


Visual Abstract

Abstract
Invasive lobular carcinoma (ILC) demonstrates lower conspicuity on 18F-FDG PET than the more common invasive ductal carcinoma. Other molecular imaging methods may be needed for evaluation of this malignancy. As ILC is nearly always (95%) estrogen receptor (ER)–positive, ER-targeting PET tracers such as 16α-18F-fluoroestradiol (18F-FES) may have value. We reviewed prospective trials at Memorial Sloan Kettering Cancer Center using 18F-FES PET/CT to evaluate metastatic ILC patients with synchronous 18F-FDG and 18F-FES PET/CT imaging, which allowed a head-to-head comparison of these 2 PET tracers. Methods: Six prospective clinical trials using 18F-FES PET/CT in patients with metastatic breast cancer were performed at Memorial Sloan Kettering Cancer Center from 2008 to 2019. These trials included 92 patients, of whom 14 (15%) were of ILC histology. Seven of 14 patients with ILC had 18F-FDG PET/CT performed within 5 wk of the research 18F-FES PET/CT and no intervening change in management. For these 7 patients, the 18F-FES and 18F-FDG PET/CT studies were analyzed to determine the total number of tracer–avid lesions, organ systems of involvement, and SUVmax of each organ system for both tracers. Results: In the 7 comparable pairs of scans, there were a total of 254 18F-FES–avid lesions (SUVmax, 2.6–17.9) and 111 18F-FDG–avid lesions (SUVmax, 3.3–9.9) suggestive of malignancy. For 5 of 7 (71%) ILC patients, 18F-FES PET/CT detected more metastatic lesions than 18F-FDG PET/CT. In the same 5 of 7 patients, the SUVmax of 18F-FES–avid lesions was greater than the SUVmax of 18F-FDG–avid lesions. One patient had 18F-FES–avid metastases with no corresponding 18F-FDG–avid metastases. There were no patients with 18F-FDG–avid distant metastases without 18F-FES–avid distant metastases, although in one patient liver metastases were evident on 18F-FDG but not on 18F-FES PET. Conclusion: 18F-FES PET/CT compared favorably with 18F-FDG PET/CT for detection of metastases in patients with metastatic ILC. Larger prospective trials of 18F-FES PET/CT in ILC should be considered to evaluate ER-targeted imaging for clinical value in patients with this histology of breast cancer.
PET/CT with 18F-FDG plays an important role in the management of patients with breast cancer (1,2). The impact of 18F-FDG PET/CT in patients with breast cancer differs between the most common histology of breast cancer, invasive ductal carcinoma (80% of cases) and the second most common histology, invasive lobular carcinoma (ILC, 10%–15% of cases) (3,4). Because of distinct molecular and pathologic features (5,6), including lower cellular density per unit volume, ILC is more difficult to detect on imaging, including mammography, ultrasound, MRI, and 18F-FDG PET/CT (7–16). Both primary and metastatic ILC demonstrates lower SUVs on 18F-FDG PET than do comparable invasive ductal carcinoma tumors (11–16). In addition, ILC differs from invasive ductal carcinoma in patterns of metastatic spread (17–20). Given these differences, 18F-FDG PET/CT may be less suited for evaluation of ILC than for evaluation of invasive ductal carcinoma (16).
ILC also differs from invasive ductal carcinoma in receptor expression. In particular, ILC is nearly always (95%) estrogen receptor (ER)–positive (5,21,22), raising the possibility of increased utility of ER-targeting PET tracers for patients with ILC. 16α-18F-fluoroestradiol (18F-FES) is an ER-targeting PET tracer with high sensitivity and specificity for detection of ER-positive tumors (23–27). 18F-FES has been used as a predictive biomarker (28–31) to demonstrate ER heterogeneity (32,33), assess the pharmacokinetics of ER-targeted agents (34), measure residual ER during endocrine therapy (35), and determine the biologic optimal dose of novel ER-targeted drugs (36).
We hypothesized that because of high ER positivity, 18F-FES PET/CT may compare favorably with 18F-FDG PET/CT in patients with ILC. Prospective trials have been conducted at Memorial Sloan Kettering using 18F-FES PET/CT to assist in determining the dose of novel ER-targeted drugs. We reviewed these trials for patients with ILC who underwent 18F-FDG PET/CT within 5 wk of the research 18F-FES PET/CT and had no intervening change in management. Here, we report this head-to-head comparison of 18F-FES and 18F-FDG PET/CT in patients with metastatic ILC.
