


Visual Abstract
Abstract
Breast cancer (BC) is a heterogeneous disease in which estrogen receptor (ER) expression plays an important role in most tumors. A clinical dilemma may arise when a metastasis biopsy to determine the ER status cannot be performed safely or when ER heterogeneity is suspected between tumor lesions. Whole-body ER imaging, such as 16α-18F-fluoro-17β-estradiol (18F-FES) PET, may have added value in these situations. However, the role of this imaging technique in routine clinical practice remains to be further determined. Therefore, we assessed whether the physician’s remaining clinical dilemma after the standard workup was solved by the 18F-FES PET scan. Methods: This retrospective study included 18F-FES PET scans of patients who had (or were suspected to have) ER-positive metastatic BC and for whom a clinical dilemma remained after the standard workup. The scans were performed at the University Medical Center of Groningen between November 2009 and January 2019. We investigated whether the physician’s clinical dilemma was solved, defined either as solving the clinical dilemma through the 18F-FES PET results or as basing a treatment decision directly on the 18F-FES PET results. In addition, the category of the clinical dilemma was reported, as well as the rate of 18F-FES–positive or –negative PET scans, and any correlation to the frequency of solved dilemmas was determined. Results: One hundred 18F-FES PET scans were performed on 83 patients. The clinical dilemma categories were inability to determine the extent of metastatic disease or suspected metastatic disease with the standard workup (n = 52), unclear ER status of the tumor (n = 31), and inability to determine which primary tumor caused the metastases (n = 17). The dilemmas were solved by 18F-FES PET in 87 of 100 scans (87%). In 81 of 87 scans, a treatment decision was based directly on 18F-FES PET results (treatment change, 51 scans; continuance, 30 scans). The frequency of solved dilemmas was not related to the clinical dilemma category (P = 0.334). However, the frequency of solved dilemmas was related to whether scans were 18F-FES–positive (n = 63) or 18F-FES–negative (n = 37; P < 0.001). Conclusion: For various indications, the 18F-FES PET scan can help to solve most clinical dilemmas that may remain after the standard workup. Therefore, the 18F-FES PET scan has added value in BC patients who present the physician with a clinical dilemma.
Breast cancer (BC) is the most common malignant disease among women worldwide (1). In The Netherlands, it is estimated that 1 of 7 women will be diagnosed with BC at some point in their life (2). Of all BC patients, roughly 10% develop distant metastases in the first 5 y after primary diagnosis (3). A clinically relevant characteristic of BC is the estrogen receptor (ER), which is expressed by most (79%) breast tumors (4). The ER is an important predictive and prognostic marker and used as a target for treatment. ER-positive breast tumors are likely to respond to hormonal therapy (5).
Currently, ER expression in BC is determined by immunohistochemistry (5,6). However, this gold standard has some limitations. A metastasis biopsy may lead to sampling errors and can be infeasible because of its invasive nature or the location of the lesion. Also, heterogeneity in ER expression between tumor lesions within patients can be a clinical challenge for clinicians (7,8). Discrepancies in ER expression between the primary tumor and the metastasis is observed in 16%–40% of patients (5,8). Furthermore, the ER expression of tumors may change over time. These factors may cause a clinical dilemma regarding both the correct diagnosis and the best choice of therapy, and regular evaluation of the ER status is therefore important. According to the guidelines of the European Society for Medical Oncology, repeated histologic biopsies are recommended to reevaluate the ER status of metastatic BC (9).
However, since it is impossible to evaluate the ER status of every lesion in the body by biopsy, a noninvasive imaging method to measure the ER expression of all tumor lesions in the body would be a useful and valuable tool. PET with 16α-18F-fluoro-17β-estradiol (18F-FES) could be such a tool (10). 18F-FES PET has the potential to visualize the ER expression of all tumor lesions and to estimate the heterogeneity in ER expression in metastatic lesions across the body and can therefore be used for individualized therapy decision making (11,12). A high correlation has been found between 18F-FES uptake and immunohistochemistry findings for determination of ER status (13–15).
18F-FES PET, recently approved for human use in France and the United States, is an evolving imaging technique and may soon play an increasingly important role in clinical practice. Small studies have shown that 18F-FES PET has added value for BC patients presenting a clinical dilemma (16–18). To confirm these initial findings, evaluation of the role of 18F-FES PET in a larger patient sample size is needed, and the role of this imaging technique in routine clinical practice remains to be further determined. Therefore, the aim of this study was to assess the value of 18F-FES PET in a large retrospective patient cohort by evaluating whether the physician’s remaining clinical dilemma after the standard workup could be solved by the 18F-FES PET findings and whether this imaging technique supported BC management.
MATERIALS AND METHODS
Study Design and Patients
This was a retrospective study of all consecutive patients who underwent clinical 18F-FES PET at the University Medical Center of Groningen between November 2009 and January 2019. 18F-FES PET scans were eligible for analysis if they were performed on patients who had, or were suspected to have, ER-positive metastatic BC and for whom pathologic assessment of the primary tumor or suspected metastasis was available but a clinical dilemma remained after the standard workup. For each patient, a 18F-FES PET scan was requested by a medical oncologist in the context of the clinical dilemma, and the validity of the request was confirmed by a nuclear medicine physician. We used only scans that were acquired on a combined PET/CT scanner; scans that were acquired with a PET-only scanner were excluded. If there was a technical imaging problem, the scan was excluded, as were scans performed as part of a clinical trial. In addition, requests for 18F-FES PET that related only to the detection of liver metastases were excluded because of unreliable image interpretation (19). All procedures were performed as part of routine care. The Medical Ethics Committee of the University Medical Center of Groningen reviewed the protocol and decided that this type of research was beyond the scope of the Medical Research Involving Human Subjects Act (METc 2018/418). All data were pseudonymized before data analysis.
