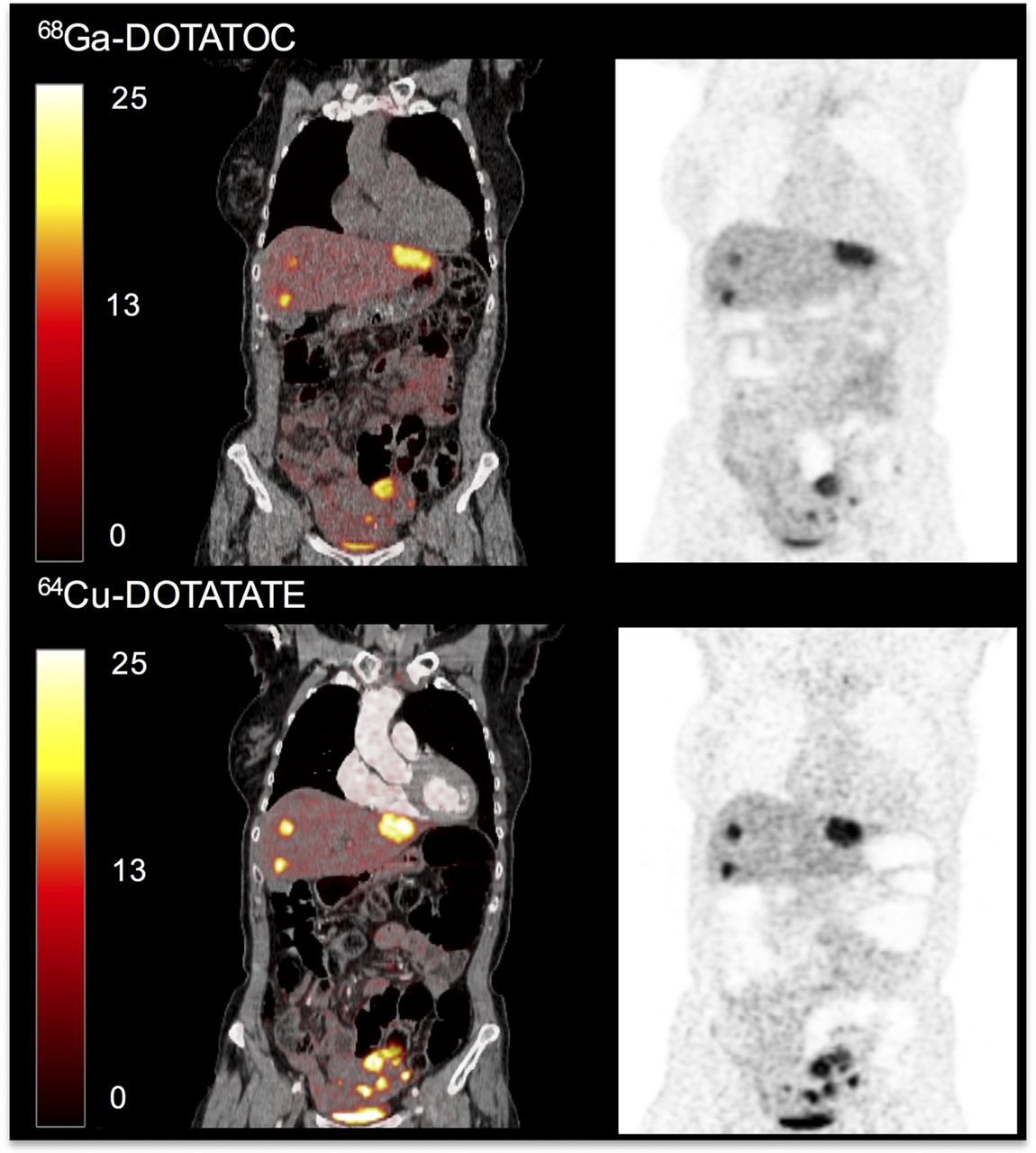
PET/CT (left) and PET (right) scans of patient with intestinal NET and multiple metastases. More lesions are seen in intestinal region with 64Cu-DOTATATE than with 68Ga-DOTATOC.
