


Visual Abstract

Abstract
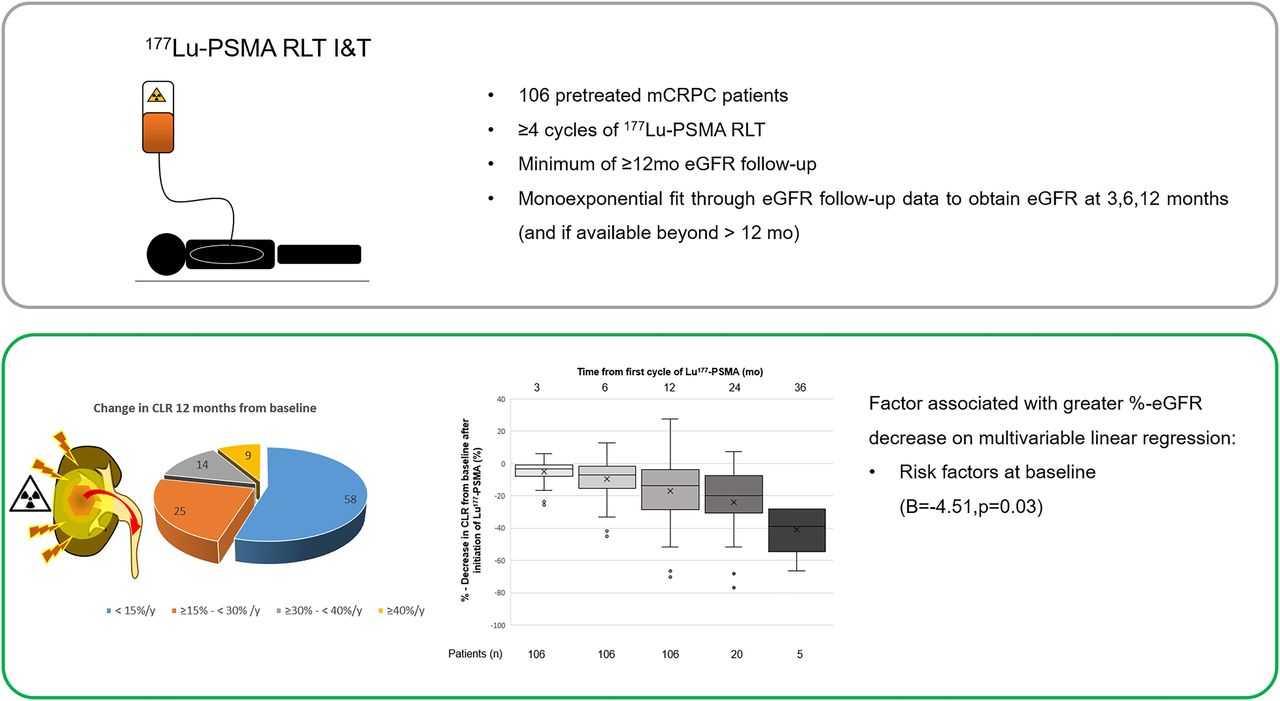
β-emitting 177Lu targeting prostate-specific membrane antigen (PSMA) is an approved treatment option for metastatic castration-resistant prostate cancer. Data on its long-term nephrotoxicity are sparse. This study aimed to retrospectively evaluate post–177Lu-PSMA estimated glomerular filtration rate (eGFR) dynamics for at least 12 mo in a cohort of metastatic castration-resistant prostate cancer patients. Methods: The institutional databases of 3 German tertiary referral centers identified 106 patients who underwent at least 4 cycles of 177Lu-PSMA and had at least 12 mo of eGFR follow-up data. eGFR (by the Chronic Kidney Disease Epidemiology Collaboration formula) at 3, 6, and 12 mo after 177Lu-PSMA radioligand therapy was estimated using monoexponentially fitted curves through available eGFR data. eGFR changes were grouped (≥15%–<30%, moderate; ≥30%–<40%, severe; and ≥40%, very severe). Associations between eGFR changes (%) and nephrotoxic risk factors, prior treatment lines, and number of 177Lu-PSMA cycles were analyzed using multivariable linear regression. Results: At least moderate eGFR decreases were present in 45% (48/106) of patients; of those, nearly half (23/48) had a severe or very severe eGFR decrease. A higher number of risk factors at baseline (−4.51, P = 0.03) was associated with a greater eGFR decrease. Limitations of the study were the retrospective design, lack of a control group, and limited number of patients with a follow-up longer than 1 y. Conclusion: A considerable proportion of patients may experience moderate or severe decreases in eGFR 1 y from initiation of 177Lu-PSMA. A higher number of risk factors at baseline seems to aggravate loss of renal function. Further prospective trials are warranted to estimate the nephrotoxic potential of 177Lu-PSMA.