MATERIALS AND METHODS
Patients
This retrospective evaluation of prospective clinical trials was performed in compliance with the Health Insurance Portability and Accountability Act and with Institutional Review Board approval. All patients provided written informed consent. Six prospective clinical trials using 18F-FES PET/CT in patients with breast cancer (NCT01823835, NCT01916122, NCT02316509, NCT02734615, NCT03284957, and NCT03332797) were reviewed for patients with metastatic invasive lobular breast cancer and standard-of-care 18F-FDG PET/CT performed within 5 wk of research 18F-FES PET/CT and who had no change in therapeutic management between scans. Both the research 18F-FES PET/CT and the standard-of-care 18F-FDG PET/CT studies were performed before therapy, without intervening change in patient management.
Electronic medical records were reviewed for age at 18F-FES PET/CT, sex, and receptor status (ER, progesterone receptor, and human growth factor receptor 2), as well as number of days between the 18F-FES and 18F-FDG PET/CT scans.
PET/CT Imaging and Interpretation
The 18F-FDG PET/CT and 18F-FES PET/CT studies were reinterpreted by a radiologist dually boarded in diagnostic radiology and nuclear medicine with 15 y of PET/CT experience, including experience with both agents.
The 18F-FES PET/CT acquisition was standardized in all studies according to a registered clinical trial (NCT01916122). 18F-FES was manufactured by the Radiochemistry and Imaging Probe Core at Memorial Sloan Kettering Cancer Center using a modified version of a published work by Knott et al. (37). Each patient was administered approximately 185 MBq (5 mCi) of 18F-FES intravenously, followed by a 60-min uptake period. PET/CT scans were acquired supine from the base of the skull to the mid thigh along with low-dose CT scans. Attenuation-corrected images were reviewed on a PACS workstation (GE Healthcare). Physiologic 18F-FES avidity was expected in the liver, bowel, kidney, and bladder. 18F-FES avidity was considered abnormal when it was focal and not considered physiologic.
For 18F-FDG PET/CT examinations, 18F-FDG was obtained from a commercial source. Patients fasted for at least 6 h before 18F-FDG administration. Each patient was injected intravenously with 444–555 MBq (12–15 mCi) of 18F-FDG when plasma glucose was less than 200 mg/dL, followed by a 60-min uptake period. PET/CT scans were acquired supine from the base of the skull to the mid thigh along with low-dose CT scans. Attenuation-corrected images were reviewed on a PACS workstation. 18F-FDG avidity was considered abnormal when it was focal and not considered physiologic or inflammatory.
For both examinations, the organ systems with disease involvement, the number of disease foci in each organ system, and the SUVmax for lesions were recorded. SUVmax was determined by placement of regions of interest around the lesions with the greatest avidity. As lesions had different 18F-FES and 18F-FDG avidity, different lesions were sometimes selected as the most avid for each study. Liver background SUVmax and SUVmean were determined by placement of regions of interest over a 1-cm3 volume of the right lobe of the liver.
Statistics
Results were described using median and range. To assess whether the distribution of the number of lesions or the SUVmax was higher with 18F-FES PET than with 18F-FDG PET, 1-sided Wilcoxon signed-rank tests for paired data were used. To account for the small sample size, results with a P value of less than 0.10 were considered statistically significant.
RESULTS
Patients
Ninety-two patients with breast cancer underwent 18F-FES PET/CT as part of 6 prospective clinical trials. Seventy-eight (85%) were excluded for non-ILC histology. Seven (8%) were excluded for no comparison 18F-FDG PET/CT. The result was 7 evaluable patients. A STARD (Standards for Reporting of Diagnostic Accuracy Studies) diagram for patient selection is presented in Figure 1. The 7 patients were all women with ER-positive, progesterone receptor–positive, and human growth factor receptor 2–negative ILC. The median age was 66 y (range, 48–69 y). For all patients, the 18F-FDG PET/CT was performed before the 18F-FES PET/CT. The median time between scans was 19 d (range, 11–35 d).

STARD diagram for patients screened in this study.