18F-FES PET Imaging
18F-FES was produced as described previously (20). To prevent false-negative results, ER antagonists had to be discontinued at least 5 wk before 18F-FES PET, whereas aromatase inhibitors could be continued (19). The tracer (∼200 MBq) was intravenously injected 60 min before a whole-body 18F-FES PET was performed, and the patients did not have to fast. A 40- or 64-slice mCT PET/CT camera (Siemens CTI) was used with a 2-mm spatially reconstructed resolution and an acquisition time of 3 min per bed position. A low-dose CT scan was acquired for attenuation and scatter correction. Some patients underwent 18F-FES PET in combination with a diagnostic CT scan. 18F-FES PET scans were evaluated qualitatively by nuclear medicine physicians, and a standard clinical report was documented in the patient’s file. The scans were divided into 2 categories: those showing ER-positive disease (i.e., at least 1 lesion showing visually increased 18F-FES uptake above the background level) and those showing ER-negative disease (i.e., no lesion showing visually increased 18F-FES uptake above the background level). In cases of ambiguous lesions on qualitative analysis of the 18F-FES PET scan, tracer uptake in the lesion was quantified, using an SUVmax of 1.5 as the cutoff (19). In patients who had also undergone 18F-FDG PET in the standard workup, a secondary (quantitative) analysis was performed. For both PET scans (18F-FDG and 18F-FES), patient preparation, tracer administration, and reconstruction were performed according to European Association of Nuclear Medicine (EANM) protocols. Quantitative analysis was performed on reconstructed images according to the method of EANM Research Ltd. (21).
Standard Workup
We used electronic patient records to assess the standard workup that had occurred before 18F-FES PET was requested. We determined which conventional imaging methods were used, such as bone scintigraphy (with SPECT if necessary), CT, 18F-FDG PET, or MRI, and whether a cytologic or histologic biopsy was performed and at which site. To ensure that the previous imaging techniques and the biopsy were used to solve the same dilemma as the 18F-FES PET, a time frame of a maximum of 3 mo was set between the standard workup and the 18F-FES PET scan.
Data Collection
The following patient data were retrieved from the electronic patient records: patient and tumor characteristics (including age, sex, BC stage, histology, and tumor receptor status), treatment before 18F-FES PET (within a maximum of 4 wk) and after 18F-FES PET (treatment decisions made within a maximum of 4 wk), previous standard workup, category of clinical dilemma, and visual interpretation of 18F-FES PET results (positive or negative).
Outcomes
The primary endpoint was the percentage of cases in which the referring physician’s clinical dilemma was solved on the basis of the 18F-FES PET results. The dilemma was considered solved if the 18F-FES PET provided a solution to the clinical dilemma or if a treatment decision (to change or continue) was based directly on the 18F-FES PET result. If the physician had doubts about the diagnosis after the 18F-FES PET examination, and additional workup was necessary for treatment decision making, the dilemma was considered not solved. Secondary endpoints were the type of clinical dilemma according to 3 categories (to determine the extent of suspected metastatic disease in cases of equivocal lesions on the standard workup or symptoms for which no abnormality could be found on conventional imaging, to determine the ER status of the disease, and to determine which primary tumor caused metastases and the frequency of solved dilemmas per category), the type of treatment before and after 18F-FES PET, and the 18F-FES PET scan results (ER-positive or ER-negative) in relation to how frequently the dilemma was solved.
Statistical Analysis
Descriptive statistics (categoric data) were used to report whether the physician’s clinical dilemma was solved and are presented as percentages. Descriptive statistics were also used to depict the secondary outcomes. Continuous variables were expressed as mean ± SD or median and range, depending on data distribution. A χ2 test was performed to evaluate whether the number of 18F-FES PET scans that solved the dilemma was dependent on the category of clinical dilemma and to assess whether the result of the 18F-FES PET scan (positive or negative) affected the success rate for solving the dilemma. Statistical analysis was performed for the qualitative assessment, and descriptive analysis was performed for the quantitative data. A P value of less than 0.05 was considered statistically significant. All statistical tests were done using SPSS, version 23.