Prostate-specific membrane antigen (PSMA)–targeted radioligand therapy (RLT) with 177Lu-PSMA-617 was recently approved for the treatment of metastatic castration-resistant prostate cancer (mCRPC) after taxane-based chemotherapy (1,2). Despite its overall favorable side effect profile, primary safety concerns during 177Lu-PSMA RLT are critical radiation doses to cancer-unaffected sites due to physiologic expression of PSMA (e.g., in the salivary glands and kidneys).
A recent systematic review and metaanalysis reported nephrotoxicity of any stage in 9.5% of 744 patients treated with 177Lu-PSMA (3). Consistently, the phase III VISION trial on 177Lu-PSMA (177Lu-PSMA-RLT plus the standard of care versus the standard of care alone) reported renal toxicity of any stage in 8.7% of patients in the intervention arm versus 5.9% in the control arm. Of note, severe renal toxicity (stages 3–5) was observed in 3.4% of patients in the 177Lu-PSMA group and in 2.9% in the group receiving the standard of care alone (2).
However, these data may underestimate the long-term incidence of renal toxicity, as it is known from external-beam radiotherapy (EBRT) and other radionuclide therapies that toxicity may develop over a longer period (>1 y) and median survival in the VISION study was only 15.3 mo. We recently reported 3 patients who developed severe radiation nephropathy with a histologically proven renal thrombotic microangiopathylike picture after extensive treatment with 177Lu-PSMA RLT (4).
Nephropathy after 177Lu-PSMA RLT is attributed mainly to the renal tubular PSMA expression and the renal excretion of 177Lu-PSMA, resulting in a prolonged retention of the β− emitter in the kidneys (5). Definitive dose limits for RLT are not established, and current thresholds are based on observations with EBRT. Here, homogeneous irradiation of the whole kidneys with 23 and 28 Gy was associated with a 5% and 50% risk of severe radiation nephritis, respectively, within 5 y after treatment (6). However, compared with EBRT, the radiation to the kidneys by 177Lu-PSMA is of lower energy, is delivered over a longer period, and is not homogeneously distributed within the kidney tissue (7).
Several, mainly retrospective, studies investigated the renal absorbed dose from 177Lu-labeled PSMA ligands. For 177Lu-PSMA 617 and 177Lu-PSMA I&T, mean renal absorbed doses of 0.5 Gy/GBq (SD, 0.2) and 0.7 Gy/GBq (SD, 0.2) have been reported (8). Extrapolating these population-based dose estimates to clinical practice, 4 and 6 cycles with a standard activity of 7.4 GBq of 177Lu-PSMA I&T would result in mean absorbed doses of 20 and 31 Gy, respectively, to the kidneys. Because of the large interindividual variability of renal doses (coefficient of variation, 40%), a significant fraction of patients will receive even substantially higher renal doses exceeding the dose limits established for EBRT (6).
The aim of our retrospective analysis was to evaluate long-term changes in the estimated glomerular filtration rate (eGFR) in mCRPC patients who underwent at least 4 cycles of 177Lu-PSMA at 3 German tertiary referral centers. We investigated the association of the number of risk factors associated with impaired renal function at baseline, the number of prior treatment lines, and the number of 177Lu-PSMA cycles with the percentage eGFR decrease 12 mo from initiation of 177Lu-PSMA RLT.
