


Abstract
Although guidelines such as those of the National Comprehensive Cancer Network consider 18F-FDG PET/CT for systemic staging of newly diagnosed stage III breast cancer patients, factors in addition to stage may influence the utility of PET/CT. Because invasive lobular carcinoma (ILC) is less conspicuous than invasive ductal carcinoma (IDC) on 18F-FDG PET, we hypothesized that tumor histology may be one such factor. We evaluated PET/CT systemic staging of patients newly diagnosed with ILC compared with IDC. Methods: In this Institutional Review Board–approved retrospective study, our Hospital Information System was screened for ILC patients who underwent PET/CT in 2006–2013 before systemic or radiation therapy. Initial stage was determined from examination, mammography, ultrasound, MR, or surgery. PET/CT was performed to identify unsuspected distant metastases. A sequential cohort of stage III IDC patients was evaluated for comparison. Upstaging rates were compared using the Pearson χ2 test. Results: The study criteria were fulfilled by 146 ILC patients. PET/CT revealed unsuspected distant metastases in 12 (8%): 0 of 8 with initial stage I, 2 of 50 (4%) stage II, and 10 of 88 (11%) stage III. Upstaging to IV by PET/CT was confirmed by biopsy in all cases. Three of 12 upstaged patients were upstaged only by the CT component of the PET/CT, as the metastases were not 18F-FDG–avid. In the comparison stage III IDC cohort, 22% (20/89) of patients were upstaged to IV by PET/CT. All 20 demonstrated 18F-FDG–avid metastases. The relative risk of PET/CT revealing unsuspected distant metastases in stage III IDC patients was 1.98 times (95% confidence interval, 0.98–3.98) that of stage III ILC patients (P = 0.049). For 18F-FDG–avid metastases, the relative risk of PET/CT revealing unsuspected 18F-FDG–avid distant metastases in stage III IDC patients was 2.82 times (95% confidence interval, 1.26–6.34) that of stage III ILC patients (P = 0.007). Conclusion: 18F-FDG PET/CT was more likely to reveal unsuspected distant metastases in stage III IDC patients than in stage III ILC patients. In addition, some ILC patients were upstaged by non–18F-FDG-avid lesions visible only on the CT images. Overall, the impact of PET/CT on systemic staging may be lower for ILC patients than for IDC patients.
The 2014 National Comprehensive Cancer Network guidelines consider using 18F-FDG PET/CT for systemic staging of patients with newly diagnosed stage III breast cancer, as the detection of distant metastases in these patients would alter treatment and prognosis (1). However, additional factors besides initial clinical stage may be important when determining whether a staging PET/CT study is clinically indicated. For example, patient age has been advanced as a potentially important clinical factor, as younger patients with breast cancer may have more aggressive disease that is more easily detected by 18F-FDG PET/CT at earlier stages (2).
Another potential factor for determining whether staging PET/CT may be of value is the histologic subtype of the primary breast malignancy. The most common histologies of breast cancer are infiltrating ductal carcinoma (IDC), which accounts for about 75%–80% of primary breast malignancies, and infiltrating lobular carcinoma (ILC), which accounts for about 10%–15% of primary breast malignancies (3,4). Although both are primary breast malignancies, IDC and ILC have distinct epidemiologic, molecular, pathologic, and imaging features (5–17). ILC is more difficult than IDC to detect on imaging, including mammography, ultrasound, and MR imaging (7,8). Primary ILC is less appreciable than comparable IDC tumors on 18F-FDG PET and demonstrates lower standardized uptake values (9–12). Metastases from ILC may also be less appreciable than comparable IDC tumors on 18F-FDG PET (17). In addition, ILC differs from IDC in its patterns of metastatic spread (13–16). Although both IDC and ILC commonly metastasize to lymph nodes, bone, and liver, ILC demonstrates a predilection for metastases to the peritoneum, retroperitoneum, hollow viscera (including the gastrointestinal and genitourinary tracts), and leptomeninges (13–16). Not only do these sites of metastatic disease often remain clinically silent until extensive, but they also may be more difficult to assess on PET/CT. Lung metastases, which may be easier to assess on the CT component of PET/CT, are more common in IDC. Given the differences in 18F-FDG avidity and patterns of metastatic spread of ILC, 18F-FDG PET/CT may be less suited for evaluation of ILC than IDC. We therefore evaluated the utility of 18F-FDG PET/CT for the systemic staging of patients with newly diagnosed stage I–III ILC.
MATERIALS AND METHODS
Study Design and Patients
This retrospective single-institution study was performed in compliance with the Health Insurance Portability and Accountability Act and with Institutional Review Board approval. The requirement to obtain informed consent was waived. The Memorial Sloan Kettering Cancer Center Hospital Information System was screened for patients with stage I–IIIC ILC who underwent 18F-FDG PET/CT between January 2006 and December 2013 before beginning treatment with chemotherapy, hormonal therapy, or radiation. Electronic medical records were reviewed, and patients with the following characteristics were excluded: known stage IV disease for the current malignancy before PET/CT, prior or concurrent malignancies (except nonmelanoma skin cancer), systemic therapy or radiation before PET/CT, or the male sex. Surgical management of the primary breast lesion and axillary nodes was allowed. Age at diagnosis and race were recorded for each patient.