RESULTS
Patients
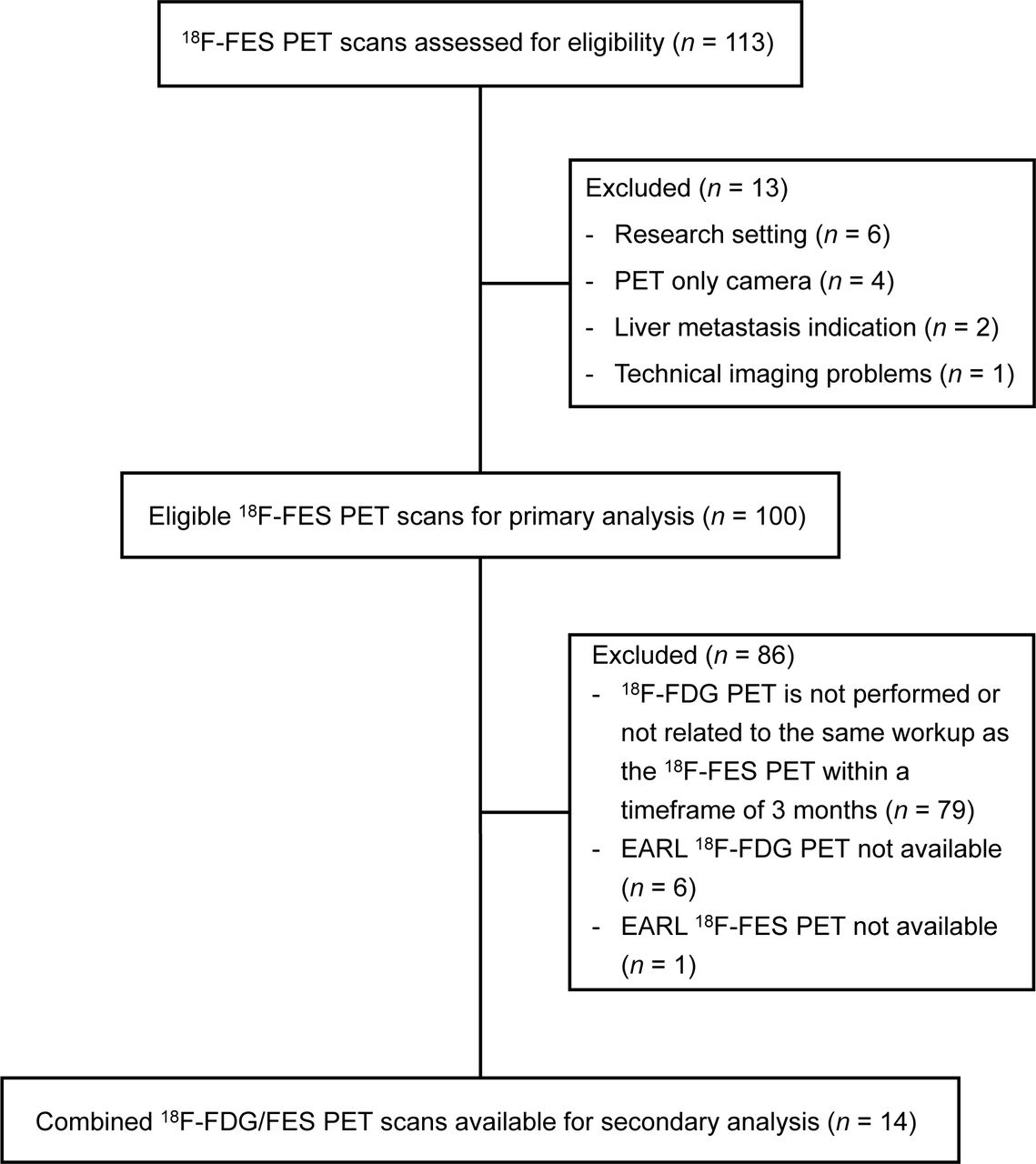
In total, 100 consecutive 18F-FES PET scans, performed on 83 patients, were included in the final database (Fig.1). Of the 12 patients with multiple 18F-FES PET scans, 9 patients had 2 scans, and 3 patients had 3 or more scans. Scan characteristics are summarized in Table 1. All patients had ER-positive BC, based on primary-tumor or metastasis biopsy, except for 2 patients. One was a patient with an ER-negative primary breast tumor and a new palpable breast mass with metastases. A biopsy was not possible, and it was unclear whether this mass was a second primary breast tumor (and possibly ER-positive) or recurrence (n = 1). The other patient was one with suspected primary BC but for whom a histologic breast biopsy indicated a gastric carcinoma with breast metastases (instead of primary BC) (n = 1). In 10 cases, full standard workup before 18F-FES PET was not feasible (Table 1). These cases were included in the analysis because they do present real-life dilemmas occurring in clinical practice.
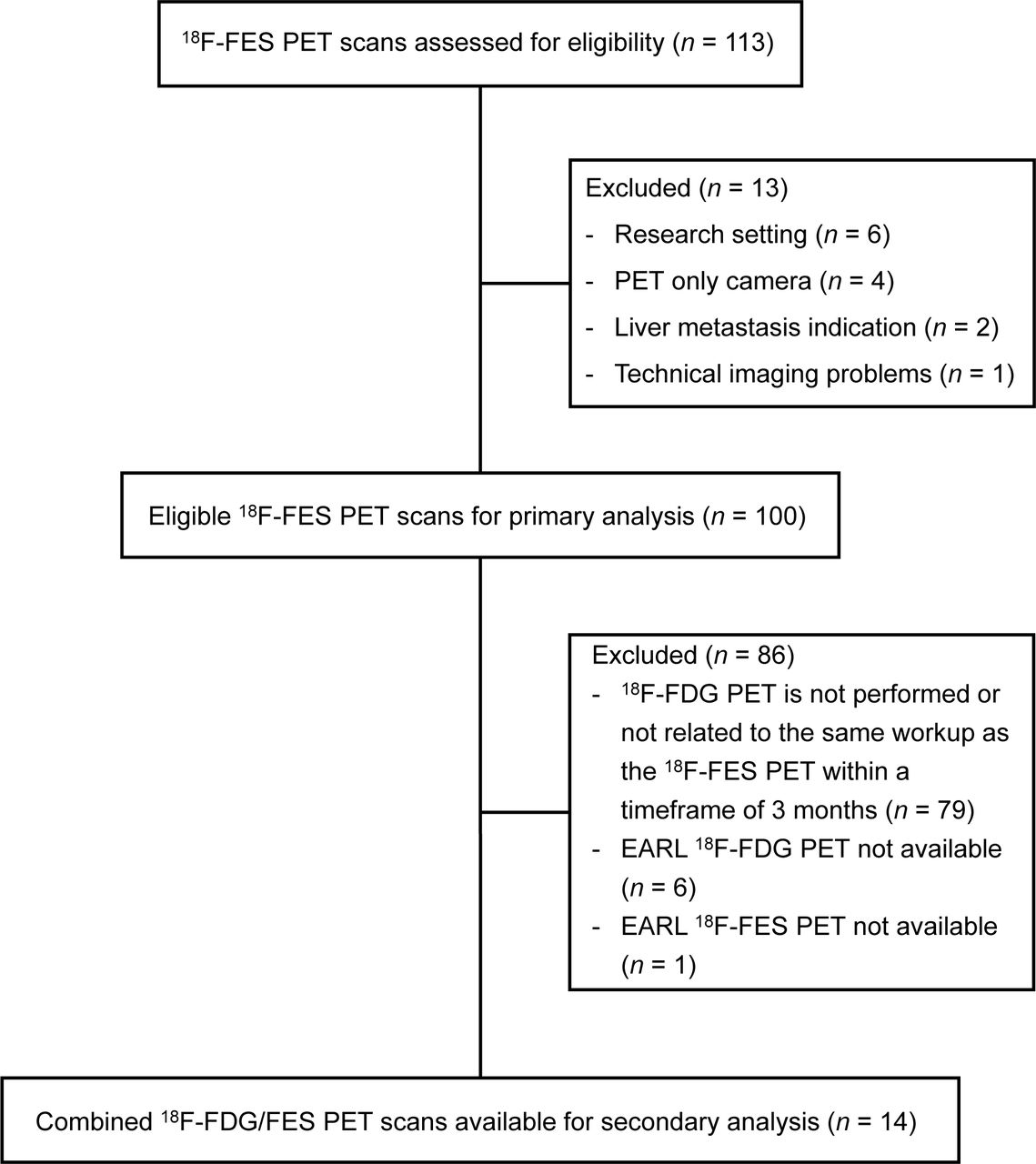
Consolidated Standards of Reporting Trials (CONSORT) diagram.