MATERIALS AND METHODS
Patients
For this retrospective analysis, the institutional databases of 3 tertiary referral centers in Germany (Technical University of Munich, University of Wurzburg, and University of Augsburg) were screened for patients who initiated and completed 177Lu-PSMA I&T RLT between December 2015 and May 2021.
Patients were included if they underwent at least 4 cycles of 177Lu-PSMA I&T RLT, had at least 1 y of follow-up eGFR data after treatment initiation, and had no evidence of urinary tract obstruction on pretreatment 99mTc-mercaptoacetyltriglycine scintigraphy. The retrospective analysis was approved by the local responsible institutional review boards (approvals 115/18S, 2020-40, and 20200609 01).
Institutional eligibility criteria for using 177Lu-PSMA I&T RLT as an individual treatment decision were previously published (9). The production and administration of 177Lu-PSMA I&T complied with the German pharmaceutical law (Arzneimittelgesetz, §13.2b) and the responsible regulatory bodies. All patients gave written informed consent and were treated under the conditions of the Declaration of Helsinki, article 37, “Unproven Interventions in Clinical Practice.” Each patient received intravenous hydration (500 mL of 0.9% NaCl) starting 30 min before treatment infusion. The 177Lu-PSMA I&T solution was intravenously administered.
Measures
All serum creatinine (Scr) values recorded at baseline and throughout a minimum of 12 mo from the initiation of therapy were collected and used to calculate the eGFR using the Chronic Kidney Disease Epidemiology Collaboration formula. This formula considers factors such as Scr, age, sex, and ethnicity. The Chronic Kidney Disease Epidemiology Collaboration equation is eGFR = 141 × min(Scr/κ, 1)α × max(Scr/κ, 1)1.209 × 0.993age, where κ is 0.9, α is −0.411, min is the minimum of Scr/κ or 1, and max is the maximum of Scr/κ or 1 (10). Renal failure stages were subsequently defined according to Chronic Kidney Disease Epidemiology Collaboration criteria at baseline and at the 12-mo follow-up.
A monoexponential curve was fitted through all available eGFR data (from initiation of treatment to at least 12 mo) for every patient to obtain a standardized eGFR estimate at the predefined time points (3, 6, and 12 mo) (11). Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org) depicts the monoexponential estimates for 2 patients. If patients had follow-up data beyond 12 mo, these were recorded up to a maximum of 36 mo from initiation of therapy.
For every patient, the percentage changes from baseline at the predefined time points (3, 6, and 12 mo) were subsequently calculated. Clinically relevant percentage eGFR decrease cutoffs from baseline were set (≥15%–<30%, moderate; ≥30%–<40%, severe; and ≥40%, very severe) as described elsewhere (12,13).
Risk factors associated with impaired renal function at baseline (arterial hypertension, diabetes mellitus, age ≥ 65 y (11), prior platinum-based chemotherapy) were recorded. Hypertension was defined as the use of antihypertensive drugs (thiazide drugs, β-blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, or calcium channel blockers). Diabetes mellitus was defined as a hemoglobin A1c of at least 6% or the use of antidiabetic medication (insulin or insulin sensitizers).
Statistical Analyses
Data analyses were conducted using SPSS 26 (IBM). Descriptive statistics were used to illustrate patient characteristics. Mean values and SD or median and interquartile range (IQR) were reported, unless indicated otherwise.
A multiple linear regression analysis was computed to determine the association of number of risk factors at baseline, number of prior treatment lines, and number of cycles of 177Lu-PSMA I&T with the percentage eGFR change 12 mo from initiation of 177Lu-PSMA I&T RLT. P values of less than 0.05 were considered statistically significant (2-sided test).
RESULTS
Patient Characteristics
Supplemental Figure 2 illustrates the recruitment flowchart. A total of 106 mCRPC patients fulfilled the inclusion criteria and underwent a total of 670 cycles of 177Lu-PSMA RLT. The median number of cycles was 6 (IQR, 5–8), and the median interval between 2 cycles was approximately 6 wk. The median administered activity per cycle and total administered activity of 177Lu-PSMA were 7.4 GBq (IQR, 6.0–7.8 GBq) and 44 GBq (IQR, 35–58 GBq), respectively. Patient characteristics are reported in Table 1.