To compare staging PET/CT results from ILC patients to patients with the more common diagnosis of IDC, a comparison cohort of IDC patients was selected sequentially during the same period. IDC patients also underwent 18F-FDG PET/CT before beginning treatment with systemic therapy or radiation. The exclusion criteria remained the same, including known stage IV disease for the current malignancy before PET/CT; prior or concurrent malignancies (except nonmelanoma skin cancer); and chemotherapy, hormonal therapy, or radiation before PET/CT. To provide an appropriate comparison with the stage III ILC patients, the IDC cohort included only patients with initial stage III disease. In addition, to allow comparison of 18F-FDG PET and 99mTc-methylene diphosphonate (99mTc-MDP) bone scan findings in the IDC cohort, only patients who had undergone both 18F-FDG PET/CT and bone scanning before treatment were included. Because IDC is much more common than ILC, the additional criterion of a pretreatment bone scan did not prevent identification of an appropriately sized comparison cohort.
Determination of Initial Stage
Initial stage was determined according to the AJCC Cancer Staging Manual (18). Initial clinical stage was determined from physical examination, mammography, breast ultrasound, and, if available, breast MR imaging or surgical findings.
PET/CT Imaging and Interpretation
All patients in this retrospective study underwent staging 18F-FDG PET/CT. Before 18F-FDG injection for PET/CT, the patients fasted for at least 6 h. Each patient was injected intravenously with 444–555 MBq (12–15 mCi) of 18F-FDG when the plasma glucose level was less than 200 mg/dL. After 18F-FDG injection, the patients rested for a scheduled 60-min uptake period followed by image acquisition. PET/CT scans were acquired from the base of the skull to the mid thigh with the patient supine. In most cases, low-dose CT scans with oral contrast material were obtained. Occasionally, intravenous contrast material was administered. In all cases, attenuation-corrected images were reviewed on a PACS (GE Healthcare) displaying a maximum-intensity-projection image and multiplanar PET, CT, and PET/CT fusion images. According to standard 18F-FDG PET/CT reporting, uptake was considered abnormal when it was focal, not considered physiologic or inflammatory, and of an intensity greater than the local background. Suspicion of malignancy was based on the integration of metabolic information from the PET images and anatomic information from the CT images. PET/CT studies were reinterpreted by a radiologist board-certified in diagnostic radiology and nuclear medicine with 9 y of PET/CT experience, who was not shown the original PET/CT report or the results of other imaging modalities. Unsuspected local extraaxillary nodal metastases (internal mammary or supraclavicular) and distant metastases were recorded. If unsuspected local extraaxillary nodal metastases or distant metastases were noted on imaging, a new stage was assigned.
Bone Scanning and Interpretation
All patients in the IDC comparison cohort underwent a pretreatment bone scan. The 99mTc-MDP bone scans were reinterpreted, and the presence of osseous metastases was recorded. Each patient had been injected intravenously with 740–925 MBq (20–25 mCi) of 99mTc-MDP, followed by a 3-h uptake period and image acquisition. Bone scans were acquired from the skull apex to the toes with the patient supine. Images were reviewed on a PACS workstation displaying anterior and posterior whole-body images as well as spot images of the skull, chest, and pelvis. SPECT images of a body region were obtained as part of 2 bone scans. Uptake was considered abnormal when it was focal, not considered physiologic or inflammatory, and of an intensity greater than that of the local background. Bone scans were reinterpreted by the same radiologist as for the PET/CT interpretation, but at a separate time, and the radiologist was not shown the original bone scan report or the results of other imaging modalities. The presence of osseous metastases was recorded. If osseous metastases were noted, a postimaging stage (stage IV) was assigned.
Verification of Metastases
All patients with newly discovered distant metastases had pathologic verification. For local extraaxillary nodal metastases, pathologic verification was preferred, but if histology was not available follow-up imaging was used. Local extraaxillary nodes had to be suspected on initial imaging and then demonstrate treatment response or progression on follow-up imaging.
Statistical Analysis
Medians and ranges were used to summarize continuous variables and frequencies, and percentages were used to summarize categoric variables, including distant metastases and upstaging to III or IV. Race was categorized as African American, Asian, Caucasian, or other. Receptor profiles were categorized as estrogen receptor–positive/human epidermal growth factor 2–negative (ER+/HER2−), HER2+, triple-negative, or other/unspecified. The association between histologic subtype and clinical parameter and rate of upstaging was evaluated using the Pearson χ2 test for categoric variables and the Wilcoxon rank sum test for continuous variables. Proportion of upstaging in ILC versus IDC patients was compared using the Pearson χ2 test and calculated the relative risk along with the 95% confidence interval. All analyses were performed using SAS, version 9.4 (SAS Institute).