18F-FES PET/CT
All 7 patients demonstrated 18F-FES–avid lesions consistent with metastases (Table 1). All demonstrated osseous metastases, and one demonstrated a biopsy-proven breast recurrence. In total, 253 18F-FES–avid osseous lesions were seen. The 18F-FES SUVmax range for osseous lesions among the 7 patients was 2.6–17.9 (median, 10.2). There was a focus representing breast recurrence in patient 3, with an 18F-FES SUVmax of 6.5. Patient 5 demonstrated a focus in the right lung hilum (SUVmax, 3.6), without a correlate on CT, of unclear etiology. This focus was not included in the lesions suggestive of malignancy, as the right hilum is unlikely to be a site of nodal metastases in a breast cancer patient without axillary or internal mammary nodal metastases. No other organ systems were found to have suggestive 18F-FES–avid foci.
Malignancy Seen on 18F-FES and 18F-FDG PET/CT in the 7 Patients
18F-FDG PET/CT
Six of 7 patients demonstrated 18F-FDG–avid lesions consistent with metastases (Table 1). Six demonstrated 18F-FDG–avid osseous metastases, 1 demonstrated an 18F-FDG–avid, biopsy-proven breast recurrence, and 1 demonstrated 18F-FDG–avid hepatic metastases. In total, 90 18F-FDG–avid osseous lesions were seen. The 18F-FDG SUVmax range for osseous lesions was 3.5–9.9 (median, 5.3). There was 1 focus representing breast recurrence in patient 3 (the same lesion as detected on 18F-FES PET/CT), with an SUVmax of 3.3. Patient 7 demonstrated 20 18F-FDG–avid hepatic metastases with an SUVmax of 5.9. Patient 1 demonstrated 18F-FDG avidity that was probably benign, adjacent to a breast implant. No other organ systems were found to have suggestive 18F-FDG–avid foci.
Comparison of 18F-FES and 18F-FDG PET/CT
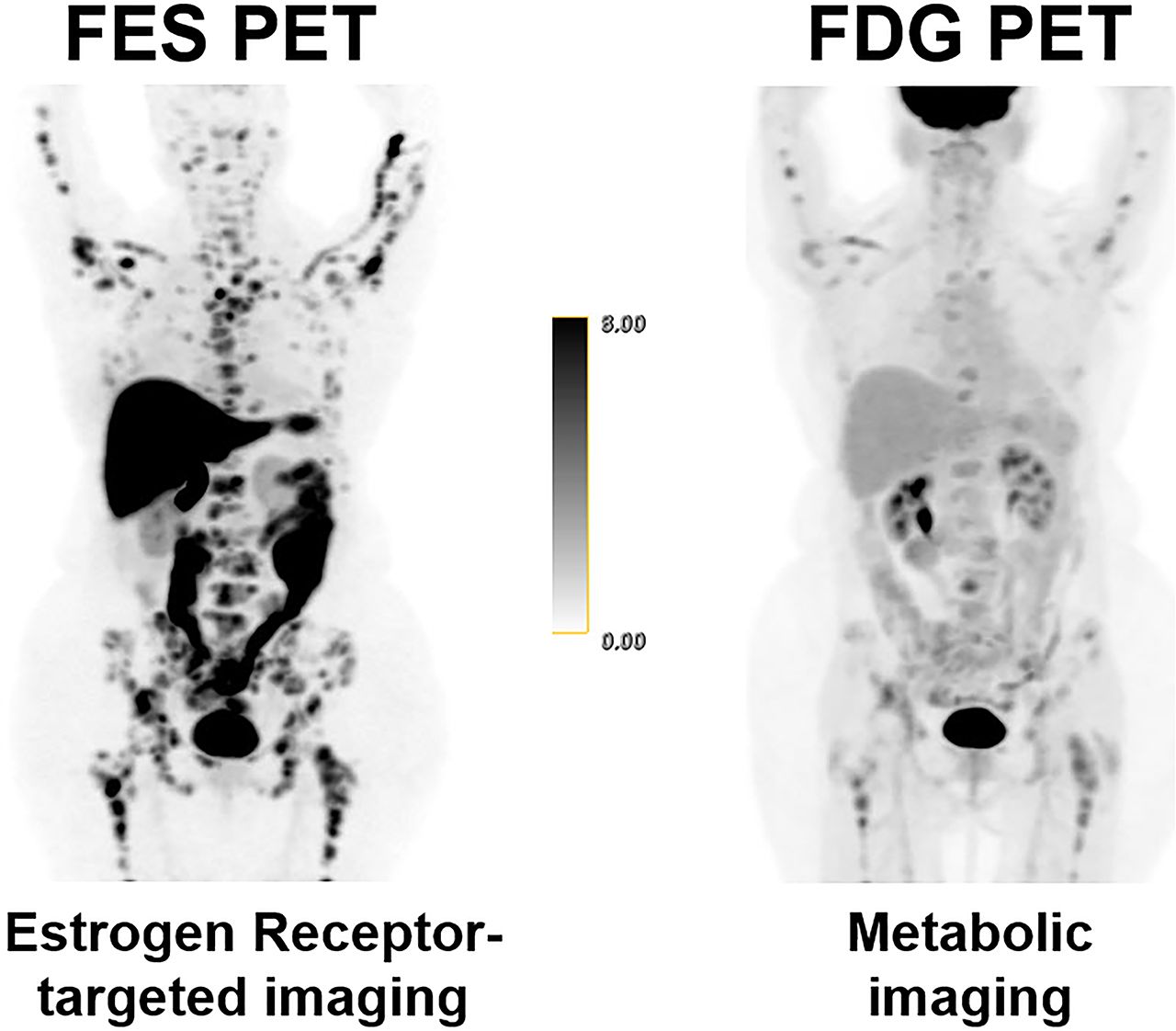
In 5 of 7 patients (71%), 18F-FES PET/CT detected more metastatic lesions than 18F-FDG PET/CT (Table 1; Fig. 2). In these 5 patients, the SUVmax of 18F-FES–avid lesions was greater than the SUVmax of 18F-FDG–avid lesions.