Tracer Uptake
SUVmax was significantly higher for 64Cu-DOTATATE than for 68Ga-DOTATOC in liver lesions, lymph nodes, pancreatic lesions, intestinal tumors, and carcinomatosis lesions (Supplemental Table 1, available at http://jnm.snmjournals.org). Bone and lung did not significantly differ. The physiologic background uptake of the tracers was lower for 68Ga-DOTATOC in all tissues except the spleen, where background uptake of 68Ga-DOTATOC was significantly higher than that of 64Cu-DOTATATE (Fig. 3; Supplemental Table 2).

68Ga- and 64Cu-DOTATATE PET/CT scans (color) and PET scans (black and white) of patient with intestinal NET and multiple metastases. Same 4 liver lesions are seen on transaxial images (left), and same 2 bone lesions are seen on coronal images (middle and right). Foci are more distinct with 64Cu-DOTATATE than with 68Ga-DOTATOC. Spleen shows much higher uptake of 68Ga-DOTATOC than of 64Cu-DOTATATE.
The TBRs for the two tracers were compared within the 6 most typical regions—liver, lymph nodes, bone, lung, pancreas, and intestines—for 64Cu-DOTATATE and 68Ga-DOTATOC, and the results are shown in Table 4.
Comparison of TBR for 64Cu-DOTATATE and 68Ga-DOTATOC in the 59 Patients with NETs
The TBR for bones was significantly higher for 68Ga-DOTATOC than for 64Cu-DOTATATE. All other regions showed no significant differences.
DISCUSSION
Data on the diagnostic performance of 64Cu-DOTATATE PET versus 111In-DTPA-octreotide SPECT in NET patients were presented recently (14). Twice as many lesions were found by 64Cu-DOTATATE, and additional organ involvement was detected in one third of the enrolled patients. There is no doubt that 64Cu-DOTATATE should be preferred whenever possible over 111In-DTPA-octreotide. However, most countries in Europe have changed their somatostatin receptor imaging of NETs to PET technology using 68Ga-based tracers, and a similar trend applies in North America. Accordingly, the true challenge is how 64Cu-DOTATATE performs in comparison with these widely used 68Ga-based somatostatin receptor imaging tracers.
Both 64Cu-DOTATATE and 68Ga-DOTATOC were a priori expected to be highly sensitive. Accordingly, it was not surprising that on a patient basis there were no differences in the diagnostic performance of the two tracers. Nevertheless, significantly more additional true-positive lesions were revealed by 64Cu-DOTATATE than by 68Ga-DOTATOC: 33 versus 7.
It is a special characteristic of NET patients that they often live many years with widespread disease while receiving multiple treatments. Changes in treatment strategy are nearly always based on clinical or imaging-based signs of progression. Thus, a high performance in the detection of any new lesions is of great value in these patients. Additional lesions found by the 64Cu-DOTATATE scan in the present study could not a priori be interpreted as a sign of progression since it was the first time this new tracer had been used in these patients. Thus, the clinical impact of these additional findings could not be evaluated in the present study.
It could be argued that the difference found in our study was not due to use of a different isotope but rather to a difference in the peptide. Accordingly, the affinity (half-maximal inhibitory concentration) toward sst2 is approximately 10-fold higher for DOTATATE than for DOTATOC. Also, DOTATOC, in contrast to DOTATATE, has some affinity toward sst5 (8). However, in NETs, expression of sst2 receptors is much higher than that of any of the other subtypes (6). Accordingly, differences in non–sst2 receptor affinity are not expected to be of any importance. Also, the difference in sst2 receptor affinity seems clinically unimportant, as a recent review of PET tracers for somatostatin receptor imaging reported only marginal and inconsistent differences in diagnostic performance in NET patients between the 3 most frequently used 68Ga-labeled somatostatin analogs: DOTATATE, DOTATOC and DOTANOC (3,21–27). In the only 2 studies that compared 68Ga-DOTATATE and 68Ga-DOTATOC head to head, by Poeppel et al., 68Ga-DOTATOC showed the greatest number of lesions and the highest uptake in lesions (22,25). In contrast, a metaanalysis from 2014 found a higher patient-based sensitivity and specificity for 68Ga-DOTATATE than for 68Ga-DOTATOC (28). Thus, no consistent conclusion exists in which peptide is the most sensitive for overall NET imaging.