RESULTS
ILC Cohort
Our search revealed 146 patients who had stage I–III ILC breast cancer, underwent 18F-FDG PET/CT before systemic therapy or radiation between 2006 and 2013, and met all eligibility criteria. The median age of the ILC cohort was 57 y (range, 34–92 y). Before PET/CT imaging, 8 patients (6%) were stage I, 50 (34%) were stage II, and 88 (60%) were stage III. Details on patient and tumor characteristics are summarized in Table 1.
Characteristics of Patients and Tumors
Comparison IDC Cohort
To compare the staging PET/CT results from stage III ILC patients to patients with the more common diagnosis of IDC, we selected a comparison cohort of IDC patients with initial stage III disease. To allow further comparison of systemic staging of stage III IDC patients with 18F-FDG PET/CT versus CT and bone scanning, only patients who had undergone both pretreatment 18F-FDG PET/CT and bone scanning were included. Our search revealed 89 patients with stage III IDC breast cancer for this comparison cohort. The median age of the IDC cohort was 59 y (range, 33–90 y). All patients in the IDC cohort were stage III by the inclusion criteria. Details on patient and tumor characteristics are summarized in Table 1.
Associations Between Clinical Parameters and Histologic Subtype
Receptor status was found to differ between the cohorts (P < 0.0001). Nearly all the ILC patients were ER+/HER2− (90.4%), compared with only about half (51.7%) the IDC patients. Additionally, 21.3% of IDC patients were HER2+ compared with 5.5% of ILC, and 25.8% of IDC were triple-negative compared with 3.4% of ILC. The differences in receptor status were expected, given multiinstitutional historic data demonstrating differences in receptor status between IDC and ILC (19). Race was found to approach significance between ILC and IDC patients (P = 0.06). The majority in both cohorts were Caucasian (88.4% vs. 77.5%, respectively); however, 14.6% (13/89) of the IDC patients were African American, as opposed to only 6.2% (9/146) of ILC patients. Additionally, 6.7% (6/89) of IDC patients were Asian, as opposed to only 5.5% (8/146) of ILC patients. The differences in race may also have been expected, given multiinstitutional data demonstrating lower rates of ILC in African American patients (19).
Upstaging by PET/CT in the ILC Cohort
PET/CT did not reveal unsuspected local extraaxillary nodes in any of the 146 ILC patients. Thirteen (9%) of 146 patients demonstrated abnormalities suggestive of distant metastases on PET/CT. In 12 of 13 patients, histology confirmed metastatic disease, including 10 patients with osseous metastases (Figs. 1 and 2), 2 with distal nodal metastases (Fig. 3), and 1 with hepatic metastases. One patient had both osseous and nodal distant metastases. In one patient, an 18F-FDG–avid (SUV, 2.9) 2.1-cm adrenal nodule with average Hounsfield units of 29 led to a biopsy demonstrating an adrenal adenoma. This lesion was stable on follow-up imaging and classified as benign and was thus deemed to be false-positive for malignancy (Fig. 4). After excluding this false-positive, 12 (8%) of 146 ILC patients had distant metastases demonstrated by 18F-FDG PET/CT. Classified by initial stage, PET/CT revealed unsuspected distant metastases in 0 of 8 (0%) ILC patients with stage I, 2 of 50 (4%) with stage II, and 10 of 88 (11%) with stage III.

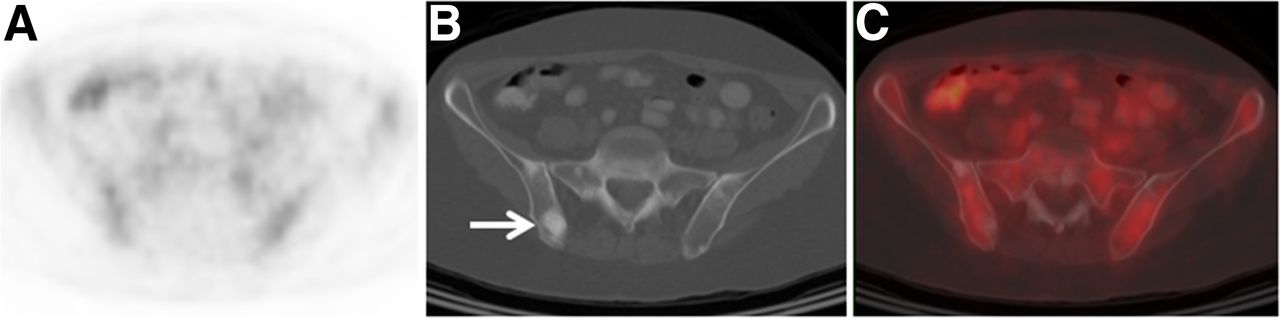
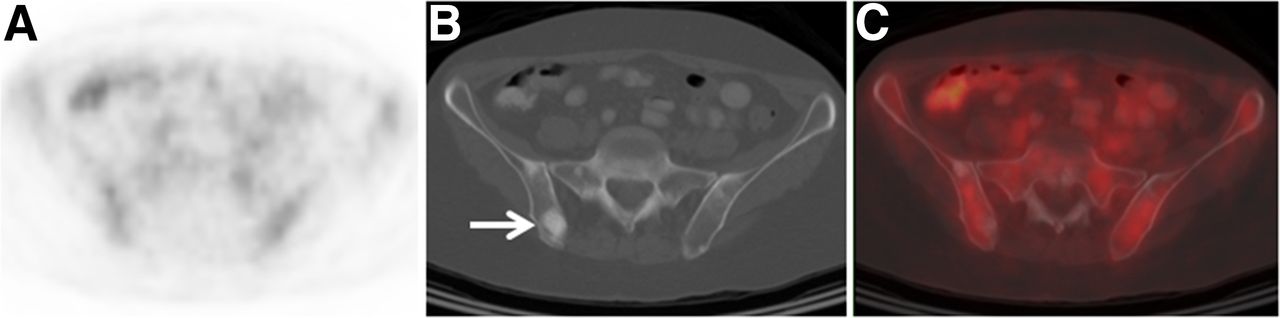
A 62-y-old woman with initial stage III ILC upstaged to IV by 18F-FDG PET and CT. (A) Axial fused 18F-FDG PET/CT image demonstrates previously unknown right humeral head metastases as 18F-FDG–avid osseous lesion (arrow). (B) Metastatic lesion is apparent as sclerotic osseous lesion on CT (arrow). Biopsy confirmed osseous metastasis.