Patient Characteristics (n = 106)
EGFR May Progressively Deteriorate After Initiation of 177Lu-PSMA
Mean baseline eGFR was 79 mL/min (SD, 17 mL/min). The median overall percentage eGFR decrease after 3, 6, and 12 mo from baseline was 3.5% (IQR, 0.9%–7.9%), 6.9% (IQR, 1.8%–15%), and 13.6% (IQR, 3.6%–28.5%), respectively. Of note, the exploratory analysis of the 20 and 5 patients with follow-up at 24 and 36 mo, respectively, after treatment initiation showed a further decline in eGFR from baseline: the median overall percentage eGFR decrease was 19.6% (IQR, 7.6%–30.6%) and 38.9% (IQR, 28.0%–54.4%) at 24 and 36 mo, respectively. Sequential percentage changes in eGFR from baseline within 12 mo and beyond are shown in Figure 1.

Box plots illustrating percentage eGFR decrease from baseline after initiation of 177Lu-PSMA. × within box plots = mean.
Individual percentage changes in eGFR from baseline for all patients with at least a 3% and less than a 3% eGFR decline at 3 mo are shown in Figure 2. In all patients with an early (≥3%) eGFR decline at 3 mo, eGFR decreased progressively without any trend toward stabilization or recovery throughout the observation period. The age-associated yearly eGFR decline of 1 mL/min for a 70-y-old man without comorbidities serves as a comparator (14).

Individual percentage changes in eGFR from baseline in 58 patients with ≥3% eGFR decline at 3 mo (left) and 48 patients with <3% or no eGFR decline at 3 mo (right) after 177Lu-PSMA RLT. Dashed line indicates expected age-associated yearly eGFR decline of 1 mL/min for 70-y-old-man without comorbidities, assuming baseline GFR of 85 mL/min. Thus, after 3 y, eGFR would have declined by 3% from baseline in this healthy man.
By predefined cutoffs, 1 y after initiation of 177Lu-PSMA I&T, 45% (48/106) of patients experienced an eGFR decrease of at least 15% from baseline (Table 2). More than half of those (52%, 25/48) had at least a severe eGFR decrease (≥30%), corresponding to nearly one quarter of the entire patient cohort (24%, 25/106). In all patients with an eGFR decrease of at least 15% after 12 mo and with an additional follow-up visit, eGFR further decreased at 24 mo (eGFR decline of 28%–77% compared with baseline in 7 patients). In 46% (6/13) of the patients with no or only a mild eGFR decrease (<15%) at 12 mo and an additional follow-up visit, eGFR decreased beyond the 15% cutoff at 24 mo. Quantitatively, the mild eGFR decrease observed at 12 mo nearly doubled at the 24-mo follow-up in those patients. Of 5 patients with a 3-y follow-up, 2 had a moderate eGFR decrease, 1 a severe decrease (30%–40%), and 2 a very severe eGFR decrease by at least 40% from baseline. By chronic kidney disease criteria, the proportion of patients with stage 3 renal failure nearly doubled 12 mo after initiation of 177Lu-PSMA compared with baseline (20% vs. 37%, Table 3).
Proportion of Patients with eGFR Decreases by ≥15% 1 Year After Initiation of 177Lu-PSMA
Distribution of Renal Failure Stages at Baseline and 1 Year After Initiation of 177Lu-PSMA (n = 106)
On the basis of the calculated multivariable linear regression model (enter method, which is commonly set as the default in many statistical programs and involves entering all input variables simultaneously), including number of risk factors at baseline, number of pretreatment lines, and number of cycles of 177Lu-PSMA, only a higher number of risk factors at baseline (−4.51, P = 0.03) was associated with higher percentage eGFR decreases from baseline 12 mo after initiation of treatment (Table 4).