Comparison of 18F-FES PET and 18F-FDG PET in 7 patients with metastatic ILC. Images are maximum-intensity projections from 18F-FES PET scans and 18F-FDG PET scans within 5 wk. In first 5 patients, 18F-FES PET detected more metastatic lesions and demonstrated higher SUVs for metastatic lesions than did 18F-FDG. In patients 1–5, more osseous metastases (solid red arrows) were seen on 18F-FES PET than on 18F-FDG PET. In particular, for patient 5, osseous disease was detected on 18F-FES PET but was not apparent on 18F-FDG. In patient 3, known recurrence in breast (dashed red arrows) demonstrated greater SUVmax on 18F-FES than on 18F-FDG. In patient 1, 18F-FDG avidity around breast implant (green arrow) was probably benign. In patient 5, right hilar focus was of unclear etiology (green arrow). In last 2 patients, 18F-FDG PET detected more metastatic lesions than did 18F-FES PET. In patient 6, more osseous metastases (arrows) were seen on 18F-FDG PET than on 18F-FES PET. In patient 7, more osseous metastases (straight red arrows) were seen on 18F-FES PET, but multiple liver metastases (curved red arrow) were seen only on 18F-FDG PET.
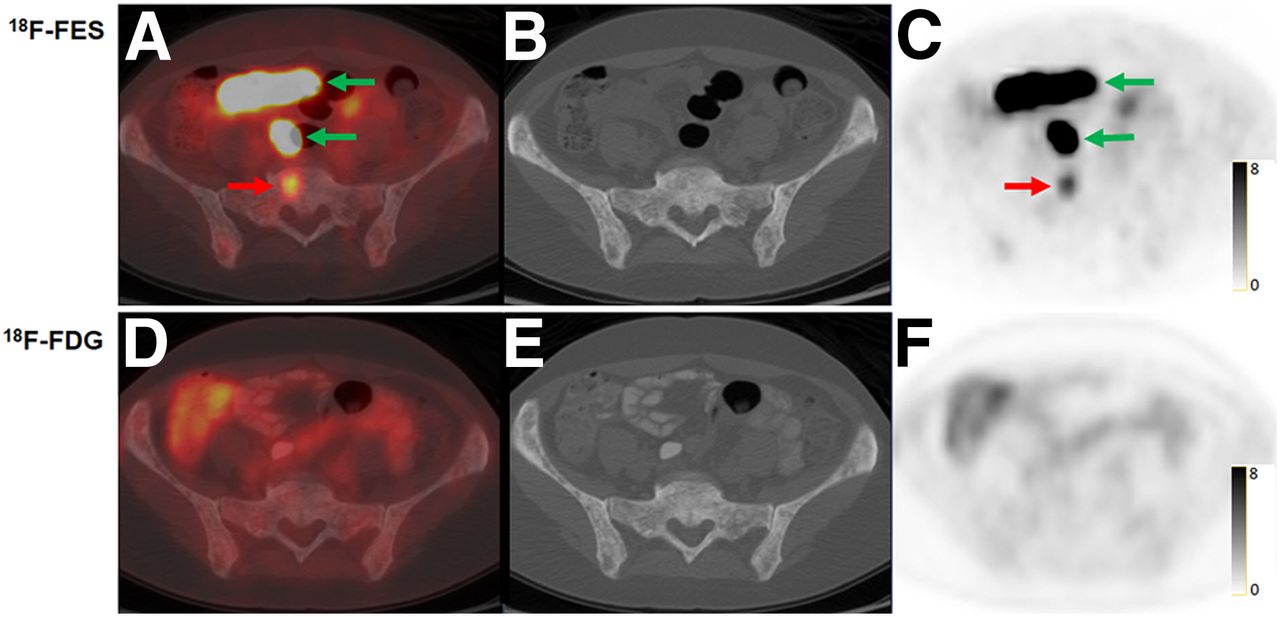
In total, 268 osseous lesions were detected by either 18F-FES or 18F-FDG PET. Of 268 lesions, 253 (94%) were 18F-FES–avid, whereas 90 of 268 (34%) were 18F-FDG–avid. 18F-FES PET detected more osseous lesions (median, 14; range, 2–146 lesions) than 18F-FDG (median, 6; range, 0–56, P = 0.08). In 6 of 7 patients, more osseous foci were detected on 18F-FES PET than on 18F-FDG PET. In 1 patient, 2 avid osseous metastases were seen on 18F-FES PET, but no avid osseous metastases were detected on 18F-FDG PET (patient 5; Table 1, Fig. 2). This patient had extensive sclerotic osseous lesions on CT (Fig. 3) and known active osseous metastases from a biopsy used to enroll the patient in the prospective clinical trial. Patients could demonstrate heterogeneity of tracer avidity, with some osseous metastases being avid for both tracers and others being 18F-FES–avid but not 18F-FDG–avid, or vice versa (patient 7; Fig. 2). Therefore, the total number of osseous metastases detected in the study was higher than the total with either tracer alone.