Patients and Scan Characteristics (n = 100 18F-FES PET Scans in 83 Patients)
Value of 18F-FES PET
The physician’s clinical dilemma was solved in 87% of the cases in which a 18F-FES PET scan was performed (87/100). In most cases (81/87), a treatment decision was based directly on the 18F-FES PET result. In 6 of 87 cases, 18F-FES PET provided a solution to the clinical dilemma (an extra site to biopsy and additional imaging based on new 18F-FES PET findings). In 13 of 100 cases, the dilemma was not solved, for the following reasons: there were still doubts about the diagnosis and an additional biopsy was considered (n = 5); the physician started treatment contradicting the 18F-FES PET result (n = 2); the origin of the lesions remained unclear (n = 2); an additional biopsy to confirm a negative 18F-FES PET scan in fact showed ER expression and thus treatment was based on ER-positive disease (n = 2; 1 patient had lack of response to endocrine treatment); there was doubt whether the metastatic disease was in remission or whether ER underwent positive to negative conversion due to 18F-FES–negative PET results, and therefore 18F-FDG PET was performed to detect metabolically active bone metastases (n = 1); and there was discrepancy between conventional imaging results and 18F-FES PET results (n = 1). Examples of cases in which the physician regarded the results of the 18F-FES PET as conclusive, as well as an example of an inconclusive 18F-FES PET scan, are shown in Figures 2–4.
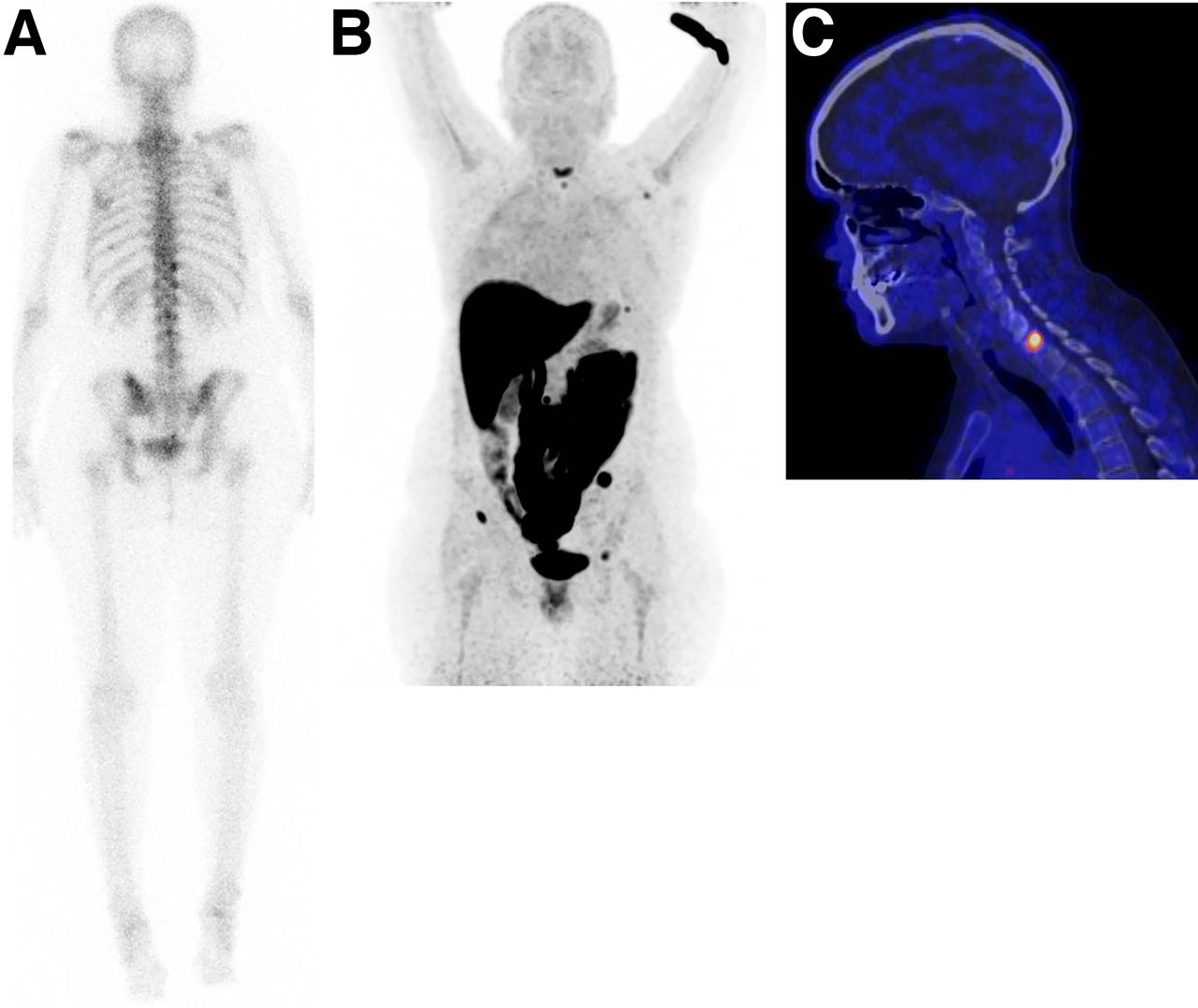
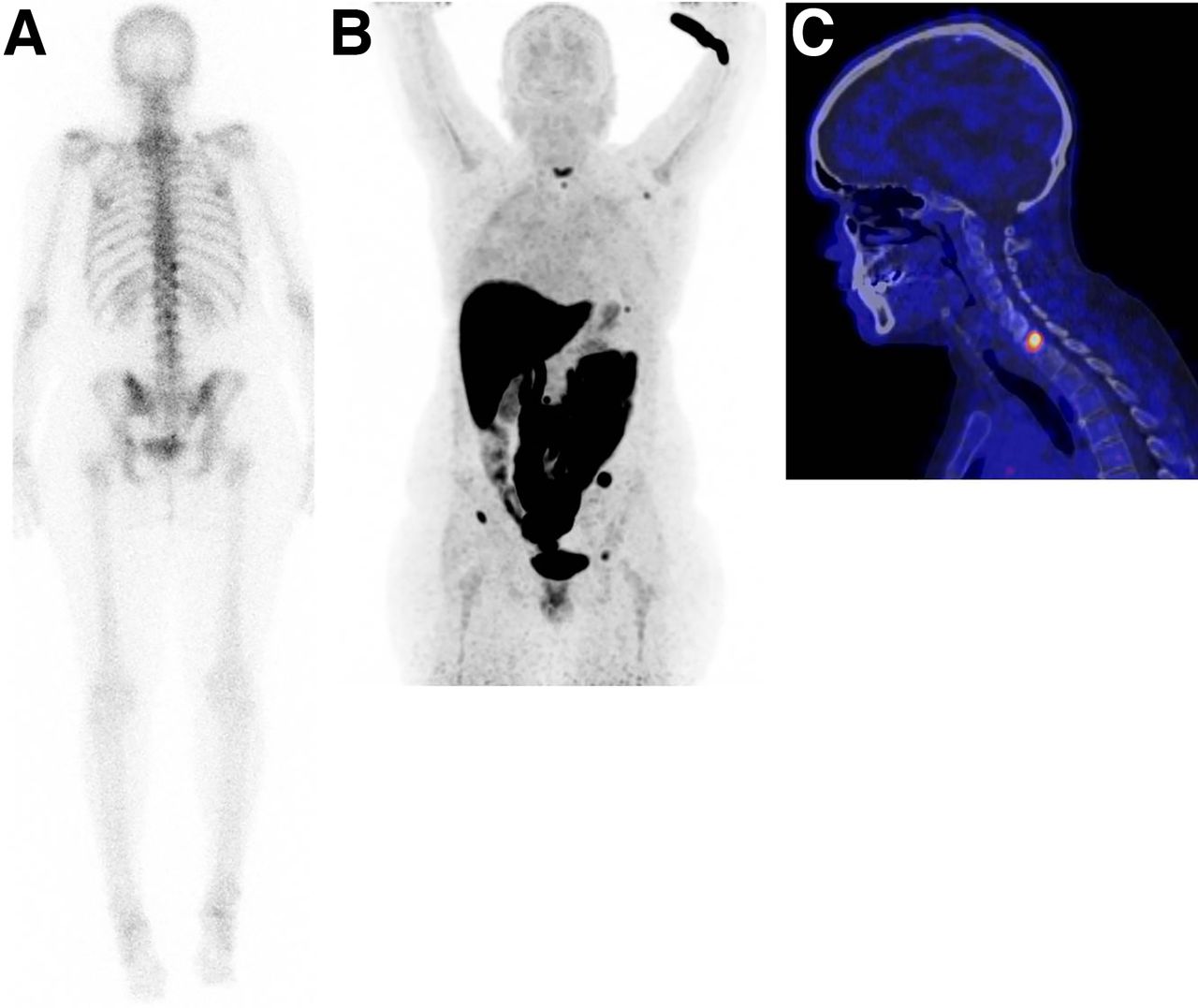
Equivocal lesions on standard workup. A 41-y-old woman known to have Bechterew disease was diagnosed with primary ER-positive BC 2 y previously. Conventional bone scanning was performed because of pain in neck region and showed heterogeneous uptake in spine and pelvis (A, static image posterior view). To differentiate between presence of bone metastases and lesions associated with Bechterew, 18F-FES PET scan was performed. Increased 18F-FES uptake was seen in multiple skeletal lesions: rib, left scapula, spine, and pelvis (B, maximum-intensity-projection view, and C, PET/CT sagittal view of cervical spine). On the basis of these findings, diagnosis was settled on metastatic BC, clinical dilemma was solved, and first-line endocrine treatment was started. In addition, patient received radiation to cervical spine.