Multivariable Linear Regression Model for Association of Risk Factors, Pretreatment Lines, and 177Lu-PSMA Cycles Received by 12 Months with Percentage Decrease in eGFR 12 Months from Initiation of 177Lu-PSMA
DISCUSSION
In our retrospective analysis, an at least moderate eGFR decline (>15%) 12 mo after treatment initiation was observed in 45% (48/106) of patients undergoing 4 or more cycles of 177Lu-PSMA RLT. A severe eGFR decline (≥30%) was present in 24% (25/106) of all patients. An exploratory analysis in a subset of patients with longer follow-up indicated a further eGFR decline over time. A higher number of risk factors at baseline was associated with a higher percentage eGFR decrease at 12 mo.
Previous dosimetry analyses indicate dose-dependent and substantial irradiation of the kidneys during 177Lu-PSMA RLT, potentially leading to radiation nephropathy when referring to dose limits that were established for EBRT (6). Data on the nephrotoxicity of 177Lu-PSMA are sparse, and most studies suggest negligible nephrotoxicity but are limited by a short follow-up and no available dosimetry (2,15). We have recently reported 3 cases of severe radiation nephropathy after extensive treatment with 177Lu-PSMA RLT (4). Long-term data on the effects of 177Lu-PSMA on renal function are urgently needed, especially given its evaluation in early mCRPC (e.g., PSMAfore, SPLASH) and even high-risk localized prostate cancer (e.g., LuTectomy) as well as hormone-sensitive prostate cancer (e.g., PSMAddition, UpFrontPSMA). With a longer life expectancy, those patients could potentially experience renal failure, which is often delayed in radionuclide treatment.
In our retrospective analysis, only a mild and clinically insignificant decrease in eGFR (median, −6.9% from baseline) was observed up to 6 mo after treatment initiation. A previous study reported a mean absolute decrease of 11 mL/min in creatinine clearance based on 51Cr-ethylenediaminetetraacetic acid measurement at 3 mo after 177Lu-PSMA RLT (16). In contrast, our study revealed a comparatively smaller eGFR decline of 3 mL/min based on calculation from creatinine levels after the same treatment duration. However, median eGFR further deteriorated and almost doubled within the next 6 mo, suggesting that renal injury may occur both early and late. At the 12-mo follow-up, 45% (48/106) of patients had an at least moderate (≥15%) decrease in eGFR from baseline: of those, 25% (12/48) showed a severe (≥30%) and 27% (13/48) a very severe (≥40%) eGFR decrease. According to chronic kidney disease criteria, there was a nearly 2-fold increase in the percentage of patients experiencing stage 3 renal failure 12 mo after commencing 177Lu-PSMA therapy as compared with the baseline assessment. Although the analysis at later time points is limited by the small number of patients, there was no indication that the annual eGFR decline slowed after 2 and 3 y. We observed that all patients with at least a 3% eGFR decline at 3 mo after treatment initiation further declined at a relatively constant rate of 3% every 3 mo. This rate is substantially higher than the expected age-associated yearly eGFR decline of 1 mL/min for a 70-y-old man without comorbidities (Fig. 2) (14). Substantial limitations of this observation are variable baseline eGFR and variable comorbidities in our patient cohort.
Hypothetically extrapolating these estimated eGFR declines of 3% every 3 mo would lead to a 50% reduction in baseline clearance and result in a substantial kidney function loss approximately 5 y after treatment initiation. This loss could be of particular importance with the potential adoption of 177Lu-PSMA in earlier-treatment algorithms: although patients with short overall survival in later stages of the disease may not experience long-term negative effects of radiation nephropathy, the use of 177Lu-PSMA in early mCRPC or even metastatic hormone-sensitive PC could potentially result in significant morbidity for these patients. Ongoing trials on metastatic hormone-sensitive or localized prostate cancer are assessing the safety and efficacy of up to 2 cycles of 177Lu-PSMA (17,18). These findings are eagerly awaited; however, existing literature focuses primarily on nephrotoxicity in advanced mCRPC, involving significantly more treatment cycles on average. This disparity in regimens and patient groups suggests a potential underestimation of dose-related nephrotoxicity in these earlier-stage trials and further emphasizes the importance of enhancing our understanding of kidney-related effects associated with 177Lu-PSMA.