Metastatic disease apparent on 18F-FES PET but not on 18F-FDG PET in 48-y-old woman with biopsy-proven metastatic ILC (patient 5). Axial 18F-FES PET/CT (A), CT (B), and 18F-FES PET (C) demonstrate 18F-FES–avid osseous foci (red arrows), consistent with avid malignancy. Physiologic activity was also seen in bowel (green arrows). Axial 18F-FDG PET/CT (D), CT (E), and 18F-FDG PET (F) did not demonstrate any 18F-FDG–avid foci suspected of being malignancy.
Additionally, 1 patient (patient 7) demonstrated 20 18F-FDG–avid hepatic metastases that were not apparent on 18F-FES PET (Table 1; Fig. 2). Detection of hepatic metastases is known to be more difficult on 18F-FES PET because of physiologic excretion of 18F-FES by the liver. As expected, in the patients in our study, physiologic liver background was higher on 18F-FES PET than on 18F-FDG PET. The median physiologic liver background 18F-FES SUVmax and SUVmean were 15.4 (range, 12.5–22.9) and 13.8 (range, 10.6–20.3), respectively, whereas the median physiologic liver background 18F-FDG SUVmax and SUVmean were 2.8 (range, 2.2–3.8) and 2.6 (range, 1.9–3.5), respectively.
Figure 4 depicts the number of lesions detected on 18F-FES PET/CT and 18F-FDG PET/CT in each patient and compares the lesional SUVmax for both radiotracers in each patient. Figure 5 graphs SUVmax for all lesions in all patients.

Comparison of lesions on 18F-FES PET/CT and 18F-FDG PET/CT in 7 patients with metastatic lobular breast cancer. (Left) Comparison of number of avid lesions suggestive of malignancy. (Right) Comparison of SUVmax of suspected lesions. In 5 of 7 patients, more lesions were detected and SUVmax was higher on 18F-FES PET/CT than on 18F-FDG PET/CT.