A 56-y-old woman with initial stage III ILC upstaged to IV on CT component of 18F-FDG PET/CT. (A) Axial 18F-FDG PET does not demonstrate suggestive foci. (B) Axial CT component of PET/CT demonstrates multiple osseous sclerotic lesions suggestive of metastases (arrow). (C) Axial fused 18F-FDG PET/CT image confirms that osseous sclerotic lesions demonstrate background 18F-FDG avidity. Biopsy confirmed osseous metastasis.
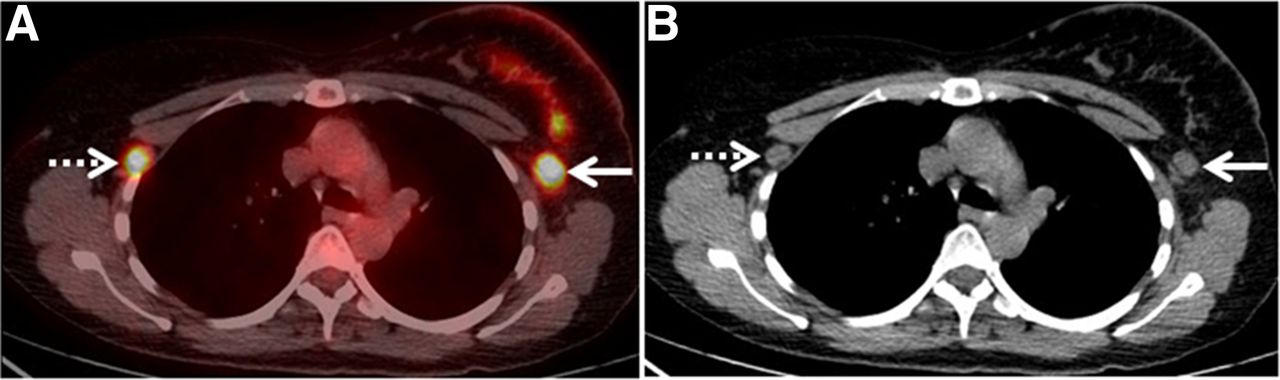
A 52-y-old woman with initial stage III left breast ILC upstaged to IV by 18F-FDG PET and CT. (A) Axial fused 18F-FDG PET/CT image demonstrates previously known ipsilateral left axillary nodal metastasis as 18F-FDG–avid lesion (solid arrow), as well as previously unknown contralateral right axillary node (dashed arrow). (B) Both ipsilateral and contralateral axillary nodal lesions are apparent as enlarged and rounded nodes on CT. Biopsy of contralateral right axillary node demonstrated nodal metastasis. Contralateral axillary nodal metastases are distant metastases (M1 disease) as classified by American Joint Committee on Cancer (18).