Determination of ER status of disease. In 59-y-old woman diagnosed with ER-positive lobular BC 2 y previously and treated with tamoxifen, ER-positive bone metastases were identified 1 y after initial diagnosis. She was treated with first-line endocrine therapy in palliative setting. Thereafter, disease became progressive and palbociclib was added. However, after 2 wk of treatment, she presented with pancytopenia. 18F-FES PET was performed to determine whether bone metastases were still expressing ER and whether there was a rationale for another line of endocrine therapy. Increased 18F-FES uptake could be seen in lymph nodes above and below diaphragm and in multiple bone lesions (e.g., spine, costae, scapulae, sternum, and pelvis) (A, maximum-intensity-projection image; B, PET/CT sagittal view; C, PET/CT transversal view of left axillary region; D, PET/CT transversal view of pelvic region with positive inguinal lymph node). In addition, bone marrow involvement was visible. Diagnosis was settled on ER-positive metastatic disease, clinical dilemma was solved, and another line of endocrine therapy could be considered. However, because of bone marrow involvement, chemotherapy was indicated to achieve therapeutic effect more rapidly.
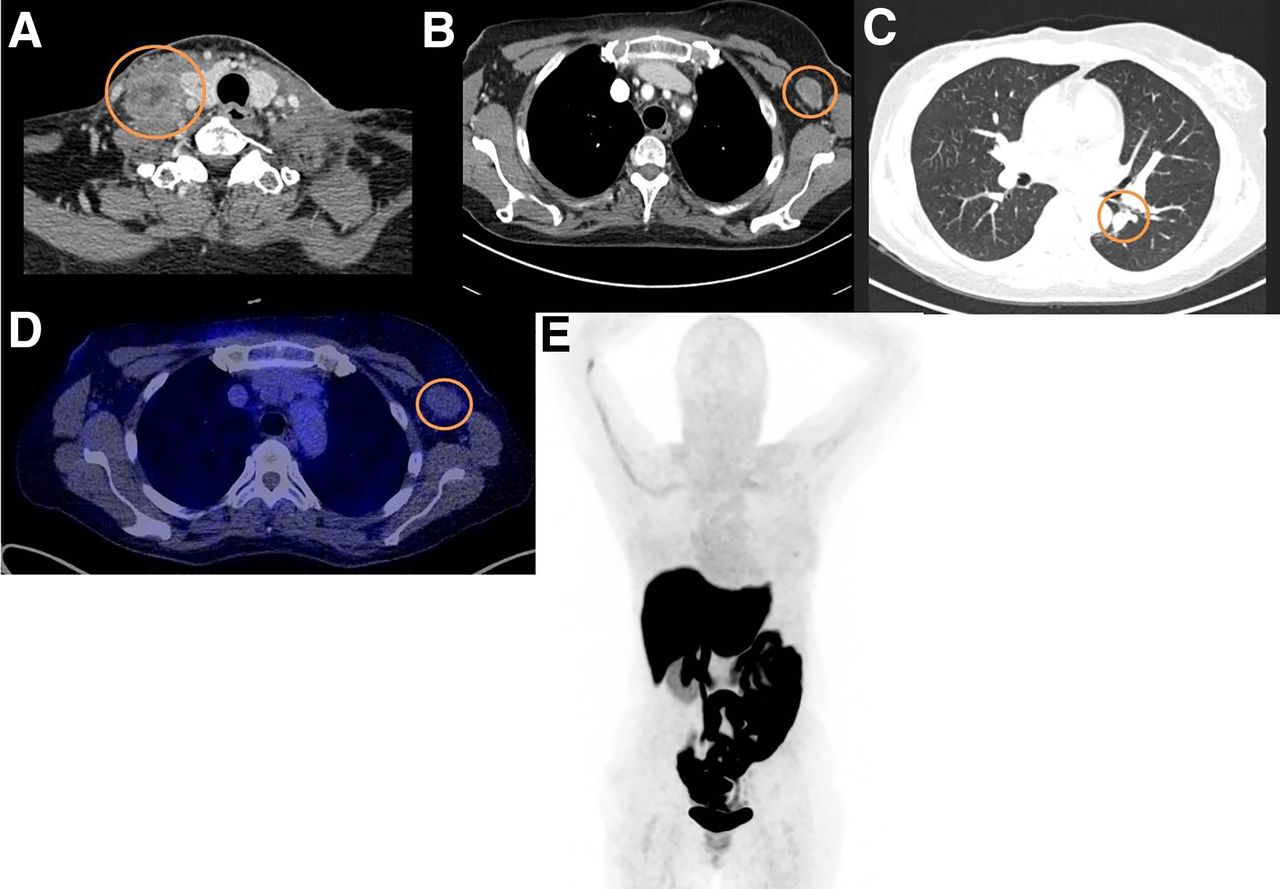
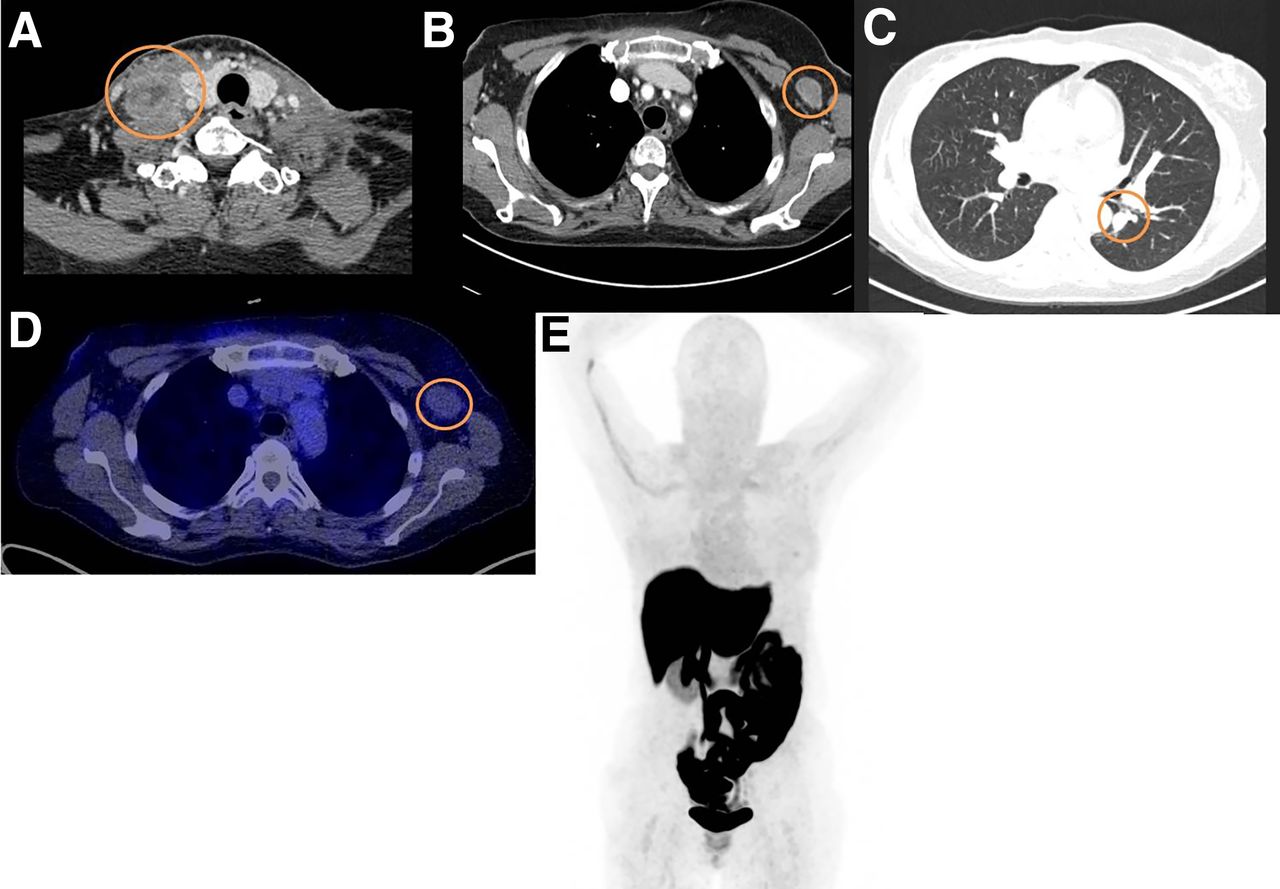
Inability to determine which primary tumor caused metastases. A 63-y-old woman known to have oral squamous cell carcinoma was recently diagnosed with ER-positive BC. At physical examination, a palpable mass was found in right neck region (level IV) and was also visible on CT (A). In addition, enlarged lymph node was visible in left axilla on CT (B), as well as abnormality in left lung (C). The dilemma was whether these metastases were associated with ER-positive BC or oral squamous cell carcinoma. 