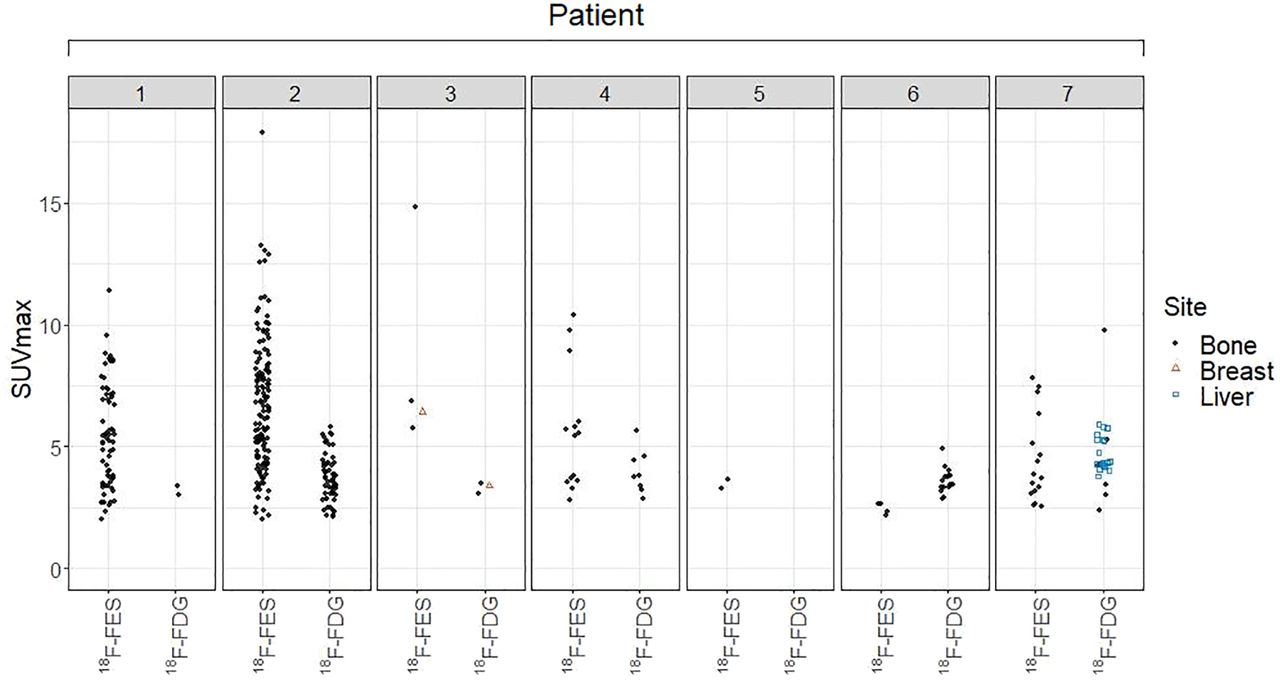
Graphical depiction of SUVmax for all avid malignancy in all PET/CT scans. There was no 18F-FDG–avid malignancy in patient 5. Most metastases were osseous. Patient 3 had breast lesion. Patient 7 had hepatic metastases seen on 18F-FDG.
DISCUSSION
ILC is a histologic subtype of breast cancer with distinct molecular and imaging characteristics. Novel methods may be needed for optimal visualization of ILC. This study took advantage of prospective trials using 18F-FES to perform a head-to-head comparison between 18F-FES and 18F-FDG PET/CT in patients with metastatic ILC and demonstrated that 18F-FES may compare favorably with 18F-FDG in these patients.
ILC is sometimes thought of as a rare tumor type, but this is a misconception. Although only 15% of all breast malignancies are ILC (3,38), 15% of 279,000 breast malignancies a year (39) represents 42,000 malignancies. If ILC was its own category of malignancy, it would be the fifth most common malignancy in women, behind only ductal breast cancer, lung, colon/rectum, and uterine cancer (39). Thus, ILC is common, and improved imaging of this malignancy could have a major impact on health care.
18F-FES PET is gaining increased recognition as a PET tracer with clinical applicability and has recently been approved by the U.S. Food and Drug Administration for evaluation of ER heterogeneity as EstroTep (Zionexae). This early study suggests that evaluation of metastatic ILC may be a clinical scenario in which 18F-FES PET/CT has clinical utility.