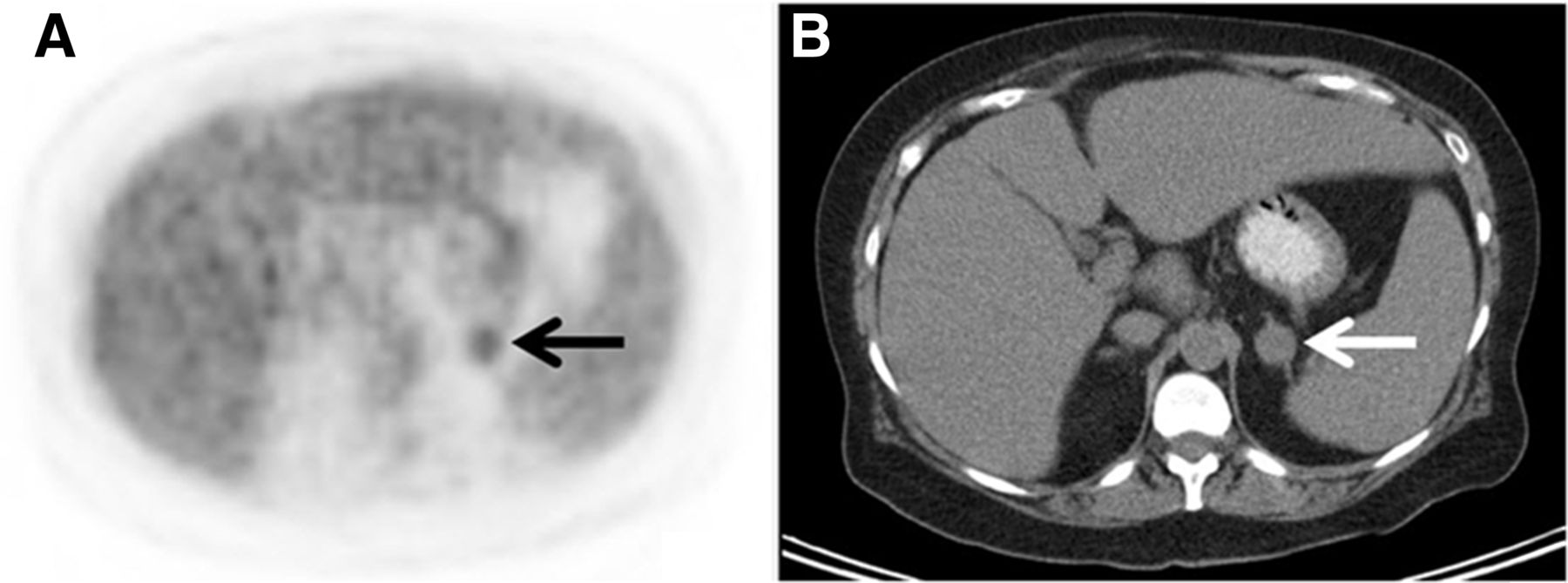
A 64-y-old woman with initial stage III ILC false-positive for distant metastasis on 18F-FDG PET/CT. (A) Axial 18F-FDG PET demonstrates 18F-FDG–avid (SUV, 2.9) focus in left abdomen (arrow). (B) Axial CT component of PET/CT demonstrates 2.1-cm adrenal nodule with average Hounsfield units of 29 (arrow). Biopsy resulted in diagnosis of benign adrenal adenoma.
Of the 12 ILC patients for whom PET/CT led to the discovery of stage IV disease, 9 (75%) demonstrated 18F-FDG–avid metastases. The remaining 3 patients (25%) were upstaged only by the CT component of the PET/CT study, as they had sclerotic osseous lesions that demonstrated only background 18F-FDG avidity (Fig. 2). All 3 with non–18F-FDG-avid metastases upstaged by the CT component of the PET/CT study were initially stage III ILC patients.
In one patient in the ILC cohort, an unsuspected synchronous malignancy was discovered, a non–small cell lung cancer, which was proven on biopsy.
Upstaging by PET/CT in the IDC Cohort
In the stage III IDC cohort, PET/CT demonstrated unsuspected local extraaxillary nodes in 7 (8%) of 89 patients, including internal mammary and supraclavicular nodal lesions. A total of 22 (25%) of 89 patients demonstrated abnormalities suggestive of distant metastases. In 20 of 22 of these patients, histology confirmed metastatic disease, including 17 patients with osseous metastases (Fig. 5), 3 with distant nodal metastases, 2 with hepatic metastases, 2 with lung metastases, and 1 with pleural metastases. Five patients had more than 1 site of distant metastases. In 1 patient, an 18F-FDG–avid hepatic focus without a CT correlate led to an MR study of the liver demonstrating out-of-phase signal loss and a diagnosis of probable hepatic adenoma. This lesion was stable on follow-up imaging, was never biopsied, and was presumed to be benign. In 1 other patient, a non–18F-FDG-avid T1 vertebral osseous sclerotic lesion underwent biopsy and had a benign histology. The osseous lesion remained stable on follow-up imaging, was classified as benign, and was thus deemed false-positive for malignancy (Fig. 6).