The difference in lesion detection rate found in the current study is presumed to relate to use of 64Cu instead of 68Ga rather than to differences in peptide. This finding was as expected, because the substantially shorter positron range of 64Cu was anticipated to lead to better detection of small lesions.
The radiation burden is higher for 64Cu-DOTATATE than for 68Ga-DOTATOC, mainly because of the differences in positron-branching fraction. The positron-branching fraction is 0.17 for 64Cu-DOTATATE and 0.89 for 68Ga-DOTATOC, leading to the need to inject a higher dose of 64Cu-DOTATATE to obtain the same number of counts as for 68Ga-DOTATOC. However, the longer half-life of 64Cu than of 68Ga pulls in the opposite direction. Therefore, only a 33% higher dose of 64Cu-DOTATATE was used despite a nearly 5 times higher branching ratio for 68Ga-DOTATOC. The higher radiation burden to the patient from 64Cu-DOTATATE has to be considered. However, in our view this is not of any safety concern. Our typical 64Cu-DOTATATE dose of 180–220 MBq results in a radiation dose of 5.7–8.9 mSv to the patient (20), whereas 120–200 MBq of 68Ga-DOTATOC results in 2.8–4.6 mSv (29). For comparison, the radioactive burden from the γ-emitting tracers 111In-DTPAOC and 111In-DOTATOC, which are still used at many centers, is higher (5.7–11.1 mSv and 7.0–10.0 mSv, respectively) (30).
The TBR, or image contrast, did not significantly differ between the two tracers except in bone. Presumably, this finding is not a determinant for detection of bone lesions since the mean TBR for bone was high for both tracers and 64Cu-DOTATATE actually did find significantly more lesions than 68Ga-DOTATOC.
As a convenient standard workflow, we scanned patients 1 h after injection of 64Cu-DOTATATE. This timing was comparable to the routine workflow for the 68Ga-labeled somatostatin receptor PET tracers. However, based on the comparison of image quality and the stable SUVs for tumors reported in our previous publication (20), an advantage of 64Cu-DOTATATE is the possibility of scanning at any time between 1 and 3 h. Potential better TBRs might be found using a later scanning time, but this possibility cannot be proven in this setup. Finally, 64Cu-DOTATATE is produced with a shelf-life of 24 h, logistically circumventing the need for coordination between radiochemistry production and patient arrival.
Our study had some limitations. It cannot be ruled out that the acquisition of a diagnostic CT scan together with the 64Cu-DOTATATE PET scan, but not with the 68Ga-DOTATOC scan, might have made it easier to detect small lesions using 64Cu-DOTATATE. However, since the images were not masked but were compared pairwise, head-to-head (lesion-to-lesion), after the initial lesion detection, the possibility that any lesions would not be found merely because of differences in the CT scan seems unlikely. Furthermore, if we had wanted to assess whether only the change in isotope makes a difference, the fact that we did not compare 64Cu-DOTATATE with 68Ga-DOTATATE would have been a limitation of our study. However, high sensitivity has been seen using both 68Ga-DOTATATE and 68Ga-DOTATOC, with no clear documentation of the superiority of one over the other, and therefore it is most likely that it was the difference in radioisotope that caused the differences in our findings. Nevertheless, our main purpose was to see whether 64Cu-DOTATATE could compete with the commonly used 68Ga-DOTATOC PET tracer.
CONCLUSION
Although patient-based sensitivity was the same for 64Cu-DOTATATE and 68Ga-DOTATOC in this cohort, 64Cu-DOTATATE had a substantially better lesion detection rate in NET patients than did 68Ga-DOTATOC. Follow-up revealed that most of the additional lesions detected by 64Cu-DOTATATE were true-positive. The lower positron range of 64Cu than of 68Ga is probably the main explanation for the better performance. Furthermore, the shelf life of more than 24 h and the flexible scanning window of at least 3 h make 64Cu-DOTATATE attractive for use in clinical routine. Whether detection of more true lesions translates into better patient management and outcome remains to be proven.