In the small subgroup of patients with longer follow-up, a moderate eGFR decrease occurred in half the patients (6/13) at 24 mo who had shown no or only mild eGFR decreases (<15%) at the 12-mo follow-up. This result highlights that radiation-mediated loss of renal function can occur at a delayed time even if no clinically significant eGFR changes are present at 12 mo. Similar to peptide receptor radionuclide therapy using somatostatin analogs for treatment of neuroendocrine tumors (19), our experience emphasizes that a long-term follow-up is pivotal when aiming to investigate radiation damage due to low-dose β− radiation. One study examining the clinical course of radiation nephropathy after EBRT found that clinical signs of glomerular pathology may not appear until after an initial 6-mo latency period (20,21). Often, it may manifest as chronic radiation nephropathy occurring more than 18 mo after exposure to critical radiation doses (20,21).
The nephrotoxicity seen in our cohort might partly also be attributed to the higher number of cycles per patient (and therefore the applied dose) than in other reports. We specifically focused on patients with at least 4 cycles, resulting in a 177Lu-PSMA median number of 6 cycles in our analysis. When data from the literature are used, this translates to an estimated median renal absorbed dose of 31 Gy, but individually a broad variation in renal doses has been observed (6). Yordanova et al. observed no relevant nephrotoxicity at a median renal absorbed dose of 16.4 Gy (15). In contrast, most of our patients substantially exceeded critical estimated renal radiation doses based on EBRT-based dose limits (23 and 28 Gy (6)). On multivariable linear regression, however, the number of treatment cycles was not associated with a greater percentage eGFR decrease from baseline at 12 mo after treatment. In an exploratory analysis, we stratified our cohort by patients undergoing fewer than 6 cycles versus 6 or more cycles, as the latter would result in a median absorbed dose of 31 Gy to the kidneys, exceeding both limits. We observed a higher percentage eGFR decrease from baseline in this group, although not statistically significant. Future studies could benefit from incorporating comprehensive dosimetry data: dosimetry assessment could help elucidate the potentially crucial relationship between absorbed radiation doses to the kidneys and renal function decline and could investigate a potential dose–response relationship that might not have been apparent in our current retrospective analysis due to sample size limitations.
Of interest, the number of risk factors at baseline (diabetes, hypertension, age ≥ 65, or previous platinum chemotherapy) was significantly associated with a greater percentage eGFR decrease from baseline at the 12-mo follow-up. Withholding a potentially effective therapy with a clear survival benefit over preservation of renal function is clearly not an option, especially since it is rather unlikely that any of the treated patients will reach end-stage renal failure with their limited life expectancy. However, accompanying the treatment with best supportive care involving all disciplines and especially nephrologists is key for managing any significant GFR loss and kidney disease–associated comorbidities (e.g., renal anemia and secondary hyperparathyroidism).