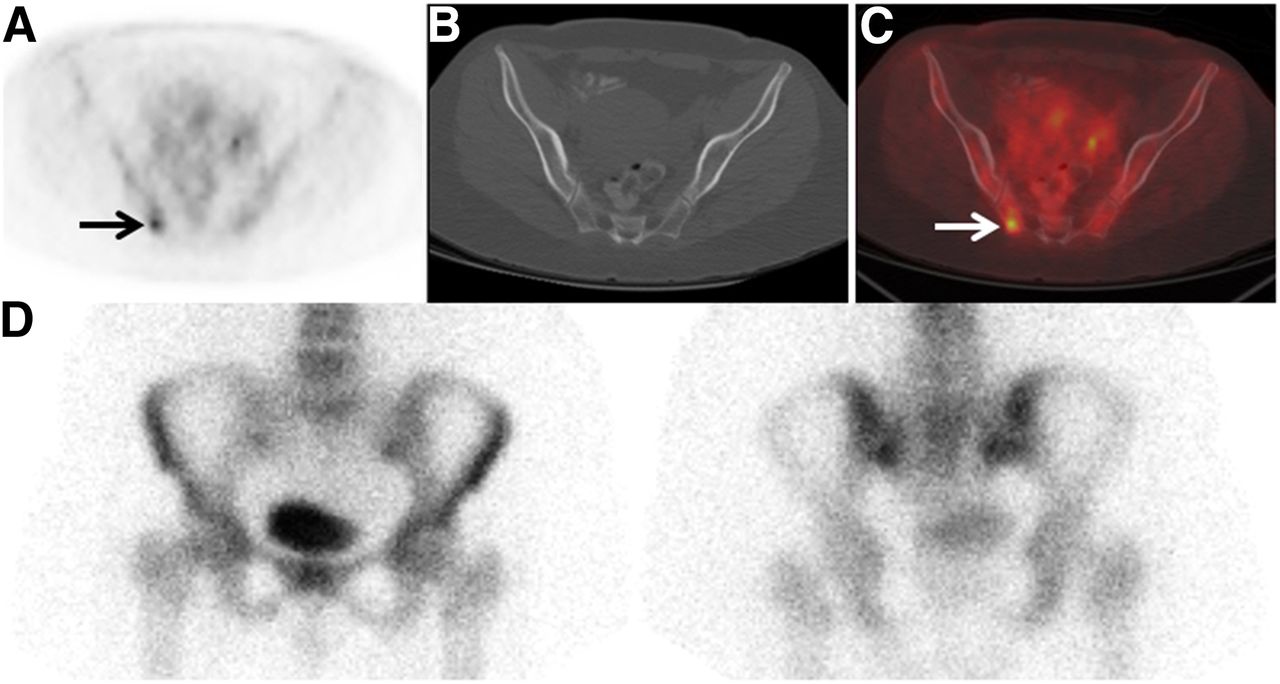
A 42-y-old woman with initial stage III IDC upstaged to IV by 18F-FDG PET. (A) Axial fused 18F-FDG PET/CT image demonstrates previously unknown right ilium metastases as 18F-FDG–avid osseous lesion (arrow). (B) No definite corresponding lesion is seen on axial CT component of PET/CT. (C) Axial fused 18F-FDG PET/CT image confirms osseous localization of 18F-FDG–avid focus (arrow). (D) No corresponding focus is seen on 99mTc-MDP bone scan (anterior [left] and posterior [right] spot views of pelvis shown). Biopsy confirmed osseous metastasis.
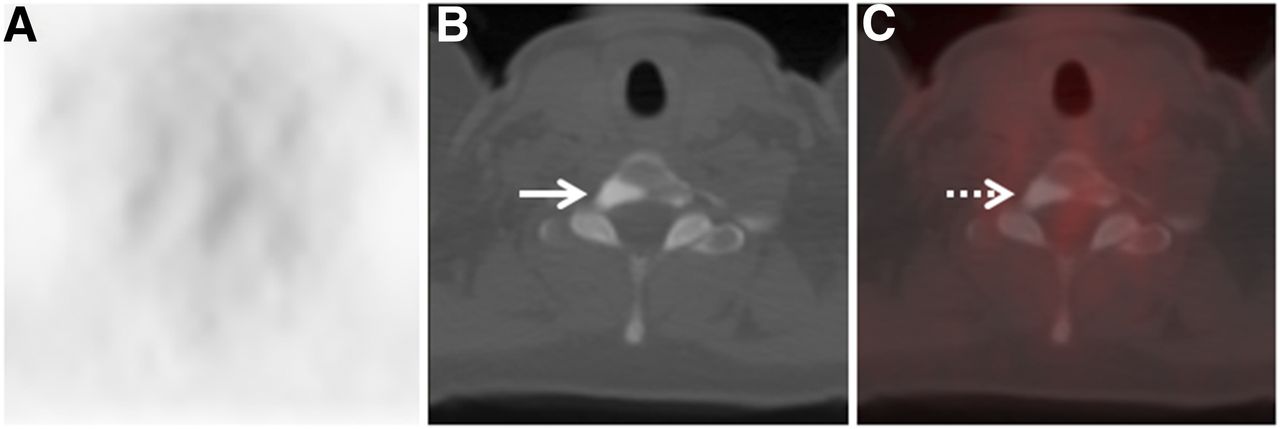
A 46-y-old woman with initial stage III IDC false-positive for distant metastasis on CT component of 18F-FDG PET/CT. (A) Axial 18F-FDG PET does not demonstrate suggestive foci. (B) Axial CT component of PET/CT demonstrates osseous sclerotic lesion (arrow) in T1 vertebra. (C) Axial fused 18F-FDG PET/CT image confirms that osseous sclerotic lesion (arrow) demonstrates background 18F-FDG avidity. Biopsy of sclerotic lesion yielded dense cortical bone without evidence of malignancy, consistent with bone island.