18F-FES PET was performed to evaluate whether these lesions were metastasis from BC (in case of 18F-FES–positive findings). However, 18F-FES PET did not show any significant tracer uptake in metastatic lesions (D and E). 18F-FES PET result did not solve dilemma, because there could be conversion from ER-positive to ER-negative status; therefore, biopsy of left axillary area was performed and confirmed presence of squamous cell carcinoma.
In 14 patients, 18F-FDG and 18F-FES PET could be compared for secondary quantitative analysis (Fig.1). As shown in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org), we did not observe negative or minimally positive 18F-FDG PET scans.
Category of Clinical Dilemma
Fifty-two of 100 18F-FES PET scans were requested because lesions were equivocal on standard workup. Thirty-one of 100 18F-FES PET scans were requested to investigate the ER status. Seventeen of 100 18F-FES PET scans were requested to determine the origin of metastases. Examples of an 18F-FES PET scan for each indication are shown in Figures 2–4. The success rate of 18F-FES PET in solving the physician’s clinical dilemma did not significantly differ between the different categories of clinical dilemmas (P = 0.334). Of the 52 18F-FES PET scans requested after an equivocal conventional workup, the clinical dilemma was solved in 47 cases (90%). When 18F-FES PET was requested to determine the ER status, the clinical dilemma of the physician was solved in 27 cases (87%). When 18F-FES PET was requested to predict the origin of a metastasis, the dilemma was solved in 13 cases (76%; Fig.5).

Value of 18F-FES PET in solving clinical dilemmas, per category.