Our study had several limitations. First, we selected only patients who received at least 4 cycles of PSMA-directed RLT. This may have led to an overestimation of the general incidence of renal impairment. Second, potentially more advanced parameters of renal function were not available in our retrospective analysis (e.g., cystatin C). Third, although we selected only patients with a least 12 mo of follow-up, data on longer follow-up are available in only a few cases mainly because of the short life expectancy of those patients. Our report currently constitutes the largest (to our knowledge) mCRPC cohort (including both patients with normal and impaired renal function at baseline) undergoing 177Lu-PSMA with a minimum follow-up of 12 mo. The short life expectancy in patients with late-stage mCRPC itself is an important risk factor, given that dehydration and lower oral food and liquid intake are reduced in patients with end-stage progressive disease and aggravate renal impairment. By a strict definition of end-stage progressive disease (overall survival < 6 mo after the 12-mo follow-up and only the best supportive care after 177Lu-PSMA), only 6 of 106 patients fell into this category. Larger studies on earlier-stage patients are warranted to further determine the role and impact of different risk factors regarding 177Lu-PSMA RLT. Finally, we cannot assess to what extent the decrease in renal function over time was caused by use of 177Lu-PSMA or by comorbidities, further complications of prostate cancer (e.g., postrenal obstruction and infections), or late effects of other therapies. Nevertheless, the association between established baseline risk factors and a more significant decline in renal function highlights the need for interdisciplinary consensus, which should consider current risk factors when recommending 177Lu-PSMA treatment. A further limitation is the lack of a control group with 177Lu-PSMA exposure, as potentially confounding factors could have contributed to the loss of kidney function (e.g., advanced disease stage). Nevertheless, the observed eGFR decreases at 12 mo in a cohort with non–end-stage progressive disease suggest at least some contribution of 177Lu-PSMA RLT and warrants further evaluation. Another limitation is the use of a monoexponential function to determine the kidney function at a defined time. The method is generally reliable with multiple time points and is accepted for approximations in the literature but is not as accurate as true measurements at a given time.
CONCLUSION
Our data indicate that in most mCRPC patients undergoing at least 4 cycles of 177Lu-PSMA, renal toxicity is moderate, with mild eGFR decreases up to 12 mo after treatment initiation. However, an at least severe decline in eGFR from baseline occurred in nearly a quarter of the entire cohort, and a further eGFR deterioration was observed in a substantial proportion of patients with longer follow-up. Thus, the results of further prospective trials with follow-up of more than 12 mo are urgently awaited to determine the risk of delayed nephrotoxicity after 177Lu-PSMA RLT in relation to other available treatments. Until such data are available, off-label use of 177Lu-PSMA RLT in patients with an expected life expectancy of more than 2 y should occur only after a careful evaluation of the benefits relative to the risks of progressive and potentially severe renal failure.
DISCLOSURE
Matthias Eiber reports fees from Blue Earth Diagnostics Ltd. (consultant, research funding), Novartis/AAA (consultant, speaker), Telix (consultant), Bayer (consultant, research funding), RayzeBio (consultant), Point Biopharma (consultant), Eckert-Ziegler (speaker), Janssen Pharmaceuticals (consultant, speakers’ bureau), Parexel (image review), and Bioclinica (image review) outside the submitted work and a patent application for radiohybrid PSMA. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What effect does 177Lu-PSMA RLT have on renal function in mCRPC patients up to 1 y after the start of treatment?
PERTINENT FINDINGS: In this retrospective multicenter cohort study on 106 mCRPC patients undergoing 177Lu-PSMA RLT, most patients experienced no or mild decreases in renal function within 1 y after treatment initiation. However, about 25% had severe eGFR decreases within 12 mo from treatment initiation. Radiation nephropathy appeared delayed: the 12-mo eGFR further deteriorated in patients with longer follow-up.
IMPLICATIONS FOR PATIENT CARE: 177Lu-PSMA can lead to moderate and even severe decreases in renal function within 1 y from initiation of treatment. Prospective data on renal toxicity and with a longer follow-up are unavailable; the off-label use of 177Lu-PSMA RLT in patients with potentially longer survival should therefore occur only after careful evaluation of the benefits relative to the risks of progressive and potentially severe renal failure.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 19, 2023.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 4, 2023.
- Revision received September 16, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mathematic Modeling of Tumor Growth During [177Lu]Lu-PSMA Therapy: Insights into Treatment Optimization
- Challenges with 177Lu-PSMA-617 Radiopharmaceutical Therapy in Clinical Practice
- Initial Experience with [177Lu]Lu-PSMA-617 After Regulatory Approval for Metastatic Castration-Resistant Prostate Cancer: Efficacy, Safety, and Outcome Prediction
- Safety and Efficacy of Extended Therapy with [177Lu]Lu-PSMA: A German Multicenter Study
- Unraveling the Impact of 177Lu-PSMA Radioligand Therapy on Renal Impairment: Distinguishing Causation from Correlation