Of the stage III IDC patients in whom PET/CT led to the discovery of stage IV disease, all 20 (100%) demonstrated 18F-FDG–avid metastases. No IDC patients were upstaged only by the CT component of the PET/CT study. In addition to the identification of distant metastases in 20 patients based on 18F-FDG avidity on PET, 11 (55%) of 20 had findings suggestive of malignancy both on the CT component of the PET/CT and on the bone scan, 2 (10%) had suggestive findings on the CT component of the PET/CT study but not on the bone scan, and 1 (5%) had suggestive findings on the bone scan but not on the CT component of the PET/CT study. Thus, of 20 stage III IDC patients who were upstaged because of the detection of 18F-FDG–avid metastases on PET, 6 (30%) had no evidence of metastases on either the CT component of the PET/CT study or the bone scan. Of these 6, 4 had 18F-FDG–avid osseous metastases without a corresponding lesion on either the CT scan or the bone scan (Fig. 5), and 2 had 18F-FDG–avid subcentimeter-sized distant nodal metastases.
Comparison of Upstaging by PET/CT in the ILC and IDC Cohorts
The relative risk of PET/CT revealing unsuspected distant metastases in stage III IDC patients (20 of 89) was 1.98 times (95% confidence interval, 0.98–3.98) that in stage III ILC patients (10 of 88, P = 0.049). When the analysis was limited to 18F-FDG–avid metastases, the relative risk of PET/CT revealing unsuspected 18F-FDG–avid distant metastases in stage III IDC patients (20 of 89) was 2.82 times (95% confidence interval, 1.26–6.34) that of stage III ILC patients (7 of 88, P = 0.007).
With respect to clinical characteristics, no differences were found between the upstaged and nonupstaged patient cohorts in terms of race, age, or receptor status in the ILC cohort (P = 1.00, 0.35, and 0.60, respectively) or the IDC cohort (P = 0.85, 0.08, and 0.94, respectively).
DISCUSSION
The systemic staging of locally advanced breast cancer is important, as the detection of distant metastases will generally alter patient management from neoadjuvant and surgical for stage II or III disease and to palliative systemic for stage IV disease. Although 18F-FDG PET/CT has proven to be valuable for systemic staging in patients with breast cancer, it is important to define patient and tumor characteristics that affect 18F-FDG PET/CT performance. Tumor histology may be one such important tumor characteristic, since ILC has distinct epidemiologic and imaging features compared with the more common IDC (5–17).
Our data suggest that for systemic staging, 18F-FDG PET/CT has a lower utility for patients with stage III ILC than for patients with stage III IDC. PET/CT revealed stage IV—distant metastatic—disease in 20 (22%) of 89 patients with stage III IDC before PET/CT, a percentage that correlates well with prior published studies (2,20,21). In comparison, PET/CT revealed stage IV disease in only 10 (11%) of 88 patients with stage III ILC before PET/CT, a histologic subtype on which there are few published data. Furthermore, all 20 stage III IDC patients upstaged to IV by PET/CT demonstrated 18F-FDG–avid distant metastases, as opposed to only 7 of 10 stage III ILC patients, with the remaining 3 being upstaged by CT findings that were not 18F-FDG–avid. Overall, the rate of detecting unsuspected 18F-FDG–avid distant metastases, and thus stage IV disease, in patients with initial stage III ILC was lower than that in patients with initial stage III IDC (P = 0.007).
Our data confirm that 18F-FDG PET has utility for the detection of unsuspected 18F-FDG–avid distant metastases in stage III IDC patients. In addition to PET/CT detecting unsuspected distant metastases in 20 (22%) of 89 patients with stage III IDC, 6 (30%) of the 20 were upstaged by the 18F-FDG PET component of the PET/CT study, without corresponding suggestive findings on CT or bone scanning. Our data support prior work suggesting that 18F-FDG PET/CT may replace CT and bone scanning for some forms of breast cancer (22,23) and extends prior work by suggesting that this replacement may be favorable in patients with IDC but not necessarily in those with ILC.
Most instances in which metastases were suspected in initial-stage III IDC patients on 18F-FDG PET/CT but not on bone scanning or CT alone were due to detection of unsuspected osseous metastases. 99mTc-MDP is a radiotracer that accumulates at sites of osteoblastic remodeling; thus, 99mTc-MDP detects the osseous response to tumor rather than the tumor itself (24). Because osteolytic tumors or marrow tumors that do not elicit a sufficient osteoblastic response may result in false-negatives on 99mTc-MDP bone scanning, the sensitivity of bone scanning is variable (62%–100%) (24). 18F-FDG PET offers more direct information about the tumor by measuring tumor metabolism. Hybrid PET/CT, which allows the integration of both metabolic and anatomic information, may enhance detection of osseous metastases compared with 18F-FDG PET alone (20,24). The lower 18F-FDG avidity of ILC tumors and the tendency for ILC osseous metastases to be more sclerotic may help explain why 18F-FDG PET/CT detected more unsuspected metastases than CT or bone scanning alone in IDC but not in ILC.