DISCLOSURE
This work was supported in part by the National Advanced Technology Foundation, Danish Cancer Society, Lundbeck Foundation, Novo Nordic Foundation, Danish Medical Research Council, Svend Andersen Foundation, Research Council for Strategic Research, Rigshospitalets Research Council, Research Foundation of the Capital Region, Arvid Nilsson Foundation, John and Birthe Meyer Foundation, and A.P. Moeller Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Andreas Kjaer and Ulrich Knigge are inventors on a filed patent application: “PET tracer for imaging of neuroendocrine tumors” (WO 2013029616 A1). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
The staff at the Department of Clinical Physiology, Nuclear Medicine, and PET is gratefully acknowledged for help in providing the PET tracers and performing the PET/CT studies.
Footnotes
Published online Sep. 22, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 30, 2016.
- Accepted for publication September 1, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Routine Use of [64Cu]Cu-DOTATATE PET/CT in a Neuroendocrine Tumor Center: Referral Patterns and Image Results of 2,249 Consecutive Scans
- Somatostatin Receptor Imaging with [18F]FET-{beta}AG-TOCA PET/CT and [68Ga]Ga-DOTA-Peptide PET/CT in Patients with Neuroendocrine Tumors: A Prospective, Phase 2 Comparative Study
- Preclinical Comparison of the 64Cu- and 68Ga-Labeled GRPR-Targeted Compounds RM2 and AMTG, as Well as First-in-Humans [68Ga]Ga-AMTG PET/CT
- Somatostatin Receptor-PET/CT/MRI of Head and Neck Neuroendocrine Tumors
- Evaluation of [68Ga]-DOTATOC PET/MRI in Patients with Meningioma of the Subcranial and Intraorbital Space
- An Investigation of Lesion Detection Accuracy for Artificial Intelligence-Based Denoising of Low-Dose 64Cu-DOTATATE PET Imaging in Patients with Neuroendocrine Neoplasms
- An Investigation of Lesion Detection Accuracy for Artificial Intelligence-Based Denoising of Low-Dose 64Cu-DOTATATE PET Imaging in Patients with Neuroendocrine Neoplasms
- SNMMI Procedure Standard/EANM Practice Guideline for SSTR PET: Imaging Neuroendocrine Tumors
- Choice Is Good at Times: The Emergence of [64Cu]Cu-DOTATATE-Based Somatostatin Receptor Imaging in the Era of [68Ga]Ga-DOTATATE
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- Semiautomatic Tumor Delineation for Evaluation of 64Cu-DOTATATE PET/CT in Patients with Neuroendocrine Neoplasms: Prognostication Based on Lowest Lesion Uptake and Total Tumor Volume
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- Treatment of advanced gastroenteropancreatic neuroendocrine neoplasia, are we on the way to personalised medicine?
- 18F-FDG PET is Superior to WHO Grading as a Prognostic Tool in Neuroendocrine Neoplasms and Useful in Guiding PRRT: A Prospective 10-Year Follow-up Study
- 64Cu-DOTATATE PET in Patients with Neuroendocrine Neoplasms: Prospective, Head-to-Head Comparison of Imaging at 1 Hour and 3 Hours After Injection
- 64Cu-DOTATATE PET/CT and Prediction of Overall and Progression-Free Survival in Patients with Neuroendocrine Neoplasms
- 64Cu-DOTATATE PET/CT for Imaging Patients with Known or Suspected Somatostatin Receptor-Positive Neuroendocrine Tumors: Results of the First U.S. Prospective, Reader-Masked Clinical Trial
- Improving Contrast and Detectability: Imaging with [55Co]Co-DOTATATE in Comparison with [64Cu]Cu-DOTATATE and [68Ga]Ga-DOTATATE
- Somatostatin Receptor 2-Targeting Compounds