Molecular imaging has demonstrated advantages over anatomic imaging for osseous malignancies. Because the attenuation and density of an osseous lesion must change 30%–50% before being detected on CT (40), molecular techniques such as bone scanning and 18F-FDG PET are often more sensitive for detection of osseous malignancy (41,42). Because of the limitations of anatomic imaging in osseous lesions, RECIST does not consider osseous lesions without soft-tissue components to be eligible as target lesions (43). As the most common site of distant metastasis in ILC is bone (44), it is important to have an imaging method that is sensitive for the detection of osseous disease. In this study, 18F-FES PET was more sensitive than 18F-FDG PET for osseous lesions on both a per-lesion and per-patient basis (Table 1). The detection of 18F-FES–avid osseous lesions in ILC can assist with evaluation of the extent of disease and could be considered a method to identify measurable lesions for clinical trials, similar to the recent use of 18F-FDG PET to expand trial eligibility in solid tumors with a predominance of osseous disease (45).
The liver is a recognized site of weakness for 18F-FES PET imaging because of physiologic excretion of 18F-FES through the hepatobiliary system. Thus, if 18F-FES PET is used for patient care, the liver will need to be evaluated by an additional method, such as contrast-enhanced CT or MRI.
Our study had several limitations. The first was the limited number of patients. This study was only an initial comparison of 18F-FES and 18F-FDG PET/CT in patients with metastatic ILC. Because 18F-FES PET/CT is not yet widespread, and because ILC was only recently recognized as a distinct breast cancer subtype requiring alternate methods of molecular imaging (46–48), limited numbers of patients are available for analysis. Second, in the patients in this article, 18F-FDG PET was always performed before 18F-FES PET. Thus, there could have been some progression of disease in the 11–35 d between scans. Third, 18F-FDG PET and 18F-FES scans might not have been performed on the same PET/CT scanner. Fourth, this was a single-institution study. Finally, we did not have histologic confirmation of imaging findings. Although all patients were biopsy-proven to have metastatic ILC, we cannot guarantee that each avid focus was a site of malignancy. However, 18F-FES and 18F-FDG PET/CT imaging findings were typical of findings for metastatic disease.
CONCLUSION
This retrospective review of prospective clinical trials using 18F-FES PET/CT provides the first, to our knowledge, head-to-head comparison of 18F-FES PET/CT and 18F-FDG PET/CT in patients with metastatic ILC. 18F-FES PET compares favorably with 18F-FDG for identifying sites of metastatic disease, particularly osseous metastases. Because ILC is a malignancy in need of improved molecular imaging, larger trials are needed to evaluate the clinical value of 18F-FES PET/CT in these patients.
DISCLOSURE
This work was supported by a Susan G. Komen for the Cure grant (KG110441 to Gary Ulaner) and an NIH/NCI Cancer Center support grant (P30 CA008748). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 18F-FES PET/CT have value for evaluating disease in patients with lobular breast cancer?
PERTINENT FINDINGS: In this retrospective review of prospective clinical trials, 18F-FES demonstrated both more metastatic lesions and higher SUVs for malignancy than did 18F-FDG in 71% of patients.
IMPLICATIONS FOR PATIENT CARE: Our results warrant larger prospective trials of 18F-FES PET/CT in ILC to evaluate potential added clinical value in patients with ILC.
Footnotes
Published online Jul. 17, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 21, 2021.
- Accepted for publication June 15, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Rare Case of Orbital Metastasis from Invasive Lobular Carcinoma: Challenges of 18F-FDG PET/CT and the Search for Consensus on Imaging
- Detecting Metastatic Patterns of Oligometastatic Breast Cancer: A Comparative Analysis of 18F-FDG PET/CT and Conventional CT Imaging
- 68Ga-FAPI PET/CT as an Alternative to 18F-FDG PET/CT in the Imaging of Invasive Lobular Breast Carcinoma
- The Current and Future Roles of Precision Oncology in Advanced Breast Cancer
- WNT4 regulates cellular metabolism via intracellular activity at the mitochondria in breast and gynecologic cancers
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol
- WNT4 executes estrogen regulation of cellular metabolism via intracellular activity at the mitochondria
- Biology of Cancer and PET Imaging: Pictorial Review
- Value of 18F-FES PET in Solving Clinical Dilemmas in Breast Cancer Patients: A Retrospective Study