Although the detection of unsuspected local extraaxillary nodal disease does not have the same impact on patient care as the detection of distant metastases, detection of such nodal disease may still increase the patient’s stage, affect prognosis, and lead to changes in a patient’s treatment plan, such as additional surgery or radiotherapy. Several studies have demonstrated the value of 18F-FDG PET/CT over other imaging modalities for the detection of local extraaxillary nodal disease (2,20,25). As with distant metastases, 18F-FDG PET/CT in this study had a greater yield for the detection of local extraaxillary nodal disease in IDC patients than in ILC patients. No additional local extraaxillary local nodal disease was identified in 88 patients with stage III ILC, whereas such disease was detected in 7 (8%) of 89 patients with stage III IDC.
Our study had several limitations. The retrospective, single-institution design lends itself to selection biases that are difficult to control. For instance, we attempted to provide a cohort of patients with stage III IDC to compare against stage III ILC patients. To allow assessment of 18F-FDG PET/CT versus CT/bone scanning, an inclusion criterion for our comparison IDC cohort was to have both PET/CT and bone scanning results available at baseline. However, the selection of patients who underwent both 18F-FDG PET/CT and 99mTc-MDP bone scanning may have caused a patient selection bias. In this retrospective study, the reasons for a patient having undergone both studies were not identified. We can state that the rate of detection of local extraaxillary and distant metastases for IDC patients in this study is comparable to that of prior breast cancer studies, but this does not negate the intrinsic selection biases. Likewise, the reasons that certain ILC patients were selected to have 18F-FDG PET/CT were not identified in this study. The potential selection biases, which are innate to this retrospective study, make prospective evaluation of these findings important for confirmation.
Although all distant metastases were histologically proven for all patients in both the ILC and the IDC cohorts, suspected local extraaxillary nodal metastases were often not histologically confirmed. When local extraaxillary nodal lesions were found in patients with distant metastases, confirmation of the nodal disease was usually not clinically relevant. Likewise, internal mammary nodes suspected of having metastases are not always confirmed histologically. The lack of histologic verification of nodal disease limits the utility of the local extraaxillary nodal 18F-FDG PET/CT findings.
Fewer breast cancer patients undergo 18F-NaF PET/CT bone scans than 99mTc-MDP bone scans, although the frequency of use of 18F-NaF PET/CT may be increasing. Because of the limited number of patients undergoing 18F-NaF PET/CT at our institution during the time of our study, our study did not evaluate 18F-NaF PET/CT as a method of systemic staging. Relatively little is known yet about the added value of SPECT/CT to 99mTc-MDP bone scanning for the detection of bone metastases in patients with breast cancer (26).
CONCLUSION
This retrospective study suggests that 18F-FDG PET/CT is more likely to reveal unsuspected distant metastases in stage III IDC patients than in stage III ILC patients. In addition, some ILC patients were upstaged only by the CT component of PET/CT because metastases detected on CT were not 18F-FDG–avid. As the impact of PET/CT on systemic staging may be lower for ILC patients than for IDC patients, we recommend that ILC patients be analyzed independently from IDC patients in future studies exploring the utility of 18F-FDG PET/CT. Prospective evaluation of the impact of tumor histology on the utility of 18F-FDG PET/CT for systemic staging of patients with breast cancer is warranted.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. We acknowledge a Susan G. Komen for the Cure research grant (KG110441) and a grant from the MSKCC Biostatistics Core (P30 CA008748). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Jane Howard for patient database assistance.
Footnotes
Published online Aug. 20, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 1, 2015.
- Accepted for publication August 4, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Potential of 68Ga-NeoB PET/CT with Estrogen Receptor- and Progesterone Receptor-Positive Breast Cancer Undergoing Staging or Restaging for Metastatic Disease
- Oncogenic NOVA1 expression dysregulates alternative splicing in breast cancer
- 68Ga-FAP-2286 PET of Solid Tumors: Biodistribution, Dosimetry, and Comparison with 18F-FDG
- 68Ga-FAPI PET/CT as an Alternative to 18F-FDG PET/CT in the Imaging of Invasive Lobular Breast Carcinoma
- WNT4 regulates cellular metabolism via intracellular activity at the mitochondria in breast and gynecologic cancers
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol
- WNT4 executes estrogen regulation of cellular metabolism via intracellular activity at the mitochondria
- Head-to-Head Evaluation of 18F-FES and 18F-FDG PET/CT in Metastatic Invasive Lobular Breast Cancer
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- 18F-FDG PET/CT for Systemic Staging of Newly Diagnosed Breast Cancer in Men
- Expression of Gastrin-Releasing Peptide Receptor in Breast Cancer and Its Association with Pathologic, Biologic, and Clinical Parameters: A Study of 1,432 Primary Tumors
- Prospective Clinical Trial of 18F-Fluciclovine PET/CT for Determining the Response to Neoadjuvant Therapy in Invasive Ductal and Invasive Lobular Breast Cancers
- Initial Results of a Prospective Clinical Trial of 18F-Fluciclovine PET/CT in Newly Diagnosed Invasive Ductal and Invasive Lobular Breast Cancers