Type of Treatment After 18F-FES PET
Of the 81 cases for which a treatment decision was based directly on the 18F-FES PET result, 51 received a new treatment (25/51 endocrine therapy with or without radiotherapy) and 30 continued their treatment. The type of treatment change is shown in Supplemental Table 2.
18F-FES–Negative or 18F-FES–Positive PET Results
Sixty-three of 100 18F-FES PET scans showed ER-positive disease, whereas 37 showed ER-negative disease. The physician’s clinical dilemma was solved in 61 (97%) of the 63 scans showing ER-positive disease and in 26 (70%) of the 37 scans showing ER-negative disease. As a result, the success rate for solving the dilemma differed significantly between the 2 groups (P < 0.001). Figure 4 provides an example of a 18F-FES PET scan showing ER-negative disease in which the scan was not directly helpful for the clinician.
DISCUSSION
In this retrospective study, we aimed to investigate the value of 18F-FES PET in the management of BC patients facing a clinical dilemma that could not be solved after the standard workup. Further investigation in such cases is of clinical importance since a persistent clinical dilemma might lead to decreased survival (22) and unnecessary therapy because of overtreatment or undertreatment (17).
To our knowledge, this was the largest study evaluating the value of 18F-FES PET in this target group. We showed that 18F-FES PET can be clinically meaningful and can support clinical decision making in most BC patients who present a persisting clinical dilemma despite standard workup. This study also provided more insight into the clinical indications for the examination and the physician’s diagnostic concerns. These findings can potentially support clinical implementation of 18F-FES PET.
The percentage of clinical dilemmas solved by 18F-FES PET (87%) is consistent with the findings of previous smaller studies (16,18). One study reported improved diagnostic understanding in 88% of cases based on the 18F-FES PET scan (16). Another study found that 18F- FES PET had added value (89%) in the diagnosis of newly diagnosed BC patients (18). By showing that 18F-FES PET can support BC management with both a changed and a continued treatment plan, the present study adds value to the previous studies.
This study identified clinical dilemmas associated with BC in which 18F-FES PET may play a role in guiding treatment selection, including, but not limited to, determination of the ER status of the disease. An accurate request for 18F-FES PET is necessary for clinical interpretation by the nuclear medicine physician and improves the 18F-FES PET report (23). In the present study, the physician’s clinical dilemma was equally solved for all 3 indication categories, as is in line with a previous study (16). One third of the 18F-FES PET scans were requested to determine ER status in known or suspected metastatic lesions, in agreement with the results of van Kruchten et al. (16). The potential indications for 18F-FES PET in the literature included assessment of ER status of disease, ER heterogeneity in metastatic disease, staging and restaging, therapeutic options for hormonal treatment, and prediction of response to hormonal therapy (13,15,19,24). However, the role of 18F-FES PET is limited in detecting ER-positive lesions in the liver, because of high physiologic 18F-FES uptake due to its metabolism.
The percentage of lobular tumors in the present study was slightly higher than in the general population (25,26). This finding supports the previously described hypothesis that metastatic lesions in lobular BC are difficult to detect with standard imaging (27,28) and that this disease presents the physician with a clinical dilemma relatively frequently. For this setting in the present study, we found that clinical dilemmas in lobular BC and clinical dilemmas in ductal BC were solved equally well by 18F-FES PET (86% vs. 88%).
Recently, a high specificity of 98% and sensitivity of 78% for the assessment of ER status by 18F-FES PET were reported, using biopsy as the gold standard (24). This means that there are few false-positive findings. Therefore, 18F-FES PET can be a good alternative tool if a biopsy is not possible or does not solve the dilemma; both cases occurred in our study. In the present study, the clinical dilemma was solved more frequently if the 18F-FES PET showed ER-positive disease than ER-negative disease—a finding that relates to its higher specificity than sensitivity. Our results are comparable to those of van Kruchten et al. (16). However, caution is necessary in scans showing ER-negative disease. In our study, 9 of 14 18F-FES PET scans of patients with known metastatic BC showed ER-negative disease despite an ER-positive primary tumor. This finding could be explained by the dynamics of BC over time (such as receptor status conversion), good response to endocrine treatment, or false-negative findings.
This study had limitations. It was retrospective, and data were retrieved from electronic patient charts. Therefore, interpretation bias may play a role. Furthermore, our retrospective design did not allow us to use questionnaires to grade how helpful the 18F-FES PET was (16). Also, the intended therapy before 18F-FES PET could not be compared with the therapy that was chosen after the scan. The strengths of this study were its large sample size, heterogeneous population, inclusion of all consecutive eligible patients over more than 9 y, and structured and detailed analysis of a real-life daily clinical practice setting.
CONCLUSION
We found that for various indications, the 18F-FES PET scan can help to solve most clinical dilemmas that remain after standard workup. 18F-FES PET improves the physician’s understanding of the disease status in BC patients and provides information for personalized treatment decision making. Therefore, the 18F-FES PET scan has added value in BC patients who present a clinical dilemma.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 18F-FES PET have added value for solving clinical dilemmas in BC patients?
PERTINENT FINDINGS: In this retrospective study in a real-life daily clinical practice setting, clinical dilemmas were solved by 18F-FES PET in most BC patients.
IMPLICATIONS FOR PATIENT CARE: Our findings support the use of 18F-FES PET as a clinically meaningful diagnostic tool that supports clinical decision making in BC patients who present a persisting clinical dilemma despite standard workup.
Footnotes
Published online May 14, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 14, 2020.
- Accepted for publication December 28, 2020.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 18F-FES PET/CT on Clinical Decisions in the Management of Recurrent or Metastatic Breast Cancer
- The Current and Future Roles of Precision Oncology in Advanced Breast Cancer
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol